
Abstract
This study deepens knowledge on the implementation of core values in servicescapes by analyzing how core value trade-offs and spillovers occur within servicescapes and how vulnerable stakeholders cope with them. We use an explorative approach and draw on rich data collected in two nursing homes. Our study demonstrates how the autonomy-security trade-offs originate in different dimensions of the servicescapes. Further analysis reveals how individual customers may conflict with the core values and core purposes of the respective servicescapes. We also contribute to the discussion on customer vulnerability by considering vulnerability in the extended customer entity and by identifying the active coping mechanisms of vulnerable customers. Practitioners can increase the quality of care by identifying and taking into account the core values of both vulnerable primary and secondary customers and by deliberately supporting their coping with core value trade-offs and spillovers.
She told me she was glad to be in a safe place—if there’s anything a decent nursing home is built for, it is safety. But she was wretchedly unhappy.
Safety and security have recently been recognized as important elements within servicescapes (Siguaw, Mai, and Wagner 2019), and questions around securing vulnerable individuals, such as the elderly in nursing homes, became especially urgent during the global COVID-19 crisis (Wang et al. 2020). Security, particularly related to vulnerable consumers, has been emphasized in transformative service research (TSR; e.g., Blocker and Barrios 2015; Rosenbaum, Sweeney, and Massiah 2014). However, even though TSR concerns “creating uplifting changes and improvements in the wellbeing of consumer entities” (L. Anderson et al. 2013, p. 1204), the impact of increased security on well-being is not unambiguous. Vulnerable consumers also require a sense of autonomy and a certain degree of actual autonomous agency (Sharma, Conduit, and Hill 2017). Even though both core values—security and autonomy—often seem to be the very basis of each other (autonomous individuals feeling secure and vice versa; cf. Abma et al. 2012), paradoxically, these two values often exist in tension with each other when it comes to vulnerable consumption (e.g., Preshaw et al. 2016).
Consequently, well-meaning transformative services may generate unintended consequences (e.g., L. Anderson et al. 2013; Rosenbaum et al. 2011): Behavior intended to increase security may diminish autonomy (Ball et al. 2004; Slettebø 2008), and attempts to enhance autonomy can lead to decreased security (Nyström and Segesten 1994; Woolford, Weller, and Ibrahim 2017). Furthermore, core value trade-offs can affect other stakeholders or third actors (cf. L. Anderson et al. 2013), thereby enlarging the sphere of unintended consequences. These spillover effects in the multistakeholder context have yet to be empirically explored (Finsterwalder and Kuppelwieser 2020).
The existing research on servicescapes largely concentrates on how servicescapes, or the specific dimensions in servicescapes, influence customers’ behavioral intentions, emotions, or experiences (Han, Kang, and Kwon 2018; Mari and Poggesi 2013). Even though the integration of values into service processes has been acknowledged (Kernaghan 2003; Williams 2016), core values have been given very little consideration in servicescape research. The similarity in core values held by multiple individuals in a given servicescape has been shown to enhance bonding between a person and a place (Rosenbaum et al. 2007), and recently, safety has been proposed as one of the dimensions of servicescapes (Siguaw, Mai, and Wagner 2019). However, there is a need to deepen the servicescape knowledge in terms of creating and coping with core value trade-offs. Consequently, the purpose of this study is to analyze how core value trade-offs and spillovers occur within servicescapes and how vulnerable stakeholders cope with them.
The context of the study is nursing homes since they can be seen as servicescapes in which the trade-off between autonomy and security prevails (Jakobsen and Sørlie 2010). Nursing homes provide service environments (in many cases, even domestic-style environments) with 24-hour care to persons who have complex health needs and increased vulnerability and who thus require assistance with the activities of daily living (Sanford et al. 2015). The autonomy experienced by the elderly seems to contribute to their mental well-being (Barkay and Tabac 2002), especially in cultural contexts that highlight autonomy as a cornerstone of living a good life and as the foundation of good care (cf. Harnett and Greaney 2008). On the other hand, caregivers who are responsible for the elderly feel the need to protect the physical well-being of their clients and to provide a safe and secure environment for them (Nelson, Allen, and Cox 2008). Consequently, they face the dilemma of balancing autonomy and security (Goethals, de Casterlé, and Gastmans 2013).
At the same time, the nursing home setting also seems to be a good example to use to explore the core value tensions that often exist in health care services providing negative services; that is, services in which customers need to cope with unwanted or stressful situations to gain the necessary benefits of the service (Miller et al. 2009; Morgan and Rao 2006). Two important value spheres that come into play in any care-related servicescape are (a) autonomy and (b) security. As care-related servicescapes usually fulfill the needs of customers who did not choose to enjoy the provided services but are in need of these services, we will gain special knowledge about how the core values of autonomy and security are interpreted within an environment in which any customer per se has a certain deficit in at least one of the two value spheres: A person who enters a nursing home, by definition, is neither capable of fulfilling all the culturally shared criteria of an autonomous person nor of living in a safe and secure manner. There are usually serious threats to the individual’s physical and psychological safety that make them become a customer within a caregiving environment, and they actually require these kinds of deficiencies to be eligible to move into care facilities.
In nursing homes, the core values of autonomy and security have been studied primarily from the caregivers’ perspective (e.g., Preshaw et al. 2016; van Thiel and Van Delden 2001), whereas studies from the perspective of the elderly are sparse (e.g., Ball et al. 2004). Studies examining these values from the multiple perspectives of caregivers, the elderly, and the family members of the elderly are even scarcer (e.g., Wikström and Emilsson 2014). Hence, we employ a multistakeholder perspective by utilizing qualitative research methods to explore autonomy and security provided by the servicescapes in two nursing homes.
Our study contributes to TSR in three important ways. First, we contribute to the servicescape research (e.g., Rosenbaum and Massiah 2011) by showing how the core value trade-offs originate from different dimensions of the servicescape and how individuals’ core values may conflict with the core values of the servicescape that they find themselves in. Second, we contribute to multistakeholder research (e.g., Johns and Davey 2019; McColl-Kennedy, Cheung, and Coote 2020; Pizam and Tasci 2019) by showing the unintended consequences produced by spillovers and by revealing the incongruent needs of primary and secondary customers. Third, we contribute to the discussion on customer vulnerability (e.g., Hill and Sharma 2020; Leino 2017) by considering vulnerability in the extended customer entity, identifying the coping mechanisms of vulnerable customers, and by highlighting the specificities of care-related servicescapes that offer services that customers need but do not want—which is a condition that breeds ambivalence and conflict and demands creativity from all involved persons.
The article begins with a discussion on the existing literature concerning vulnerable primary and secondary customers in servicescapes, the trade-offs between autonomy and security, and the spillover effects faced by vulnerable customers. This is followed by a description of and justification for the qualitative methods used in the empirical study. Next, the findings of the empirical research are outlined and discussed. The article concludes with theoretical and managerial implications and research limitations, leading to suggestions for further studies.
Theoretical Background
Vulnerable Primary and Secondary Customers in Servicescapes
Customer vulnerability can be defined as either an experienced or observed “state in which consumers are subject to harm because their access to and control over resources are restricted in ways that significantly inhibit their ability to function in the marketplace” (Hill and Sharma 2020, p. 551). In itself, being old, for instance, does not necessarily mean being vulnerable if one is able to access and control individual resources (e.g., money and health), interpersonal resources (e.g., social capital and belonging), and structural resources (e.g., engagement in business practices and access to available goods and services; Baker, Gentry, and Rittenburg 2005; Hill and Sharma 2020).
The degree of customer vulnerability may vary, may be self-perpetuating, and may also be contagious for other customers. It can be experienced or observed in a continuum ranging from more extreme vulnerability to less extreme vulnerability (Hill and Sharma 2020). Vulnerability can be permanent or it can diminish, even disappearing if given sufficient time (Pavia and Mason 2014). It may also extend from those being primarily vulnerable (e.g., the elderly suffering from dementia) to those who are secondarily vulnerable (e.g., their family members), as it reflects on the access to and control of their resources, behavior, and well-being (Baker, Gentry, and Rittenburg 2005; Leino 2017; Pavia and Mason 2014). Pavia and Mason (2014) propose that there are often more resources for primarily vulnerable than for secondarily vulnerable individuals, which is why the secondarily vulnerable may seek help from systems designed for the primarily vulnerable. Networks and ecosystems (e.g., Akaka, Vargo, and Lusch 2012; Heinonen and Strandvik 2015) have been studied to a great extent, but service providers’ specific acknowledgment of secondarily vulnerable individuals, thus secondary customers, still seems to be inadequately explored—neither as such nor in relation to the primarily vulnerable customers. In particular, the customer viewpoint and expectations toward the service provider in this extended customer entity lack attention.
Hence, servicescapes may have to deal with the needs of both vulnerable primary and vulnerable secondary customers. Originally, the term “servicescape” was used to mean a physical setting including the ambient conditions, spatial layout and functionality, and signs, symbols, and artifacts (Bitner 1992). Initially, the research on servicescapes emphasized how single physical setting cues shape the expectations, behaviors, and satisfaction of customers and employees (Bitner 1992; Mari and Poggesi 2013). However, people are prone to holistically responding to the physical setting cues, and therefore, researchers have tended to increasingly focus on the impact of multiple cues (Mari and Poggesi 2013).
Furthermore, only concentrating on the physical setting can be regarded as too narrow a perspective since other aspects of the service consumption setting may also influence customer and employee behaviors (Mari and Poggesi 2013; Rosenbaum and Massiah 2011). Consequently, Rosenbaum and Massiah (2011) expanded the servicescape framework to contain, in addition to the physical dimension, three other dimensions: the social (employees, customers, social density, and the displayed emotions of others), socially symbolic (signs/symbols and objects/artifacts), and natural (being away, fascination, and compatibility) dimensions. Recently, it has been suggested that the servicescape should also include a separate safety-related dimension (consisting of crime, hazard, and fear) since safety has been largely ignored in servicescape research (Siguaw, Mai, and Wagner 2019).
Servicescape research on transformative services has shown the influence of servicescape dimensions on the well-being of vulnerable customers. The range and organization of dimensions have been found to influence and improve the well-being of hospital patients (Hamed, El-Bassiouny, and Ternès 2019) and participants in the health care system (S. Anderson, Nasr, and Rayburn 2018). It has also been shown how cancer centers and senior centers improved their patrons’ well-being by utilizing the natural (restorative) dimension of servicescapes in relieving the fatigue associated with illness (Rosenbaum, Sweeney, and Massiah 2014; Rosenbaum, Sweeney, and Smallwood 2011).
It has been proposed that since the servicescape serves the needs of various different stakeholders, and since these stakeholders also interact with each other, research should adopt a multistakeholder perspective on servicescapes (Colm, Ordanini, and Parasuraman 2017; Pizam and Tasci 2019). TSR has also indicated that multistakeholder interactions enhance transformative outcomes for vulnerable customers (Johns and Davey 2019). However, researchers rarely scrutinize the viewpoints and needs of both primary and secondary customers, instead only considering the actions and outcomes of primary customers and omitting the specific needs of vulnerable secondary customers who should be an integral part of the service design (Leino 2017).
Autonomy and Security of Vulnerable Customers—Trade-Offs and Spillovers
Definitions of autonomy vary, and its distinction from related concepts, such as independence, self-determination, freedom, and agency, is often blurred. In line with earlier studies (e.g., Ball et al. 2004; Perkins et al. 2012), we follow Hofland’s (1990) conceptualization and view autonomy as consisting of physical, psychological, and spiritual dimensions. The physical dimension concerns the freedom of mobility, physical independence, and the use of the least restrictive environment (Hofland 1990), and it might be called independence (Ball et al. 2004). The psychological dimension relates to control over one’s environment and choice of options. The spiritual dimension refers to continuity in one’s sense of personal identity over time and decision making that is consistent with an individual’s long-term values and life meaning (Abma et al. 2012; Hofland 1990).
Autonomy develops in relationships (van Loon et al. 2019) and is shaped by individuals’ perceptions of themselves in relation to their environment (cf. Lefcourt 1973). Consequently, we can speak about perceived autonomy, which is a complex, dynamic, and relational concept (van Loon et al. 2019). However, it seems that the prevalent understanding of autonomy does not entail the complexities involved in caring for vulnerable people with diminished capacities caused by, for example, dementia or depression (cf. Harnett and Greaney 2008; Welford et al. 2012)—or simply caused by the fact that people in nursing homes have a deficit in handling their lives by themselves per definitionem.
For instance, a study on nursing homes indicated that perceived autonomy was influenced by whether the servicescapes were regarded as places to live or places where one is cared for. Individuals taking the first perspective advocated autonomy and self-help, whereas those adopting the latter perspective emphasized security: the protection of residents’ physical well-being and the prevention of injuries (Wikström and Emilsson 2014). Whereas many elderly are afraid of losing all their autonomies in nursing homes (Harrefors, Sävenstedt, and Axelsson 2009), the security provided by nursing homes is one of the primary motivators behind the decision of many residents and their family members to move themselves or their loved ones into such facilities (Slettebø 2008). In any case, providing autonomy without compromising on security is a considerable challenge in elderly care, particularly for those residents who suffer from dementia (Harnett and Greaney 2008; Jakobsen and Sørlie 2010).
In practice, there is often a trade-off between security and autonomy in servicescapes for vulnerable customers, and autonomy tends to be overridden to ensure security and safety (Dunworth and Kirwan 2012; Preshaw et al. 2016). The trade-off is likely to lead to unintended consequences when autonomy decreases due to the actions taken to increase security and vice versa (e.g., Ball et al. 2004; Woolford, Weller, and Ibrahim 2017). In a multistakeholder context, the trade-offs experienced by one actor can create unintended positive or negative spillovers in other actors. Spillovers go beyond the services’ intended outcomes, and they may be fairly immediate or may be realized with a delay. Calls have been made for further research on these spillover effects, especially the negative ones (Finsterwalder and Kuppelwieser 2020).
Vulnerability can be seen to influence the ways in which customers cope with both trade-offs and negative spillovers. Coping is a process of making adaptations to manage and respond to the demands of the environment in order to maintain or enhance feelings of well-being (Zeitlin, Williamson, and Rosenblatt 1987). Hill and Sharma (2020) divided the coping mechanisms of vulnerable customers into nondefensive and defensive mechanisms; the former refers to customers’ tendencies to submit to their situation, and the latter refers to their tendencies to resist or combat their situation. Nondefensive coping has been further divided into giving up (resignation and acquiescence to the conditions) and giving in (accepting or embracing consumption restrictions as their own fault and conforming to the current situation). Defensive coping includes transcending (rising above the circumstances), rebelling (disrupting and damaging the circumstances), and creating new structures (establishing or exploiting contexts in which customers have greater possibilities for control; Hill and Sharma 2020). As there are various coping mechanisms, and as a multistakeholder context is likely to add more intricacy to their utilization, we decided to adopt a qualitative research approach that allowed us to take these complexities into account.
Method
We utilized qualitative research methods to explore the trade-offs and spillovers of autonomy and security and the coping of vulnerable stakeholders in servicescapes, the latter being represented by two selected Finnish nursing homes in this study. The selection criteria for the nursing homes were related to ownership, operating history, and environment. First, both homes are run by well-established, private companies offering nursing services for elderly people. Hence, operating in the private sector presumably makes them emphasize the core human values more than average, as these companies are particularly keen on keeping customers happy so that they remain in-house as paying customers. Second, the history, size of the parent company, and operating environment differed in the chosen nursing home units, which contributed to more heterogeneous case sampling for our study. The company Diamond (a pseudonym) has two units, of which we selected the one established in the 1990s in a town with 190,000 inhabitants. The company Pearl (a pseudonym) has several units, of which we selected the one opened in the 2010s in a town of 40,000 inhabitants. This enhances opportunities to explore a variation in servicescape implementations and thereby improves the grounds for the transferability of the findings.
As the research dealt with vulnerable individuals, a supporting ethical statement was first obtained from the Research Ethics Committee at our university. The residents and their family members were then informed about the study. The residents (or family members in cases where the residents had impaired decision-making capacities) were left to decide whether they wanted to take part, and the signed permissions for interviewing residents were acquired both from relatives and residents (regarding ethics and informed consent, see Israel and Hay 2006). If the decision concerning resident participation was made by a family member, the resident’s willingness to participate was also ascertained prior to the interview stage. It was emphasized that participation was voluntary, and the informants were ensured of confidentiality, and that they could withdraw at any time without any negative consequences regarding their care and treatment.
We focused on the hows of the creation and implementation of, and coping with, the core values of autonomy and security through servicescapes. The flexibility of qualitative methods enables the richness and diversity of understanding the implementations of the abstract concepts to be captured. Thus, we undertook a field study with ethnographical features (Berg 2004). The data were gathered through interviews in everyday social settings at the nursing homes and through observations (making notes in notebooks)—a recommended method for studying autonomy (van Loon et al. 2019). The observations took place during two sequential periods (at Pearl in 2014 and at Diamond in 2018) because after undertaking our data collection and preliminarily analyzing the results from one nursing home, we felt there was a need to enrich the analysis and validate certain results by studying the importance of the continuity of care in another nursing home (see Table 1).
Data Collection.

Pearl had 12 residents at the time of the study. Diamond had 36 residents. Most of the residents entered the nursing homes following a decision made by their family members; some came willingly, some reluctantly. A majority of the residents suffered from dementia, but some were only physically frail. The main difference in the entry between the homes was that, in Pearl, most residents came from another (more hospital-like) nursing home, whereas in Diamond, most came from their private homes. Both homes offered a single room with bathroom facilities for each resident. In Pearl, the big, shared room had a kitchen, dining room, and a TV corner. In Diamond, the shared spaces consisted of smaller kitchen spaces and living room spaces with sofas, a TV, bookshelf, piano, and some homely items.
In the interviews, we studied the autonomy and security created for the residents. To understand these aspects fully, we also needed to engage their family members and nurses as informants since many residents were not able to express themselves fully. Thus, we were also able to triangulate the viewpoints of the residents, family members, and nurses even on an individual basis. The interviews with the residents and family members were based on predetermined themes (on nursing home conceptions, individual home-related histories, and the experiences of nursing home services). The interviews were recorded if the interviewees agreed to this.
For the interviews of the residents, the time and place of the interview were planned together with the nurses to optimally suit the residents’ normal daily routines and habits. This is why these interviews took place in the residents’ own rooms, in public indoor spaces, or outside in the inner yard. The average length of these interviews was only half an hour in order not to cause too much fatigue for the interviewees. The interviews of the family members of the residents were arranged at Pearl and Diamond on such days and times when the family members normally visited the residents, with the length of each interview varying from 1 to 2 hours. Fifteen residents and 27 family members were interviewed for this study. The low number of residents is due to the majority of them having severe memory disorders that made it impossible to interview them. Further, altogether, 22 nurses were interviewed on interpreting the others’ trade-offs and spillovers. The interviews were conducted during their working hours, carefully avoiding disruptions to their daily routines and leading to a great variation (15 minutes to 2 hours) in the length of these interviews. The nurses interviewed at Pearl had 1–15 years of working experience in care services (on average, over 6 years). Except for one nurse, all of them had worked in several other nursing homes before. In Diamond, the nurses’ experience in care services varied between 2 and 30 years (13 years on average). All nurses interviewed had at least 1 year of experience working at Diamond.
The observation data were collected systematically on multiple separate days, in Pearl in June and October by four researchers, and in Diamond between May and October by two researchers. The observations concentrated on the daily life of Pearl and Diamond and the interactions and behaviors taking place between the residents, family members, and nurses. The researchers wrote field notes on their observations of daily life and of the informal discussions at the nursing homes, and they drew individual charts of private rooms and public spaces. The prolonged time for the data collection made it possible to observe the development in customers’ perceptions and experiences regarding the service environments, both at the cognitive and emotional levels. The more time the researchers spent in the place, the more familiar they became with the informants, thus decreasing their mistrust toward outsiders. The informal discussions with residents and their relatives took place on a daily basis.
The data were initially analyzed at the time of the interviews and when observing the service environment. Nevertheless, the transcribed data were analyzed in three phases. First, the researchers read the transcripts several times to produce an overview of the service environment emerging from the data. Based on this review, a loose frame of analysis was determined, including the concepts of autonomy/lack of autonomy, security/lack of security, and the source of the information (resident, family member, and nurse). Second, the data, including the observational notes, were imported to NVivo 12, where they were coded using the abovementioned concepts. The inductive coding was utilized to allow novel interpretations and classifications to arise from the data. The aim was to find upper-level categories for single subcategories that could finally be integrated into some more abstract patterns, also illustrating their intertwining relationships. This required several iteration cycles, where the terms and codes (based on quotations) were combined, discussed, and finally conceptualized by the researchers (cf. Gioia, Corley, and Hamilton 2014). This resulted in a cocreated understanding of the core value trade-offs in the nursing home experienced by residents (vulnerable primary customers), spillovers experienced by both other residents (other vulnerable primary customers) and the family members (vulnerable secondary customers), and coping mechanisms utilized by both residents and family members (vulnerable primary and secondary customers; see Figure 1). The following Findings section follows this logic. Quotations (pseudonymized) to illustrate the analysis are integrated in the text and in Tables 2–5.
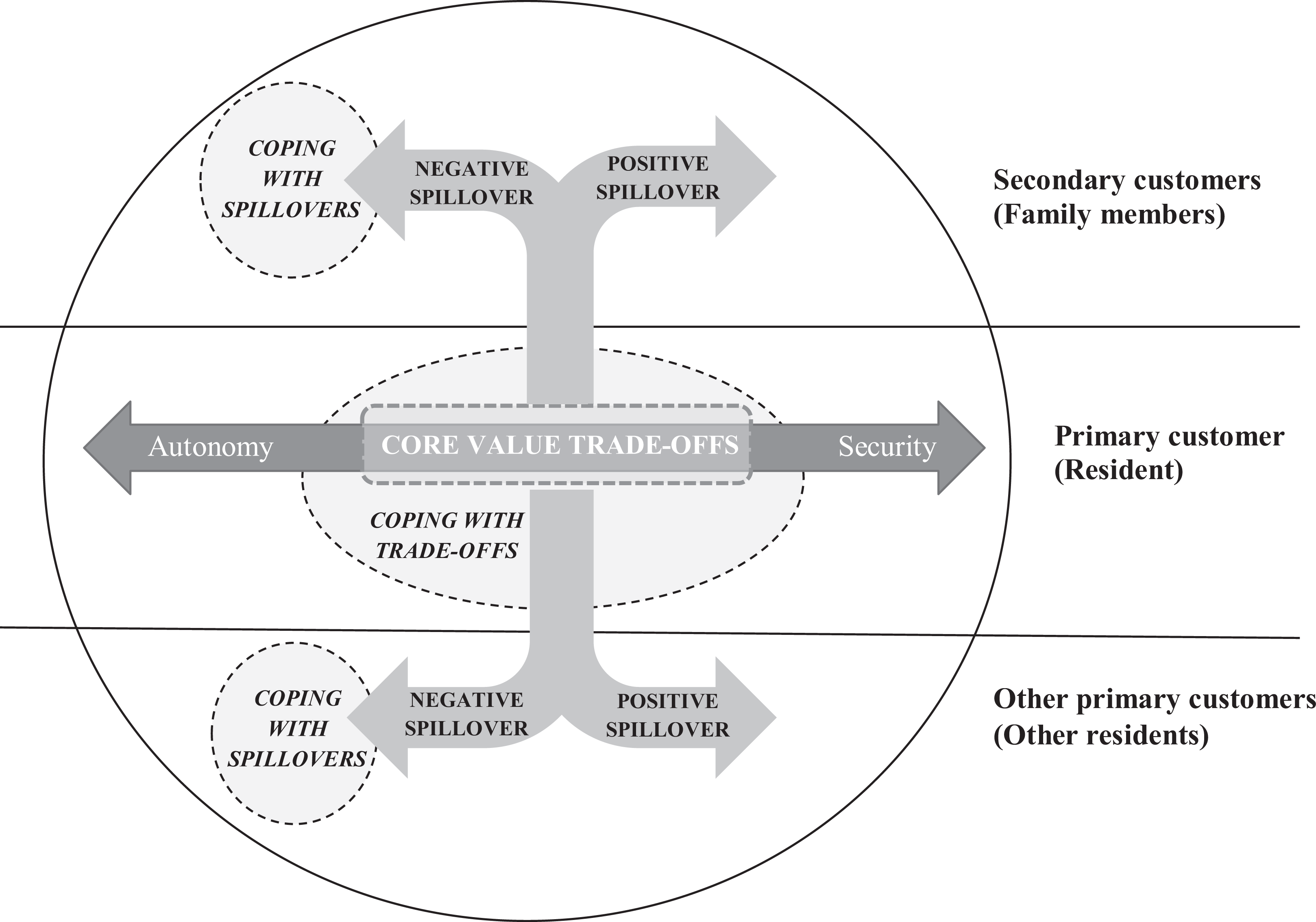
Core value trade-offs, spillovers, and coping in the extended customer entity.
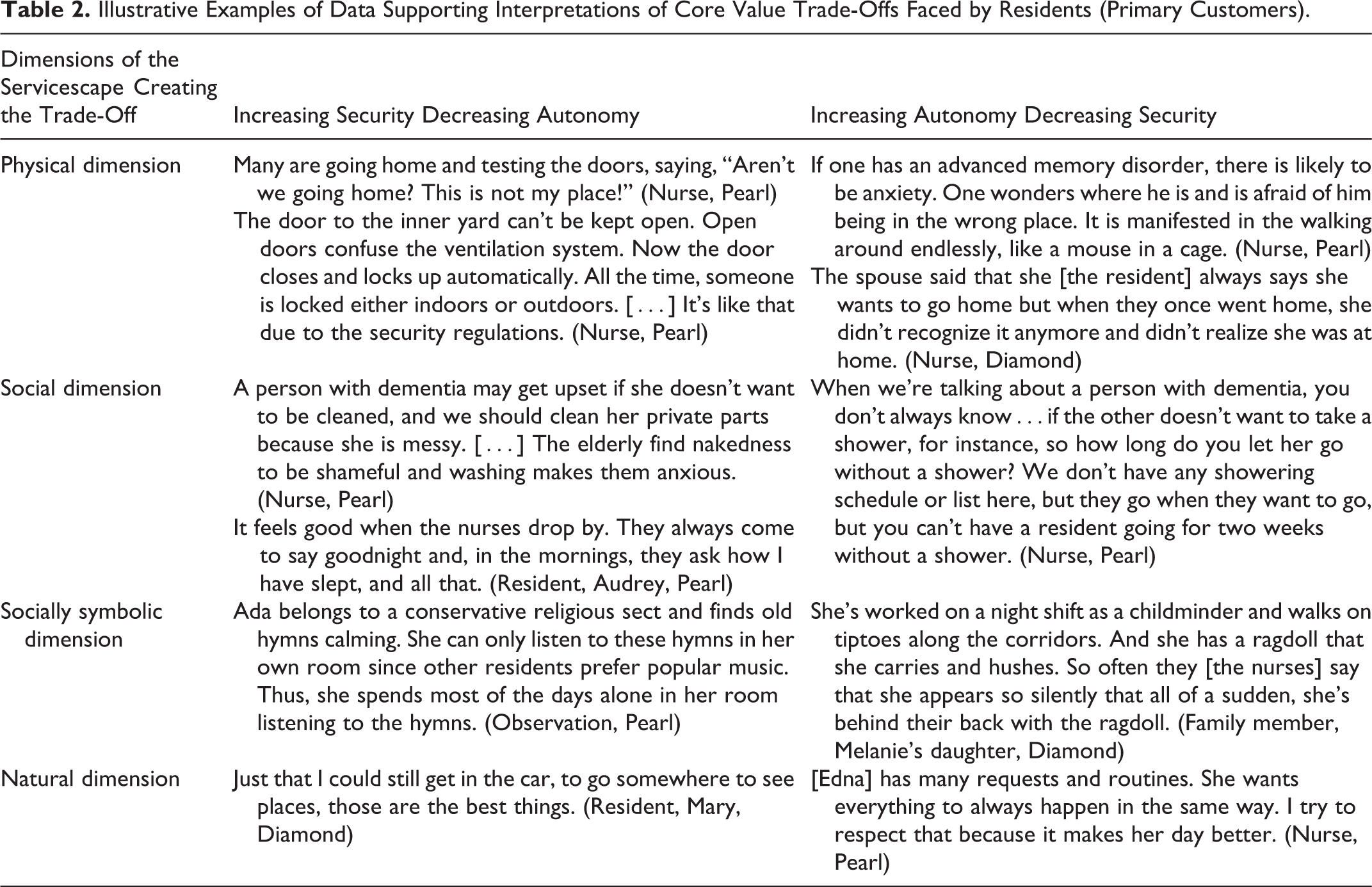
Illustrative Examples of Data Supporting Interpretations of Core Value Trade-Offs Faced by Residents (Primary Customers).
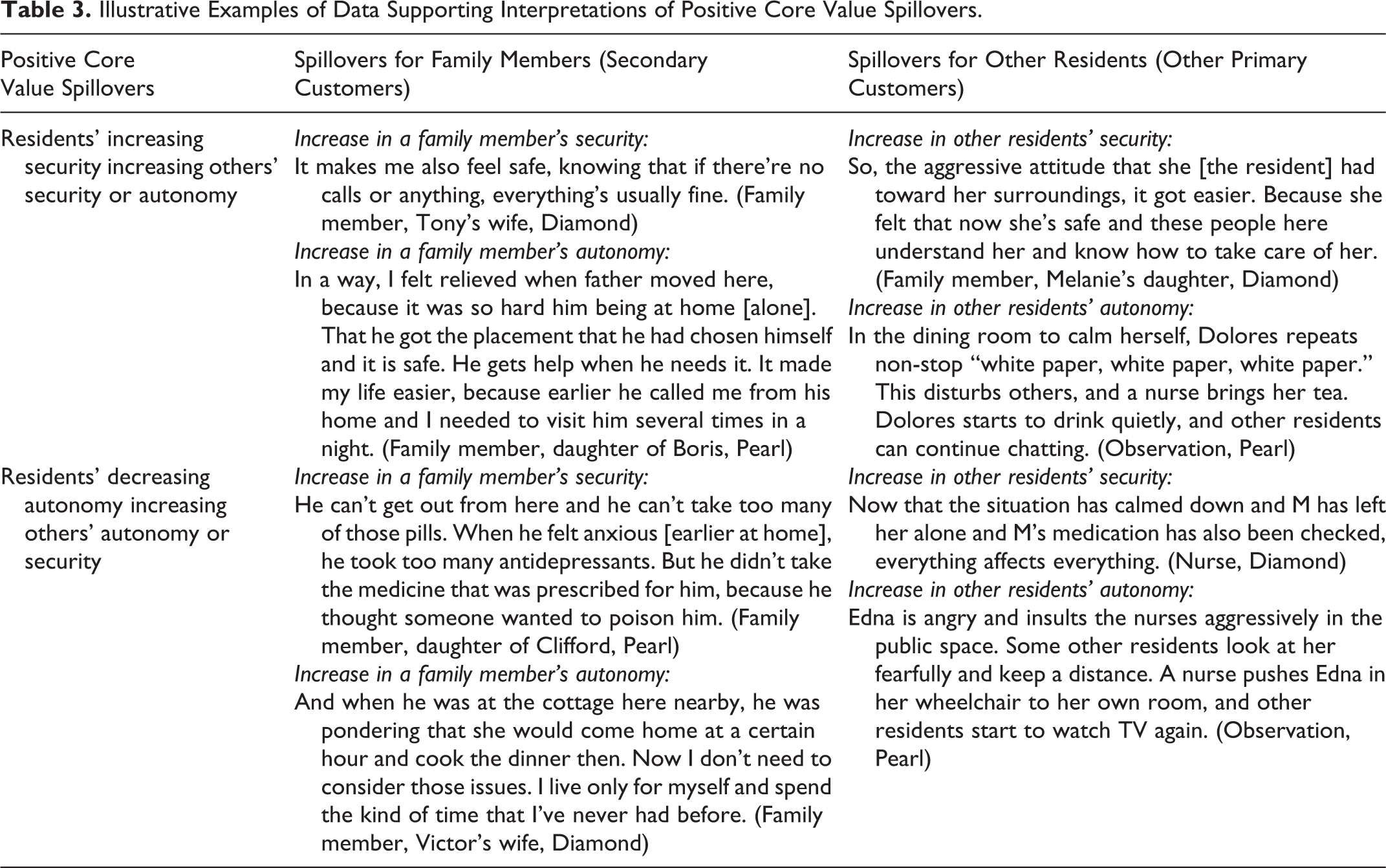
Illustrative Examples of Data Supporting Interpretations of Positive Core Value Spillovers.
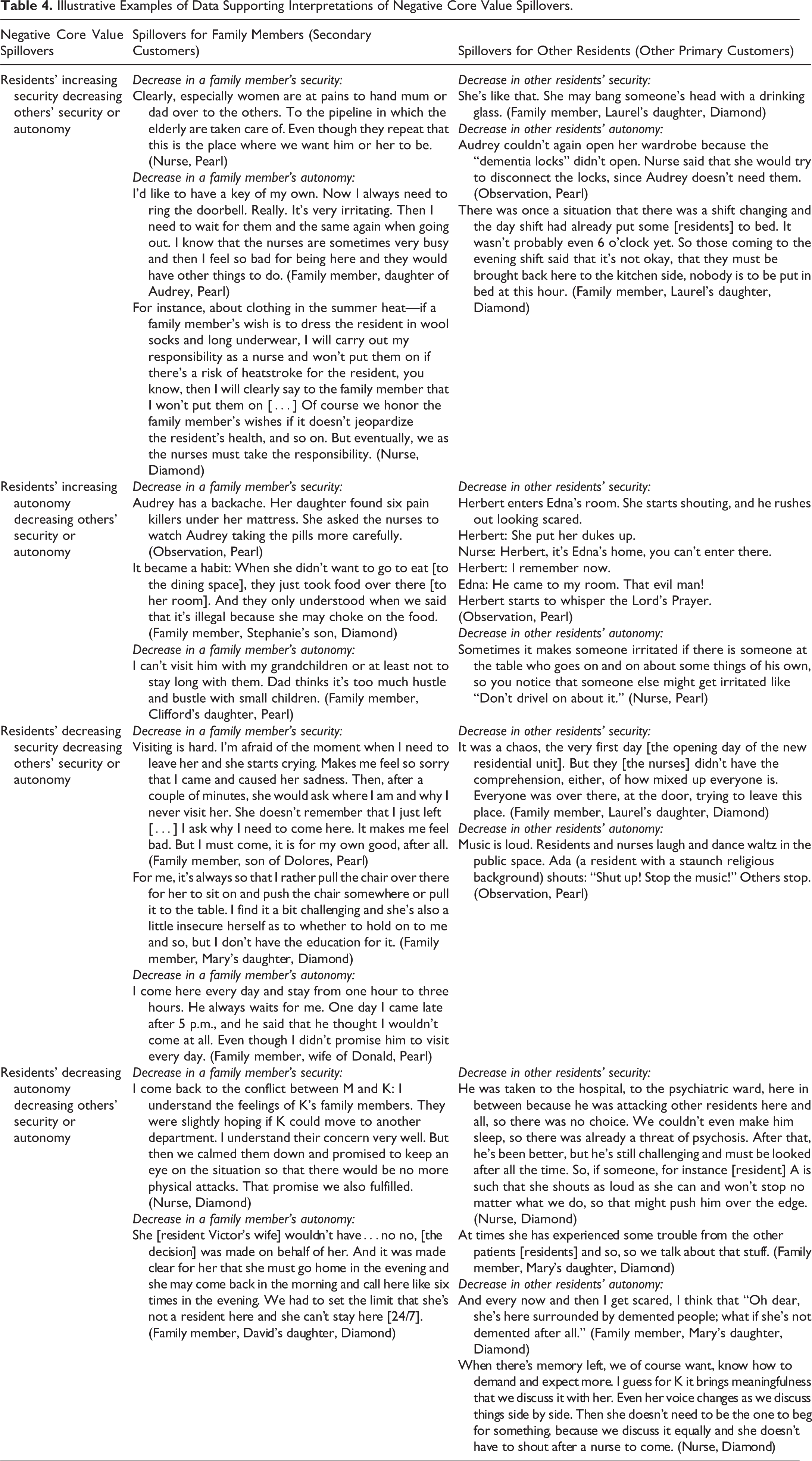
Illustrative Examples of Data Supporting Interpretations of Negative Core Value Spillovers.
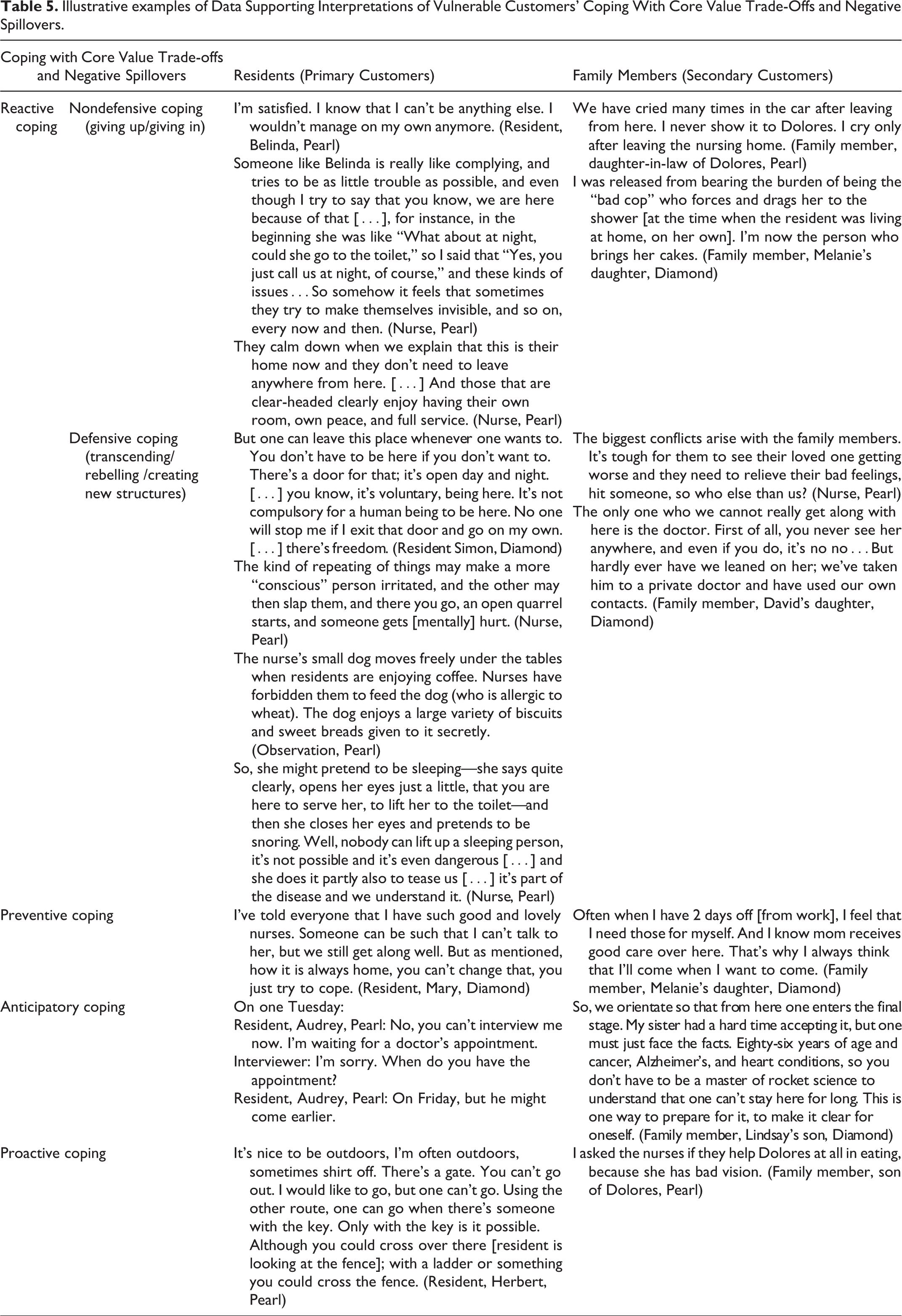
Illustrative examples of Data Supporting Interpretations of Vulnerable Customers’ Coping With Core Value Trade-Offs and Negative Spillovers.
Findings
Overview
Our findings provide insights into the unintended consequences manifested in core value trade-offs and spillovers. The findings take into consideration the perspectives of multiple vulnerable stakeholders in nursing homes: the primary customer (resident), secondary customers (family members of the resident), and other primary customers (other residents). Since the communication capability of many residents was diminished due to memory disorders, we consider both expressed and perceived trade-offs and spillovers. The service providers’ (nurses’) perspective is not included since the core values of autonomy and security are more accentuated for vulnerable customers; however, the insights of the nurses are utilized in interpreting the others’ trade-offs and spillovers. Figure 1 illustrates the organization of and relations between the key constructs of the study.
Core Value Trade-Offs in Nursing Homes
In nursing, the key aspect is to protect the well-being of the recipients of care (e.g., James, Ardeman-Merten, and Kihlgren 2014). Thus, security guidance was emphasized in the servicescapes of nursing homes. However, increasing the security of the residents decreases their autonomy and vice versa (see Table 2). The physical dimensions of the servicescapes that were built to highlight security, such as locked doors, automatic lights, and ventilation, evoked uncomfortableness or even fear: We have automatic lighting in the toilets [of the residents’ private rooms] and they have sliding doors, so, for instance, when the night nurse comes to peek from the door, the light turns on if the sliding door has been left open. So, one of our residents always thinks that there is thunder at night and she’s scared. The sort of things that you don’t realize until in practice…that you think is such a handy system, you don’t need to think about whether to turn the light on or off, but in the end, it may cause fear to some. (Nurse, Pearl) It’s like a prison here. There’s a fence around and you don’t go over it. The nurses are guarding. […] And one walks around in circles in the inner yard. I have thought, how long still? If I live to a hundred years, I still have sixteen years left. (Resident, Clifford, Pearl)
Residents were allowed to move around freely in the nursing homes’ shared space. The free-moving possibilities did, however, increase the search for a sense of security, manifested in the wandering behaviors (see, e.g., Tufford et al. 2018) of some people suffering from memory disorders: “You shouldn’t allow her to wheel too long over there [with the wheelchair]. She reacts like a small child, wants to go on and on, claiming that she’s not tired” (Family member, Stephanie’s son, Diamond).
The social dimension of servicescapes, particularly the nurses, played a key role in restricting unsafe wandering and in creating other trade-offs between security and autonomy. The nurses emphasized that residents, especially those suffering from dementia, needed to be controlled for their own well-being. Thus, the servicescape-inherent hierarchy of values was visible: The nurses’ understanding of what they should provide was safety in the first instance. There were certain issues for which there was no flexibility, such as medication and body belts for protection from falls. To a certain extent, flexibility was provided through eating and personal hygiene: Some matters need to be taken care of. One needs to be washed eventually, even if she doesn’t like it. Basic things like hygiene and nutrition need to be taken care of, but not by force. One needs to lure and give alternatives. (Nurse, Pearl) So, in this kind of place it’s a bit…that even though one has a memory disorder, you knock on the door even if he has called me to come to his room. The individuality, dignity, that is there. (Nurse, Pearl)
There were no fixed visiting hours, and visits by family members were encouraged at any time. Residents spent time with the visitors both in public spaces and in their private rooms. However, the nurses found it problematic when reacting to the residents’ sexual lives and trying to provide them with autonomy and privacy without compromising on security: Then, when the [new] spouse comes here, we would notice it and would not go to that room…think about it, they have spent three years together […] they’ve had like a sexual life to the full. And now they need to, in a way, share their sexual life with us all, just like this. (Nurse, Pearl)
The natural dimension was reflected in getting away from the servicescape (cf. Rosenbaum and Massiah 2011: being away in the servicescape) and breaking routines. Many wanted to have the autonomy to leave the nursing home, to go to see the city, to go to a cafeteria, or to see their old homes: Then there are of course people for whom it’s a disappointment that they have been given a different kind of image of this place; the kind where everything is possible in here and you can go to the marketplace from here every day. With the resources that we have, it’s not possible to release one of us two nurses to go somewhere for many hours [with the residents]. So, some also have feelings of disappointment. (Nurse, Pearl) It appeared, with one person for example, that she always had tea and toast. So, it doesn’t pay off to ply her with porridge. […] Now this person, for instance, eats the entire piece of toast without complaining and drinks the warm tea and is very happy. And she wants four lumps of sugar in it. If she’s given only two lumps of sugar and honey, it’s not enough. So, these kinds of personal habits. (Nurse, Pearl) It’s okay to have some variety. It just so happened that we had a troubadour visiting us. We didn’t inform the residents beforehand, but the musician just came and started to set up his instruments. It happened at a time that they would normally go to take an afternoon nap. No one went. They didn’t mind missing their nap at all. Well, Herbert was slightly disapproving, in that he said, “What’s going on? We didn’t have this kind of activity earlier at this time.” But even he stayed and seemed to enjoy it. (Nurse, Pearl)
Positive Core Value Spillovers in Nursing Homes
The resident’s (primary customer’s) trade-off between security and autonomy created spillovers both for other residents (other primary customers) and for family members (secondary customers). Even though negative spillovers were accentuated, there were also some positive spillovers, which are presented in this section and in Table 3. It is noteworthy that the positive spillovers that were detected were related to residents’ increasing security or decreasing autonomy, that is, emphasizing one end of the security-autonomy continuum.
Residents’ increasing security calmed the family members and gave them more autonomy. Many of the family members had taken 24-7 care of the residents prior to them entering the nursing homes. When they knew that the resident was taken care of, they could rest and organize their days more freely. Residents who felt secure also calmed other residents down: They are like calm and they might even comfort the others by saying it’s okay, let’s just wait here and all. Like “It’ll be okay, soon we’ll get to eat,” trying to sort of calm others down as well, indicating that there’s nothing to worry about. (Nurse, Diamond) Mum became more and more addicted to alcohol. The last days at her home were quite chaotic. I never knew how she was going to be when I entered her home. I found her many times passed out on the floor; often I called an ambulance. And she didn’t take her medicine either. It was crazy. (Family member, daughter of Audrey, Pearl)
Residents’ decreasing autonomy was occasionally compensated for by the autonomy of the family members. For instance, when a resident arrived at the nursing home from the hospital, her daughter fulfilled her own vision of decorating the resident’s room: It may be that she would have wanted to have a curtain with flowers, but I didn’t, so…I think a light-colored [curtain] was better suited [laughs]. So, I hung them there before grandma came here. So, the room was like ready, already, and she just came here. (Family member, daughter of Audrey, Pearl) So, it was also a question of mother’s wellbeing. It seemed impossible to keep him at home anymore; soon we’d have both dad and mum at the hospital. This place was like a gift from heaven. A light and warm room. We can all visit him here. (Family member, daughter of Clifford, Pearl)
Negative Core Value Spillovers in Nursing Homes
The resident’s (primary customer’s) trade-off between security and autonomy created various negative spillovers both for other residents (other primary customers) and for family members (secondary customers). They are presented in this section and in Table 4.
Negative spillovers could result either from the resident’s positive or negative experiences. In the former case, spillovers originated from the resident’s increasing security or increasing autonomy. The resident’s increasing security decreased the security or the autonomy of family members or other residents. Even though the family members felt relieved at seeing their loved one in a safe place, they often shared a long history of worrying and caring, and it was difficult to hand that responsibility over to the nursing home. As the security of the residents is the key issue in the nursing homes, many dimensions of the servicescapes that provided security to the residents restricted the autonomy of the family members. The locked doors, particularly, were annoying for the visitors. Nurses also noted that family members may not always know what is best for the resident: I think she should have clothes that are easy to dress her up in, because her joints are stiff and sore, but her family members sometimes bring her such clothes that are unthinkable. They couldn’t be put on her at all, or at least it would be awfully difficult. (Nurse, Diamond) There was a nasty incident, when once, well I may have fondled her front a little. Then the nurse asked her if I had done that, and she answered: “Yes, but she didn’t approve of that.” […] After that, some nurses have taken a dim view of me. […] But I like her, seriously. (Family member, partner of Delia, Pearl)
Nursing homes tried to provide as much autonomy to the residents as they could without compromising on security. Sometimes, the resident’s increasing autonomy decreased the security or autonomy of family members or other residents. Family members needed to accommodate their visits to meet the requests of the residents and felt insecure when they felt responsible for the residents: Last summer we walked around quite a lot in the yard over there, but this summer we haven’t yet walked further, only here in this inner yard. But it has become more difficult for him to move, so it’s more insecure, so I don’t know whether I have the courage to go anymore. (Family member, Tony’s wife, Diamond) She’s also like a bit aggressive and she may just go to someone else’s room and go lie down on the bed and you can’t get her out of there. So yeah, when considering that it’s your home…if someone comes to lie down on your bed, is it a home then? (Nurse, Pearl) So it [the dispute] arises from minor things like how the tablecloth is placed, since Stephanie is so precise about the cloth and about the flowers, so it must be just as she wants it—she is quite eager to say [her opinion]. (Nurse, Diamond)
However, we also noticed negative spillovers resulting from residents’ negative experiences: decreasing security or decreasing autonomy. Residents’ decreasing security decreased the security or autonomy of family members or other residents. Feelings of insecurity spread fast. When the residents openly showed that they felt unsafe and would rather be elsewhere, family members were disturbed: There was another patient [resident] who, like, attacked her—pulling her hair and pushing and shoving her, it went on for a few weeks…and she also said herself that she knows this person is ill, but it was a situation that caused us anxiety. It was quite shocking to come here and hear from the nurse that this person had pulled a bunch of hair from mother that day. (Family member, Mary’s daughter, Diamond) Abel died today at the hospital. He was moved there on Monday. After that, one of our residents asked where he was. I said that he’s in the hospital. They need to know. […] Now we need to tell everyone that he has passed away. We’ll do it during afternoon tea. Everyone will be told because they’d notice it anyway and ask questions. For them, death is an issue that you can talk about. (Nurse, Pearl) At some stage I went outdoors with him but I can’t get him anywhere by myself and I probably don’t even know how to dress him up since his joints are somehow awfully stiff. So, when I’m here around noon and they have the hassle with lunch and everything, I can’t bring myself to ask if someone would come and dress him. (Family member, Victor’s wife, Diamond)
Coping With Core Value Trade-Offs and Negative Spillovers in Nursing Homes
Residents and family members employed various ways of coping with core value trade-offs and negative spillovers. In line with Hill and Sharma (2020), we identified both nondefensive and defensive coping mechanisms. However, even though these reactive forms of coping were accentuated in the data, we also identified coping mechanisms that entailed a forward-time perspective: preventive, anticipatory, and proactive coping (see Table 5).
Nondefensive coping mechanisms consisted of both giving up and giving in (see Hill and Sharma 2020). Giving up was reflected in understanding the inevitability of the trade-off between autonomy and security, comparing the nursing home with other possible options (home care or hospital), and accepting it with either sadness or anger: It is miserable to speak about enjoying one’s stay. One needs to be somewhere. […] I’m all by myself here as long as I have time left. One doesn’t know how long. One needs to grin and bear it. (Resident, George, Pearl) Mum has begun to really feel at home. The positive change was noticeable right away, and the nurses were frequently commenting on it. Because they saw how aggressive, resistant, and scared she was when she came here. And how fast she then changed into a cooperative person. […] She could be herself. Didn’t need to defend herself. (Family member, Melanie’s daughter, Diamond) A human being starts to lose his or her autonomic way of life so easily, even for a person who has lived at home and gone downtown, and out and about, so when coming to a place like this, the routine is built, however, around the meals, and it’s just…a human being quite soon changes to kind of…becoming a bit apathetic and “I don’t wanna go out” and “I don’t want this and I don’t want that.” (Nurse, Pearl) Today, it’s been quite a good day. I’ve been over there, in the yard […] for outdoor games; you can run over there […] You can go to the swing over there and you’re allowed to go at some speed, too. […] You can also play on that other swing, sitting. It swings at high speed. Then you need to hold on to something, otherwise you can fall down. (Resident, Wendy, Diamond)
However, we also noticed indirect and hidden rebelliousness. For example, some ladies were served their afternoon soup, and they started to joke with the nurses and request vodka instead. We also witnessed how Herbert (a 97-year-old resident) tiptoed to the kitchen, took handfuls of sugar cubes, and hurried with them to his own room. The nurses did not notice this, but some other residents started to scold Herbert for stealing.
There were also occasions when residents tried to create their own structures and hierarchies of reality, for example, by faking their needs or by denying something that they did not approve of. An example of the latter is related to the safe electric fireplace that was installed in Pearl’s public space to generate a “homelike” atmosphere. The residents hated it because it was not a real fireplace. They said that they tried to pretend that it did not exist. They chose their chairs so that they did not need to see the fireplace. We also saw how Delia (a resident with severe memory loss) took the cord from the fireplace, hid it in her handbag, and carried it away.
In preventive coping, one prepares for reducing the risk of stressful events and minimizing the severity of the impact of potential distress (Schwarzer and Luszczynska 2008). A particularly important element that the residents used for their own security (yet, diminishing the autonomy of others) was using lockable doors for their private rooms. Since some residents accidentally entered the wrong rooms, other residents preferred to use locks, at least during the night: Next door, there is that kind of person who enters here, just walks in like that. It is not nice. This is my room now. I have asked the nurses to lock my room at nights. (Resident, Boris, Pearl)
In anticipatory coping, individuals deal with imminent threats, a critical event that they assume will occur in the near future and that may cause them harm or not (cf. Schwarzer and Luszczynska 2008). Since life in the nursing homes was quite monotonous, those residents who did not have memory disorders prepared well in advance for changes, waiting a couple of hours for visitors to arrive, or preparing a couple of days ahead for a visit by the doctor. Family members were also preparing for and planning terminal care: Well it [the wishes regarding the spouse’s caretaking] culminates in that terminal phase, to make it humane, it would be important. Now I’m feeling a bit fearful about it because I suppose that the resources don’t enable it, after all…so those are the issues that make me worry about what the future is going to be like. (Family member, Ingrid’s husband, Diamond)
Additionally, some family members were actively trying to influence the treatment of their loved ones. Their experiences from the nursing homes also made them consider how to shape their own elderhood: It’s distressing to note how one’s social circle might get small…I thought that my own old age is just around the corner. It’d be good to maintain social contacts [then]. (Family member, daughter of George, Pearl)
Discussion and Conclusion
Theoretical Contribution
By adopting a multistakeholder approach and analyzing the values of autonomy and security in the specific setting of nursing homes, this article provides insights into unintended consequences that certain core values, their hierarchization, their concrete enforcements, and the negotiations connected to them may have on both vulnerable primary customers and vulnerable secondary customers. By revealing the trade-offs in core values made by vulnerable consumers and the spillovers of these trade-offs to other vulnerable consumers, we make three main contributions to the literature. First, we contribute to the servicescape literature by showing how the core value trade-offs originate in different dimensions of the servicescape. Second, we contribute to multistakeholder research by showing how spillovers and trade-offs produce unintended consequences for different stakeholders. Third, we contribute to the discussion on consumer vulnerability by considering vulnerability in the extended customer entity and by identifying the active coping mechanisms of vulnerable consumers.
Our first contribution extends the understanding of servicescapes (Mari and Poggesi 2013; Rosenbaum and Massiah 2011) by showing how core values can be integrated into the servicescape discussion. Rosenbaum et al. (2007) showed that accepting the service providers’ and other customers’ core values fosters customers’ place attachment. By focusing on the customers’ experience of two—often contrary—core values, we were able to show how the servicescape is used to support core values. Contrary to the suggestion by Siguaw, Mai, and Wagner (2019), we did not see security as a separate dimension of the servicescape but rather we saw it—and also autonomy—as an element penetrating all the dimensions. This view is particularly useful in researching care-related servicescapes because their main purpose is to ensure safety on all servicescape dimensions. Thus, security as a prioritized value is considered in each servicescape dimension. However, there are other core values, such as autonomy, and even umbrella values, such as dignity (Menzfeld 2018; see Shore [1996] for a detailed elaboration on moral umbrella models), that are important for holistic well-being, and servicescape dimensions should acknowledge all of them. Concentrating only on one core value would jeopardize the high standards of holistic care and overall well-being that are rightfully demanded of care-related servicescapes (Burack et al. 2012).
Furthermore, the study reveals that incorporating core values into servicescapes is not a straightforward process that is easily established. Incorporating heterogeneous values into everyday conduct and services involves trade-offs: Supporting one value may unintentionally decrease or strengthen the other. Thus, a service that is created to increase well-being could turn out to be harmful—at least in some respects—thus showing “the dark side” of servicescapes (cf. Mari and Poggesi 2013). The way core values are prioritized—and what trade-offs take place between them—reflects on how servicescapes are built. We suggest that the concrete purpose of a particular servicescape needs to be carefully reflected on when analyzing the core value trade-offs. In nursing homes, security is of paramount importance. However, for instance, in the context of recreational services, autonomy is likely to be emphasized over security—to a certain degree. In this field, services have reacted to the need for individuals to experience both security and autonomy by generating servicescapes providing “engineered adventures” such as escape rooms or organized adventure trips.
Our second contribution addresses the calls to include the multistakeholder perspective in TSR (cf. S. Anderson, Nasr, and Rayburn 2018; Johns and Davey 2019; McColl-Kennedy, Cheung, and Coote 2020) and in servicescapes (Pizam and Tasci 2019) in particular. We showed how core value trade-offs experienced by one customer create a ripple effect and spillovers in others (see Figure 2). Earlier research on the customer copresence influence has considered more visible aspects of consumer behavior (such as interactions and copresence in the same facilities) (Colm, Ordanini, and Parasuraman 2017). We contribute to that by showing that the core values experienced, argued for, or acted out by one customer may also influence others via spillovers. Thus, our findings support the conceptual study by Finsterwalder and Kuppelwieser (2020) by empirically showing how the spillovers created both unintended negative and positive consequences. The multistakeholder perspective showed that service providers have an important role in balancing these core value conflicts: They can act as advocates, even defenders, of primary customers by explaining the current/changed needs of the primary customer to the secondary customers.
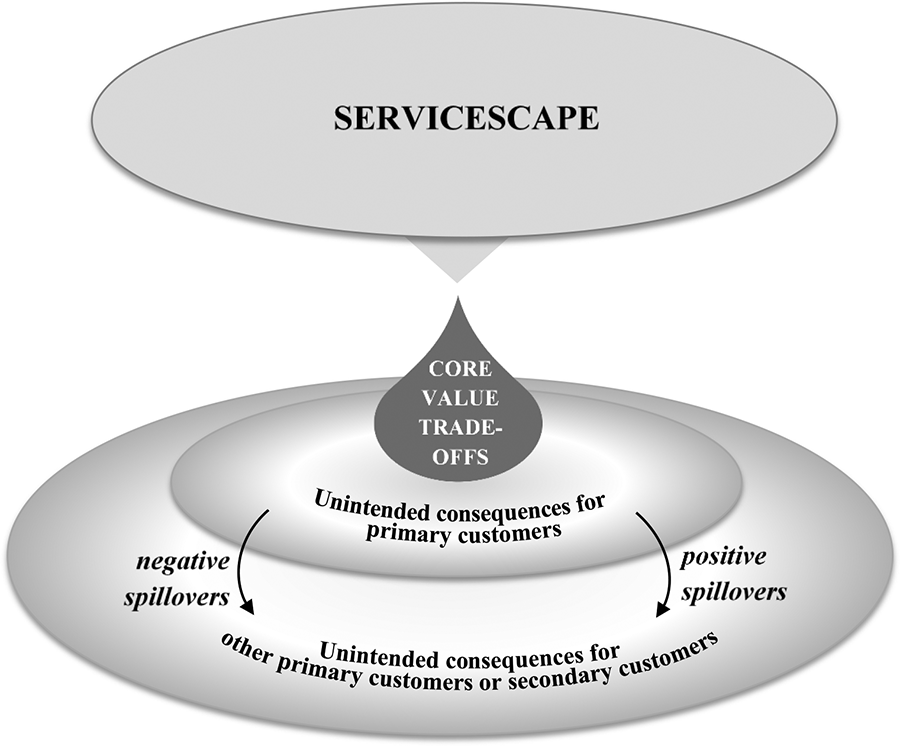
Unintended consequences from core value trade-offs within servicescapes.
Furthermore, by analyzing primary and secondary customers, we enrich the extant research on multiple stakeholders and demonstrate how the relationship between the core value–related needs of primary and secondary customers is far from being straightforward or one-directional but shows reciprocal influences and mutual dependencies. The actual needs, and also the perceptions of one’s own and others’ needs, are not necessarily aligned. Additionally, the vulnerability of the primary customers influences the wishes and judgments made by the secondarily vulnerable customers since it may bias the secondary customers’ assessment of the primary customers’ needs. This is why open communication with the nurses is essential to guarantee a truthful, up-to-date understanding of the primary customers’ abilities and needs.
Our third contribution is to accelerate the vulnerability discussion in TSR. In line with Leino (2017), our study shows that vulnerability extends from primary customers to secondary customers, thereby confirming the relevance of the extended customer entity. Leino (2017) suggests that the conceptual division between primary and secondary customers and, hence primary and secondary vulnerability, is useful for TSR, especially when considering the interplay between services and the well-being of individuals and families (cf. L. Anderson et al. 2013; Ostrom et al. 2010; Rosenbaum et al. 2011). This study provides specific evidence on how primary customers’ core value trade-offs influence not only themselves but also result in positive or negative spillovers in the extended customer entity, thus often influencing the secondary customers’ and other primary customers’ well-being either positively or negatively. Due to secondary vulnerability, the influence of spillovers can become especially meaningful and powerful. Thus, the insight into vulnerability in the extended customer entity deepens our understanding of the specific characteristics needed from transformative services and servicescapes.
Furthermore, the study provides empirical support for the defensive and nondefensive coping mechanisms of vulnerable consumers as suggested in the conceptual paper by Hill and Sharma (2020). We expand the categorization of coping mechanisms by showing that even extremely vulnerable consumers may also utilize more active coping mechanisms—even proactiveness. Thus, we suggest an intensified incorporation of active (even though in many ways limited) agency in the consumer vulnerability discussion.
Practical Implications
This study suggests that service contexts need to pay attention to core value trade-offs and spillovers. Especially in care-related services, the security-autonomy trade-off needs to be taken into account in all servicescape dimensions. When contemplating customers’ well-being, it is important to understand that their perceived autonomy and security matters—even though absolute security or autonomy cannot be created. One task for the nursing home, for example, could be to develop and maintain the experience of autonomy—to make the elderly feel that they have free choice. However, in the best-case scenario, care-related services may also bring about new experiences: In addition to offering feelings of autonomy similar to those that the customers have lost, services can develop and emphasize new or different kinds of autonomy.
The study showed that the residents of nursing homes were treated almost equally whether they suffered from memory loss or not. Consequently, those without dementia were also locked down and not given the freedom to leave the facility, even though they still possessed the capabilities to explore the outside world by themselves, without restrictions and without carers needing to escort them. In addition, nondemented residents had to face the distress of witnessing dementia on a daily basis: This included dealing with demented coresidents’ lack of recognition of the concept of privacy, resulting in, for example, demented persons entering nondemented persons’ rooms. Therefore, we recommend that, in order not to restrict the autonomy of those who do not need restrictions—and to protect those who require maximum security at the same time—there should be (partly) separate accommodation facilities for those who are only physically frail outside of the spaces for those who suffer from decreased cognitive abilities (such as dementia). For instance, private rooms and dining spaces could be located in different sections of the home, but shared living rooms could allow all residents to socialize with each other.
This study also highlights that the core values of both primary and secondary customers need to be taken into account in servicescapes. Since vulnerability has a considerable influence on customers as service users, the core values need to be acknowledged in such a way that they diminish vulnerability and do not increase it. The notion of extended vulnerability (primary vulnerability creating secondary vulnerability) poses additional, special expectations for service providers because secondarily vulnerable customers use servicescapes created for the needs of the primarily vulnerable. Our research shows the need to also develop servicescapes to better meet the needs of the secondarily vulnerable customers, and, at the same time, we discuss the unintended consequences, such as trade-offs and negative spillovers, which service providers should acknowledge.
Furthermore, vulnerability extends not only from individual to individual but also over time; the secondary customers’ vulnerability may endure long after the primary customer no longer exists. Additionally, if a company copes well with primary customers’ vulnerability, this could reduce secondary customers’ vulnerability at a later time. In nursing home contexts, we witnessed how family members anticipated having greater success in dealing with the evident loss of their loved one if they could be sure that they had received good care until the end of their life. Thus, good experiences of the service (on the part of the primary and/or secondary customer) can, in fact, support secondary customers’ well-being after the actual service relationship has ended, while unfavorable experiences can cause long-term negative consequences. This is why the service should also pay special attention to temporarily extended customership and the secondary customers’ needs and vulnerability, also considering their possible needs for the service after the primary customer is gone.
Our findings also encourage paying more attention to how vulnerable customers deal with unintended consequences since their coping strategies are versatile. The role of service providers, for instance, nurses, is acknowledged in supporting the coping of customers (e.g., Garity 2006). However, this study showed that service providers can also utilize the different dimensions of servicescapes (e.g., other customers or ambient conditions) to support coping. Furthermore, we emphasize how treating vulnerable individuals as if they were persons who only react to circumstances neglects their agency as active stakeholders. Vulnerability is not equivalent to passivity, and vulnerable individuals can play an important role in influencing and developing the dimensions of servicescapes.
The recent COVID-19 pandemic has accentuated the trade-offs between the core values of autonomy and security in society. Restrictions executed in the name of security have decreased feelings of autonomy, especially among the most vulnerable individuals (see D’cruz and Banerjee 2020). The pandemic may offer an arena for servicescape innovations that enable bringing primary and secondary vulnerable customers together without risking their security.
Limitations and Future Research Directions
This exploratory study has unavoidable limitations, opening up avenues for further research. First, by concentrating on two core values, we were able to analyze them thoroughly. However, at the same time, other core values were left out of the scope of this research. While focusing on core value trade-offs, we also neglected the complexity of relationships between core values and did not consider nested or mutually reinforcing core values. Further work is needed to explore other core values, such as self-direction, benevolence, and traditions (see Schwartz et al. 2012), and relationships between values in servicescapes. As core values have been rather extensively studied and measured in psychology (e.g., Saroglou, Delpierre, and Dernelle 2004), these measurements could be combined with servicescape dimensions, thus providing possibilities to quantify the interplay between core values and servicescape dimensions.
Second, our research only focused on companies in Finland. It is acknowledged that the relationship between autonomy and well-being depends on culture, and autonomy is valued highly in Finnish (and some other) cultures (cf. Markus and Schwartz 2010). Extending the research to other countries would also expand our understanding of core values as well as coping with trade-offs in different settings and, for example, in cross-cultural contexts.
Third, our analysis did not consider how the customers’ previous biographical experiences reflect on their experience of autonomy and security—although we noted that those who entered the nursing home from the hospital seemed to appreciate the autonomy aspect, whereas those entering from their own homes tended to especially value the security provided by the nursing home. Further studies could research the effect of customers’ backgrounds on their experience of core values in servicescapes in more detail.
Fourth, as our focus was on core values, we took the existing and widely used division of servicescape dimensions as given. It may be that some other dimensions, such as affective and sensory dimensions, may also be relevant, especially when contemplating core values.
Fifth, while we were concentrating on the meso-level of servicescapes, we neglected the other elements of services, such as the microlevel of a respective customer journey and the macro-level of the wider service ecosystem. Exploring intertwining core values in the light of concepts and frameworks on a different level would extend the theory further and offer more managerial insights for service development. For instance, it would be beneficial to study (on a microlevel) the individual customer journeys over time: How primary and secondary customers’ expectations and experiences regarding the support for their core values in the servicescapes affect their well-being and at which touch points the interventions of service providers are especially needed (cf. Johns and Davey 2019).
Finally, as the vulnerability studied was prolonged in nature, the need for autonomy and security was presumably highlighted differently compared to the case of temporary vulnerability when individuals are not permanently threatened. Thus, further studies should focus on how the nature of vulnerability is reflected in the core values. This could mean, for instance, studying how (systemic, enduring) class-based vulnerability and (transient, temporary) state-based vulnerability (Commuri and Ekici 2008) differ in their influence on the core values and how these influences should be taken into account by service providers. For instance, does the comfort of a customer with class-based vulnerability need to be fostered more than that of a customer with state-based vulnerability, and how can this be performed in servicescapes?
As values are relatively stable, but not invariable, we also have to take into account that coping strategies related to spillovers might influence core values and how they are experienced by primary customers. Values are not simply out there, but they are formed in interrelations between persons. How exactly this takes place would be an important subject for further research.
Supplemental Material
Supplemental Material, sj-pdf-1-jsr-10.1177_10946705211012472 - Autonomy or Security? Core Value Trade-Offs and Spillovers in Servicescapes for Vulnerable Customers
Supplemental Material, sj-pdf-1-jsr-10.1177_10946705211012472 for Autonomy or Security? Core Value Trade-Offs and Spillovers in Servicescapes for Vulnerable Customers by Birgitta Sandberg, Leila Hurmerinta, Henna M. Leino and Mira Menzfeld in Journal of Service Research
Footnotes
Acknowledgments
The authors thank the special issue editors, the anonymous reviewers, Professor Niina Nummela, and Associate Professor Eriikka Paavilainen-Mäntymäki for constructive comments and suggestions, which allowed us to improve the article. The authors are grateful to the Emil Aaltonen Foundation for providing a project grant that enabled this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Emil Aaltonen Foundation.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.