
Abstract
Objectives
The aim of this study was to describe a series of cats suffering from thoracic dog bite wounds, in order to detail the clinical, radiographic and surgical findings, and evaluate outcomes and factors associated with mortality.
Methods
The medical records of cats with thoracic dog bite wounds presenting to a single institution between 2005 and 2015 were retrospectively reviewed. Data relating to clinical presentation, wound depth and management, radiographic findings, surgical findings and mortality were collected. Wound depth was defined as no external wound, superficial, deep or penetrating, and wound management was defined as conservative, exploratory or thoracic exploration. Statistical analyses were performed using Fisher’s exact test, the Mann–Whitney U-test and the χ2 test.
Results
Twenty-two cats were included, of which two were euthanased on presentation. In cats where wound depth could be assessed (21/22), six had no external wounds, four had superficial wounds, three had deep wounds and eight suffered penetrating wounds. Sixteen cats also suffered wounds elsewhere, most commonly to the abdomen. Neither an abdominal wound nor abdominal surgery were associated with mortality. Pneumothorax was the most common radiographic finding (11/18). Individual radiographic lesions were not significantly associated with respiratory pattern, presence of pseudo-flail, need for thoracotomy or lung lobectomy, or survival. The presence of ⩾3 radiographic lesions was associated with the presence of a penetrating wound (P = 0.025) and with having thoracic exploration (P = 0.025). Local exploration was performed in 7/20 cats, while 8/20 underwent thoracic exploration. Wound management type was not significantly associated with mortality. Overall mortality rate was 27%.
Conclusions and relevance
Presence of ⩾3 radiographic lesions should raise suspicion of a penetrating injury and may be suggestive of injury requiring a greater level of intervention. The treating veterinarian should have a high index of suspicion for penetrating injury and be prepared in case thoracic exploratory surgery is necessary, particularly in the presence of pseudo-flail chest, pneumothorax or ⩾3 radiographic lesions.
Introduction
Dog bite wounds are commonly encountered in the small animal emergency setting and are reported to be the second most common traumatic presentation in cats. 1 The thorax is a commonly bitten region1–5 and bites here have been associated with higher mortality rates.2,4,6
Bite wounds are unique because they cause a combination of crush, tear, avulsion and puncture injuries,3,4 along with inoculation of bacteria. 7 Additionally, the external wound is often not representative of underlying injury. Two previous studies evaluating thoracic bite wounds (predominantly in dogs, although eight cats were included) found discrepancies between external wounds and underlying radiographic and surgical findings.8,9 This is likely a result of the high skin mobility and elasticity of the rib cage in dogs and cats, meaning that there can be significant damage to underlying structures with only minimal external damage.2,4,8,9 The study by Scheepens et al reported either rib fractures (40/45), flail chest (35/45), pneumothorax (31/45), muscle lacerations (44/45) or a combination of these in a majority of cases, despite 16 dogs having no evidence of skin perforation. Additionally, half of the cases requiring lung lobectomy had no evidence of skin penetration.
To our knowledge, there have been 13 cats with thoracic bite wounds described in the literature in the past 20 years. It is not possible to determine details of their injuries and treatment, as findings were summarised with dog populations.6,8
The aim of this study was to describe a series of thoracic dog bite wounds in cats, in order to detail the clinical, radiographic and surgical findings, and to evaluate outcomes and factors associated with mortality. We hypothesise that initial examination findings are not associated with radiographic and surgical findings, or outcome.
Materials and methods
This study was approved by the Royal Veterinary College Ethics and Welfare Board. Electronic patient records of a single first-opinion emergency and referral veterinary centre (Queen Mother Hospital for Animals [QMHA], UK) were retrospectively searched for cases presented between March 2005 and May 2015. Cats were included if they were confirmed to have suffered a dog bite to the thoracic area and if medical records were complete. Data relating to clinical examination, blood tests, bacteriology, radiographic lesions, surgical findings, management and outcome were recorded.
Clinical examination
Tachypnoea was defined as a respiratory rate >40 breaths per minute and dyspnoea was defined as an increase in respiratory effort or a requirement for oxygen supplementation as judged by the treating veterinary surgeon. Any paradoxical movement of part of the chest wall during respiration was interpreted as pseudo-flail chest, unless radiographic findings confirmed true flail segment (⩾2 fractures of at least two adjacent ribs). 10
Radiographic findings
Specific radiographic lesions, noted as present or absent in each case, were rib fracture, sternal fracture/luxation, pleural effusion, pulmonary contusions, diaphragmatic hernia, pneumothorax and pneumomediastinum.
Pleural effusion and pneumothorax were defined as the presence of fluid or air within the pleural space, respectively. Areas of poorly marginated, increased soft tissue opacity in the lung were interpreted as pulmonary contusions. 11
Surgical findings
In order to aid comparison with previous literature, wound depth of the thoracic lesion was retrospectively classified (in accordance with the descriptions by Cabon et al) as no external wound, superficial (skin only), deep (involving subcutaneous tissue) or penetrating (communication between external thorax and pleural space). 8 In the case of multiple thoracic wounds, the case was classified according to the more severe lesion. The presence or absence of injury to other body areas was noted.
Likewise, wound management was retrospectively classified from evaluation of the surgery report (according to the description by Cabon et al) as: conservative (no surgical exploration), exploratory (local exploration) or thoracic exploration (entry into thoracic cavity) and details of the specific management of each case were documented. 8
Surgical findings were recorded as per the classification of radiographic lesions. Pulmonary contusions were recoded as present if lung parenchyma was described in the surgical record as contused, discoloured or containing areas of haemorrhage within the parenchyma.
Surgical treatment and subsequent care was at the discretion of the attending veterinary surgeon.
Complications/postoperative progression
The primary care practices of any cases that had been transferred were contacted via telephone in order to try to establish outcome.
Where possible, the cause of death was recorded. In cases where owners elected euthanasia, the underlying cause was reviewed. Cats euthanased owing to financial constraints were excluded from mortality calculations.
Statistical analysis
Data were assessed for normality using the Kolmogorov–Smirnov test. Statistical analyses were performed using the Fisher’s exact test, Mann–Whitney U-test, the χ2 test and the Kruskal–Wallis test. Normally and non-normally distributed data are reported as mean ± SD, and median (interquartile range [IQR]), respectively. Statistical tests were undertaken using a statistical software package (SPSS Statistics, version 24; IBM). P values <0.05 were considered significant.
Results
Descriptive
Twenty-two cats met the inclusion criteria, including two entire females, 10 neutered females, four entire males and six neutered males. There were 20 domestic shorthair cats, one Abyssinian and one British Blue cat. Median age was 48 months (IQR 17–72 months) and mean body weight was 4.35 ± 1.14 kg. Ten cases were presented as referrals, while 12 were initially presented to the institution’s emergency first-opinion service. Eight of these were subsequently referred for specialist management.
Clinical examination
Only 4/22 cats were considered to have normal respiration on presentation, with 15/22 and 12/22 presenting with tachypnoea or dyspnoea, respectively, with nine cats presenting with both.
Assessment of thoracic wounds revealed that 6/22 cats had no external wounds. One cat with no externally visible wound was euthanased shortly after arrival and was excluded from further detailing of wound depth and management. Another cat, with a visible thoracic wound, was euthanased shortly after arrival, and it was not possible to comment further on wound depth in this case. Of the remaining 20 cases, 4/20 were deemed to have superficial wounds, 3/20 were deep and 8/20 were penetrating. Further details regarding each case can be found in Table 1.
Table detailing respiratory status, number of radiographic lesions, wound depth, wound management and progression of each case
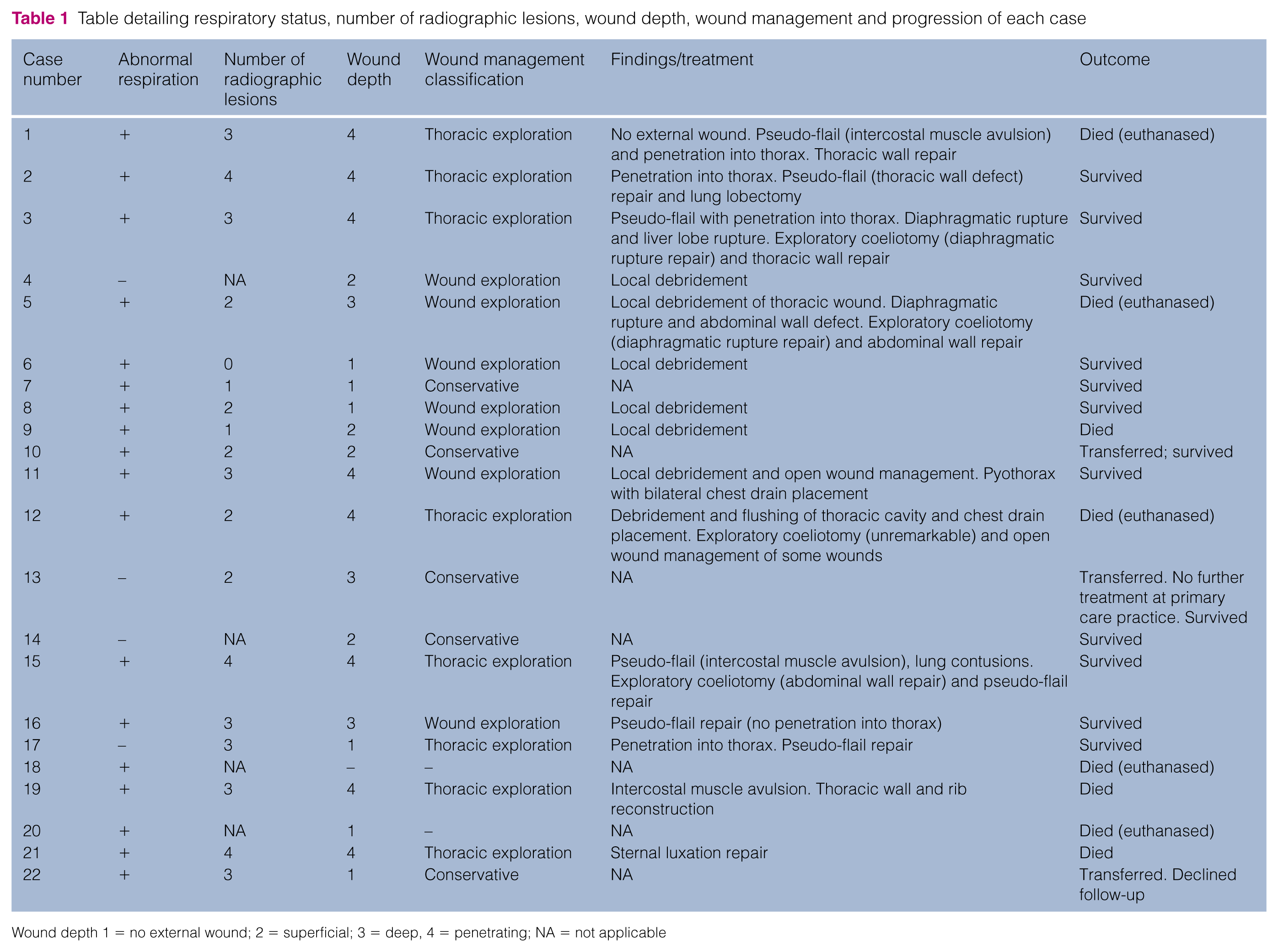
Wound depth 1 = no external wound; 2 = superficial; 3 = deep, 4 = penetrating; NA = not applicable
A majority of cases (16/22) had wounds elsewhere, predominantly affecting the abdomen (11/22) and limbs (7/22). Pseudo-flail chest was present in 9/20 cases. Respiratory status was not significantly associated with the presence of pseudo-flail, wound depth, wound management, surgical findings or survival.
Radiographic findings
The two cats that were euthanased shortly after arrival did not undergo thoracic imaging and were excluded from further evaluation. Radiographs were performed in 18/20 cats. The reason for not performing radiographs was financial constraints in one case and unclear in the other. A subsequent CT scan was performed in a single case. In the case where a CT scan was performed, a rib fracture, pulmonary contusions and pleural effusion were diagnosed in addition to the pneumothorax noted on radiographs. The most common radiographic lesion was pneumothorax (11/18), followed by pulmonary contusions (7/18), pleural effusion, sternal fracture and rib fracture (6/18 cases each).
Individual radiographic lesions were not significantly associated with respiration, presence of pseudo-flail, need for thoracotomy or lung lobectomy, or survival. The presence of ⩾3 radiographic lesions was, however, significantly associated with the presence of a penetrating wound (P = 0.025), as well as with undergoing thoracic exploration (P = 0.025). Of cats that underwent thoracic exploration, 7/8 had ⩾3 radiographic lesions. Of the remaining cats that underwent radiography and treatment, only 3/10 had ⩾3 radiographic lesions. The presence of ⩾3 radiographic lesions was not significantly associated with survival, or length of hospitalisation. The presence of a sternal fracture was also significantly associated with having a thoracic exploration (P = 0.043)
The presence of rib fractures was significantly associated with having a deep wound (P = 0.025). There was otherwise no association between individual radiographic lesions or grouped number of radiographic lesions and wound depth or wound management.
There was no statistically significant association between the presence of pneumothorax and pseudo-flail chest (P = 0.05).
Clinical pathology
An in-house blood gas, electrolyte and metabolite panel was performed in 17/22 cats. Hyperlactataemia was present in 9/17 cases. Hyperlactataemia was not associated with respiratory status, radiographic findings, wound depth, wound management or survival.
Bacteriology was performed in 16/20 cats, of which six were positive, most commonly culturing Staphylococcus species (3/6) or Escherichia coli (2/6).
All but one cat were treated with broad-spectrum antibiotic therapy, most commonly amoxicillin–clavulanate. Based on the culture results, the organisms cultured in 4/6 cats were susceptible to amoxicillin–clavulanate.
Of the isolates not sensitive to amoxicillin–clavulanate, one sample cultured a multi-resistant E coli and a multi-resistant coliform. 12 Antimicrobials to which both organisms were susceptible were amikacin, polymyxin B and imipenem only. Culture from the other case isolated a coagulase negative Staphylococcus species, as well as Pseudomonas species. The Staphylococcus species was sensitive to amoxicillin–clavulanate, whereas the Pseudomonas species was susceptible only to enrofloxacin or oxytetracycline.
Surgical management
Of the cats managed for their bite wounds, 5/20 were initially treated conservatively, although 3/5 were transferred to their primary care practice for further management as necessary. Both of the two cats that remained at the QMHA and that were managed conservatively survived to discharge. Local exploration was performed in 7/20 cats, while 8/20 underwent thoracic exploration, of which five and four cats survived, respectively (Figure 1). Wound management type was not significantly associated with mortality (conservative [P = 0.52]/exploration [P = 0.99]/thoracic exploration [P = 0.34]) or length of hospitalisation (P = 0.357). Neither an abdominal wound (P = 0.99) nor abdominal surgery (P = 0.99) was associated with mortality. The presence of a sternal fracture was significantly associated with thoracic exploration (P = 0.043), as was the presence of a penetrating wound (P = 0.001). There was not a statistically significant association between pseudo-flail chest and thoracic exploration (P = 0.05).

Flowchart illustrating case progression
Postoperative progression
Mean length of hospitalisation was 10 ± 6.3 days. In total, 11 cats survived to discharge and three were transferred to their primary care practice, prior to definitive treatment. One cat was lost to follow-up, while the other two survived. Of the two with follow-up information available, one did not require further management of thoracic injuries. It was not possible to determine treatment in the other case, although the patient was known to be alive 5 months after injury.
Two cats were euthanased shortly after presentation, owing to financial constraints. These were excluded from mortality calculations. During hospitalisation, six cats died or were euthanased owing to worsening of their condition, most commonly due to sepsis/systemic inflammatory response syndrome (SIRS) (5/6 cases). Overall mortality rate was 27% (6/22 cases).
Discussion
This study describes the largest reported population of cats suffering from thoracic dog bite wounds at the time of publication. These cases can be challenging to manage given the potential for severe underlying pathology, in the absence of externally visible injuries or clinical signs, as evidenced by the lack of association between underlying injury and respiratory status or radiographic signs in this study.
Despite a majority of cases presenting with dyspnoea/tachypnoea, this was not associated with outcome, which is in agreement with previous studies. 8 Given the retrospective nature of this paper it was not possible to determine the influence of other factors, such as pain, on respiration.
Of the 18 cats in which thoracic radiography was performed, all but one were found to have at least one radiographic lesion. Pneumothorax was diagnosed in a majority of cases, suggesting penetrating injury or lung lobe laceration, and potentially requiring further interventions. In contrast to findings by Cabon et al, 8 who evaluated eight cats and 54 dogs suffering from thoracic dog bite wounds, our study found a significant association between the presence of ⩾3 radiographic lesions and a penetrating wound, as well as a need for thoracic exploration. It is possible that more severe radiographic findings influenced decision-making regarding the need for surgery, leading to bias in those undergoing thoracic exploration. Additionally, sternal fracture and rib fracture were associated with thoracic exploration and presence of a deep wound, respectively. Presence of these radiographic lesions are therefore likely to affect the course of treatment and may also require additional intervention. These results suggest that thoracic radiography should be performed in all cats suffering from thoracic dog bite wounds, which is in accordance with previous recommendations in the literature. 8
Of the cats managed at the QMHA (excluding the two that were euthanased shortly after presentation and three that were transferred elsewhere), 15/17 underwent surgical exploration. Older literature advocated a conservative approach to management of bite wounds,3,4 while more recent publications recommend exploratory surgery.5,6,8,9,13,14 One study advocated thoracic exploration in any cases found to have rib fracture, radiographic evidence of lung contusions, pneumothorax or severe subdermal trauma, which resulted in only one unnecessary thoracotomy. 9 Application of these guidelines to our study population in which radiographs were performed would have resulted in exploratory thoracic surgery in 16/18 cases. In actuality, eight of these 16 cases underwent exploratory thoracic surgery, four underwent wound exploration, one was managed conservatively and three were transferred to their primary care practice. Of the five cases that underwent wound exploration only or were managed conservatively, that is to say, the cases that were not managed according to the aforementioned recommendation, only one did not survive to discharge. Our results suggest that thoracic exploratory surgery (ie, thoracotomy/sternotomy) may have been unnecessary in some of these cases.
Pseudo-flail chest was present in 9/20 cases in this study. Seven underwent thoracic exploration and pseudo-flail repair, one was transferred to the primary care practice and one underwent wound exploration, pseudo-flail repair and was found not to have a penetrating injury. A retrospective evaluation of management of flail chest in dogs and cats, caused by various traumatic events, did not reveal a significant difference in outcome between surgically and conservatively managed cases. 10 The previously mentioned study evaluating dogs suffering thoracic bite wounds revealed that 35% of dogs with flail chest required lung lobectomy. 9 As a result they also advocated surgical exploration in cases of flail- or pseudo-flail-chest. Although only one case in our population required lung lobectomy, the vast majority of cases with pseudo-flail (7/8) were found to have penetrating injuries, warranting exploration, debridement and lavage. The flail segment was surgically addressed in all eight cases. This would support the recommendation of surgical exploration in all cases of pseudo-flail.
Although no set protocol exists at the study institution, surgical exploration is advocated for a number of reasons. Bite wounds are inoculated with bacteria from the patient’s skin and the attacking dog’s mouth.3,4 Additionally, the resultant injury can cause ischaemia and necrosis of surrounding tissue, leading to increased susceptibility to infection.15,16 Publications evaluating bacteriology of dog bite wounds in a dog population reported positive culture results in 52–80% of cases, which is higher than our study.7,17 In contrast to the aforementioned publications, at our institution intra-operative swabs are obtained following lavage, which may be associated with the lower rate of positive culture results in our study. The most commonly cultured bacteria in these studies included E coli, Staphylococcus species, Streptococcus species, Enterococcus species and Pasteurella species, of which 85.4–100% were susceptible to amoxicillin–clavulanate. Although two culture results in the current study revealed organisms non-susceptible to amoxicillin–clavulanate, our results suggest that this is an appropriate empirical choice, in keeping with responsible antimicrobial stewardship. 18 Additionally, the leading cause of death in our population was sepsis/SIRS. For these reasons, debridement and removal of bacterial contamination is advocated in all bite wounds. An additional advantage of surgical intervention is that it allows underlying injury to be identified and addressed as necessary.
Interestingly, a recent publication evaluating cats surgically managed for thoracic trauma (of varying aetiology) found a significant difference in animal trauma triage (ATT) score of survivors vs non-survivors and an overall mortality rate of 13%. 19 Evaluation of ATT scores was not possible in our study but could be considered in future investigations.
Mortality rates of 12.5–27% have been reported in dogs and cats suffering from dog bite wounds.6,8,9 One study reported a mortality rate of 11% in dogs and 27% in cats and included patients that had suffered dog bite wounds to any area of the body. To our knowledge, there are two studies specifically evaluating dog bite wounds to the thorax. One of these included only dogs and reported a mortality rate of 17.7%, while the other reported an overall mortality rate of 15.4%.8,9 The latter study included only eight cats, of which seven survived to discharge (equating to a feline mortality rate of 12.5%). Overall mortality rate in our study was 27%. This is within previously reported values in patients suffering from bite wounds and is higher than that reported for surgically managed feline thoracic trauma of varied aetiology. This could be reflective of the severity of bite injury vs other injury and we also speculate that the smaller body size of cats could mean that they are susceptible to more severe injuries than dogs.
There are limitations to this study, predominantly concerning the retrospective nature and limited case number. Reliance on case records was necessary, including classification of wound depth as described by the treating veterinary surgeon. There is potential for inherent bias in the determination of wound depth in the conservatively managed cases, as these were presumed to be less severely affected, without definitive surgical assessment being carried out. Cases were managed by various veterinary surgeons, meaning potential variability between assessments and treatment. Some cases were transferred to their primary care practice, meaning further evaluation was not possible and long-term follow-up was not performed.
Conclusions
Cats with thoracic bite wounds are challenging to manage as they are susceptible to injury of underlying structures, despite absence of externally evident injuries or clinical signs. Moreover, inoculation of bacteria and multifaceted tissue damage mean that these patients are at risk of developing wound infection with potentially fatal consequences. The presence of ⩾3 radiographic lesions should raise suspicion of a penetrating injury and may be suggestive of an injury requiring a greater level of intervention. Although an association is reported, radiographic findings should not be relied upon solely for determination of severity of injury. Given the limitations of assessing wound severity based on clinical and radiographic findings, the authors advocate surgical exploration of all thoracic dog bite wounds in cats. The treating veterinarian should have a high index of suspicion for penetrating injury and ought to be prepared in case extension to thoracic exploratory surgery is necessary.
Footnotes
Author note
The abstract was presented at the BSAVA Congress, Birmingham, UK, 8 April 2017.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.