
Abstract
Objectives
The aim of this study is to describe the presentation, surgical management and perioperative outcome of cats with acetabular fractures.
Methods
Case records and radiographs of cats with acetabular fractures were reviewed from presentation to the end of follow-up. Surgical technique, complications, radiographic reduction and the presence of neurological deficits were recorded.
Results
Sixteen cats with 17 acetabular fractures met the inclusion criteria. All fractures were associated with concurrent orthopaedic injuries. All cats were either moderately or severely lame on presentation. Five fractures were stabilised using screws, wire, pins and polymethylmethacrylate, nine were repaired using a straight dynamic compression plate and three were repaired using a locking plate. Two of seven cats that were neurologically normal prior to surgery developed transient neuropraxia following surgery. There were three major complications and no minor complications. At the end of follow-up 3/16 cats had full function, whereas 13/16 had acceptable function.
Conclusions and relevance
All cats undergoing surgical stabilisation of acetabular fractures returned to full or acceptable function by the end of the follow-up period and there was a low number of intraoperative and short-term complications. Neurological deficits were common preoperatively, but the majority of these deficits had resolved by follow-up.
Introduction
Pelvic fractures are a common occurrence in cats, representing 20–22% of fractures in published studies.1–4 Of these, acetabular fractures comprise 17.5–26%, are commonly unilateral and often two-piece.2,5 Despite this, there is a paucity of published material on the outcome of acetabular fracture repair in cats. Acetabular fractures are considered to be extremely challenging fractures for orthopaedic surgeons; 6 however, pelvic fractures managed conservatively often stabilise in their displaced positions, 7 which may result in long-term complications, including narrowing of the pelvic canal, obstipation, neurological deficits, degenerative joint disease and joint pain.1,8,9
Historically, the caudal third of the acetabulum in both the cat and dog was considered a region that did not contribute significantly to coxofemoral load share and as such non-displaced fractures in this region could be managed conservatively.10,11 Recent ex vivo studies evaluating the topography of the coxofemoral joint have refuted these findings in both the dog and cat,12,13 suggesting that all regions of the acetabulum are involved in weightbearing and, as such, fracture location should not be an important factor in deciding between surgical or conservative management. As acetabular fractures are articular, principles for treatment of articular fracture fixation should be followed, with emphasis placed on anatomical reduction, rigid internal fixation and inter-fragmentary compression.9,11,14,15
Several techniques have been described in in vivo studies for fixation of acetabular fractures in dogs, including the use of veterinary acetabular plates (VAP),10,16 figure-of-8 wire, screws and pins (SWP), 17 figure-of-8 wire, screws and pins augmented with polymethylmethacrylate (SWP-PMMA),18,19 and locking plates (LP), 20 with recent studies suggesting that SWP-PMMA and LP provide comparable stability to conventional or acetabular plates, without demonstrating superiority of any one technique.20,21 There are limited descriptions of acetabular fracture fixation in cats describing SWP, VAP and LP but with no comparisons of technique utility or outcome.5,22
While canine studies demonstrate variable results in the outcome of conservatively managed acetabular fractures,23,24 surgical stabilisation is associated with a good prognosis for return to function.15,16,25,26 A study of the long-term outcome of acetabular fractures in cats has shown that many cats develop painful hips and associated muscle atrophy when managed conservatively; 1 however, in a recent paper on pelvic trauma in cats, only 50% of acetabular fractures were managed surgically, 5 despite the indications for surgery. The aim of this study is to describe the presentation, surgical management and perioperative outcome of cats with acetabular fractures. 27
Materials and methods
The case records and radiographs of all cats presenting to Langford Veterinary Services, University of Bristol, between 2009 and 2017, with acetabular fractures were reviewed. Cases were excluded if primary surgical stabilisation was not attempted, if follow-up data (including radiographs) were not available at a minimum of 4 weeks postoperatively and if there had previously been surgery carried out on the affected coxofemoral joint.
Information recorded included signalment, weight, cause of injury, neurological assessment and lameness grade on presentation, surgical approach, implants used, immediate postoperative outcome and postoperative fracture reduction grade. Follow-up information was determined from clinical notes and radiographs obtained at 4–12 week follow-up appointments. Information recorded included fracture reduction grade, lameness grade, neurological assessment and subjective clinical outcome. 22
Acetabular fracture reduction was evaluated following the subjective assessment scheme as described by Preston Stubbs et al. 21 Grade 1 indicated no visible gap or malalignment of the articular surface at the osteotomy site (anatomical); grade 2 indicated slight (<1 mm) gap, malalignment, or both, of the articular surface at the osteotomy site (near anatomical); and grade 3 indicated a >1 mm gap, malalignment, or both, of the articular surface (poorly reduced).
Fisher’s exact two-tailed test was used to analyse the statistical significance of differences in fracture reduction grade between methods of stabilisation.
Complications and subjective clinical outcome were classified as described by Cook et al. 27
Complications were classed as catastrophic (complication or associated morbidity that causes permanent unacceptable function); major (complication or associated morbidity that requires further medical or surgical treatment to resolve based on current standards of care); and minor (not requiring additional surgical or medical treatment to resolve [eg, bruising, seroma, minor incision problems, etc]).
Subjective clinical outcomes were full function (restoration to full intended level and duration of activities from pre-injury or pre-disease status [without medication]); acceptable function (restoration to intended activities from pre-injury or pre-disease status that is limited in level or duration and/or requires medication to achieve); and unacceptable function (all other outcomes).
Based on clinical notes, lameness was graded as mild (1/2 of 5), moderate (2/3 of 5) or severe (5 of 5). Similarly, hindlimb neurological deficits were graded as mild (sensory deficits), moderate (reduction in reflexes or mild ataxia) or severe (marked motor deficits).
Results
Records for 31 cats with acetabular fractures were identified. Of these, four were managed conservatively, two had femoral head and neck excisions performed on the affected joint, and 25 had surgery performed. Complete data were available for 16 cats with 17 acetabular fractures (Table 1). The age of the cats ranged from 11–100 months (median 36 months). Weight ranged from 2.7–5.8 kg (mean 3.7 kg). All fractures were associated with concurrent orthopaedic injuries: 13/16 had multiple (>1) injuries. All cats were either moderately or severely lame on presentation, and only seven were judged to be free of hindlimb neurological deficits on initial examination. All cats had a history of suspected or confirmed road traffic accident trauma. All fractures were operated on by board-certified veterinary orthopaedic surgeons.
Clinical data

DSH = domestic shorthair; MN = male neutered; XR = conventional radiography; S# = sacral fracture; P# = pubis fracture; Is# = ischial fracture; GT = gluteal tenotomy; DCP = dynamic compression plate; CT = computed tomography; I# = ilial fracture; PCN = pelvic canal narrowing; FN = female neutered; SIL = sacroiliac luxation; SWP = screw, wire and polymethylmethacrylate; F# = femoral fracture; LP = locking plate; PAX = Securos PAX plate; TO = greater trochanter osteotomy; Fib# = fibular fracture; M# = maleollar fracture; T# = tibial fracture; CFL = coxofemoral luxation; Spn# = spinal fracture; HA = hamstring avulsion; LCP = locking compression plate
Approach to the acetabulum was via a dorsolateral approach with gluteal tenotomies in 12 surgeries and by a dorsolateral approach with an osteotomy of the greater trochanter in five surgeries. 9 Five fractures were stabilised using SWP-PMMA, nine were repaired using a straight dynamic compression plate (DCP) and screws (Figure 1), and three were repaired using LP (one PAX plate, two locking compression plates [Figure 2]). Owners of all cats in the study were instructed to strictly cage rest animals for a minimum of 6 weeks postoperatively. Seven cats were judged to be neurologically normal prior to surgery; however, after surgery hindlimb neurological deficits were noted in 11 cats (two of which did not have deficits prior to surgery); the majority of deficits were short term and had resolved by the time of final clinical assessment.
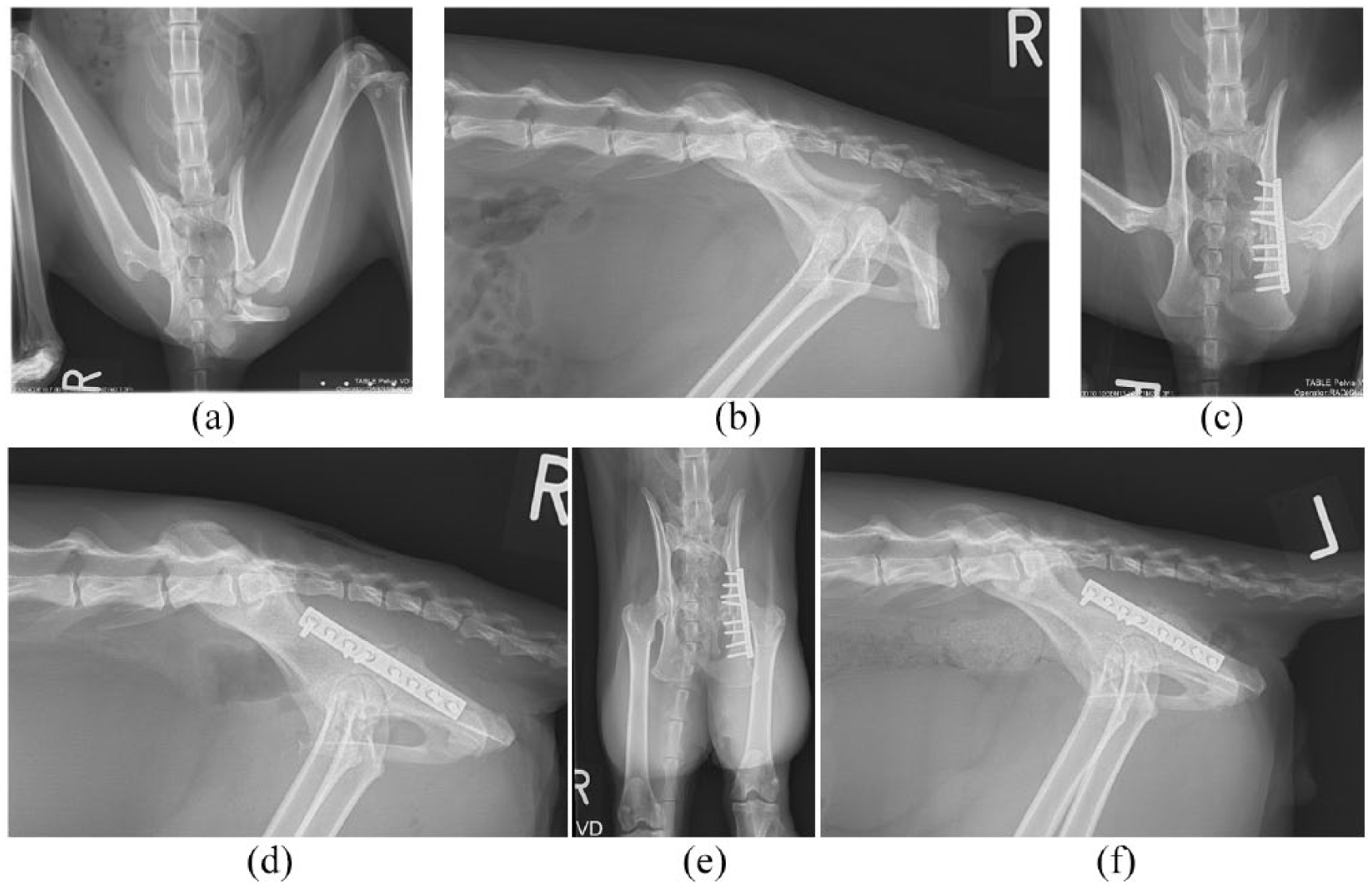
(a,b) Case 1 presented with a chronic comminuted left acetabular fracture, a non-displaced sagittal sacral fracture and right-sided neurological deficits. (c,d) The acetabular fracture has been stabilised using a straight dynamic compression plate and eight screws. (e,f) At the 11 week follow-up the fracture and implants are stable and there is evidence of bony healing
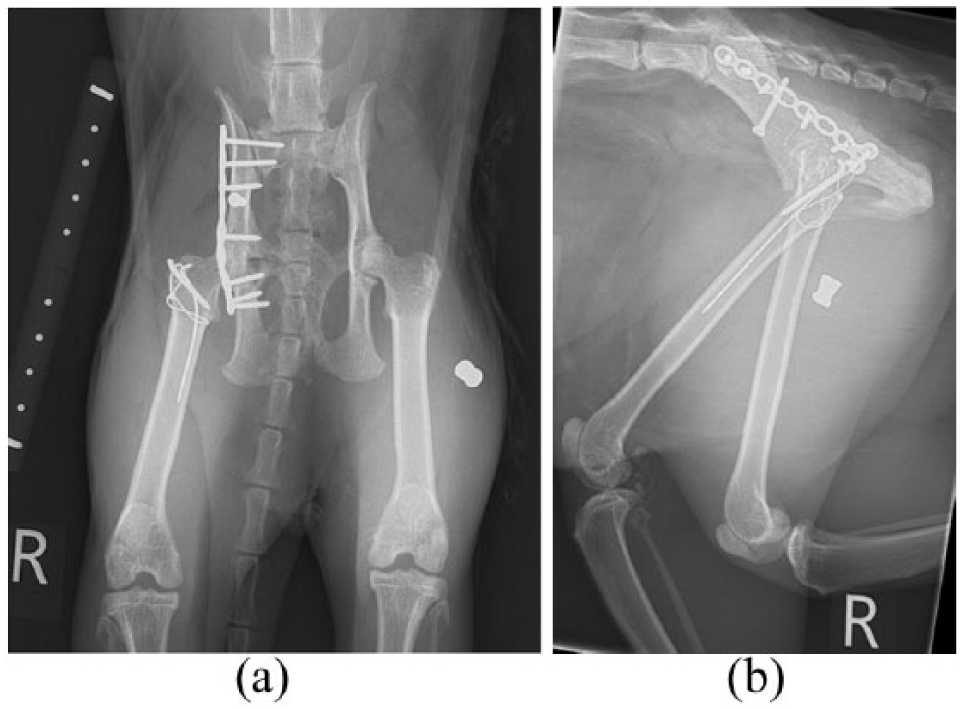
(a,b) Case 16: Immediate postoperative radiographs of a right-sided long oblique fracture of the ilial wing that included the acetabulum. The fracture has been stabilised using a combined locking compression plate and seven locking screws. A lag screw has been placed from ventral to dorsal to stabilise the ilial wing. The fracture was approached via an osteotomy of the greater trochanter, which was repaired using two pins and a figure-of-eight tension band wire. One pin (the longer, thinner pin) was found to have loosened and migrated at 6 week follow-up radiographs, requiring minor surgery to remove. There is a metallic pellet visible in the soft tissues, which was an incidental finding
All cats were clinically examined and had repeat imaging at 4–6 weeks. Fifteen cases were re-evaluated at the referral hospital, and one at the referring veterinary surgery. There was a mean follow-up of 55 days (range 34–121 days) (Table 2). Major complications included implant failure (two fractures), one requiring the cat to have a unilateral excision arthroplasty (Figure 3), and loosening of the trochanteric osteotomy pin (Figure 2), requiring pin removal. There were no minor complications recorded. At the end of follow-up 3/16 cats were judged from client history to have full function, whereas 13/16 had acceptable function.
Follow-up data

FHNE = femoral head and neck excision
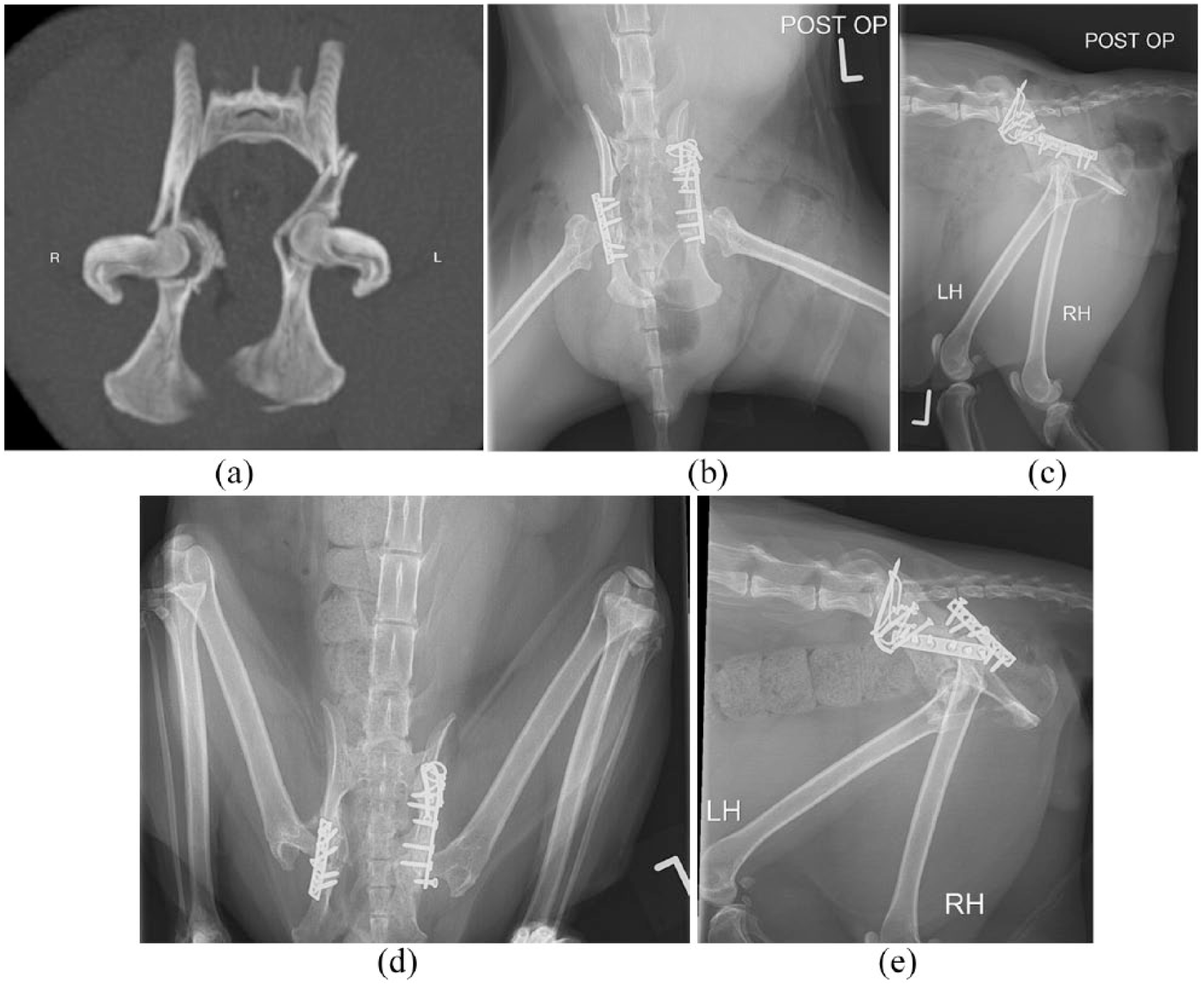
Case 2. (a) A preoperative CT scan demonstrated bilateral comminuted acetabular fractures. (b,c) Immediate postoperative radiographs. The acetabular fractures have been stabilised using straight plates; the ilial wing fracture on the left side has been stabilised using lag screws, pins and wire. The reduction is imperfect on the left side, with a step of approximately 1 mm and only two screws present caudal to the fracture line. On the right side there is poor reduction, with a step of >1 mm and only two screws present caudal to the fracture site. (d,e) Radiographs taken at 12 weeks postoperatively show loosening of the implants on the right side, with all screws cranial to the fracture backing out and no evidence of radiographic union. A right femoral head and neck excision was performed following these images. The left side appears to be stable, with evidence of radiographic healing, although the most caudal screw is backing out, likely due to insufficient screws caudal to the fracture line
Discussion
In this study all 16 cats that underwent surgical stabilisation of acetabular fractures returned to full or acceptable function by the end of the follow-up period and there was a low number of intraoperative and short-term complications, despite often challenging multi-trauma presentations. Neurological deficits were common preoperatively; there was a small increase in incidence postoperatively, but the majority of these deficits had resolved by follow-up. Anatomical reduction was more likely with simple fractures than with comminuted fractures.
Ten of the 16 cases had initial imaging by CT, which is the preferred method of imaging at this institution. While CT is not universally available and not necessarily superior to high-quality radiographs, it may be beneficial where there is uncertainty around complicated fractures (Figure 3), allowing multi-plane reconstruction and three-dimensional visualisation of fragments. This is particularly true for acetabular fractures, 28 providing greater sensitivity, greater definition of fracture fragments and allowing more accurate surgical planning. 9
Cats in this study demonstrated a 75% incidence of concomitant orthopaedic injuries outside the pelvis. This is within the range of 59–84% described in other surveys of pelvic fractures in cats.5,29 This likely reflects the high-energy nature of pelvic fractures, which were all associated with confirmed or suspected road trauma in this study.
All fractures were approached by a dorsolateral approach to the acetabulum with either trochanteric osteotomy or gluteal tenotomies performed at the discretion of the surgeon. Both of the described approaches are considered to be equally as good at enabling visualisation of the dorsal aspect of the acetabulum and the sciatic nerve, 30 and both resulted in similar outcomes in our study, although one case with a trochanteric osteotomy did require a second surgery to remove a loose osteotomy pin (Figure 2).
Neurological deficits were a common finding in cats in our study – found in 9/16 cats on presentation and occurring postoperatively in 2/7 cats that were neurologically normal on presentation. This was a much higher incidence than in a recent study of pelvic fractures in cats by Meeson and Geddes, 5 in which pre- and postoperative rates of neuropraxia were 23% and 13%, respectively, although Meeson and Geddes’ study included all cases of pelvic fractures in cats, rather than being specific to acetabular fractures.
As our study is retrospective, neurological deficits were often not fully investigated; however, sciatic neuropraxia is likely the underlying cause of the majority of these deficits. The sciatic nerve is particularly vulnerable to damage from movement of acetabular fracture fragments prior to stabilisation, or manipulation of the sciatic nerve at surgery on the dorsal aspect of the hip, 31 as it is closely associated with the medial surface of ilium at this point; 32 although as many of these fractures were multi-trauma, it is not possible to exclude concurrent injuries (eg, spinal or sacral fractures) as the cause of the deficits. Even with good visualisation, acetabular fractures often require manipulation of the sciatic nerve to allow implant placement, 30 which is likely the cause of the two cases of temporary postoperative neuropraxia.
Only 3/16 cats had persistent nerve damage at follow-up, all of which had presented with initial nerve deficits, so it is unlikely that any surgeries in this case series caused persistent iatrogenic nerve deficits. It is also possible that these deficits might have been seen to resolve had longer follow-up been possible. 32
Nine fractures were stabilised using bone plates (Figure 1), none of which were acetabular plates. This is in contrast to a recent study, in which 2/5 feline acetabular fractures were stabilised using acetabular plates. 5 Acetabular plates in theory require less contouring than straight plates;9,14,26 however, they need to be combined with additional implants if the fracture extends further cranially along the ilial wing or caudally into the ischium, which requires significant bone stock both cranial and caudal to the acetabulum for screw placement. Acetabular plates are, as a result, mainly of benefit for simple mid-acetabular fractures. Straight plates are more adaptable to comminuted fractures and fractures extending away from the acetabulum, 26 such as long oblique ilial/acetabular fractures, which are common in cats. 3 Compared with the canine pelvis, the comparatively straight topography of the feline dorsal ilial wing lends itself to the use of a straight bone plate, as minimal contouring is required. In this study, the straight DCP plate was the most commonly used implant for acetabular fractures in cats and continues to be so at this institute.
Three pelvic fractures in this series were repaired using LP (Figure 2) and four were repaired using SWP-PMMA (Figure 4). These techniques have potential advantages over straight plates for specific types of fractures. SWP-PMMA application is described as being simpler than conventional plating, consistently achieving anatomical reduction in simple acetabular fractures. 18 Locking plates reduce the need for plate contouring, often one of the most challenging aspects of acetabular fracture surgery, and also have the potential for increased stability in poor-quality, highly comminuted fragments. 20 The most recent case series of the surgical management of acetabular fractures in dogs (Butterworth et al) 23 described 21 surgical repairs, none of which utilised SWP-PMMA or LP. However, the Butterworth et al study dates from before the publication of several cadaveric studies, which subsequently suggested that SWP-PMMA and LP may give equivalent stability to conventional plate fixation.20,21 To our knowledge the only feline case series describing the surgical stabilisation of acetabular fractures describes surgical management of five acetabular fractures, two with acetabular plates, two with locking/reconstruction plates and one with SWP-PMMA. 5 Case numbers are low but, in conjunction with our results, this would suggest that clinical use of SWP-PMMA and LP is becoming more common for repair of acetabular fractures.

(a) Case 3 presented with multiple pelvic fractures and a right sacroiliac luxation. (b,c) Immediate postoperative radiographs. The acetabular fracture has been stabilised with four screws, wire and polymethylmethacrylate. (d,e) Six week follow-up radiographs. The fractures and implants are stable and there is evidence of bony healing
In this study, anatomical fracture reduction (grade = 1) was achieved in 3/8 fractures managed with straight plates, 3/5 fractures managed with SWP and 0/3 fractures managed with LP. Fractures were significantly more likely to have anatomical reduction if they were classified as simple on presentation, rather than comminuted (P = 0.0063). All simple fractures were managed with a fixation method capable of compression, either SWP or a straight plate, whereas locking implants were reserved for fractures where comminution was present. Variation in reduction grade between different fixation methods therefore likely reflected original fracture configuration rather than efficacy of technique.
All cats were judged to have full or acceptable function at 4–6 week follow-up. This compares favourably with similar case studies in dogs, which report 76–80% acceptable function.23,25 It is interesting that even in the case that required joint salvage, the owner felt the cat had acceptable function. This perhaps reflects the ability of cats to tolerate a degree of joint dysfunction or lameness, or owners’ inability to accurately recognise lameness in cats. The use of this subjective outcome measure, encompassing a variety of disease states, is a limitation of our study, along with the short follow-up, meaning that no conclusions can be drawn about the medium-to-long-term functional outcome of cats with surgically treated acetabular fractures; however, it does demonstrate a useful measure of client satisfaction. Butterworth et al subjectively observed that in acetabular fractures in dogs, surgically managed cases continued to improve up to 16 weeks postoperatively. 23 It could therefore be expected that some cats in this study will have continued to improve beyond the end of follow-up.
This study demonstrated a low number of surgical complications, with one case requiring joint salvage (Figure 3), one requiring postoperative medical management and one requiring removal of a trochanteric osteotomy pin (Figure 2). The case requiring joint salvage was the only case in this study to involve bilateral fractures. Acetabular fractures are articular fractures and therefore there is likely to be some long-term joint dysfunction, even if the joint is perfectly anatomically reconstructed. 15 In our study only 6/17 fractures had radiographically perfect reconstruction. This is comparable to human studies of acetabular fracture fixation,6,33 reflecting the challenging nature of reconstructing these fractures. In long-term studies in humans, rates of joint salvage after acetabular fracture repair are described as 8–10%;6,33 shorter-term studies in dogs describe rates of 0–14%.16,23,25 However, even if reduction is imperfect, surgically reconstructed acetabular fractures would appear to have a better prognosis than those managed conservatively, 15 and the low number of observed perioperative complications is a useful consideration for decision-making in these cases.
Conclusions
This study demonstrates positive perioperative clinical outcomes in a group of cats with acetabular fractures stabilised with a variety of fixation methods. It shows low intraoperative and short-term complication rates and consistently acceptable outcomes, despite often challenging multi-trauma presentations.
Footnotes
Acknowledgements
The authors would like to thank Alex Bradnick for help with data collection and Alison Major for help with preparing images for publication.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.