
Abstract
Global importance:
Leptospirosis is the most widespread zoonosis worldwide. Mammals (eg, rats, horses, cows, pigs, dogs, cats and aquatic species, such as sea lions and northern elephant seals) can all be infected by leptospires. Infection in animals occurs through contact with urine or water contaminated with the bacteria. In people, the disease is acquired mainly from animal sources or through recreational activities in contaminated water.
Practical relevance:
Literature on the clinical presentation of leptospirosis in cats is scarce, although it has been demonstrated that cats are susceptible to infection and are capable of developing antibodies. The prevalence of antileptospiral antibodies in cats varies from 4% to 33.3% depending on the geographical location. Urinary shedding of leptospires in naturally infected cats has been reported, with a prevalence of up to 68%. Infection in cats has been associated with the consumption of infected prey, especially rodents. Thus, outdoor cats have a higher risk of becoming infected.
Clinical challenges:
Clinical presentation of this disease in cats is rare and it is not known what role cats have in the transmission of leptospirosis. Ongoing work is needed to characterise feline leptospirosis.
Audience:
This review is aimed at all veterinarians, both general practitioners who deal with cats on a daily basis in private practice, as well as feline practitioners, since both groups face the challenge of diagnosing and treating infectious and zoonotic diseases.
Evidence base:
The current literature on leptospirosis in cats is reviewed. To date, few case reports have been published in the field, and information has mostly been extrapolated from infections in people and dogs. This review is expected to serve as a guide for the diagnosis and management of the disease in cats.
Aetiology
Leptospirosis is caused by spirochetal bacteria of the genus Leptospira. These are highly motile, elongated and helically coiled bacteria that differ morphologically from other spirochetes by having a ‘question mark’ or hook-shaped end.1–3 The genus Leptospira was originally divided into two species: Leptospira interrogans, containing the pathogenic serovars, and Leptospira biflexa, containing the non-pathogenic saprophytic serovars. 4 However, this phenotypic classification has been largely superseded by genetic classification, based on genotypic identification techniques, that includes all serovars of L interrogans sensu lato and L biflexa sensu lato (sensu lato is a Latin phrase meaning ‘in the broad sense’ and is often used taxonomically to indicate a species complex). 3
Currently, 22 species of Leptospira have been identified; 4 at least 10 of these are pathogenic. There are also seven saprophytic species and five species of indeterminate pathogenicity. 5 It is likely that more species will be described in the future. Pathogenic Leptospira species are divided into serovars, each with distinct antigenic compositions; to date, over 260 pathogenic serovars, arranged into 26 serogroups, have been identified. This serological classification, based on determining antigenic characteristics, is more useful diagnostically and also better serves epidemiological purposes.
All mammals may be susceptible to Leptospira infection. 3 There are primary (definitive) or carrier hosts for some serovars (eg, dogs are hosts for Canicola; cows and sheep for Hardjo; pigs for Pomona and Bratislava; and rats for Icterohaemorrhagiae and Copenhageni). These contribute to a greater extent to the spread of bacteria in the environment compared with incidental or dead-end hosts (ie, that suffer acute disease and are unlikely to serve as a source of transmission; eg, humans). The definitive host is typically infected at a young age and commonly exhibits minimal clinical disease, whereas animals infected with non-host-adapted serovars are expected to exhibit more severe clinical signs. 3
Epidemiology
Leptospirosis is endemic in almost all regions of the world. 2 Its incidence usually increases at the end of the summer months, while in the tropics most infections occur during and after periods of rainfall.1,2 Pathogenic Leptospira species experience optimal growth at temperatures of 28–30°C. Although they do not replicate outside of the host, they can survive for months in moist soil saturated with urine,1,3 and this can lead to significant environmental contamination. In people, there are three main factors associated with the risk of disease transmission: (1) water exposure; (2) exposure to carrier rodents; and (3) transmission from livestock or pets. 6
Feline leptospirosis was first described in 1972, 7 and prevalence studies show the main serovars belong to serogroups Australis, Autumnalis, Canicola and Sejroe,8–18 although there are geographical variations. The most frequent serovars involved in feline leptospirosis in Europe – according to the European consensus statement on leptospirosis, and based on the prevalence of antibodies measured by the microscopic agglutination test (MAT) – belong to serogroups Australis, Autumnalis, Ballum, Canicola, Grippotyphosa, Icterohaemorrhagiae, Pomona and Sejroe. 19 The most commonly reported serovars in cats in the USA belong to serogroups Australis, Autumnalis, Grippotyphosa and Pomona.8,20 Figure 1 shows the countries where the prevalence of leptospirosis in cats has been reported, based on MAT and/or urinary and blood PCR. Table 1 summarises previous research on feline leptospirosis prevalence by MAT diagnosis. Overall seropositivity reported in these studies ranged from 4% to 33.3%, with no clear association with clinical disease.

Map indicating (in red) the countries where the prevalence of leptospirosis in cats has been reported, based on microscopic agglutination test (MAT) and/or urinary and blood PCR
Prevalence data for leptospirosis in cats diagnosed by microscopic agglutination test

Most prevalent serovar reported in the study
Leptospiral infection in cats has been associated with the consumption of infected prey, 29 involving serovars of the Autumnalis and Ballum serogroups. 3 Outdoor cats have an increased risk of becoming infected with leptospires since they are in close contact with reservoir hosts. In rural areas, cats can also become infected via urine from pigs and cows.12,15,28–30 The presence of another cat in the household significantly increases the risk of seropositivity for leptospirosis. 14
At present, it is not completely understood which serovars cause incidental infections in cats. Based on previously published reports of acute leptospirosis in cats, serovars belonging to Autumnalis, Australis, Ictero-haemorrhagiae, Grippotyphosa, Pomona and Sejroe serogroups are involved.14,18,30–32 Several studies have confirmed renal carriage of Leptospira species by PCR, and these cats had antibodies mainly against serovars belonging to Australis, Canicola, Ictero-haemorrhagiae and Pomona serogroups. Given this fact, cats could be a chronic reservoir host for the bacteria and a possible risk factor for human infection.10,11,13,14,16,26,30,33,34
Table 2 summarises the scant research that has been carried out in cats in different countries to determine the prevalence of Leptospira DNA shedding in urine. In these studies, the prevalence ranged from 0% to 67.8%, with no clear association with clinical disease. The prevalence may differ depending on the geographical location and the PCR-selected primers, among other factors.
Summary of current research on prevalence of urinary shedding of Leptospira DNA in cats

Pathogenesis
Depending on the host and infecting serovar, leptospiral infection may cause a spectrum of syndromes from asymptomatic carriage to fulminant, acute disease. 3 Reports of clinical disease due to Leptospira species in pet cats are scarce.
Leptospires can enter the body through cuts and abrasions, mucous membranes, such as the conjunctiva, or through moist, weakened skin. The bacteraemia lasts around 7 days. The pathogenesis of the disease in cats remains unknown, although it is assumed to be similar to that in humans and dogs 37 (Figure 2). Acute clinical disease occurs with the bacteraemic phase of the disease.1,2,38 It is seen mainly in young incidental hosts and is usually associated with haemolysin-producing bacteria, such as the Ictero-haemorrhagiae or Pomona serogroups, which cause haemolytic disease, haemoglobinuria, jaundice and, in severe cases, death. 3 After leptospires have reached a critical level in the blood, clinical signs appear due to the action of leptospiral toxins or toxic cellular components.1,2,38 Organ damage occurs as a result of leptospires replicating and inducing cytokine production and by direct invasion of inflammatory cells. 3

Proposed pathogenesis of leptospirosis in cats. The figure depicts the transmission mechanisms through which a cat can become infected by Leptospira species: preying on rodents, sharing the environment with farm animals that shed the bacteria in urine, or through standing water containing bacteria. Once the animal has become infected it suffers a period of bacteraemia of approximately 7 days and leptospires can be identified in blood. The main target organs in cats are the kidney and the liver; lungs, brain and eyes may also be affected, especially in dogs. Replication of leptospires occurs in the kidney leading to urinary bacterial shedding. Image ©Biorender
The primary lesions develop in the endo-thelium of the small blood vessels, leading to localised ischaemia, and resulting in renal tubular necrosis, among other target organ damage (Figure 2). Renal colonisation occurs in most infected animals because the bacteria replicate and persist in the cells of the renal tubule epithelium. This multiplication process causes the release of cytokines and the recruitment of inflammatory cells, which trigger nephritis.1,2,38 Chronic interstitial nephritis, which may result in chronic renal damage, has been described in cats infected with leptospires. 16 After 10 days of infection, leptospires enter the tubular lumen and are eliminated in the urine over a period of days to months.1,2,38 The duration of elimination via the urine and its intensity varies from species to species and animal to animal, and depends on the infecting serovar; 3 precise information on these aspects is currently unavailable in cats.
As mentioned earlier, cats can act as carrier hosts, not developing clinical disease, but shedding bacteria into the environment in their urine. An epidemiological study has confirmed the presence of leptospiral DNA in the urine of cats for more than 8 months after infection, with little or no association with disease. 11 However, this does not rule out the possibility that infected animals could develop kidney disease at a later stage. The development of the carrier state and the specific mechanisms required for leptospires to enter the lumen of the proximal renal tubules, adhere to renal epithelial cells, evade antibodies in the filtrate and acquire the nutrients they need to replicate are not well understood. 3
Leptospiral pulmonary haemorrhage syndrome (LPHS) has been recognised in people and dogs. This syndrome may be present in 70% of dogs infected with leptospires. 39 The clinical signs associated with canine LPHS are mainly acute and findings correspond to severe alveolar and subpleural haemorrhages, which cause an associated dyspnoea. While, to date, LPHS has not been described in cats, chronic liver inflammatory infiltration, fibrosis and multifocal hepatic necrosis have been reported.14,16,31 Damage to organs including the spleen, eyes, meninges, muscle and placenta has also been reported in species other than cats.2,3,40
Diagnosis
Clinical signs
In cats, clinical signs are, at most, mild, despite the presence of leptospires in the blood and urine.
Clinical signs reported in infected cats (based on confirmation by MAT and/or PCR) include polyuria, polydipsia, haematuria, uveitis, lameness, lethargy, anorexia, weight loss, ascites, vomiting, diarrhoea, pain on handling, and inflammatory lesions on the skin and digits.11,14,17,18,25,30-32,59 Pathological findings reported in these animals include the presence of haemorrhagic or straw-coloured thoracic and peritoneal fluids.31,18 Some cats with antibodies against Leptospira species have been found to have signs associated with renal disease and/or histopathological evidence of renal inflammation.14,16,30,35,59 As in dogs, leptospirosis in cats can cause acute kidney injury that leads to chronic kidney disease.19,60 Lesions in the liver of affected cats have been reported less commonly than in dogs.11,18,29,31,32 Tables 3-5 collate information from several papers that detail the clinical signs in cats at the time of presentation, the laboratory test used for diagnosis and the Leptospira serovars involved. The cases have been divided into cats with acute disease (Table 3), those identified as chronic carriers (Table 4) and those with a history of exposure (Table 5).
Clinical signs of leptospirosis in cats based on published studies of acute disease

MAT = microscopic agglutination test; + = positive; – = negative; AKI = acute kidney injury; NP = not performed; 4+, 8+ = number of positive cats in the study
Clinical signs of leptospirosis in cats according to published studies of chronic carrier cases
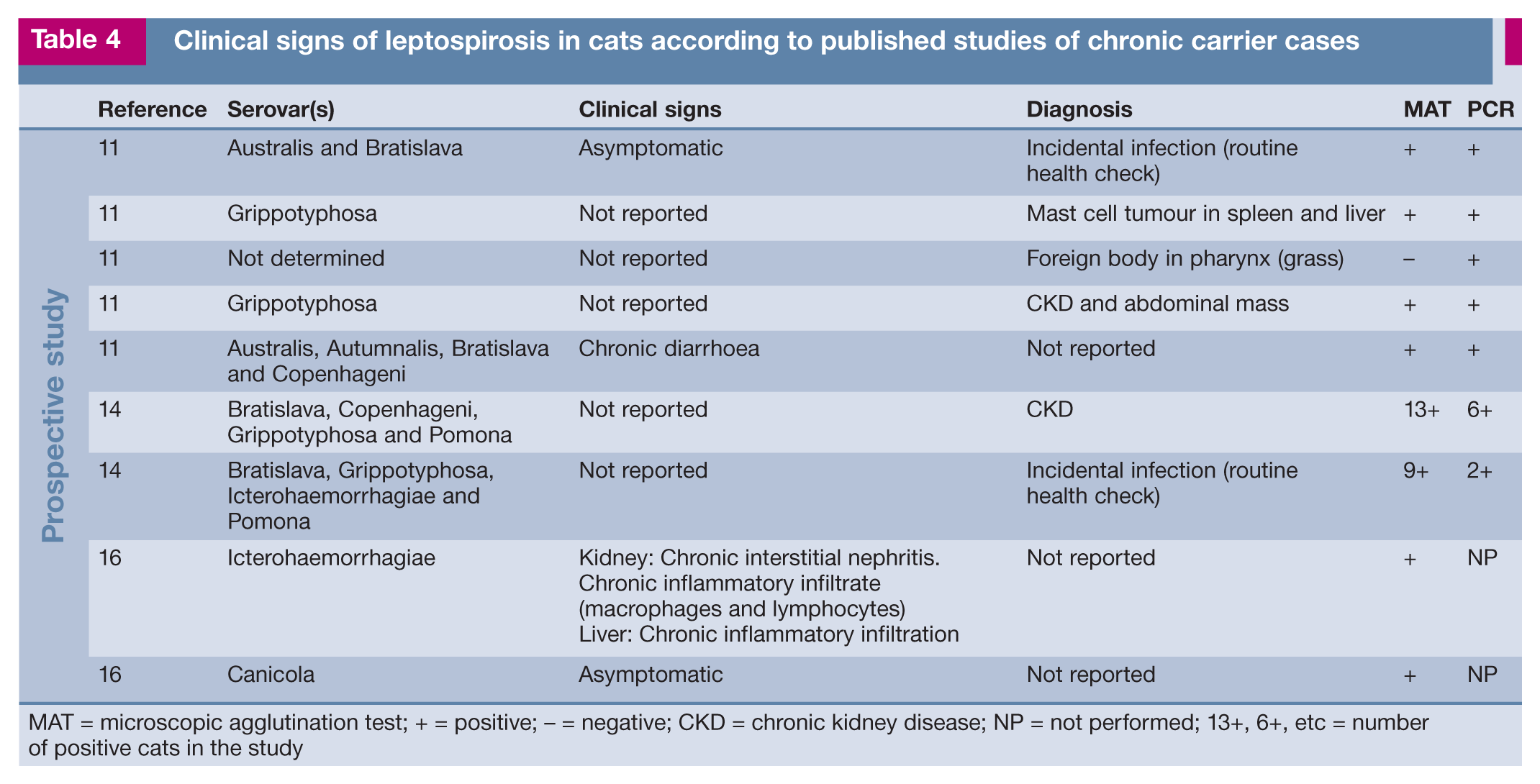
MAT = microscopic agglutination test; + = positive; – = negative; CKD = chronic kidney disease; NP = not performed; 13+, 6+, etc = number of positive cats in the study
Clinical signs of leptospirosis in cats based on published studies of animals with a history of exposure

Clinicopathological data
Table 6 summarises some of the most common clinicopathological abnormalities associated with leptospirosis in cats.

USG = urine specific gravity; FeLV = feline leukaemia virus; FIV = feline immunodeficiency virus
Complete blood count
Leukocytes can fluctuate according to the stage and severity of infection. Leukopenia is a possibility during leptospiraemia, evolving to leukocytosis owing to neutrophilia with a left shift. In advanced states, leukocyte counts may be in the range of 16.5–45 x 109/1 (reference interval 2.75–11.75 x 109/1).18,19,60,61
Serum biochemistry
Urea and creatinine concentrations are increased in 80–90% of cases of canine lepto spirosis. 60 Most infected cats present with azotaemia at the time of diagnosis. The increase is usually moderate to severe.11,14,25,31,32,59 In affected dogs, serum liver enzyme (alkaline phosphatase [ALP] more commonly than alanine aminotransferase [ALT]) and total bilirubin increases are associated with liver dysfunction.38,40,60 Conversely, in feline leptospirosis these increments are not as characteristic, and only slight increases have been reported.11,18,25,31,32 Leptospire toxins inhibit Na+K+-ATPase activity in the epithelial cells of the renal tubules in cats and dogs, which can lead to significant renal losses of electrolytes, resulting in severe hypo-ka laemia. 60 In cats, increases in serum phosphorus concentration have been reported, probably associated with a decrease in the glomerular filtration rate. 31
Urine analysis
Findings in dogs include isosthenuria or occasionally hyposthenuria, glycosuria, proteinuria, bilirubinuria, haematuria, pyuria and the presence of casts in fresh urine sediment.38,60 In cats, hyposthenuria, haematuria and proteinuria have been reported.30,31 Leptospires are not visible on routine fresh urinary sediment examination, as the size of the bacteria is below the resolution of light microscopy. 19
Ultrasonographic findings
The few published reports of feline leptospirosis describe renal ultrasonographic findings that are similar to those in canine leptospirosis, including a granular appearance of the kidney, enlarged kidneys with a cortex that is thinner than the medulla, a slightly hyperechogenic renal cortex and a decrease in the definition of the corticomedullary junction.31,32 Heterogeneity in the pancreatic and liver parenchyma has also been reported in one case. 32
Specific testing
Laboratory diagnosis of leptospirosis in veterinary medicine is usually based on the demonstration of serum antibodies by MAT and ELISA, and/or isolation of Leptospira DNA from blood and urine by PCR. Bacterial culture of blood and/or urine is not widely used because it is time consuming. Specific diagnostic tests that are available for cats are MAT and PCR.
Microscopic agglutination test
Determination of antibody titre by MAT is the recommended technique for leptospirosis diagnosis, as MAT reactivity to a serovar suggests exposure to a serovar belonging to the corresponding serogroup (though not necessarily to the specific serovar tested). 62 The selection of the serogroups and the serovars to be evaluated depends on the geographical location of the patient’s likely exposure. Antibodies (IgM and IgG) are detected at around 15 days post-infection by MAT. 3 Little information is available on the duration of these antibodies in the blood of cats. Clinical interpretation should always be based on the results of paired serum titres, and it is worth noting that some infected animals may produce a result that is lower than the widely accepted minimum significant titre result of 1:100. 3 It is even possible that seroconversion in cats is expressed at a lower titre compared with dogs. 59
MAT results are strongly dependent on laboratory quality control, and there is considerable inter-laboratory variability. 63 Practitioners are encouraged to submit diagnostic samples to laboratories that adhere to a proficiency scheme. 64 Test interpretation may be more reliable in cats than in dogs because no interference with vaccine antibodies exists as cats are not vaccinated. 37 Furthermore, laboratory-reared young adult specific pathogen-free cats infected with Borrelia burgdorferi did not form antibodies against Leptospira species as a cross-reaction. 59 The authors of that study suggest that positive Leptospira species MAT results from cats in the field are likely to reflect antibodies against leptospires and not B burgdorferi.
ELISA and rapid immunodiagnostic screening tests
ELISAs used for leptospirosis identify the presence of leptospiral antibodies (specific IgM class antibodies) earlier than MAT, at between 4–6 days post-infection. 3 The main advantages of ELISA compared with MAT are, in the authors’ opinion, the stability of antigenic preparations and the genus specificity, meaning all types of leptospires can be diagnosed with a single antigenic preparation, irrespective of the causal serovar. 65 In dogs, a combination of ELISA plus MAT is recommended for leptospirosis diagnosis. 19
Rapid patient-side tests for leptospirosis diagnosis were developed almost a decade ago. 66 Curtis et al performed a recombinant LipL32-based rapid in-clinic ELISA (SNAP Lepto) for the detection of antibodies against Leptospira species in dogs in 2015. 67 Neither of the tests distinguish between serovars, nor do they provide a titre magnitude. The first test 66 is based on the detection of Leptospira-specific IgM and has demonstrated a sensitivity and specificity of 100% and 95.3%, respectively. It can therefore detect dogs with clinically suspected acute leptospirosis. Dogs previously vaccinated or suffering from an acute but subclinical infection can also produce positive results. A LipL32-based in-clinic ELISA for the rapid detection of Leptospira-specific antibodies in dogs is not IgM specific, but the study authors considered it a convenient tool to assess Leptospira antibody status in dogs. 67
Neither rapid test techniques, nor ELISA, to diagnose leptospirosis in cats have yet been developed.
PCR
PCR directly identifies leptospiral DNA. It does not determine the infecting serogroup or serovar, but it can indicate the Leptospira species. The test can be performed on blood, urine, cerebrospinal fluid and body tissues. In cases of acute leptospirosis, this would be the test of choice to perform on blood and urine in cats. Compared with culture, PCR gives fast results, contributing to an early diagnosis. 65 Real-time PCR techniques are recommended, due to their greater sensitivity and specificity. Genes that have more than one copy in the genome, such as lig or rrs, should be selected with the aim of increasing the sensitivity of the technique. Genes present only in the pathogenic species can also be added as they will increase the specificity of the test. 68
A positive PCR result means that leptospiral DNA is present in the sample. In acute infections or in chronic carriers, the test would be positive in urine, indicating that bacterial DNA is being shed. However, negative results in blood and urine do not rule out leptospirosis, as leptospiraemia is transient (only occuring in the initial phases of the disease); also results are usually negative if the cat has received antibiotic therapy,19,60 and shedding in urine can be intermittent. 3 In one report, leptospires were cultured from cat urine and the results were confirmed by PCR, 34 suggesting that cats can shed living Leptospira bacteria, not just their DNA.

Treatment
Supportive therapy
Intravenous fluids should be given to affected animals to correct the electrolyte fluid imbalance. The use of centrally acting antiemetics and the parenteral administration of gastric protectors is recommended in cats that develop associated renal failure. Pain management is particularly important in the early stages of the disease to treat painful swollen kidneys, muscle, joints and gastrointestinal tissue. 19

Enteral feeding tubes are highly recommended in cats with anorexia, until they can feed themselves in a self-sufficient manner, minimising the risk of secondary complications. 38
Antimicrobial therapy
The antimicrobial therapy suggested in cats is based on the treatment recommended for dogs. Intravenous ampicillin may be the antibiotic of choice while the patient is stabilised. Once the animal is stable, 6 weeks of doxycycline oral suspension has been suggested in order to eliminate the carrier state. 37 Monohydrate salt of doxycycline, which is less irritating to the cat’s oesophagus than hyclate or hydrochloride doxycycline salt, is marketed as tablets or suspension. Doxycycline monohydrate tablets should be administered immediately before a meal or with a treat in order to avoid secondary oesophagitis.69,70
Prevention
There is no commercial vaccine available for cats. However, one study has shown that cats can produce antibodies (of lower titre magnitude than vaccinated dogs) when experimentally inoculated with a commercial dog vaccine (containing four different serovars). 59 The follow-up time for the animals was 42 days, at which point only one animal maintained antibody levels. The authors of that study suggest further work is needed before a vaccine against Leptospira species for cats can be considered.
Given the current lack of a vaccine, the best way to avoid infection in cats is via prevention of exposure. Cats that are kept indoors have a lower risk of being infected. 37 Prevention of predation opportunities and avoidance of contact with stagnant water, urine from infected animals and dogs at risk of clinical leptospirosis is recommended.6,30,31,37 For cats that share an environment with a positively diagnosed animal, doxycycline can be given at 5 mg/kg PO q12h or at 10 mg/kg PO q24h for 2 weeks.19,60
Key Points
Cats may act as chronic reservoir hosts of Leptospira bacteria and are a possible risk factor in the transmission and maintenance of leptospirosis, the most widespread zoonosis worldwide.
Research on leptospirosis should highlight the importance that cats have in the disease maintenance cycle.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no specific financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. For any animals individually identifiable within this publication, informed consent for their use in the publication (either verbal or written) was obtained from the people involved.