
Abstract
Objectives
Bite wounds are a common cause of trauma in cats; nevertheless, large-scale studies of this trauma in cats are lacking. The aims of the present study were to characterise the clinical and clinicopathological findings in these cats, to assess the association of these variables and therapeutic measures with survival, and to assess the association between the animal trauma triage (ATT) score and severity of injuries score (SS) at presentation with survival.
Methods
The medical records of cats presented to a veterinary teaching hospital and two large referral clinics were reviewed retrospectively.
Results
The study included 72 cats diagnosed with canine bite wounds (with the dog attacks having been witnessed). Seventy-one percent of cats suffered multiple injuries, and there was a significant association between the number of injured body areas and survival, and between severity of injury and survival (P = 0.02 and P = 0.012, respectively). The median ATT scores and SSs for non-survivors were significantly higher compared with survivors (P <0.0001). There was a strong and significant correlation between ATT scores and SSs (r = 0.704, P <0.0001). Total protein and albumin were significantly lower and alanine aminotransferase significantly higher in non-survivors compared with survivors (P ⩽0.032). Fifty percent of cats were treated conservatively, 32% by local surgical debridement and 18% of cats required an exploratory procedure. Cats undergoing more aggressive treatments were significantly less likely to survive (P = 0.029). Fifty-seven cats (79%) survived to discharge.
Conclusions and relevance
Cats sustaining canine bite wounds have a good overall prognosis for survival to discharge. High ATT score, high SS, multiple body area injuries, penetrating injuries, radiographic evidence of vertebral body fractures and body wall abnormalities, as well as hypoproteinaemia and elevated alanine aminotransferase, are negative predictors of survival.
Introduction
Bite wounds (BWs) are a common cause of trauma in cats, accounting for 10–20% of traumatic injuries in this species, with most cats being attacked by dogs.1–3 Canine teeth may reach a force of up to 150–450 pounds per square inch, inflicting significant tissue damage by a combination of crush, tear, avulsion forces and puncture wounds.4–7 The initial trauma occurs as a result of the physical contact of teeth with tissues and organs, with injuries ranging from minor bruises to complicated wounds with or without systemic effects. The visible skin damage (laceration or puncture) may mistakenly be assumed to be negligible; however, it commonly does not reflect the degree of damage to underlying subcutaneous and deeper structures, and is often referred to as ‘the tip of the iceberg’.2–9 Teeth may crush and tear muscles and subcutaneous fat, creating large areas of dead space, which, in conjunction with devitalised tissues and compromised blood supply, promote bacterial growth. Secondary infection originates from cutaneous flora, environment or oral flora from the attacking animal.9–11 Several studies have described BWs in small animals; however, only a small numbers of cats are described.2,6,8,12–17 Moreover, only a few studies specifically evaluated BWs in this species.3,11
The animal trauma triage (ATT) score has been validated in dogs and cats, and its association with the outcome and treatment cost has been confirmed both retrospectively and prospectively.3,18,19 The ATT summarises the scores of six physiological categories, ranking abnormalities within each category from 0 to 3, yielding an overall score range from 0 to 18, with higher overall scores indicating increased injury severity. ATT scores are consistently higher in non-surviving animals sustaining trauma than in survivors.3,18,19
The severity of injuries score (SS) for rating traumatic injuries was suggested by Rochlitz 20 for cats injured and killed in road traffic accidents, based on a method developed to score vehicular trauma in human patients.21,22 A modified version of this scale was used in a study by Kolata et al, 1 describing patterns of trauma in dogs and cats. In the SS method, injuries are scored on a scale from 1 (none or very minor) to 5 (severe, potentially life-threatening) injuries; while cats that are dying, moribund or dead are scored 6. This method of assessing trauma severity was applied to cats suffering mostly vehicular trauma,20,23 and – to the best of our knowledge – was not validated in cats suffering BWs.
The purposes of this retrospective study were to (1) characterise the clinical and clinicopathological findings in cats suffering trauma due to canine BW; (2) assess clinical and clinicopathological variables and therapeutic measures associated with survival; and (3) assess the association between ATT and SS at presentation and survival.
Materials and methods
Study population and data collection
following a witnessed attack by a dog were included. Cats were excluded if the attack was unwitnessed or when owners declined treatment purely owing to financial constraints. Data collected from the medical records included signalment, body weight, physical examination findings, systemic signs, clinicopathological data, imaging data (radiography, ultrasound and point of care ultrasound), type of surgical intervention and findings during surgery, duration of hospitalisation, supportive care given and outcome.
For each cat, the severity and location of BWs was categorised as follows: (1) lesion severity was divided into four categories based on depth of bite penetration: no visible skin penetration, superficial skin wounds, deep wound (penetrating the skin and muscle in the areas) and penetrating wound (communication between skin and peritoneal cavity, thoracic cavity and retroperoperitoneum); and (2) number of body areas affected (eg, abdomen, thorax, limbs, back, head, perineum, neck, tail, ears).
Survival to discharge was recorded; cats that died or were euthanased owing to a grave prognosis were defined as non-survivors.
The ATT 18 score at presentation and the SS 20 were retrospectively calculated by the authors based on data from the medical files. ATT scores and SSs were determined separately and independently.
Statistical analysis
The distribution pattern of quantitative variables was assessed using the Shapiro–Wilk test. Quantitative data are presented as median and range. Continuous variables were also divided ordinally using defined cut-off values (reference interval [RI]): below, within and above standard RIs. Comparison between survivors and non-survivors was performed using a χ2 test and differences in medians were assessed using the Mann–Whitney rank-sum test. Survival models were evaluated for discrimination using the area under the receiver operating characteristic curve (AUROC). Adjusted odds ratios with 95% confidence intervals (CIs) were derived from logistic regression model (LRM). The significance for all tests was set at P <0.05.
Results
Signalment and history
Seventy-two cats met the inclusion criteria, of which 56 (78%) were admitted to the HUVTH and 16 (22%) to two large emergency referral clinics. Forty cats (56%) were males (16 [40%] intact; 24 [60%] castrated) and 32 (44%) females (10 [31%] intact; 22 [69%] spayed). Median age was 13 months (range 0.2–216). Median weight was 4.0 kg (range 0.78–7.5). There was no association between sex, age, weight and outcome (P = 0.330, P = 0.312 and P = 0.850, respectively). All cats except one had regular outdoor access prior to the assault. The attacking dogs’ breeds were documented in 14/72 cases (19%) and included Pit Bull (n = 9/14; 64%), German Shepherd (n = 2/14; 14%), Rottweiler (n = 2/14; 14%) and Malinois (n = 1/14; 7%). The time from injury to hospital admission was documented in 64 of the cases with a median of 2 h (range 1–168); there was no association between time to admission and outcome (P = 0.290). Prior to hospital admission 16/72 cats (22%) received primary medical care at another clinic; in all cases treatment was conservative and included one or more of the following: intravenous (IV) fluids, antibiotics, analgesia and oxygen supplementation. There was no difference in survival rate between cats with or without prior veterinary care (P = 0.569).
Severity and location of BWs
Of the 72 cats, 51 (71%) suffered multiple injuries (defined as BWs to more than one body area), with no association between overall multiple injuries and outcome (P = 0.129). Nevertheless, there was a significant association between the number of injured body areas and survival (P = 0.02); 95% of cats with BWs to one area survived vs survival rates of 83%, 71% and 43% in cats with BWs to two, three and four areas, respectively. The most commonly injured body areas were the abdomen, the limbs and the thorax (Table 1). A significant difference was found between survivors and non-survivors in cats with BWs to the thoracic spine (P < 0.0001). The proportion of all cats bitten in the abdomen, thorax or both was 71%. Of the non-survivors, 14/15 (93%) suffered BWs to the abdomen, thorax or both. In three cats (4%), wound severity was not documented and none survived to discharge. Three cats (4%) presented without visible wounds; two of them (66%) survived to discharge and the non-survivor was euthanased due to a vertebral body fracture. Twenty-four cats (33%) had superficial wounds (of which 23 [96%] survived), 29 (40%) cats suffered deep wounds (of which 25 [86%] survived) and 13 (18%) cats suffered penetrating wounds (with only 7 [54%] surviving to discharge). The severity of injury was significantly associated with survival (P = 0.012).
Distribution of body parts injuries in 72 cats admitted to a veterinary hospital following canine bite wounds
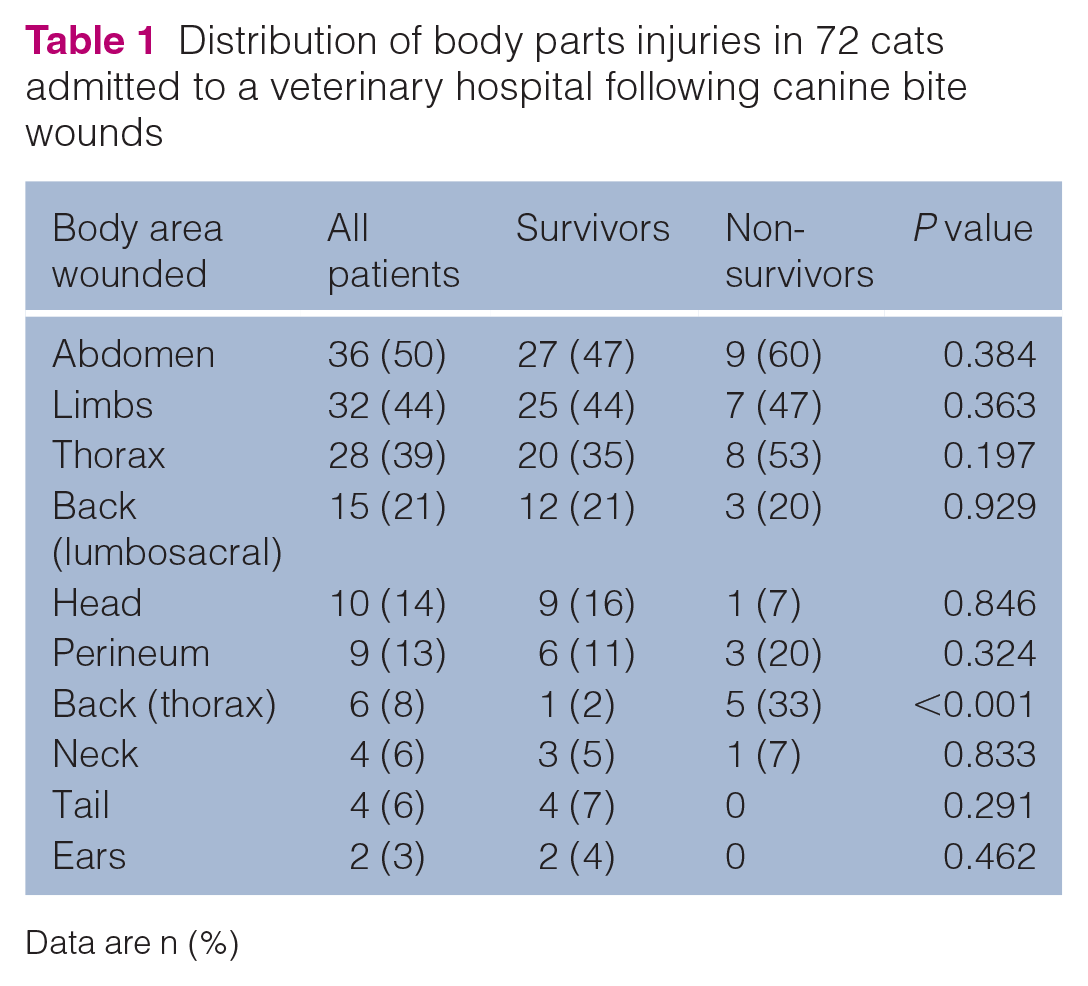
Data are n (%)
ATT scores and SSs
The ATT score was calculated for 69 cats (in three cats, missing data in the medical record prevented completion of ATT score calculation). The median ATT score was 4 (range 0–12), the median ATT score for non-survivors was significantly higher compared with survivors (9 [range 6–12] vs3 [range 0–8], respectively) (P <0.0001) (Figure 1). The probability for survival was plotted against the ATT score using an LRM (Figure 2). For every point increase in the ATT score, the odds for survival decreased by 3.16. An ATT of >5 had a 100% sensitivity and a 79% specificity for predicting non-survival (AUROC 0.958, 95% CI 0.91–1.00).

Box and whisker plots of the acute trauma triage (ATT) scores at presentation in cats sustaining dog bite wounds, demonstrating higher median scores in the non-survivors than the survivors

Logistic regression curve assessing the probability for survival against acute trauma triage (ATT) score. For every 1 point increase in the ATT score, the odds of surviving was decreased by 3.16
The median SS was retrospectively calculated for all 72 cats and was 3 (range 1–6); the median SS for non-survivors was significantly higher compared with survivors (5 [range 3–6] vs 3 [range 1–4], respectively) (P <0.0001) (Figure 3). The probability for survival was plotted against the SS using an LRM. For each point increase in SS, the odds of surviving decreased by 6.9 (Figure 4). An SS of >4 had a 60% sensitivity and a 100% specificity in predicting non-survival (AUROC 0.891, 95% CI 0.80–0.98).

Box and whisker plots of the severity of injuries scores (SSs) at presentation of cats sustaining dog bite wounds, demonstrating higher median scores in the non-survivors than the survivors

Logistic regression curve assessing the probability for survival against severity of injuries score (SS). For every 1 point increase in the SS, the odds of surviving was decreased by 6.9
There was a strong and significant correlation between ATT scores and SSs (r = 0.704, P <0.0001).
Clinicopathological data
Table 2 summarises haematological and biochemical analytes at presentation. Hyperbilirubinaemia, hypertriglyceridaemia, hyperglycaemia, hyperphosphataemia, elevated creatinine and increased activities of aspartate transaminase (AST), alanine aminotransferase (ALT) and creatine kinase (CK) were documented in all cats for which these parameters were measured. The only significant differences between survivors and non-survivors were in total protein (TP), albumin and ALT (P = 0.025, P = 0.032 and P = 0.032, respectively).
Selected haematological and biochemical analytes of cats suffering canine bite wounds at presentation to hospital
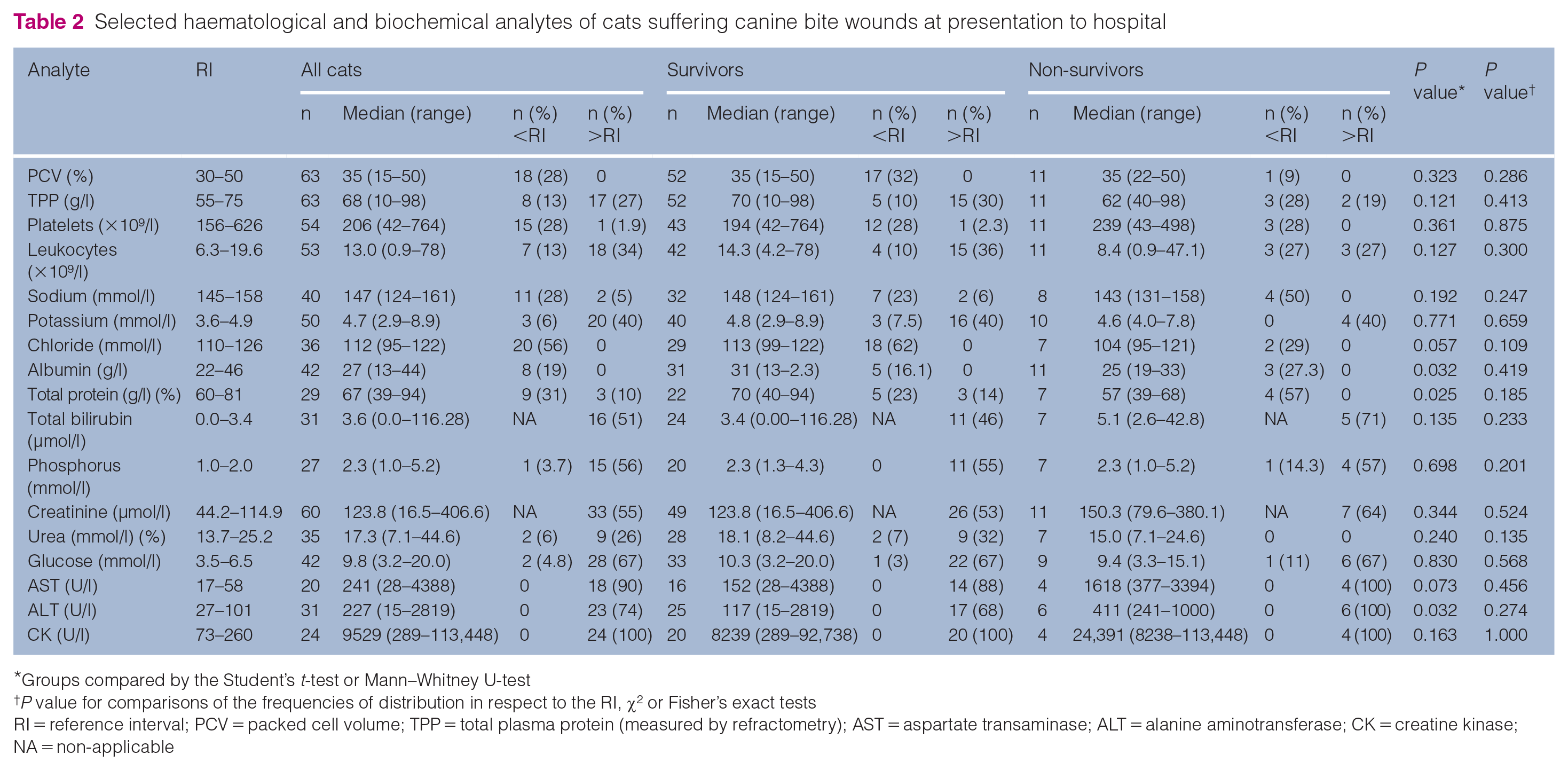
Groups compared by the Student’s t-test or Mann–Whitney U-test
P value for comparisons of the frequencies of distribution in respect to the RI, χ2 or Fisher’s exact tests
RI = reference interval; PCV = packed cell volume; TPP = total plasma protein (measured by refractometry); AST = aspartate transaminase; ALT = alanine aminotransferase; CK = creatine kinase; NA = non-applicable
Diagnostic imaging
Diagnostic imaging was performed in 62 (86%) of the cats. Radiography alone was performed in 39/62 (63%) cats, ultrasonography alone was performed in three (5%) cats, both radiography and ultrasonography were performed in 19 (31%) cats and one cat underwent a CT scan.
Figure 5 summarises the diagnostic imaging findings. Vertebral body fractures and body wall defects were significantly associated with a negative outcome (P = 0.005 and P = 0.046, respectively). There was no association between the number of radiographic lesions and outcome (P = 0.9).

Diagnostic imaging findings in cats sustaining dog bite wounds
Supportive treatment
IV crystalloids were administered to 66/72 (92%) of the cats, colloids (hydroxyl starch) in 10 (14%), mannitol in seven (10%), fresh frozen plasma (FFP) in three (4%), packed red blood cells (pRBC) in four (6%) and fresh whole blood (FWB) in three (4%). Administration of FFP and FWB were associated with a negative outcome (P = 0.001 and P = 0.046, respectively).
Antimicrobial treatment was administered to 65/72 cats (90%); the most commonly used antimicrobials were amoxicillin–clavulanate (64%), enrofloxacin (29%), and a combination of amoxicillin–clavulanate and enrofloxacin was used in 24% of the cats. Other antimicrobials used (alone or in a combination with other agents) included cefazolin (14%), clindamycin (11%), metronidazole (9%), marbofloxacin (6%), ampicillin (5%), long-acting amoxicillin (5%), ceftriaxone (3%), cefovecin–sodium (3%) and azithromycin (2%). Thirty of 65 (46%) cats were treated with more than one antimicrobial agent. Culture and susceptibility were obtained in 5/72 (7%) cases with one negative culture and isolations of Escherichia coli, Fusobacterium russii, Pseudomonas putida and a mixed bacterial culture.
Wound treatment and outcome
Median hospitalisation time was 2 days (range 0.0–13.0) with no significant different between survivors and non-survivors (P = 0.131). Fifty-seven cats (79%) survived to discharge, while 15 cats (21%) died or were euthanased owing to medical deterioration despite treatment (n = 9/72 and n = 6/72, respectively).
Four cats died/were euthanased prior to wound treatment. Of the remaining 68 cats, 34 (50%) were treated conservatively by clipping and local cleansing, 22 (32%) by local surgical debridement and 12 (18%) cats required an exploratory coeliotomy or thoracotomy (n = five [42%] had an exploratory celiotomy, one [8%] an exploratory thoracotomy and six [50%] had both). When comparing survivors with non-survivors, cats undergoing more aggressive treatments were significantly less likely to survive (P = 0.029).
Discussion
The present study describes the injuries, outcome and risk factors for mortality in 72 cats sustaining canine BWs. In the present study no differences were found regarding the sex of bitten cats, and the median age was 13 months, which is younger than previously reported.3,11 The young age of bitten cats can be explained behaviourally, as these cats have not yet learned to avoid dogs, or perhaps could not escape fast enough.
BWs were inflicted to all body areas, with the abdomen, limbs and thorax being the most common locations. No significant differences in survival were found between the various areas of injury, except those inflicted to the thoracic spine. Nevertheless, 93% of the non-survivors suffered BWs to the abdomen, thorax or both, in accordance with a previous studies, both in dogs and cats.2,11,24–26 Most cats in the present study (71%) suffered BWs to more than one body area; this is in line with a previous study of thoracic canine BWs in cats in which 73% of cats suffered multiple injuries. 11 Other studies of feline trauma have also reported polytrauma in 25–73% of patients.1,11,20,23 Cats are relatively small-sized victims, which predisposes them to multiple injuries. 10 A significant association was found between the number of injured body areas and survival, which is in agreement with the study by Hernon et al, 23 where 63% of feline trauma cases sustained polytrauma and were at greater risk of mortality. Moreover, a recent study found that multiple organ dysfunction syndrome is a frequent complication of polytrauma in cats and its development was associated with increased disease severity and worse outcomes. 24
The ATT score and SS have previously been shown to correlate with trauma severity and outcome.1,3,18,19,20,23,24 ATT was evaluated in cats suffering BWs, 3 whereas SS was evaluated in cats suffering vehicular trauma. In accordance with previous reports, the median ATT score was 4.3,18,19,24 The median ATT score for non-survivors was significantly higher compared with survivors. This agrees with studies in cats 24 and dogs, 27 where an ATT score of ⩾5 was most predictive of non-survival. Although the feline study involved solely polytrauma patients, it is interesting to note that 71% of our study population were polytrauma patients.
This is the first large-scale study to evaluate the injury severity scoring system in cats sustaining BW injuries. The median SS in the present study was 3 and, as previously reported,1,20,23 the SS for non-survivors was significantly higher compared with survivors. This agrees with previous reports in cats, where the mortality rate increased with increasing SS, and those assigned an SS ⩾5 having a higher mortality rate.20,23 Nevertheless, to date and to the best of our knowledge, no predictive performance of the SS has been evaluated and/or validated in injured cats, in general, and feline victims of BWs, in particular. The SS applied in the present study is a more ‘crude’ measure/index than the ATT and is based on objective clinical parameters with or without imaging; nonetheless, use of this injury-based SS system may provide some prognostic information related to mortality in cats following a traumatic event. Moreover, there was a strong and significant correlation between the ATT score and SS in the present study, warranting a continued assessment and validation of both scoring systems separately and in tandem as a tool for early recognition of severely injured feline patients.
Severe haematological or biochemical abnormalities were not found at presentation. This may reflect prompt arrival to the hospital (median of 2 h) and the fact that only laboratory parameters at presentation were evaluated, which did not allow for secondary body system damage to occur and be documented. An assessment of laboratory analyte alterations during hospitalisation and their association with survival may be needed in order to better characterise the haematological response of BW in cats.
Muscle enzymes (eg, CK, AST and ALT) were markedly elevated in all cats at presentation, with no difference in CK and AST between survivors and non-survivors. Elevations in muscle enzymes are expected as a result of muscle crushing and ischaemia. It was previously found that severe increases in CK activity are common in cats following polytrauma, although, similar to our findings, they were inaccurate outcome predictors. 28 Hyperglycaemia was also a common finding, with no difference seen between survivors and non-survivors. Hyperglycaemia commonly occurs along with stressful events in cats and is strongly correlated with changes in mean lactate and norepinephrine (noradrenaline) concentrations. 29 Catecholamine, lactate and cortisol release following a traumatic event may contribute to stimulation of gluconeogenesis, glycogenolysis and increased insulin resistance, which can lead to hyperglycaemia. In human patients with trauma, hyperglycaemia at presentation is significantly associated with increased morbidity and mortality rates.30,31 The clinical implication of stress hyperglycaemia in traumatised cat is unclear and additional studies are warranted.
Significant differences between survivors and non-survivors were found in total protein, albumin and ALT. In human patients with trauma, hypoalbuminaemia is an independent early predictor of death. 32 Albumin has important physiological functions,32–34 and hypoproteinaemia and/or hypoalbuminaemia at presentation may reflect an unapparent haemorrhage, the presence of systemic inflammatory response syndrome (SIRS), sepsis and severe tissue damage, and may potentially lead to decreased colloid–osmotic pressure and oedema, drug pharmacokinetics and acid–base disturbances, as well as delayed wound healing. Elevated ALT was also more common in non-survivors. Skeletal muscles in small animals contain a small amount of ALT, necessitating severe muscle injury for serum ALT to rise. ALT is considered more hepato-specific and therefore increased serum ALT activity usually reflects hepatocyte injury. 28 It is thus possible that increased ALT activity, in addition to muscle damage, also reflects liver damage, which could be sustained as a result of direct or blunt abdominal trauma, and this elevation might correlate with the severity of trauma.
Radiographic evidence of vertebral body fractures and body wall defects were significantly associated with outcome. All cats with vertebral body fractures had neurological deficits; all cats that had body wall defects were bitten in their abdominal area. As was reported in two previous studies,6,11 there was no association between radiographic evidence of thoracic lesions and outcome. In the present study there was no association between number of radiographic lesions and outcome.
There is little information in the veterinary literature regarding bacterial contamination, indications for antimicrobial treatment and choice of specific antibacterial agents in BWs.9,11,14,35,36 In two canine studies, the most common in vitro antimicrobial susceptibility was observed for sulfamethoxazole–trimethoprim and amoxicillin–clavulanate.14,36 Antibiotics were given as part of the initial treatment regimen to 90% of the cats in the present study. The most common antimicrobial drug used was amoxicillin–clavulanate, with 46% of cats treated with more than one antibiotic. Owing to the retrospective nature of the study and the lack of susceptibility information for most of the cases, it is unclear whether the decision to treat with more than one antibiotic was based on clinician preference, clinical judgement based on injury severity or the deterioration of the patient. Prospective studies to assess bacterial strains and the need for antimicrobial treatment in these cases are warranted.
In this study, most of the cats were managed conservatively. As expected, cats that required an exploratory coeliotomy or thoracotomy had an increased mortality rate. Controversy exists regarding indications for surgical intervention in thoracic bite wounds in animals. There are no large-scale studies evaluating whether surgical intervention is mandatory in cats with penetrating thoracic BWs. In a 2020 study that investigated 22 cats with thoracic BWs, 15/17 cats underwent an exploratory surgery, and of these 50% had an exploratory thoracotomy, 25% a wound exploration and 25% were either managed conservatively or transferred to their primary care practice. 11 The authors concluded that exploratory thoracotomy may have been unnecessary in some of these cases. In dogs, older literature advocates a conservative approach to the management of BWs,4,5 while more recent publications advocate for exploratory surgery.2,6,9,16,35,37
Seventy-nine percent of cats in the present study survived to discharge. To date, there are no publications reporting mortality rates in large populations of cats suffering canine BWs. In a study evaluating thoracic BWs in 22 cats, the survival rate was 73%. 11 The survival rate in a large population of cats suffering different causes of trauma was 83.5% 19 In that study, 90% of feline deaths were due to euthanasia, rendering mortality rates between the studies incomparable.
There are several limitations to this study, predominantly concerning its retrospective nature. The study was conducted in three different referral hospitals; cases were managed by different veterinarians, introducing potential variability in assessments and treatment. Cats were excluded when their owners declined treatment or hospitalisation, which can cause a selection bias. Lastly, the study, although the largest yet, included a relatively limited number of cats, thereby limiting the power of statistical analyses.
Conclusions
Cats sustaining canine BWs have a good overall prognosis for survival to discharge. High ATT score, high SS, multiple body area injuries, penetrating injuries, radiographic evidence of vertebral body fractures and body wall abnormalities, as well as hypoproteinaemia and elevated ALT, are negative predictors of survival.
Footnotes
Author note
A portion of this manuscript includes some results of a DVM dissertation, submitted by Dr O Madhala to the Koret School of Veterinary Medicine, Hebrew University of Jerusalem, Israel.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.