
Abstract
Objectives
The aims of this study were to: (1) describe the source, route of surrender and signalment of hoarded cats relinquished to the Toronto Humane Society (THS); (2) document the prevalence of medical conditions by group (place of origin); (3) compare medical conditions between institutional hoarding (IH) and non-institutional hoarding (NIH) environments; and (4) report length of stay (LOS) and outcomes in hoarded and non-hoarded cats.
Methods
A retrospective, descriptive epidemiological study was performed using THS records from between July 2011 and June 2014. The prevalence of medical conditions was calculated for the different groups. Univariable logistic regression with a random intercept to account for autocorrelation among animals from the same group was used to examine the influence of IH and NIH environments on selected medical conditions. LOS and outcomes were calculated for hoarded and non-hoarded cats.
Results
Three hundred and seventy-one hoarded cats from 14 sources were included. The majority (n = 352/371) were surrendered voluntarily, many with the assistance of a community intermediary. Upper respiratory infection (URI) was the most common medical condition (38% of cats), followed by dermatological disease (30%). The prevalence of medical conditions varied substantially between groups. The odds of URI at intake (odds ratio [OR] 4.35, P = 0.044) and chronic URI (OR 23.70, P <0.0001) were significantly greater for IH compared with NIH. Adoption rates, euthanasia rates and LOS were similar for hoarded and non-hoarded cats.
Conclusions and relevance
The different prevalence of medical conditions in groups of hoarded cats indicates a continuum of harm and severity in animal hoarding. Hoarded cats can have LOS and live release rates comparable with non-hoarded cats. Cats from IH were significantly more likely to have chronic URI. This study highlights the need for a greater focus on IH, as well as the role of community intermediaries and the potential for a harm reduction approach to animal hoarding.
Keywords
Introduction
Animal hoarding is a poorly understood phenomenon characterized by the pathological accumulation of more than the typical number of companion animals, failure to provide minimum standards of care, and denial of this failure and its impact on the animals and people involved.1,2 Animal hoarding is considered to be a special manifestation of object hoarding disorder.3–6
In a review of 4695 media reports of animal cruelty, animal hoarding accounted for 9% of cases. 7 The mean numbers of deaths were higher for hoarding cases than for other forms of cruelty. 7 Numbers of hoarded animals range from ⩽10 to >900,2,8–10 with typical numbers of 30–40.1,2,9,11 Large-scale and severe hoarding cases are expensive and resource-intensive, legal aspects are complex and costly, and many animals may have untreatable medical and behavioral conditions.8,10,12–15
As with other psychiatric disorders, animal hoarding disorder can be expected to encompass a range of severity. 16 This remains unexplored, because the published literature has focused on large-scale cases and/or those involving prosecutions.1,10,17–19 There is little published information on smaller-scale cases, particularly those associated with a collaborative approach that may involve voluntary relinquishment. 8 No studies have directly addressed institutional hoarding (IH), although it is a recognized phenomenon.17,18,20–23 The peer-reviewed animal hoarding literature is small, with only a few studies that describe medical conditions in hoarded animals.1,8,17–19,24,25
A retrospective study of 371 hoarded cats, relinquished to the Toronto Humane Society (THS) from 14 different sources from July 2011 to June 2014, was conducted. The objectives were to: (1) describe the source, route of surrender and signalment of hoarded cats relinquished to the THS; (2) document the prevalence of medical conditions in groups of hoarded cats from multiple sources; (3) compare medical conditions between cats from IH and non-institutional hoarding (NIH) environments; and (4) report length of stay (LOS) and outcomes in hoarded and non-hoarded cats.
Materials and methods
Study design
This retrospective, descriptive epidemiological study examined case records from the THS between 26 July 2011 and 11 June 2014. Cats were included if they were identified as having originated from a hoarding environment by a shelter veterinarian, a shelter manager and/or an intermediary (typically a community animal activist/volunteer or a partner agency), based on (1) having more than the typical number of companion animals and (2) failing to provide appropriate nutrition, sanitation, shelter and veterinary care. This included cats housed in large numbers with no control over breeding. The information provided by the owner or intermediary and any prior information about the owner were taken into account. The shelter does not carry out cruelty investigations or seizures and relies on intermediaries or partner agencies to identify hoarding situations and facilitate relinquishment. The majority of hoarded cats were relinquished voluntarily for the purpose of rehoming. In cases where the shelter accepted a subset of cats from a larger group that had been surrendered or seized elsewhere, the group was only included if at least 10 cats were received. This was a subjective cut-off below which calculated proportions were not considered to be informative.
The THS shelter is a private, limited-admission, adoption-guarantee (‘no-kill’) shelter with a full-service veterinary hospital. A standardized intake protocol was followed for all cats: veterinary examination, treatment for internal and external parasites, core vaccines, Wood’s lamp screening for dermatophytosis and retroviral screening. Additional diagnostics and treatment were provided as needed.
Information was retrieved from paper and electronic records (PetPoint Data Management System).
Descriptive statistics and medical conditions
Hoarded cats were assigned a group number based on their place of origin. Descriptive statistics and medical conditions were recorded. Denominators were adjusted for missing data points when necessary. Immature kittens (0–6 weeks of age) were excluded from the analysis of oral and dental disease. Definitions for medical conditions are provided in Table 1.
Definitions used to categorize age group and medical conditions in hoarded cats surrendered between July 2011 and June 2014

URI = upper respiratory infection
IH and NIH
IH was classified as hoarding occurring within an organization with a designated facility for housing animals and advertising itself to the public as a rescue or shelter, while NIH occurred in a home environment. Groups were excluded from this part of the analysis if there was insufficient information to allow classification.
Outcomes and LOS to adoption
Data for outcome and LOS to adoption were retrieved for cats surrendered to the shelter during the study period. Cats were excluded from this part of the analysis if there were missing or inaccurate data. If more than one outcome occurred during the study period (eg, adoption and return adoption), only the first outcome was included. Live release rate (LRR) was calculated as ([adopted + barn placement + return to owner]/[total number of cats – active cats]). Two LOS periods were assessed: total LOS (ie, from intake to adoption, including periods waiting for surgery or receiving medical care, etc) and LOS after being made available for adoption.
Data analysis
Descriptive and summary statistics were generated using Microsoft Excel. Univariable logistic regression models were fitted to identify associations between originating from an IH vs NIH source and the occurrence of selected medical conditions. A random intercept was included to account for autocorrelation among cats from the same group (place of origin). No statistical tests were conducted for feline immunodeficiency virus (FIV), feline leukemia virus (FeLV), chronic diarrhea and non-parasitic otitis owing to their absence in the groups classified as NIH. STATA version 15.0 was used for statistical analyses. A P value <0.05 was considered statistically significant.
Results
Descriptive statistics
Three-hundred and seventy-five hoarded cats from 14 different groups (places of origin) were identified (Table 2). Four cats were excluded because of missing data, leaving 371 for analysis. The number of cats from each source ranged from 10–77 (mean 26.5; median 20.5). Nine groups of cats originated from homes, two from rescues and one from an informal rescue, about which no further information was available. Infor-mation about the source environment was not recorded for two groups, which were surrendered through community intermediaries.
Descriptive statistics for 371 hoarded cats surrendered between July 2011 and June 2014
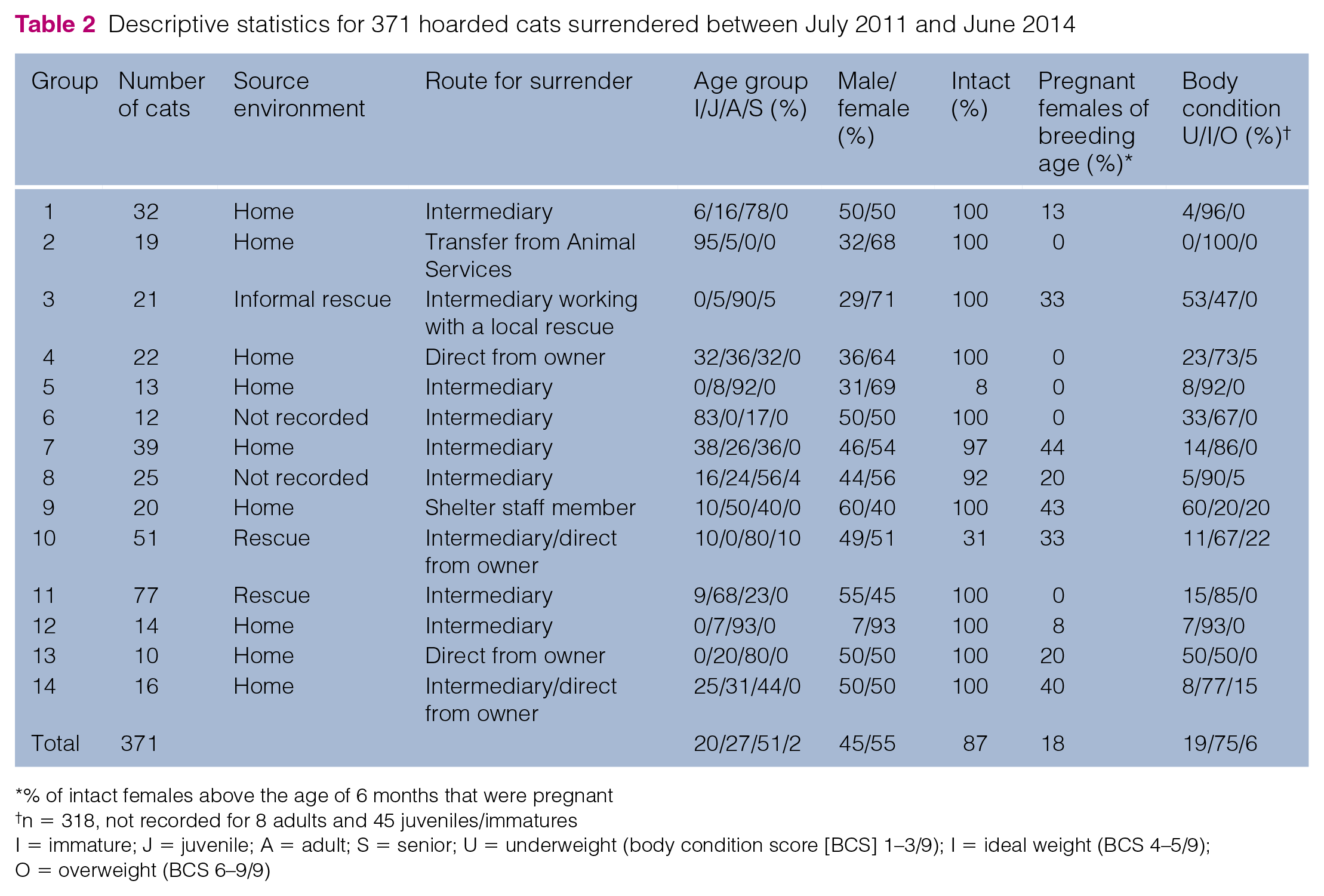
% of intact females above the age of 6 months that were pregnant
n = 318, not recorded for 8 adults and 45 juveniles/immatures
I = immature; J = juvenile; A = adult; S = senior; U = underweight (body condition score [BCS] 1–3/9); I = ideal weight (BCS 4–5/9); O = overweight (BCS 6–9/9)
Two groups were relinquished directly by the owner or a family member, one was transferred from Animal Services and 11 were brought in by or with the help of intermediaries (community rescue groups, community or shelter volunteers and in one case a shelter staff member). Two hundred and fifty-three cats (68%) were brought in by intermediaries alone, with another 67 (18%) surrendered by the hoarder with help from an intermediary. Other than group 2, which had been seized by Animal Services, all cats (n = 352/371; 95%) were brought in voluntarily. Cats from groups 10 (51 cats) and 11 (77 cats) were brought in over a period of 12 and 33 months, respectively.
The majority of cats were immature/juveniles (47%) or adults (51%), with 2% seniors (Table 2). Eighty-seven percent of the cats were intact and 18% of breeding age females were pregnant. Body condition was recorded as ideal in 75% of cats, underweight in 19% and overweight in 6%.
Medical conditions in hoarded cats
The prevalence of medical conditions varied between groups (Table 3). Upper respiratory infection (URI) at intake (present in 13/14 groups), skin disease (12/14 groups), fleas (10/14 groups), ear mites (9/14 groups) and gingivitis (9/14 groups) were found in the largest number of groups. FeLV (present in 1/14 groups), FIV (3/14 groups), chronic diarrhea (3/14 groups) and non-parasitic otitis (3/14 groups) were less common. Groups 3 and 10 had higher-than-average prevalence for 9/13 and 10/13 tabulated conditions, respectively.
Prevalence of 13 medical conditions in 371 hoarded cats from 14 groups, surrendered between July 2011 and June 2014

Prevalence is shown as %. Bold values show above-average prevalence
NIH = non-institutional hoarding; U = unclassified; IH = institutional hoarding; URI = upper respiratory infection; FIV = feline immunodeficiency virus; FeLV = feline leukemia virus
URI
URI was diagnosed at intake in 142/371 hoarded cats (38%). Of these, 112/142 (79%) had mild clinical signs, 26 (18%) had moderate and four (3%) had severe. An additional 63/222 cats (28%) developed URI post-intake. Chronic URI was recorded for 47/362 cats (13%), of which 40/47 (85%) had URI diagnosed at intake. The highest prevalence of URI at intake was in groups 3 (71%) and 6 (83%); these groups also had the highest prevalence of chronic URI, with 38% and 45%, respectively.
Retrovirus testing
Results were available for 366/371 (99%) cats (Table 3). Five percent (n = 19/366) were FIV positive and 1% (n = 3/366) were FeLV positive. One cat was both FIV and FeLV positive. Within groups 3, 8 and 10, FIV prevalence was 57%, 4%, and 12%, respectively, and FeLV prevalence in group 10 was 6%.
Diarrhea and intestinal parasites
Diarrhea was recorded within 72 h of intake in 19/369 (5%) cats from four groups (Table 3). Prevalence was 6% each in groups 1 and 11, 43% in group 3 and 8% in group 7. Diarrhea was recorded after 72 h for an additional 84/343 cats (24%). Chronic diarrhea was identified in 5% (n = 19/362) and occurred in groups 3 (38% of cats), 10 (15%) and 11 (5%).
Fecal flotation or gross parasite identification was performed for 84 cats, 54 of which had diarrhea. Giardia ELISA was performed on 11 samples. Parasites were found in 24/84 samples (29%) and consisted of: tapeworm (n = 10); Isospora species (n = 4); Giardia species (n = 4); Toxocara species (n = 4); both Toxocara and Giardia species (n = 1); and both Toxocara and Isospora species (n = 1).
Dermatological disease
Skin lesions were noted in 112/369 cats (30%). Of the 112 cats with skin lesions, 40% had inflammation, 27% had alopecia and 35% had wounds or injuries. Dermatophytosis was diagnosed by fungal culture in 15/112 (13%); only clinically suspicious cats were cultured. Live fleas or flea dirt were recorded in 82/369 cats (22%), and in 100%, 71% and 81% of cats in groups 2, 3 and 14, respectively. Thirty-eight percent of cats with fleas (n = 31/82) had skin lesions.
Aural disease was noted in 108/369 cats (29%). Ear mites were recorded in 88% (n = 95/108) of affected cats and non-parasitic otitis (including purulent otitis) in 12% (n = 13/108). Sixty of the 95 cats with ear mites (63%) also had skin lesions, and 66/112 cats (59%) with skin lesions also had otitis or ear mites.
Oral and dental disease
The majority of cats (307/367; 84%) had no oral disease or mild gingivitis, 52 (14%) had moderate to severe gingivitis, and eight (2%) had gingivostomatitis (Table 3). Dental cleaning or extractions were required for 70 cats (19%): cleaning alone was required for 15; 1–3 extractions for 25; four or more extractions for 21; and full-mouth extractions for nine.
Other medical conditions
Heart murmurs were auscultated in 20/369 cats (5%) for which this data was recorded and were most prevalent in group 5 (38%). Nine cats had hematuria; seven of these were from group 1.
Medical conditions in cats from IH and NIH environments
From the 10 groups that could be classified, 128 cats (two groups) were from IH and 163 cats (eight groups) were from NIH environments (see Table 3 for groups). Group 3 was suspected to originate from an IH environment but was not classified owing to very limited information.
Group (place of origin) was a significant random effect for the univariable analyses of URI at intake, skin disease, fleas, gingivitis, ear mites and heart murmurs, indicating that in this study population, these conditions clustered by group. After controlling for clustering within groups, significant differences in odds ratios (ORs) for IH vs NIH cats were found for URI at intake (OR 4.35; P = 0.044) and chronic URI (OR 23.70; P <0.0001) (Table 4).
Univariable analysis of eight medical conditions in 291 cats surrendered from institutional hoarding (IH) (n = 128) and non-institutional hoarding (NIH) (n = 163) environments

Bold indicates statistical significance
Moderate/severe gingivitis to gingivostomatitis
OR = odds ratio; CI = confidence interval; URI = upper respiratory infection
Outcomes for hoarded and non-hoarded cats
First outcomes were analyzed for 371 hoarded cats and 6359 non-hoarded cats surrendered to the shelter during the study period (Table 5). In 11/14 hoarded groups, ⩾90% cats were adopted (Table 6). In groups 1, 7 and 9, where <80% were adopted, a higher proportion of cats were placed in barns and/or euthanized for medical reasons. Outcomes for hoarded and non-hoarded cats were broadly similar (Table 5). The LRR was 95.9% for hoarded cats vs 92.5% for non-hoarded cats.
Outcomes for 371 hoarded cats and 6359 non-hoarded cats surrendered from July 2011 to June 2014

No outcome at the time of data collection
Outcomes for 14 groups of hoarded cats (n = 371) surrendered from July 2011 to June 2014

No outcome at the time of data collection
LOS for hoarded and non-hoarded cats with adoption outcomes
LOS to adoption was calculated for 249 hoarded and 4171 non-hoarded cats (Table 7). Medians and interquartile ranges were similar for the hoarded and non-hoarded cats, with a longer maximum LOS for the non-hoarded cats.
Length of stay (LOS) in days for hoarded and non-hoarded cats surrendered from July 2011 to June 2014

Data are median (25th–75th percentile; maximum)
Discussion
Previous reports have mainly focused on large-scale hoarding situations in which regulatory intervention was typically required.1,10,17–19 In the current study, the majority of the animals were surrendered voluntarily. The role of community intermediaries is noteworthy, as the majority of cats were surrendered with their assistance. This type of intervention has been reported infrequently, 19 and the proportion of hoarded animals relinquished in this way is unknown. The intermediaries were typically colony cat caregivers and/or involved with local rescue groups. They were able to provide a navigable pathway between the animal hoarders and the shelter.
The study results support recent findings that some hoarding situations can be managed using a harm-reduction approach. 8 Animal hoarders tend to be extremely opposed to euthanasia; 26 voluntary relinquishment to the THS may have been considered acceptable because it is a low-euthanasia shelter with the resources to treat and house sick and long-stay animals. The study reflects a limited geographic area, a well-resourced shelter and, largely, a group of individuals who were willing to seek or accept help. Findings can be expected to differ in other areas and in cases where the only way to address hoarding is by legal seizure. It should be noted that the traditional legal seizure model can result in delayed responses to hoarding situations, stress for the animals and owners, overwhelming costs, extended LOS (due to legally mandated holding times) and lower LRR,8,12,13,15 without necessarily resolving the underlying problem.10,13
Hoarded cats in this study had a LRR of 95.9%, and similar adoption rates and LOS to non-hoarded cats. This was made possible by the investment of considerable medical and staff resources, as well as manageable group sizes and managed intake (cats from groups 10 and 11 were relinquished over a period of time). The higher euthanasia rate and longer LOS for non-hoarded cats may reflect the nature of the shelter intake, which includes neonates and animals with complex medical or behavioral conditions. Most of the hoarded cats were young and most medical conditions were curable or manageable. Once available for adoption, LOS for young, friendly animals is short at this shelter, even if medical or behavioral conditions are present. A recent report of a collaborative, multidisciplinary and multi-agency animal hoarding strategy also reported a high LRR (92%), 8 reflecting a shift in the expectations and abilities of shelters to successfully manage and rehome hoarded cats.
The high proportion of unaltered cats in this study (almost 90%) is consistent with previous findings that uncontrolled breeding is often a major factor in hoarding.1,10 Spay or neuter programs could be offered at least as an interim solution when immediate removal of all or most of the cats is impractical or impossible. Provision of primary healthcare may also be a way to build trust and pave the way for subsequent surrender of animals for rehoming. 8
Diseases of malnutrition, overcrowding and general neglect are common in hoarded animals.1,8,19,27 They include emaciation, matted coats, wounds, URI, parasites, stomatitis, diarrhea and retroviral infections, as well as infections that are unusual in their severity or prevalence.8,17–19,24 The common medical conditions in this study were typical for hoarded cats.17,28 Health status varied widely between the groups. The most common condition was URI, which is associated with stress and crowding in cats. 29 Some conditions, such as chronic diarrhea and non-parasitic otitis, were only present in a small number of groups. This most likely reflects endemic and/or opportunistic infections. A high retrovirus prevalence could be due to stress and antagonistic interactions, 17 or might be due to actively rescuing positive animals. Inbreeding can be expected in many hoarding environments and may account for the high prevalence of heart murmurs in group 5.
To our knowledge, this study provides the first comparison of disease prevalence in cats from IH vs NIH environments. Hoarding masquerading as legitimate sheltering or rescue was identified as a growing trend some years ago and it was noted that the line between legitimate and hoarding institutions can be indistinct.13,22,23 Such organizations are able to raise funds, attract enablers and easily add animals. While the existence of IH is well recognized,17,18,20–23 and, in fact, was part of the motivation behind the development of the Association of Shelter Veterinarians’ Guidelines for Standards of Care in Animal Shelters (Patronek; https://www.aspcapro.org/sites/default/files/aspca_asv_webinar_slides.pdf), it has not been clearly defined or studied as a distinct phenomenon. IH was identified in five large-scale hoarding cases,17,18 four of which were described as ‘sanctuaries’, but the phenomenon was not discussed further. 17
In the current study, IH was defined as hoarding occurring within an organization with a designated facility for housing animals and advertising itself to the public as a rescue or shelter. This is proposed as a working definition. The term ‘rescuer hoarder’22,23 is distinct from IH because not all rescuer hoarders operate in an institutional framework and not all institutional hoarders are ‘altruistic’ (eg, exploiter hoarders). 22
In the present study, group 3 (thought to be an informal rescue but with insufficient information for classification) and group 10 (a registered charity) had a high prevalence of many of the medical conditions reported. Group 11, a rural rescue, had a high prevalence of URI, chronic URI and non-parasitic otitis. Otitis media caused by Streptococcus equi subspecies zooepidemicus was confirmed in several cats from this group (data not shown). The increased odds of URI, and especially chronic URI (OR 23.70), in the IH cats vs NIH cats most likely resulted from untreated disease, stress and overcrowding over a long period, as well as prolonged exposure to specific endemic infections.
A limitation of the study was its retrospective nature, combined with the fact that the shelter was the recipient of the cats and not the initiator of their removal from the hoarding environments. This resulted in limited information about the hoarders and source environments. The assessment of hoarding was based mainly on the number of animals, information gathered directly from the owners and information from third parties. To our knowledge, none of these third parties had any formal training about animal hoarding. While there is no substitute for visiting a hoarding environment and assessing it first hand, it is also the case that animal hoarding is broadly defined, with no standardized criteria.1,2,30 Previous studies of animal hoarding have not had access to psychiatric evaluation and have focused instead on animal numbers, health and living conditions.
Conclusions
The findings support recent work showing that a high LRR is feasible for hoarded animals. 8 At least in some circumstances, shelters taking in hoarded cats may not be overburdened with an extremely long LOS, and may be able to adopt out most of the cats. However, considerable resources are needed to resolve some of the medical conditions found in hoarded cats. The different disease prevalence and outcomes between hoarded groups demonstrates a continuum of harm and severity in animal hoarding.
The findings highlight the need for a greater focus on IH. They also highlight alternatives to the traditional seizure of animals and the role that can be played by community members. More research is needed to better understand the practicalities and long-term outcomes of a harm-reduction approach to animal hoarding.
Footnotes
Acknowledgements
The authors are deeply grateful to Dr David Kozuch for his support, without which this study would not have been possible. We gratefully acknowledge the support of the management and Board of the Toronto Humane Society.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors thank Procter & Gamble for funding a summer internship for JG at the Toronto Humane Society.