
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. Ultrasound examination of the pancreas is a vital part of the investigation into feline pancreatic disease.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even for the experienced ultrasonographer, differentiating between incidental findings such as nodular hyperplasia and pathological changes such as neoplasia can be challenging.
Aim:
This review, part of an occasional series on feline abdominal ultrasonography, discusses the ultrasonographic examination and appearance of the normal and diseased pancreas. Aimed at general practitioners who wish to improve their knowledge of and confidence in feline abdominal ultrasound, this review is accompanied by high-resolution images and videos available online as supplementary material.
Equipment:
Ultrasound facilities are readily available to most practitioners, although use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Scanning the pancreas
B-mode ultrasonography is the modality of choice to image the feline pancreas and is widely available to most practitioners. It provides information regarding the size, echotexture and echogenicity of the pancreas, while permitting concurrent evaluation of the peripancreatic fat and regional lymph nodes. Aspiration of the pancreas, regional lymph nodes and suspected metastatic disease is also facilitated using ultrasound guidance. 1 Abdominal radiographs are very insensitive in the evaluation of the pancreas. Ultrasound is superior to radiography, particularly in cats in poor body condition or those that have an abdominal effusion, both of which decrease serosal detail and reduce the clinician’s ability to assess the pancreas radiographically.
The main indications for ultrasonography of the feline pancreas are suspected pancreatitis and pancreatic neoplasia; ultrasonography may also be conducted as part of an investigation into extrahepatic biliary obstruction. 2 As mentioned in previous articles in this series, the principal disadvantage of ultrasonography is that its use as a diagnostic tool is largely dependent upon clinician experience, which is very variable.
Preparation
Where possible, animals waiting for an elective examination should be fasted for 12 h prior to ultrasound. Any abdominal hair in the region to be scanned should be clipped and acoustic coupling gel applied to remove the air gap between the transducer surface and the skin. Sedation is preferable wherever possible to immobilise the patient and achieve maximum relaxation of the abdominal wall muscles. Owing to the inherently small size of the feline pancreas, the use of a high frequency (around 11–15 MHz) linear transducer is advisable to provide optimum image resolution, thereby allowing the pancreas to be assessed in detail. Readers are referred to the articles on the liver and normal gastrointestinal tract in this series (see the box on page 255) for a more detailed discussion pertaining to patient preparation and transducer choice.
Scanning technique
The pancreas can be scanned with the cat in left or right lateral, dorsal or ventral recumbency. 1 The author’s preference is to scan the left lobe while the animal is in right lateral recumbency and the right lobe with the animal in left lateral recumbency (Figure 1).


Transducer positioning for the left (a) and right (b) lobes of the pancreas
Anatomy and ultrasonographic identification of the pancreas
The pancreas is divided into two lobes that are united at the body of the pancreas, which is situated ventral to the portal vein. The close proximity of these two structures makes the portal vein an excellent landmark for the identification of the pancreatic body (Figure 2). It should be noted that the pancreatic body in the cat is much closer to the midline than in the dog, and the angle between left and right pancreatic lobes is also much smaller. 3
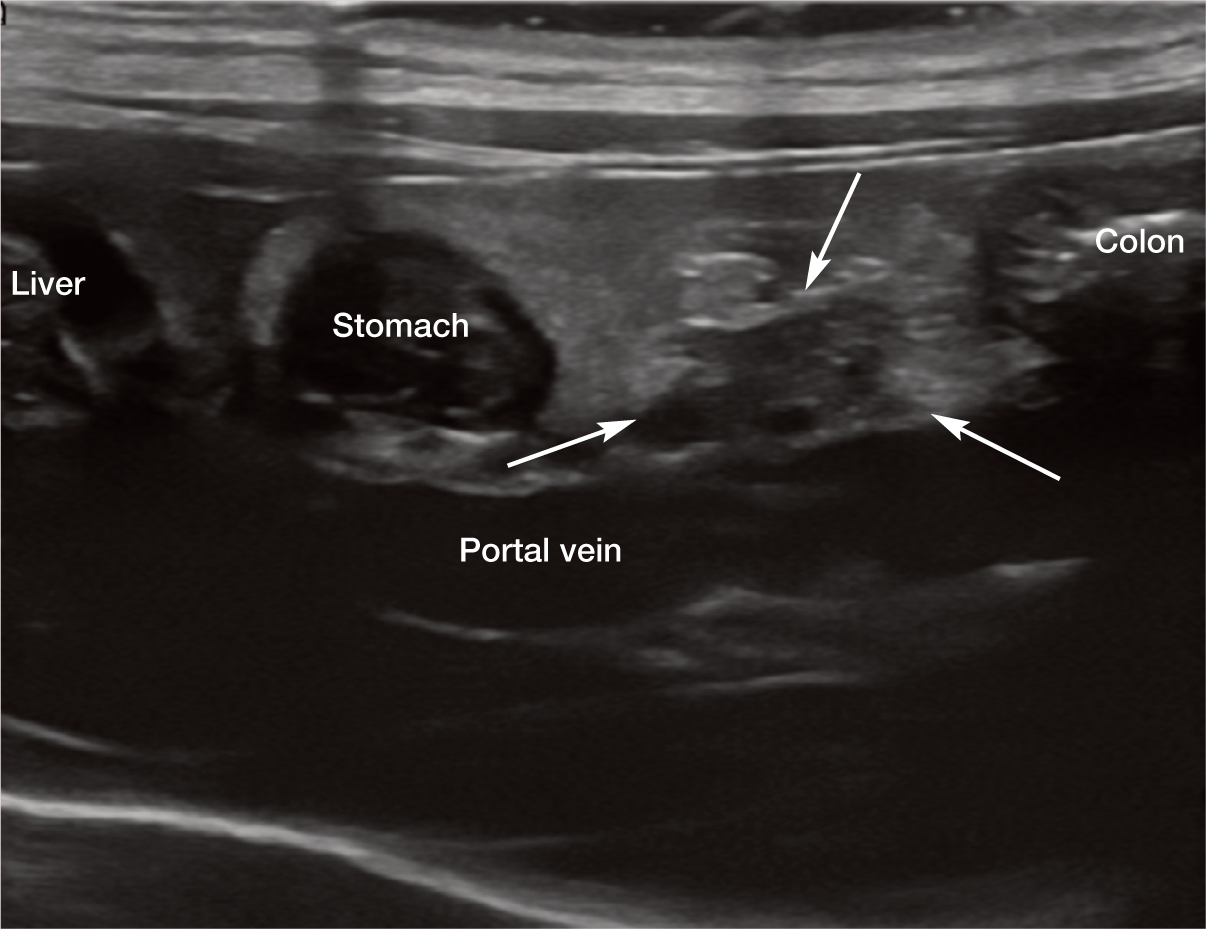
Ultrasonographic landmarks for the pancreatic body (arrows)
Recognition of adjacent landmarks is key to the successful identification of the pancreas. The left pancreatic lobe is sandwiched between the stomach cranially and the transverse colon caudally (Figure 3). The tip often extends medially to the head and body of the spleen, which acts as an acoustic window, and the splenic vein usually runs caudally and dorsally to the left pancreatic lobe. The right lobe of the pancreas is located medially or dorsomedially to the descending limb of the duodenum (Figure 4). 1 Unlike the dog, the distal portion of the right pancreatic lobe in the cat turns back on itself, creating a hook-like shape (Figure 4c). 4 The left lobe of the pancreas is larger (5–9 mm thickness) in the cat than the right lobe (3–6 mm thickness) and usually, therefore, more easily identified.5,6 This is in contrast to the dog, in which the right lobe of the pancreas is normally easier to locate with ultrasound.

Ultrasound images of the normal left pancreatic lobe (arrows) in transverse (a,b) and sagittal (c,d) planes in healthy cats. In (d) the thin-walled colon (*) is visible just caudal to the pancreas

(a,b) Ultrasound images from two cats to show the normal appearance and location of the right pancreatic lobe (arrowheads). The descending limb of the duodenum (arrow) is visible in transverse in (b). (c) The white line indicates the margins of the distal right pancreatic lobe where it forms a hook-like shape
Normal appearance of the pancreas
The feline pancreas is a well-defined organ when imaged with a good quality ultrasound machine and a high frequency transducer, although it can initially appear somewhat inconspicuous to the untrained eye. It is isoechoic to slightly hypoechoic relative to the surrounding fat and has a similar echogenicity to the liver.1,6,7
Most dogs have two larger pancreatic ducts into which the smaller ducts that link the pancreatic acini drain. 8 In contrast, there is usually just one pancreatic duct in the cat, known as the major pancreatic duct. This duct is consistently visible on ultrasound as an anechoic tubular structure, flanked by thin hyperechoic walls, running within the central portion of the left lobe from the tip towards the body (Figure 5).1,9 It can be differentiated from a blood vessel by the absence of flow signal when interrogated with colour Doppler. This is because flow within a pancreatic duct is considerably slower than blood flow and, as such, does not generate a Doppler signal.
Ultrasound image of the normal major pancreatic duct (arrows) within the left lobe of the pancreas of a 6-year-old male neutered domestic longhair cat. A video showing the normal pancreatic duct within the left lobe of the pancreas is available as supplementary material
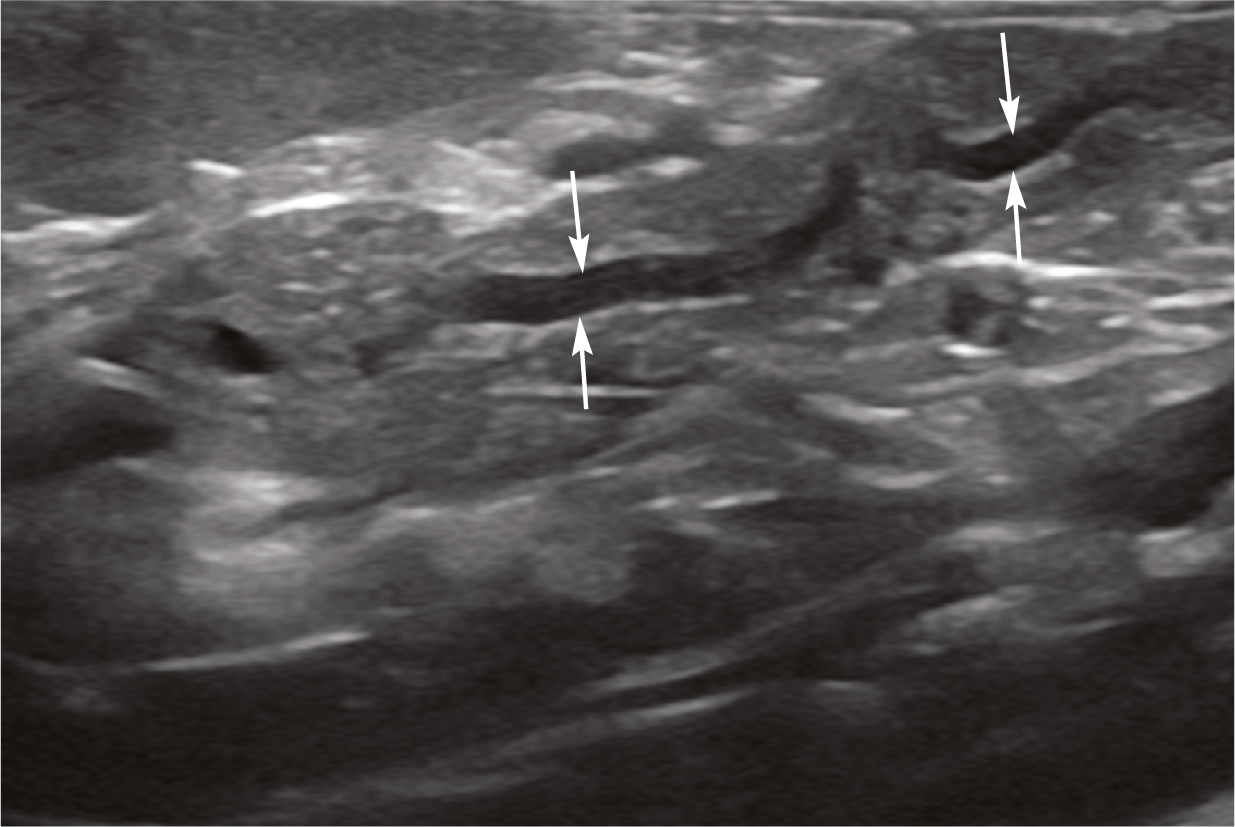
The diameter of the major pancreatic duct has been reported in 20 healthy cats <10 years of age. In these cats, the mean diameter was determined to be 0.8 ± 0.25 mm (range 0.5–1.3 mm). 7 In a separate study involving a group of cats >10 years of age, the mean diameter of the pancreatic duct was recorded as 1.3 ± 0.4 mm (range 0.6–2.4 mm). 5 Dilation of the duct up to 2.5 mm diameter has been shown to occur as an incidental ageing change in older cats with no signs of pancreatic disease (Figure 6).5–7 A satisfactory explanation for this phenomenon has yet to be found. One suggested hypothesis for the same change in humans is that widening of the pancreatic duct with age occurs as a result of atrophy of the pancreas.5,10

(a) Mild dilation of the pancreatic duct (arrows) within the left pancreatic lobe of an 11-year-old male neutered domestic shorthair cat. This was presumed to be an incidental age-related change. (b) Note the absence of colour within the pancreatic duct when a colour Doppler window is applied over the pancreas
The major pancreatic duct merges with the common bile duct at the ampulla of Vater immediately prior to its entry into the duodenum at the major duodenal papilla. 11 The major duodenal papilla is located along the dorsal wall of the duodenum, approximately 3 cm distal to the pylorus (Figure 7). 12 In a minority of cats, the major pancreatic duct and common bile duct open into the duodenum separately, but immediately adjacent to each other. 13 In around 20% of cats, a second minor or accessory duct is present that drains into the duodenum via the minor duodenal papilla, which is located approximately 2 cm distal to the major duodenal papilla. 12

Ultrasound image of a normal duodenal papilla (arrows). A video showing the pancreatic and common bile ducts fusing before entering the duodenal papilla is available as supplementary material
Lymphatic drainage from the pancreas is supplied by the pancreaticoduodenal, jejunal, hepatic and splenic lymph nodes. Each node also supplies other organs and hence abnormalities of these lymph nodes are not necessarily indicative of pancreatic disease.
Abnormalities of the pancreas
Pancreatitis
Pancreatitis is the most commonly diagnosed disorder of the feline exocrine pancreas 14 and yet, despite this, an underlying cause is not identified in the majority of cases and the condition is often considered to be idiopathic.15–17 Cats of all ages may be affected, with reports in animals from 3 weeks to 20 years.16,18 While any breed may be affected, Siamese are thought to be over-represented. 18 The left lobe and body are usually more commonly affected by inflammation, in contrast to the situation in dogs in which the right lobe is more commonly affected, although any portion may be affected in either species. 3
The clinical signs and results of clinico-pathological tests in cats with pancreatitis are often vague and non-specific, making the diagnosis challenging. 19 Furthermore, since the disease can affect the pancreas multifocally, histopathology may fail to detect evidence of inflammation in biopsy specimens. 15 Fortunately, the clinician’s ability to detect pancreatitis has improved over the years, thanks to the development of a feline-specific pancreatic lipase assay. One potential drawback of this assay, however, is that it may be less well suited to the diagnosis of mild and chronic forms of the disease. 15 Consequently, diagnostic imaging still has an important role to play in the diagnosis of pancreatitis. Anticipated radiographic changes include a mass effect in the region of the pancreas, loss of serosal detail due to peripancreatic effusion and the presence of dilated bowel loops due to ileus.20–23 Nevertheless, in spite of these potential abnormalities, abdominal radiography is neither sensitive nor specific for feline pancreatitis. Ultrasound, on the other hand, provides much more comprehensive information relating to the health of the pancreas and surrounding tissue, and is recommended in cats with suspected pancreatitis.
The sensitivity of ultrasound for the detection of pancreatitis in the cat has traditionally been regarded as relatively low, with three studies between 2000 and 2002 reporting values of 11%, 24% and 35%.22,24,25 In 2004, a further study reported a much higher sensitivity of 80% for cats with moderate to severe pancreatitis and 62% for those with mild pancreatitis. 26 Two potential explanations were offered by the authors for this dramatic difference in sensitivity relative to the earlier studies. The first was an inherent bias towards a diagnosis of pancreatitis such that the radiologist, being aware of the nature of the study, would have evaluated the pancreas more extensively than in previous ultrasound studies, which were of a retrospective nature. In these earlier studies, the pancreas was evaluated during a routine ultrasound examination and hence was not the focus of the study. Secondly, there have been, and continue to be, significant advances in ultrasound technology and markedly improved radiologist skill levels that are likely to contribute to greater sensitivity levels. 26 Interestingly, an even higher sensitivity of 84% and a specificity of 75% for diagnosing pancreatitis were reported in a much more recent study. 27 However, in this study elevated serum feline pancreatic lipase immunoreactivity (fPLI) was used as the standard for diagnosis of pancreatitis, which has been shown to have only fair agreement with ultrasonography in cats with a suspicion of pancreatitis. 28 Of the 35 cats included in the study, only six cats had histopathological evaluation of the pancreas; 27 therefore, this figure for sensitivity should be interpreted with caution. It should also be noted that all of these studies were conducted at university teaching hospitals and most ultrasound examinations would have been performed by board-certified radiologists using high-end equipment. Hence, it is reasonable to assume that sensitivity is liable to be reduced when scans are performed by clinicians less experienced in ultrasound using lower quality equipment. 14
Concurrent inflammatory bowel disease, cholangitis/cholangiohepatitis and hepatic lipidosis have been reported in 50–56% of cats diagnosed with pancreatitis.24,26,29,30 In a study of 23 cats with inflammatory bowel disease, 16 cats had elevated serum fPLI concentrations (>6.9 μg/l). 31 Therefore, due to the link between pancreatitis and intestinal tract and hepatic disease, the liver and gastrointestinal tract should be evaluated ultrasonographically at the same time as the pancreas.
Acute pancreatitis
In contrast to the situation in dogs, chronic pancreatitis has traditionally been considered to be more common than acute necrotic pancreatitis in the cat, although both may be relatively under-diagnosed.3,15,23,32,33 Several studies have, however, resulted in increased recognition of the acute form of the disease in this species.18,24,34,35 Acute pancreatitis can be mild, moderate or severe and affect the pancreas focally, or as a multifocal or diffuse disease. When ultrasonographic abnormalities suggestive of acute pancreatitis are identified, they are often more subtle than those seen in the dog; furthermore, and in the light of the sensitivities discussed above,3,24 the absence of changes on ultrasound is not sufficient to rule out the possibility of pancreatitis. In those cases where the ultrasonographic appearance of the pancreas is unremarkable but the clinical suspicion of pancreatitis remains high, ultrasound can be repeated after 2–4 days, which may allow sufficient time for ultrasonographic changes to appear. 36
The ultrasonographic features of acute pancreatitis in cats are reasonably specific and mirror those described in dogs. Typical abnormalities include enlargement of the pancreas (which if sufficiently substantial can result in a mass effect), a reduction in echogenicity of pancreatic tissue (owing to necrosis and/or oedema), severely irregular pancreatic margins, hyperechogenicity and hyperattenuation of peripancreatic mesenteric fat (due to saponification following the release of pancreatic enzymes) and localised peritoneal effusion (Figure 8).20,25,27,29,35 When inflammation of peripancreatic fat is severe, it can become hazy in appearance and pancreatic margins may appear ill-defined.
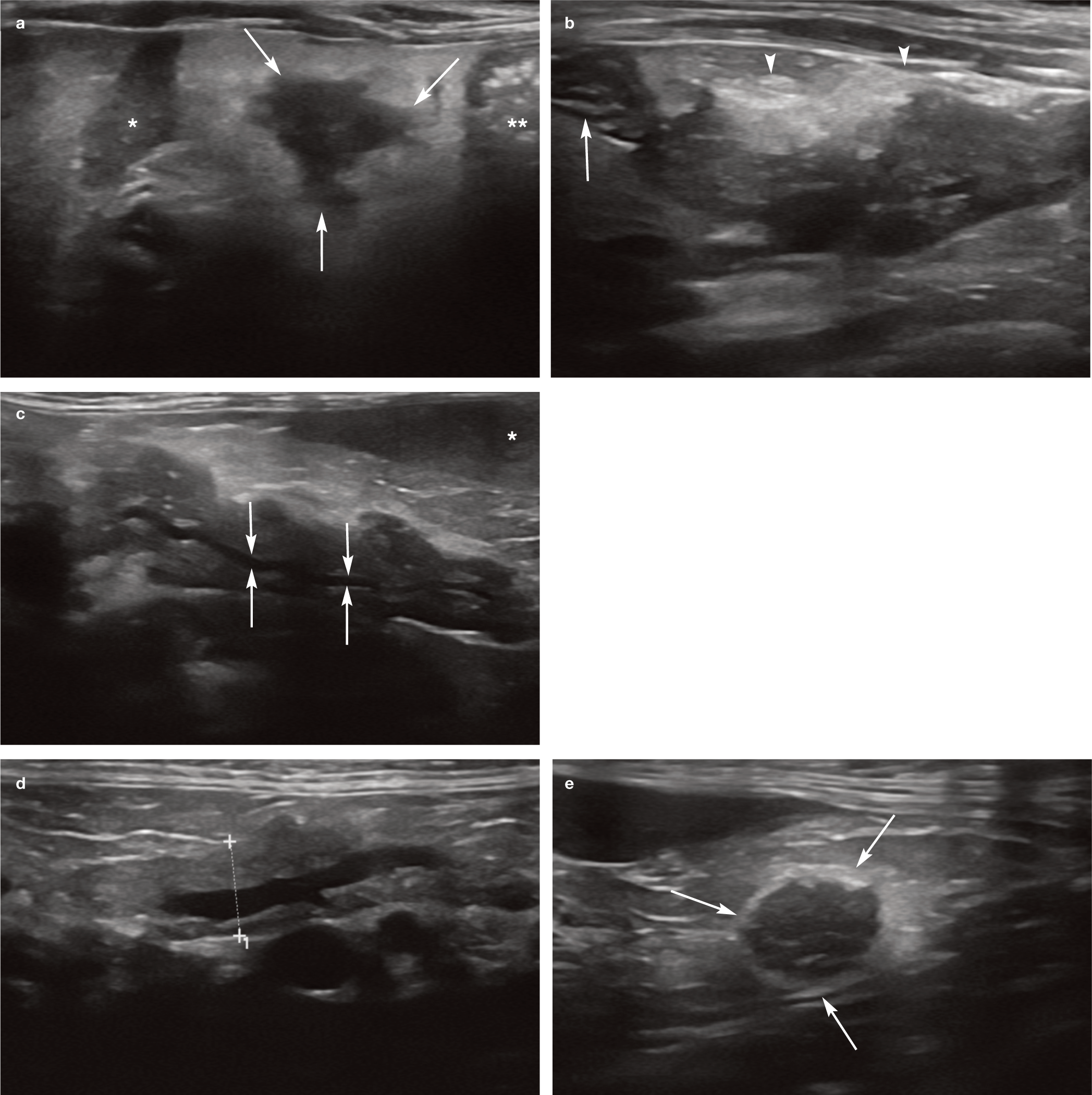
Acute pancreatitis. (a) Left lobe of the pancreas (transverse plane) of a 14-year-old female neutered Birman presenting with a 10-day history of lethargy and inappetence, and severe weight loss over a longer period of time. The pancreas (arrows) is enlarged and hypoechoic and surrounded by markedly hyperechoic peripancreatic fat. The spleen (*) is to the left of the pancreas and the transverse colon (**) is to the right. (b) The right pancreatic lobe in the same cat is also affected. Note the hyperechoic fat (arrowheads) adjacent to the pancreas. The duodenum (arrow) is seen in the transverse plane to the left of the pancreas. Videos showing the left and right pancreatic lobes in this cat are available in the supplementary material. (c) Pancreatitis affecting the left lobe of the pancreas (longitudinal plane) of a 4-year-old female neutered domestic shorthair cat referred for further investigation of icterus that had developed following a period of reduced appetite and weight loss. The pancreas is diffusely hypoechoic and surrounded by hyperechoic fat. The anechoic tubular structure (arrows) running through the centre of the left lobe is the pancreatic duct. The spleen (*) is visible in the top right of the image. (d,e) Pancreatic changes affecting the caudal tip of the left pancreatic lobe of an 11-year-old female neutered domestic shorthair cat presenting with a recent history of weight loss and inappetence. (d) The left lobe (being measured between the calipers) is predominantly normal in appearance, although the pancreatic duct is mildly dilated. (e) In contrast, the caudal tip (arrows) is enlarged, hypoechoic and irregularly marginated and surrounded by hyperechoic fat
Hyperechoic peripancreatic fat may be one of the most sensitive indicators of pancreatitis; it was identified in 68% of cats (n = 35) that had concurrently elevated serum fPLI in one study 27 and was the most frequently identified ultrasonographic abnormality in 55% of cats with raised fPLI in another study. 37 Accordingly, this would suggest that there is a moderate probability of cats with pancreatitis having this abnormality on ultrasonographic examination, although it is important to note that the authors of these studies do not differentiate between cats with acute and chronic pancreatitis.27,37 The authors of the earlier of these two studies report that, in addition to hyperechoic pancreatic fat, the presence of a thick left pancreatic limb and severely irregular pancreatic margins in cats with appropriate clinical signs and raised serum fPLI concentrations is highly supportive of pancreatitis. 27
Pancreatic oedema results in pancreatic enlargement and fluid accumulation within the interlobular septae. This gives rise to multiple hypoechoic striations dispersed throughout the parenchyma – the so-called ‘tiger stripe’ appearance. 38 Although this finding is reported specifically in dogs, the author has also observed this change in cats (Figure 9). It can be seen in cases of pancreatitis but can also occur as a result of portal hypertension and hypoalbuminaemia and hence is not considered to be pathognomonic for inflammation. 38
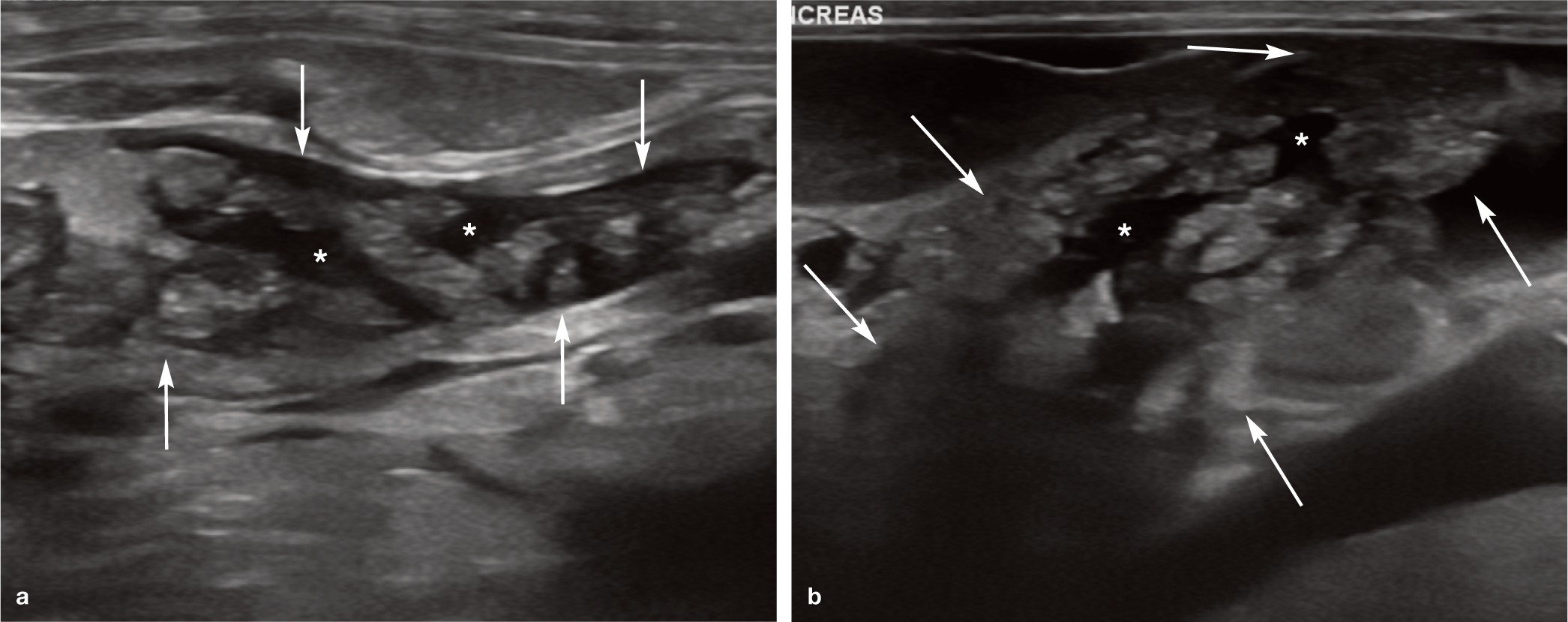
Pancreatic oedema in two cats. (a) Ultrasound image from a 5-year-old female neutered domestic shorthair cat presenting for further investigation of acute renal failure. Pleural and peritoneal effusion developed as a result of poor urine output. The pancreas is enlarged (arrows) and multiple anechoic striations (asterisks) dissect between pancreatic lobules giving rise to a ‘tiger stripe’ appearance, indicative of pancreatic oedema. (b) Ultrasound image from a 4-year-old male neutered domestic shorthair cat presenting with marked hypoalbuminaemia, ascites and peripheral oedema secondary to protein-losing nephropathy. The arrows indicate the margins of the pancreas, and the asterisks indicate the anechoic striations within the pancreas. Videos showing pancreatic oedema, including in a cat with severe hypoalbuminaemia, are available in the supplementary material
Dilation of the biliary tree owing to compression of the common bile duct by an inflamed pancreas and mesenteric lymphadenopathy are further changes that have also been reported in association with pancreatitis.11,22,39,40 On ultrasound, the normal common bile duct should measure no greater than 4 mm in diameter, whereas a diameter >5 mm is suggestive of extra-hepatic biliary obstruction (EHBO). 11 It should, of course, be remembered that there are several other differentials for EHBO aside from pancreatitis, such as cholelithiasis. 11 The ultrasonographic appearance of EHBO was discussed in more detail in the article on the biliary tree in this series (see box on page 255).
Further changes that may be appreciated on ultrasound in cats with acute pancreatitis include thickening and/or altered layering of the gastric or duodenal wall and a mildly dilated, hypomotile descending duodenum, possibly with concurrent corrugation (due to paralytic ileus).1,25,41 In some cats, these may be the only abnormalities present.
Chronic pancreatitis
Recurrent episodes of inflammation over months or years can lead to the development of chronic pancreatitis. Whereas acute pancreatitis is typically associated with neutrophilic inflammation, necrosis and oedema, chronic pancreatitis leads to irreversible acinar loss and fibrosis, 9 and resembles the process seen in humans where fibrosis is more pronounced than inflammation. 32 The condition is often mild and asymptomatic and has a high prevalence in apparently healthy cats, causing some to question its clinical significance. 15 Histological evidence of chronic pancreatitis was identified in 67/115 cats undergoing necropsy in one study; in comparison, 18 cats showed histological evidence of acute pancreatitis. 32 Despite this, there is relatively little in the literature regarding the ultrasonographic appearance of feline chronic pancreatitis.
As for acute pancreatitis, a normal ultrasound examination does not exclude the possibility of chronic pancreatitis, since the disease processes present may be insufficient to induce an alteration in the appearance of the pancreas on ultrasound. 14 Similarly, the ultrasonographic changes observed have a tendency to be somewhat variable between individuals, thus complicating the diagnosis further. 1 In the dog, reported abnormalities include an increase or decrease in the size of the pancreas, increased (possibly due to fibrosis), decreased or mixed echogenicity of the pancreatic parenchyma and normal or mildly hyperechoic peripancreatic mesentery, although any increases in mesenteric echogenicity are usually less pronounced than those seen with acute pancreatitis.1,42–44
Abnormal pancreatic thickness, an irregular pancreatic margin, nodularity and hypo-echogenicity of the pancreas, hyperechoic mesentery and abdominal effusion have all been reported in cats with chronic pancreatitis confirmed by histopathology (Figure 10).5,20,27 Thus, it appears that there is a degree of overlap in the ultrasonographic appearance of acute and chronic pancreatitis in the cat. Fibrosis and calcification of the pancreas as a result of chronic pancreatitis can lead to the presence of shadowing hyperechoic foci. As with acute pancreatitis, dilation of the common bile duct may also be recognised and, if adhesions form secondarily to chronic inflammation, the duodenum and/or part of the stomach can become displaced from their normal position within the abdomen. 1

(a,b) Chronic pancreatitis in a 5-year-old male neutered domestic shorthair cat presenting with a history of lethargy, inappetence and occasional vomiting of 1 week’s duration. The left lobe of the pancreas (arrows) is enlarged, diffusely hypoechoic and surrounded by abnormally hyperechoic fat suggestive of a localised steatitis. Exploratory coeliotomy was performed to acquire biopsies of the liver, small intestine and pancreas. Final diagnoses based on histopathology were cholangiohepatitis, inflammatory bowel disease and marked chronic pancreatitis with accompanying fibrosis and nodular regeneration. A video showing chronic pancreatitis affecting the left lobe of the pancreas in the same cat with triaditis is available in the supplementary material
In humans with chronic pancreatitis, irregular widening of the pancreatic ducts has been reported and is believed to be due to periductal fibrosis. 10 Dilation of the pancreatic duct has also been reported in cats with chronic pancreatitis by the authors of one study. 45
However, a further separate study found no correlation between pancreatic duct width and clinically significant pancreatic disease. 5 Furthermore, since dilation of the pancreatic duct can occur as a normal ageing change, it should not be used as the sole indicator of pancreatitis in the geriatric cat.
As with most diagnostic tests, ultrasound has its limitations. As mentioned above, results suggest that it may not be possible to distinguish between acute necrotising and chronic non-suppurative pancreatitis with ultrasound, even when the history, physical examination findings, results of clinicopathological testing and any radiographic abnormalities present are taken into account. 20 Furthermore, the authors of a recent retrospective study of 42 cats presenting with at least two clinical signs of pancreatitis and raised fPLI values were unable to identify any significant correlation between ultrasonographic changes and outcome; 37 thus the use of ultrasound for prognostic purposes appears limited.
In view of the fact that the ultrasonographic diagnosis of chronic pancreatitis is not always straightforward, attempts have been made to discover alternative means of obtaining a more definitive diagnosis using ultrasound in combination with a hormone called secretin. In healthy individuals, secretin stimulates the pancreas to secrete bicarbonate, resulting in dilation of the pancreatic duct, which is identifiable ultrasonographically.46,47 It has been shown that in humans with chronic pancreatitis, the duct fails to dilate and it is thought that this occurs as a result of periductal fibrosis.47,48 To investigate the potential use of this hormone as a diagnostic tool for chronic pancreatitis in cats, the effect of exogenous administration of secretin on the diameter of the pancreatic duct in healthy cats was recorded. 49 Mean pancreatic duct diameter increased from 0.77 ± 0.33 mm to 1.42 ± 0.40 mm following secretin administration and the mean percentage increase in pancreatic duct diameter over basal diameter up to 15 mins after secretin administration was 101.9 ± 58.8%. 49 To date, the relationship between secretin administration and ductal diameter in the diseased feline pancreas has not been evaluated and, therefore, the ability of this diagnostic procedure to identify cats with chronic pancreatitis has yet to be determined.

Exocrine pancreatic insufficiency
Chronic pancreatitis is the most common cause of exocrine pancreatic insufficiency (EPI), a condition seen only rarely in the cat.36,50 Pancreatic nodularity and inhomo-geneity have been reported in two cats with EPI based on feline trypsin-like immunoreactivity assay results. 5 Hyperechogenicity and a reduced volume of the pancreatic parenchyma, in association with dilation of the pancreatic duct with or without pancreatic calculi, have also been reported with this condition. 3 Hypermotility and distension of the intestinal tract may be observed concurrently due to EPI-related malabsorption. 3
Cystic pancreatic abnormalities
Cystic pancreatic abnormalities include pancreatic cysts and pseudocysts, abscesses and pancreatic bladder. Neoplasia is discussed in a separate section below, alongside nodular hyperplasia.
Pancreatic cysts
Pancreatic cysts are occasionally identified in cats 1 and can be classified as true cysts, pseudocysts or retention cysts. True cysts have an epithelial lining, do not communicate with the pancreatic duct and are usually incidental.51,52 To date, they have only been reported in a handful of cases.53–55 A peduncu-lated true cyst attached to the body of the pancreas, which was presumed to be congenital in origin, has been reported in a 5-year-old cat. 53 On ultrasound examination, the cyst was 3.91 cm in length, multilocular and had a thick wall with anechoic contents and occasional septations. Histopathological examination of the cyst confirmed the presence of a lining comprising a single layer of cuboidal to columnar epithelial cells. 53 Multiple recurrent true pancreatic cysts of unknown aetiology, associated with pancreatic inflammation, atrophy and diabetes mellitus, have also been reported in a 14-year-old domestic shorthair cat. 54 Similar ultrasonographic findings are described in the most recent report: a well-defined multilobulated cystic structure located craniomedial to the left kidney was described on ultrasound in a 15-year-old female neutered domestic shorthair cat. At laparoscopy, a 7 cm diameter cyst was confirmed originating from the left pancreatic limb and subsequently omentalised. 55
Pseudocysts form as a result of pancreatitis and pancreatic duct rupture. They have a non-epithelialised fibrous capsule and are filled with fluid rich in pancreatic enzymes and debris.56,57 It is postulated that focal pancreatic necrosis and pancreatic duct rupture occur as a result of pancreatitis. Pancreatic juices leak into the area of necrotic tissue and an inflammatory exudate forms, eventually becoming enclosed within a fibrous connective tissue capsule. The term ‘pseudocyst’ is appropriate because they lack a true epithelial lining. Identification of a pancreatic cystic lesion in a patient with a clinical history of pancreatitis should raise the suspicion of a pseudocyst. 58
There are occasional descriptions in the veterinary literature detailing the ultrasono-graphic appearance of pancreatic pseudocysts in cats.59,60 The wall of a pseudocyst is typically much thicker and more irregular than that of a true cyst and the lumen may be septated and contain internal echoes.59,61 An accompanying distal acoustic enhancement artefact is often present owing to the fluid component of the cyst. Complications arising from larger pseudocysts, such as compression of the common bile duct causing EHBO, have been reported in humans. 62 Furthermore, pseudo-cysts that become infected may form abscesses and ruptured pseudocyts in humans have been reported to cause severe peritonitis. 63 Spontaneous regression of human pancreatic pseudocysts has also been reported. 64
Aspiration of luminal contents from a pseudocyst under ultrasound guidance is considered to be a safe procedure and will typically reveal high levels of amylase and/or lipase.59,65 This can be invaluable in helping to differentiate pseudocysts from abscesses and cystic neoplasms, all of which can appear similar ultrasonographically.59,65
The third type of cyst described in the pancreas, the retention cyst, forms due to the blockage of a pancreatic duct followed by the accumulation of glandular secretions. In humans, retention cysts are reported to be incidental findings and have no clinical significance. 58 They are usually small and have an epithelial lining and are more likely to contain anechoic rather than echogenic fluid, in contrast to inflammatory pseudocysts.1,58 To the author’s knowledge, retention cysts associated with the pancreas have not been reported in the cat.
Cats with polycystic kidney disease develop numerous cysts throughout the kidneys but can also develop cysts concurrently within the liver and pancreas (Figure 11). 66 Consequently, it is prudent to scan both the liver and pancreas in cats presenting with this condition.
Ultrasound images from a 14-year-old male neutered Persian cat with polycystic kidney disease. (a) Large (approximately 8 cm diameter) thin-walled cyst containing mildly echogenic fluid associated with the pancreas. (b) Multiple, variably sized, smaller cysts are visible throughout the entire pancreas (arrows). Concurrent cysts were also present throughout both kidneys and the liver (not shown)
Pancreatic abscessation
Pancreatic abscesses are uncommon in cats but may develop as a consequence of pancreatitis or an infected pseudocyst. 67 Pancreatic abscessation has also been identified in a cat with diabetes mellitus. 68 Abscesses can be highly variable in appearance but usually present as thick-walled cavitary lesions with hyper-echoic or flocculent contents (Figure 12).67,68 Occasionally gas is also present and recognised on ultrasound by the presence of hyperechoic foci associated with a reverberation artefact. 1

Pancreatic abscessation in two cats. (a,b) Ultrasound images from an 11-year-old male neutered Norwegian Forest Cat presenting for investigation of weight loss. Abdominal ultrasound revealed the presence of multiple, variably sized cavitary lesions throughout the pancreas. Most lesions had a thick wall and contained gravity-dependent sediment (arrows). Hyperechoic fat is also visible adjacent to the lesions. Aspiration of the fluid from the largest of these yielded a non-septic, neutrophilic exudate consistent with abscessation. (c) Ultrasound image from an 8-year-old female neutered diabetic Bengal cat. Multiple thick-walled cavitary lesions (arrows) are present within the right lobe of the pancreas. Lesion contents varied from anechoic to echogenic. Note the marked hyperechogenicity of the peripancreatic fat, reflecting adjacent steatitis. Lesion aspiration was consistent with abscessation. Three videos showing pancreatic abscessation are available in the supplementary material
Pancreatic bladder
A pancreatic bladder refers to cystic dilation of the pancreatic duct, a rare condition in the cat.50,69,70 Some prefer the term pancreatic pseudobladder since there is no true bladder associated with the pancreas, unlike the urinary and biliary systems. 1 On ultrasound, pancreatic bladders are fluid-filled structures associated with the pancreas that can be confused with a bipartite gall bladder or a pancreatic cyst.69,70 Identifying a connection between the cystic structure and the ductal system of the pancreas confirms the true nature of the lesion. 70 While they may be incidental, they can reach a size sufficient to obstruct the common bile duct, thereby causing icterus. 69 The presence of marked saccular dilation of the pancreatic duct in the absence of an obstructive process has also been described in cats. 3 Concurrent thickening of the pancreatic duct wall and the presence of anechoic to echo-genic fluid within the duct lumen were additional findings reported in these cases. 3 The cause of the severe ductal distension could not be determined.
Pancreatic bladder has also been reported in association with pancreaticolithiasis. The latter is a rare condition that describes the presence of one or more calculi within the ductal system or parenchyma of the pancreas. Calculi are usually easily recognised by their characteristic strongly hyperechoic interface and distal acoustic shadowing (Figure 13). Obstruction of the pancreatic duct by a stone (pancreatolith) has been reported in a 14-year-old Maine Coon with chronic pancreatitis. 70 It was thought that the obstruction of the duct resulted in pancreatic duct dilation and subsequent pancreatitis. In the same cat an anomalous cystic structure containing calculi that communicated with the pancreatic ductal system was also identified and found to represent a pancreatic pseudobladder following exploratory surgery. Migration of a calculus from the pseudobladder into the pancreatic duct was considered to be the most likely explanation for the pancreaticolithiasis. 70

Pancreaticolithiasis in an 8-year-old female neutered domestic shorthair cat. (a) Two calculi (arrows) are visible within the dilated pancreatic duct of the left lobe. (b) Marked dilation of the pancreatic duct within the right lobe (arrows) in association with further calculi (arrowheads)
Nodular hyperplasia and pancreatic neoplasia
Nodular hyperplasia of the pancreas is a common incidental finding in older cats. 71 The ultrasonographic appearance of nodular hyper-plasia in five cats has been described as multiple hypoechoic nodules within the pancreas varying in size from 3 mm to 10 mm in diameter. 72 Small pancreatic cysts have the potential to appear similar on ultrasound, although a distal acoustic enhancement artefact is expected with cysts due to their fluid content, thus allowing them to be distinguished from solid nodules. 3
Exocrine pancreatic neoplasia, of which adenocarcinoma is the most frequently encountered type, is rare in the cat, particularly when compared with pancreatitis, with incidences of 0.013% and 0.05% being reported in large cohorts of cats.73,74 Pancreatic adenocarcinoma usually affects older cats; in two studies comprising a total of 48 cats with malignant pancreatic tumours, the approximate mean age was 12 years.72,75 Any part of the pancreas may be affected 75 and cases of pancreatic adenocarcinoma have been reported in association with paraneo-plastic alopecia.76–78 On ultrasound examination, pancreatic neoplasia typically presents as a hypoechoic nodule or mass in the region of the pancreas, although diffuse infiltration or even a normal-appearing pancreas is also possible (Figure 14).1,72,75,79 Solitary masses exceeding 2 cm diameter in at least one dimension are reported to be more likely to be neoplastic. 72 The presence of multiple pancreatic nodules measuring 1.5 cm to 6 cm in diameter has also been reported in cats with pancreatic adenocarcinoma. 75 Although hyperplastic nodules tend to be smaller than this, there is still considerable overlap in the ultrasonographic appearance of both conditions and hence cytology and/or histopathology remains necessary for definitive differentiation.

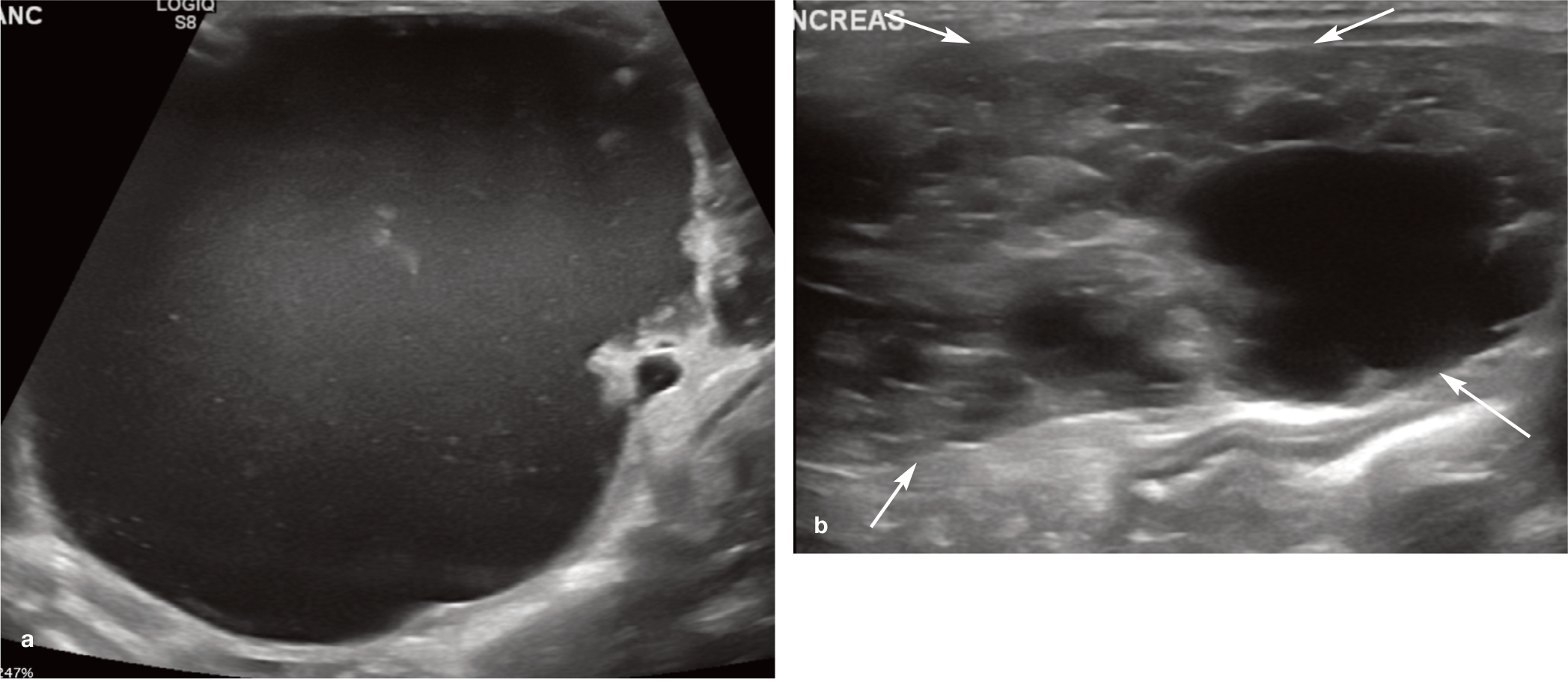
Pancreatic adenocarcinoma in three cats. (a) Ultrasound image of the pancreas of a 10-year-old male neutered domestic shorthair cat presenting with a 2-month history of progressive lethargy, intermittent diarrhoea and, more recently, vomiting. The pancreas is moderately and diffusely enlarged up to 2.4 cm in thickness, with a mass in the right lobe (arrows). Pancreatic borders are irregular and the parenchyma is heterogeneous throughout. Cytology from ultrasound-guided fine-needle aspiration (FNA) was most consistent with pancreatic adenocarcinoma. (b) A 1.5 cm x 2.5 cm mixed echogenicity mass (arrows) within the right lobe of the pancreas of an 8-year-old male neutered domestic shorthair cat presenting for further investigation of inappetence and weight loss. Histopathology results were consistent with tubular adenocarcinoma of the exocrine pancreas and concurrent nodular hyperplasia. (c) Ultrasound image of a poorly circumscribed hypoechoic mass (arrowheads) associated with the left lobe of the pancreas in a 14-year-old British Shorthair presenting with lethargy, inappetence and ascites. The spleen is visible in the near field of the image. Multiple poorly defined hypoechoic nodules (arrows) are visible throughout the hyperechoic mesentery and a moderate volume of slightly echogenic peritoneal fluid is also present. FNA results were consistent with pancreatic adenocarcinoma and widespread carcinomatosis
Ancillary findings in cases of pancreatic neoplasia include evidence of pancreatic mineralisation, 72 invasion of the duodenal wall, free abdominal fluid, hyperechogenicity of peripancreatic fat, lymphadenopathy and obstruction of the common bile duct.72,75 The presence or absence of abdominal effusion can also be used as a prognostic indicator. In one report of 34 cats with pancreatic adeno-carcinoma, the median survival of those cats with abdominal effusion at diagnosis (16 in total) was 30 days compared with 165 days for cats with no effusion. 79 Unfortunately, feline pancreatic adenocarcinoma has a poor prognosis and has often metastasised by the time of diagnosis, particularly to the liver, lung and small intestine.73,75
Lymphoma of the pancreas is also recognised in the cat but may represent pancreatic involvement in multicentric disease rather than a primary tumour of the pancreas. 72 It has been reported to result in irregular margination, diffuse enlargement and hypo-echogenicity of the pancreas (Figure 15). 3
Pancreatic adenomas have likewise been described in the cat and can present as smoothly defined nodules with an echogenicity similar to that of adjacent pancreatic tissue.3,73 However, the concurrent ancillary changes described above, including lymphadenopathy, would not usually be expected.

(a,b) Pancreatic lymphoma in a 16-year-old male neutered domestic shorthair cat referred for assessment of an abdominal mass. The pancreas is markedly enlarged and contains multiple well-circumscribed hypoechoic masses throughout. Fat surrounding the pancreas is mildly hyperechoic. Concurrent hepatosplenomegaly and a gastric mass were noted at the time of abdominal ultrasound in addition to marked enlargement of hepatic, gastric and jejunal lymph nodes
Neoplasia of the endocrine pancreas
Neoplasia of the endocrine pancreas is extremely rare in the cat and, as a result, descriptions of the ultrasonographic findings are scarce. An insulinoma has been described in a 15-year-old female neutered domestic shorthair cat in which it presented as a 9 mm diameter, mildly hyperechoic, spherical nodule within the left pancreatic lobe. 80 The tumour was considered to be a benign islet cell adenoma based on well-differentiated cell morphology and lack of invasive growth. 80 Another report documents the presence of a 1 cm diameter nodule in the body of the pancreas of a 17-year-old male neutered Siamese cat, confirmed to be an islet cell carcinoma following histopathology. 81 In this cat, metas-tases were identified in the liver and regional lymph nodes. 81 The ultrasonographic findings from both of these reports in cats are similar to those in dogs; canine endocrine pancreatic tumours are also typically small nodules (usually <2.5 cm diameter) that can be challenging to detect on ultrasound.1,82 These descriptions are further supported by the most recent report of insulinoma, in a 14-year-old male neutered domestic shorthair cat, which describes the presence of a focal, well-defined hypoechoic pancreatic mass measuring 16 mm x 23 mm diameter. 83
Metastatic neoplasia
There are only occasional reports of metastatic disease occurring within the pancreas in cats. Pancreatic metastases were identified in 2/26 cats with visceral haemangiosarcoma in one study, 84 and in an 11-year-old cat secondarily to a prostatic adenocarcinoma, 85 although the specific ultrasonographic features were not described.
Rupture of the pancreas
Pancreatic rupture is a very rare event that has been documented in cats with high-rise syndrome. 86 Leakage of pancreatic enzymes into the abdominal cavity ensues, resulting in pancreatic autodigestion and saponification of adjacent fat. Without the correct diagnosis and treatment, the condition can lead to multi-organ failure and death. On ultrasound, the pancreas in four affected cats appeared hyper-echoic and was surrounded by hyperechoic peripancreatic mesenteric fat. 86 Additional findings in all affected cats included ascites and hypomotility of the gastrointestinal tract. It is thought that the left pancreatic lobe may be particularly vulnerable to rupture and, in the four cases described, the diagnosis of pancreatic rupture was confirmed either at surgery or at post-mortem examination.
Traumatic pancreatitis has also been reported in association with high-rise syndrome. 87 Abdominal ultrasonography of affected cats may reveal any combination of pancreatic enlargement, decreased or heterogeneous pancreatic echogenicity, hyperechoic mesentery and peritoneal effusion. 87
Contrast-enhanced Doppler ultrasound
Contrast-enhanced Doppler techniques have been used in the human field to differentiate between pancreatitis and neoplasia, to detect parenchymal necrosis in individuals with acute severe pancreatitis and to assess pancreatic tumours.88–90 Accordingly, the feasibility of using contrast-enhanced Doppler ultrasound to evaluate the feline pancreas has also been investigated.91,92 The perfusion pattern of
the normal pancreatic parenchyma has been described in detail in 10 clinically healthy cats using a second-generation contrast medium containing sulfur hexafluoride (SonoVue; Bracco UK). 92 Additionally, significantly higher pancreatic blood volumes and vascularity are present in cats with pancreatic disease compared with normal cats, regardless of the Doppler method used (ie, pre-contrast vs post-contrast, colour vs power Doppler). 91 As expected, power Doppler yields higher Doppler values than colour Doppler and is thus superior. Contrast-enhanced ultrasonography has also been used in the diagnosis of pancreatic insulinoma in a cat. 83 Further research is required to determine whether this technique can be used in cats that are suspected of having pancreatic pathology but have normal B-mode scans, and to determine the accuracy of Doppler with regard to differentiating the various disorders of the pancreas.


Key Points
The left lobe of the pancreas is larger than the right in the cat and easier to identify on ultrasound examination. The pancreatic duct within the left lobe is usually clearly visible on ultrasound.
The landmarks that facilitate identification of the left pancreatic lobe are the stomach cranially, colon caudally and spleen laterally.
The landmark for the right lobe of the pancreas is the descending limb of the duodenum.
The feline pancreas is well-defined and isoechoic to slightly hypoechoic relative to surrounding fat.
Key ultrasonographic abnormalities suggestive of acute pancreatitis include enlargement and reduced echogenicity of the pancreas, and increased echogenicity of peripancreatic fat.
Ultrasonographic findings suggestive of chronic pancreatitis include abnormal echogenicity and/or size of the pancreas, irregularity of pancreatic margins, a nodular appearance and mild hyperechogenicity of peripancreatic fat.
As a minimum, the liver and small intestine should also be examined with ultrasound if features indicative of pancreatitis are identified.
Multiple pancreatic nodules <1 cm diameter are more likely to represent nodular hyperplasia, whereas a solitary mass >2 cm diameter is more likely to be neoplastic.
Potential consequences of pancreatitis include extrahepatic biliary obstruction and the formation of pancreatic pseudocysts or abscesses. Pseudocysts and abscesses typically have thick walls and may contain echogenic contents and, as such, it may not be possible to distinguish between them ultrasonographically. Differentiation may be possible through aspiration of contents and determination of amylase and lipase levels.
Since pancreatitis can appear mass-like on ultrasound and neoplasia can produce diffuse pancreatic changes, FNA of the pancreas may be warranted and is considered to be a safe and minimally invasive technique.

Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.