
Abstract
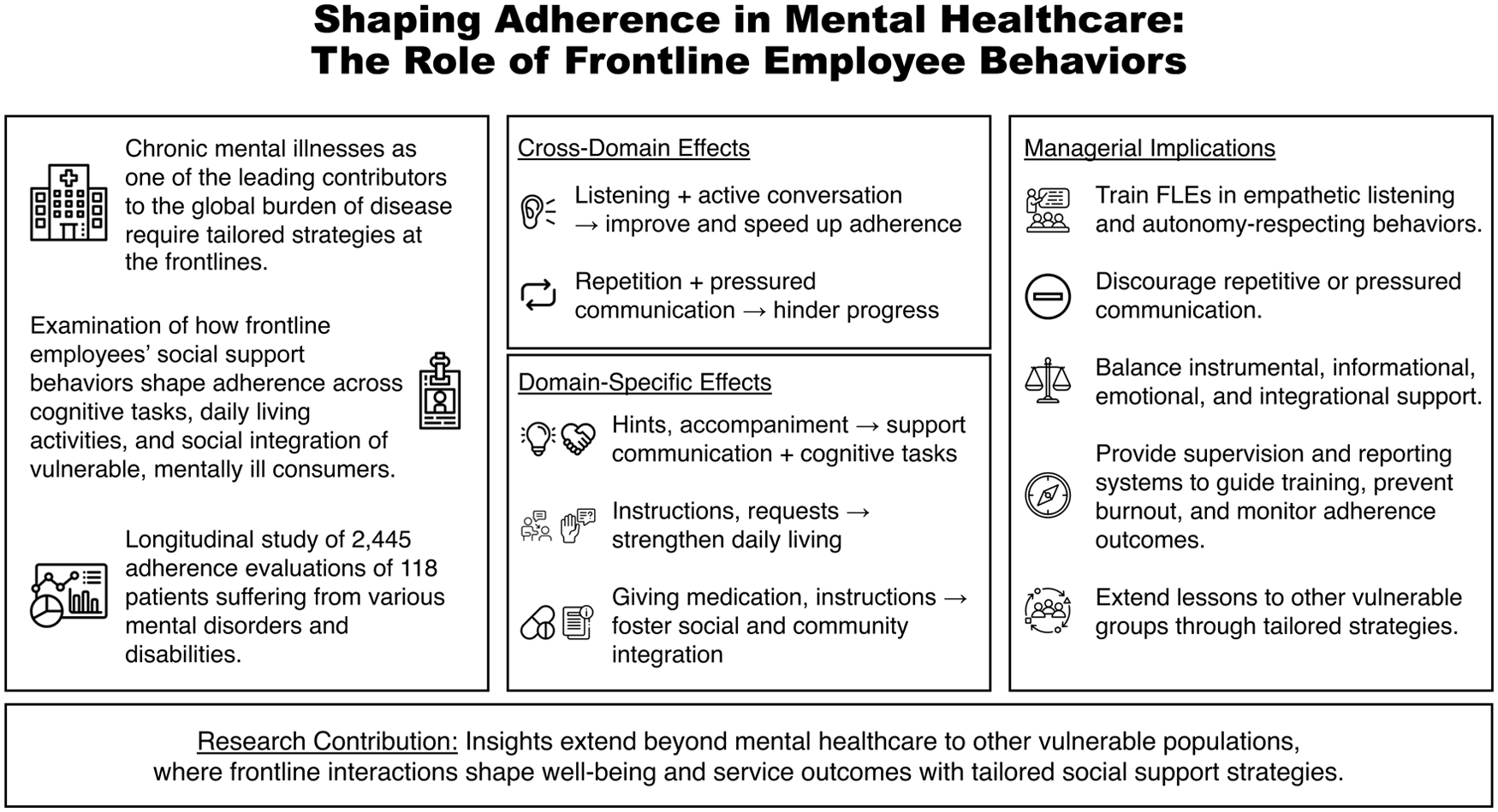
As mental illnesses surge globally, delivering effective care for mentally disordered and disabled individuals is crucial. While frontline employees play a critical role in service interactions with vulnerable consumers—a central issue in transformative service research—there is limited understanding of how frontline employees’ behaviors can influence adherence, defined as the extent to which individuals follow healthcare providers’ recommendations. Taking an empirics-first approach, we analyze longitudinal field data from 118 individuals with mental illnesses over 12 months, yielding 2,445 observations. Guided by social support theory, we employ a split-hazard model to examine how distinct frontline employee behaviors affect adherence in Communication and Cognitive Tasks, Daily Living Activities, and Social and Community Integration. Our findings highlight the need for tailored behavioral strategies, showing that listening and active conversation consistently enhance adherence, while repetition significantly reduces it. Our study offers novel insights into how frontline employee behaviors can improve the well-being of vulnerable consumers, particularly in mental healthcare. These insights inform both theory and practice by advancing social support as a framework for frontline service delivery and providing actionable strategies to improve care and adherence.
Keywords
Introduction
The worldwide rise in chronic mental illness diagnoses has made them one of the leading contributors to the global burden of disease (GBD 2019 Mental Disorders Collaborators 2022; The Lancet Global Health 2020). Mental disorders—such as depression, bipolar disorder, schizophrenia, and other psychoses—affect over 1 billion people worldwide, including over 200 million with severe or chronic mental and intellectual disabilities (The Lancet Global Health 2020; World Health Organization 2025b). Individuals with these conditions often experience cognitive impairments, emotional dysregulation, and behavioral difficulties (World Health Organization 2022), making them more vulnerable than the mentally healthy population “because [vulnerable individuals’] access to and control over resources is restricted in ways that significantly inhibit their abilities to function [in society]” (Hill and Sharma 2020, p. 554). Treating mental disorders imposes enormous and rising costs on healthcare systems, projected to increase by 150% by 2030 (The Lancet Global Health 2020), alongside substantial economic losses (World Health Organization 2025a). As resources tighten, effective service delivery becomes increasingly important (World Health Organization 2025a).
Frontline employees (FLEs) play a pivotal role in shaping individuals’ experiences and health outcomes within healthcare services (Berry 2019). Among the most consequential and challenging objectives in healthcare is fostering adherence, 1 defined by the World Health Organization (2003, p. 3) as “the extent to which a person’s behavior—taking medication, following a diet, and/or executing lifestyle changes—corresponds with the agreed recommendation from a healthcare provider.” Non-adherence undermines clinical effectiveness, prolongs recovery, contributes to relapse, and escalates healthcare costs (Sokol et al. 2005; Spanjol et al. 2015; Viswanathan et al. 2012).
The challenge of promoting adherence is even more pronounced in mental healthcare, where FLEs must navigate complex, emotionally charged interactions with individuals that require unique competencies compared to other healthcare or service settings. Despite FLEs’ central role, little is known about how their behaviors influence adherence in mental healthcare (Allen, Sugarman, and Wennerstrom 2017; Clement and Bigby 2012; Mende et al. 2024). Transformative service research (TSR) has emphasized the importance of studying vulnerable populations, particularly within behavioral and mental health services (e.g., Boenigk et al. 2021; Danaher and Gallan 2016; Ostrom et al. 2015).
Specifically, TSR scholars have urged further investigation into how service interactions unfold and shape outcomes over time, especially in settings where individuals encounter substantial life challenges (Ostrom et al. 2015). However, existing adherence research in health services primarily addresses medical (Bowman, Heilman, and Seetharaman 2004; Prigge et al. 2015; Spanjol et al. 2015) or behavioral adherence (Dellande, Gilly, and Graham 2004; Seiders et al. 2015), with little focus on populations affected by chronic mental illness. Although FLE behaviors have been studied across industries (e.g., Gremler and Gwinner 2008; Güntürkün, Haumann, and Mikolon 2020; Marinova, Singh, and Singh 2018), the distinctive demands of mental health encounters remain overlooked.
This study seeks to address this critical gap by examining how interactions between FLEs and patients shape adherence outcomes in mental healthcare settings. Guided by TSR, we focus on patient adherence and well-being, prioritizing patient-centered outcomes over organizational or financial metrics. Although improvements in patient outcomes may yield economic benefits for healthcare organizations, these effects fall beyond the scope of the present study. Specifically, we investigate two interrelated research questions:
(1) What types of FLE behaviors foster medical and behavioral adherence among individuals with mental disorders and disabilities?
(2) Which FLE behaviors are most effective in accelerating adherence relative to others?
To address our research questions, we collaborate with a large healthcare organization and acquire proprietary longitudinal field data capturing real-world interactions between FLEs and patients in mental healthcare. Grounded in social support theory, our study investigates how distinct FLE behaviors—such as ensuring, reminding, reflecting, and accompanying—influence adherence outcomes across multiple domains, including communication and cognitive functioning, daily living tasks, and broader goals related to social and community integration. Using split hazard regression, we identify which FLE behaviors facilitate adherence and how these behaviors influence both the likelihood and timing of improvement.
Our findings underscore the importance of tailored behavioral strategies in supporting adherence across these domains. Specifically, behaviors that involve actively listening and engaging dialogue significantly enhance adherence outcomes, whereas repetitive and disengaged behaviors reduce the adherence likelihood by up to 5.28% and delay progress. These findings yield several key contributions.
First, we advance the TSR literature by positioning mental healthcare interactions with chronically mentally ill individuals as a vital context for understanding service delivery to vulnerable consumers (Boenigk et al. 2021; Danaher and Gallan 2016; Ostrom et al. 2015). Second, we extend research on medical and behavioral adherence (Bowman, Heilman, and Seetharaman 2004; Chen et al. 2020; Spanjol et al. 2015) by identifying what individuals with chronic mental illness require to progress toward adherence in complex, real-world settings. Third, we enrich the FLE management literature by uncovering context-sensitive actions that FLEs employ during repeated service encounters with cognitively impaired individuals—providing more granular insights into effective service practices. Although our study focuses on mental healthcare, these behavioral insights are relevant to other vulnerable populations, including the elderly, individuals with chronic conditions, and those facing socioeconomic hardship, underscoring the broad applicability of adaptive, person-centered frontline behaviors across service sectors. Fourth, we respond to calls for empirically rigorous research in healthcare services (Danaher et al. 2024; Spanjol et al. 2015), by demonstrating how detailed, real-world interaction data reveal behavioral mechanisms often missed by traditional models—contributing more meaningfully to research on health-related well-being (Golder et al. 2023; Mick 2006; Stremersch et al. 2023).
From a managerial perspective, improving adherence not only enhances clinical outcomes and reduces healthcare costs but also increases service effectiveness. Focusing on the micro-behaviors that shape adherence allows providers to deliver more dignified, autonomous, and responsive care to vulnerable populations—including the mentally ill, elderly, and those in long-term treatment settings. Ultimately, our findings encourage greater sensitivity and deeper understanding of individuals’ needs in sustained relational care environments.
The next section conceptualizes individuals with mental illness as vulnerable consumers and outlines the role of adherence in service delivery. We then introduce social support theory as our guiding framework and review extant literature on FLE service interactions. Subsequent sections detail the dataset, method, and results, followed by theoretical implications, and practice-oriented recommendations. We conclude with a discussion of limitations and outline avenues for future research at the intersection of TSR and mental healthcare.
Conceptual and Theoretical Background
Consumer Vulnerability in Transformative Service Research
TSR is grounded in the pursuit of positive change and the enhancement of well-being across multiple stakeholders, including individual consumers, employees, communities, and broader service ecosystems (Anderson et al. 2013). Evolving from transformative consumer research (TCR), TSR addresses fundamental human challenges and seeks to improve life circumstances shaped by service and consumption. As Mick (2006, p. 2) articulates, both TCR and TSR focus on “investigations that are framed by a fundamental problem or opportunity, and that strive to respect, uphold, and improve life in relation to the myriad conditions, demands, potentialities, and effects of consumptions.” This perspective emphasizes context-sensitive real-world inquiry to identify interventions that meaningfully enhance consumer well-being (Davis and Pechmann 2020). Central to this endeavor is the study of vulnerable consumers—those whose life circumstances may constrain their ability to access, understand, or benefit from services (e.g., Anderson and Ostrom 2015; Mick 2006).
Building on Hill and Sharma (2020) and Mende et al. (2024), we conceptualize consumer vulnerability as a dynamic and situational condition in which individuals face heightened risks of harm due to restricted access to, control over, or capacity to utilize essential resources. These limitations hinder their full participation in social and economic life and may stem from factors such as socioeconomic disadvantage, demographic characteristics, or health-related conditions. Because vulnerability varies in depth and manifestation (Mende et al. 2024), addressing it requires context-specific, empowering strategies that mitigate risks while fostering resilience and agency.
Following Danaher and Gallan (2016), this study contributes to TSR by focusing on a highly vulnerable population: individuals with behavioral and mental health conditions. People with mental illness often face cognitive, emotional, and behavioral challenges that impede healthcare decision-making and complicate treatment adherence (Dixon, Holoshitz, and Nossel 2016; World Health Organization 2022). Stigma further compounds these barriers by fostering marginalization, isolation, and reliance on care professionals (Corrigan and Watson 2002; Dodds et al. 2023; Henderson, Evans-Lacko, and Thornicroft 2013). As a result, individuals with mental illness are medically, socially, and psychologically vulnerable, making them a vital focus for transformative inquiry. This study seeks to deepen the understanding of how FLE behaviors can be designed and delivered to support the unique needs of individuals with mental illness to meet the distinct needs of these individuals, thereby promoting well-being, dignity, and autonomy.
Consumer Adherence
Adherence, also referred to as compliance, has long been examined in medical contexts and has gained attention in marketing and service research (Dellande, Gilly, and Graham 2004). Broadly, adherence refers to the extent to which individuals follow prescribed formal or informal rules (Kuiper et al. 2023). Within service contexts, it captures the degree to which consumers act in accordance with provider recommendations (Seiders et al. 2015). Adherence is critical across various domains—including healthcare, financial planning, and wellness counseling—as it ensures that consumers derive the intended value of professional guidance (Wang and Yim 2019). Understanding the factors that drive or impede adherence offers actionable insights to service providers to design more effective interventions, improve service delivery, and enhance consumer outcomes.
In healthcare specifically, adherence reflects individuals’ sustained effort to implement medical or behavioral recommendations—such as taking medication or maintaining healthy routines (Thompson and McCabe 2012; World Health Organization 2003)—to “achieve, maintain or promote optimal levels of functioning, health and well-being” (Laranjeira et al. 2023, p. 9). However, non-adherence remains a pervasive and costly problem, diminishing treatment effectiveness and straining healthcare systems (Sokol et al. 2005). Research shows that up to 50% of individuals fail to follow treatment recommendations, and adherence drops below 20% for complex behavioral regimens like long-term dietary changes or exercise programs (DiMatteo 2004; Kripalani, Yao, and Haynes 2007). Both medication and behavioral lapses contribute to disease relapse, progression, and a marked decline in quality of life. These issues are especially pronounced in mental healthcare, where adherence is complicated by cognitive impairment, emotional dysregulation, and low health literacy. For instance, consumers suffering from depression are 27% more likely to be non-adherent (DiMatteo, Lepper, and Croghan 2000) and often rely on structured, trust-based service interactions to manage daily routines (Thompson and McCabe 2012).
In this context, interpersonal dynamics become pivotal as consistent and attuned interactions with care professionals enhance adherence (DiMatteo 2004; Street, Gordon, and Haidet 2007). Such relationships motivate individuals to stay committed to therapeutic goals (Allen, Sugarman, and Wennerstrom 2017). Yet, despite the recognized importance of service interactions, the literature provides little insight into which specific FLE behaviors most effectively support adherence among individuals with mental illness.
Social Support in Mental Healthcare Services
We reason that for vulnerable consumers, such as individuals with chronic mental conditions, social support serves as a pivotal mechanism in fostering both medical and behavioral adherence. The role of social relationships in promoting well-being has long been recognized across disciplines, with research consistently highlighting their importance in coping with adversity and promoting resilience (Bambina 2007). Originally introduced by Cobb (1976), social support is conceptualized as a protective factor that buffers individuals from the adverse effects of life stress. According to social support theory, access to supportive social relationships significantly enhances well-being, adaptability, and physical and mental health outcomes (Cobb 1976). In healthcare settings, FLEs—as consistent and trusted figures—play a particularly influential role in providing this support, often acting as critical sources of stability and emotional scaffolding for individuals experiencing chronic distress (Cohen and Wills 1985; Nausheen et al. 2009; Yao, Zheng, and Fan 2015). Research shows that individuals in stable support networks are more likely to follow treatment, experience less depression and anxiety, and face lower relapse risk (Cohen and Wills 1985; Uchino 2006; World Health Organization 2003). These benefits are especially critical in mental healthcare, where illness often involves clinical symptoms alongside cognitive, emotional, and social challenges. Thus, the relational context of care is a central determinant of adherence.
Given the heterogeneous nature of mental health experiences, we adopt a social support theory lens without imposing predefined hypotheses. Instead, we employ a grounded, empirics-first approach aligned with calls for contextual specificity and interpretive flexibility in TSR. This enables practice-oriented insights without oversimplifying complex psychosocial dynamics (Golder et al. 2023) and allows for a grounded and nuanced, yet specific understanding (Madan et al. 2023; Stremersch et al. 2023) that builds on adherence research across service domains. To structure our analysis, we draw on the foundations developed by Berkman et al. (2000), Taylor (2014), and Robinson et al. (2019), and delineate four distinct types of social support.
Instrumental Support refers to tangible assistance with tasks or resources that help individuals meet their daily needs or achieve specific goals. It involves actions that directly contribute to a person’s well-being or functioning (Cohen and Wills 1985). Instrumental support encompasses a range of behaviors including ensuring that individuals’ basic needs are met (Thoits 2011), monitoring for early risk indicators (Semmer et al. 2008), and administering medication (Cutrona and Russell 1990).
Informational Support comprises guidance, advice, and feedback that facilitate understanding and informed decision-making (Berkman et al. 2000; Bitner, Booms, and Tetreault 1990). In mental healthcare, this includes explaining care plans, reinforcing information, or reminding patients about scheduled activities and appointments (Cohen and Wills 1985; Thoits 2011).
Emotional Support comprises expressions of empathy, reassurance, and validation that alleviate psychological distress (Berkman et al. 2000) and help individuals feel valued and less isolated (Cobb 1976; Finn 1999). In mental healthcare, it is fundamental in nurturing an individual’s psychological resilience and emotional stability. This includes motivational encouragement, reflective dialogue, and feedback that enhance self-awareness and emotional regulation (Cutrona and Russell, 1990; Thoits 2011). By being involved in meaningful dialogue through listening and active conversations, FLEs create a supportive environment to foster a sense of connection and validation (Semmer et al. 2008; Thoits 2011).
Integrational Support, also referred to as companionship (Rosenbaum, Baniya, and Seger-Guttmann 2017), fosters belonging, social identity, and community participation (Robinson et al. 2019). Although less studied (Cutrona and Russell 1990), it is especially critical in mental health, where social isolation is a major risk factor (Henderson, Evans-Lacko, and Thornicroft 2013). Professionals help mitigate isolation by engaging in shared activities that promote sustained social integration (Robinson et al. 2019). Integrational support thus encompasses efforts to promote inclusion, companionship, and social participation (Berkman et al. 2000; House, Umberson, and Landis 1988). One of its core expressions lies in the act of “accompanying” the individual—either through physical presence or active involvement in their lived experiences—which reflects the dynamic and participatory nature of social activity (Berkman et al. 2000; Cohen and Wills 1985).
Frontline Employee Behaviors and Their Role in Social Support Interactions
FLEs are the visible representatives of organizations, shaping customer experiences, influencing satisfaction, loyalty, and retention (Bitner, Booms, and Tetreault 1990; Zeithaml, Bitner, and Gremler 2010). In the context of healthcare services, FLEs can influence adherence by shaping experiences in service interactions (Berry and Bendapudi 2007; Seiders et al. 2015; Thompson and McCabe 2012).
Drawing on social support theory, we categorize FLE behaviors across the four dimensions described above and examine their distinct effects on adherence outcomes (see Table 1). 2 Table 1 summarizes the study’s contribution relative to past research on FLE management, frontline interactions in healthcare services, and adherence. Service research typically contrasts the effects of instrumental and emotional behaviors (e.g., Güntürkün, Haumann, and Mikolon 2020; Marinova, Singh, and Singh 2018; Sirdeshmukh, Singh, and Sabol 2002), whereas healthcare studies often emphasize informational versus emotional behaviors (e.g., Dellande, Gilly, and Graham 2004; Hausman 2004). Prior work shows that instrumental behaviors—such as demonstrating competence, proactive engagement, and effective problem resolution—enhance customer satisfaction (Marinova, Singh, and Singh 2018), transactional outcomes like share of wallet and purchase intentions (Güntürkün, Haumann, and Mikolon 2020), and relational outcomes including trust and loyalty (Sirdeshmukh, Singh, and Sabol 2002). Informational support, such as advice and knowledge-sharing, similarly fosters trust and rapport (Gremler and Gwinner 2008; Sirdeshmukh, Singh, and Sabol 2002), demonstrating that both support types contribute not only to functional success but also to relationship development. In healthcare, informational support is particularly impactful. Studies by Hausman (2004) and Dellande, Gilly, and Graham (2004) emphasize its role in enhancing adherence and satisfaction, while Seiders et al. (2015) and Chen et al. (2020) find that it contributes to operational metrics like reduced service costs and higher screening completion rates.
Literature Review.
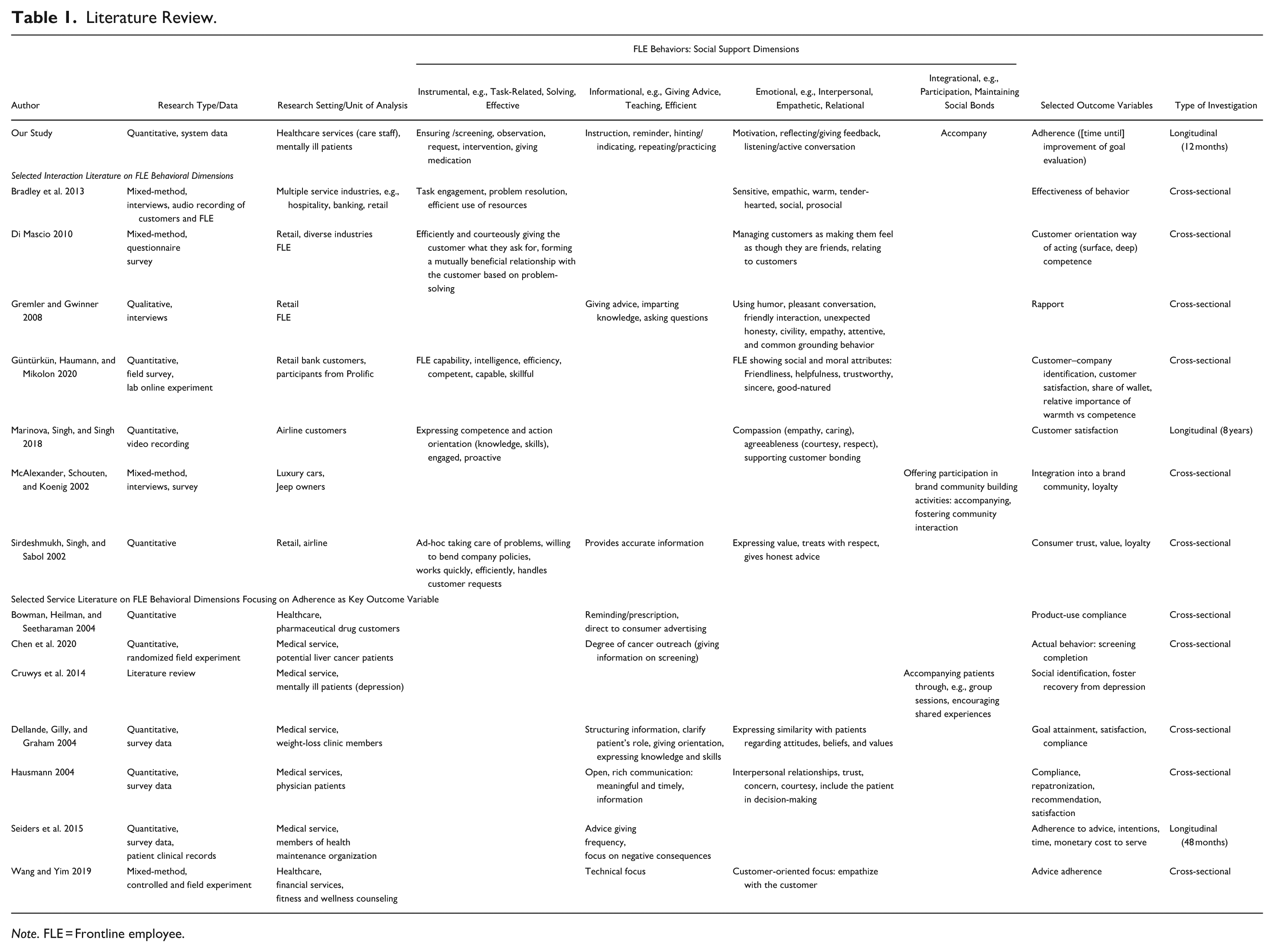
Note. FLE = Frontline employee.
In contrast, relational behaviors—such as empathy, kindness, and courteousness—are instrumental in strengthening the consumer–provider bond beyond financial metrics (Güntürkün, Haumann, and Mikolon 2020). These behaviors build trust (Sirdeshmukh, Singh, and Sabol 2002), rapport (Gremler and Gwinner 2008), satisfaction (Marinova, Singh, and Singh 2018), and long-term loyalty, while also supporting adherence (Dellande, Gilly, and Graham 2004; Hausman 2004; Wang and Yim 2019).
Interestingly, Marinova, Singh, and Singh (2018) reveal that the effectiveness of FLE behavior evolves over the course of interactions; instrumental work boosts satisfaction but diminishes when paired with excessive relational behavior. These insights underscore the need for nuanced and flexible FLE strategies—an idea echoed by Wang and Yim (2019), who show that adaptive behavior enhances the effectiveness of advice and adherence outcomes.
Moreover, social integration behaviors extend the benefits of emotional and informational support by strengthening belonging and shared identity (Cruwys et al. 2014; McAlexander, Schouten, and Koenig 2002). For instance, in brand communities, FLE participation reinforces loyalty and advocacy (McAlexander, Schouten, and Koenig 2002; Schau, Muñiz, and Arnould 2009). In healthcare, FLEs’ involvement in peer support groups or communal sessions enables individuals to connect, and share experiences, fostering social identity and facilitating recovery (Cruwys et al. 2014).
Our study is among the few longitudinal investigations within this service domain, and to our knowledge, the only study focused on mental health and adherence. Moreover, it is the first to simultaneously examine all four dimensions of social support—instrumental, informational, emotional, and integrational. This multifaceted perspective offers actionable insights for providers and support networks aiming to enhance medical and behavioral adherence among vulnerable populations, ultimately contributing to improved well-being and quality of life for individuals with chronic mental health conditions.
Method
Research Setting
We conducted our study in collaboration with a large hospital network in Germany that provides a range of services, including stationary long-term care for individuals with mental disorders and disabilities (see Supplemental Appendix A for a comprehensive overview of the study context). Longitudinal data were collected over a 12-month period, from January to December 2021. The dataset includes FLEs’ daily log entries from the hospital’s administrative system, capturing records of patient-related activities, evaluations of adherence, and detailed documentation of FLE behaviors during interactions with individuals. 3 These recorded behaviors were categorized into broader activity types based on the Nursing Interventions Classification (NIC) (Butcher et al. 2018), a standardized framework widely adopted for care documentation and management. Utilizing NIC ensured evidence-based alignment and consistent categorization for systematic comparison. Supplemental Appendix B provides a detailed mapping of the behavior categories, corresponding NIC intervention examples, and their classification into specific dimensions of social support.
To ensure the reliability of our categorization into social support dimensions, an intercoder reliability analysis was conducted. Two independent coders classified each behavior into one of the four social support dimensions. Agreement between coders was assessed using Cohen’s Kappa, a statistic accounting for agreement occurring by chance. The resulting Kappa value of 0.89 indicates a high level of consistency. Remaining discrepancies were resolved through discussion, reinforcing the validity and robustness of our classification.
Sample
To enable longitudinal analysis of adherence, we selected patients who had undergone at least two adherence assessments over time. 4 This yielded a dataset of 118 patients (out of a total of 273) observed continuously over a 12-month period across 19 group homes. On average, each patient had 10 personalized adherence-related goals, resulting in a total of 2,445 patient-adherence evaluations. 5 The sample included individuals with the following primary diagnoses: schizophrenia (38.9%), intellectual disability (24.1%), and other psychiatric conditions (37.0%). 6 This distribution reflects a mix of moderate to severe mental health conditions. Additionally, group homes were heterogeneous in terms of the FLEs providing care and the diagnoses of fellow residents. Table 2 presents the demographic and diagnostic characteristics of the sample, broken down by adherence/goal area. As individuals often have goals across multiple domains, they may appear in more than one subsample.
Sample Demographics.
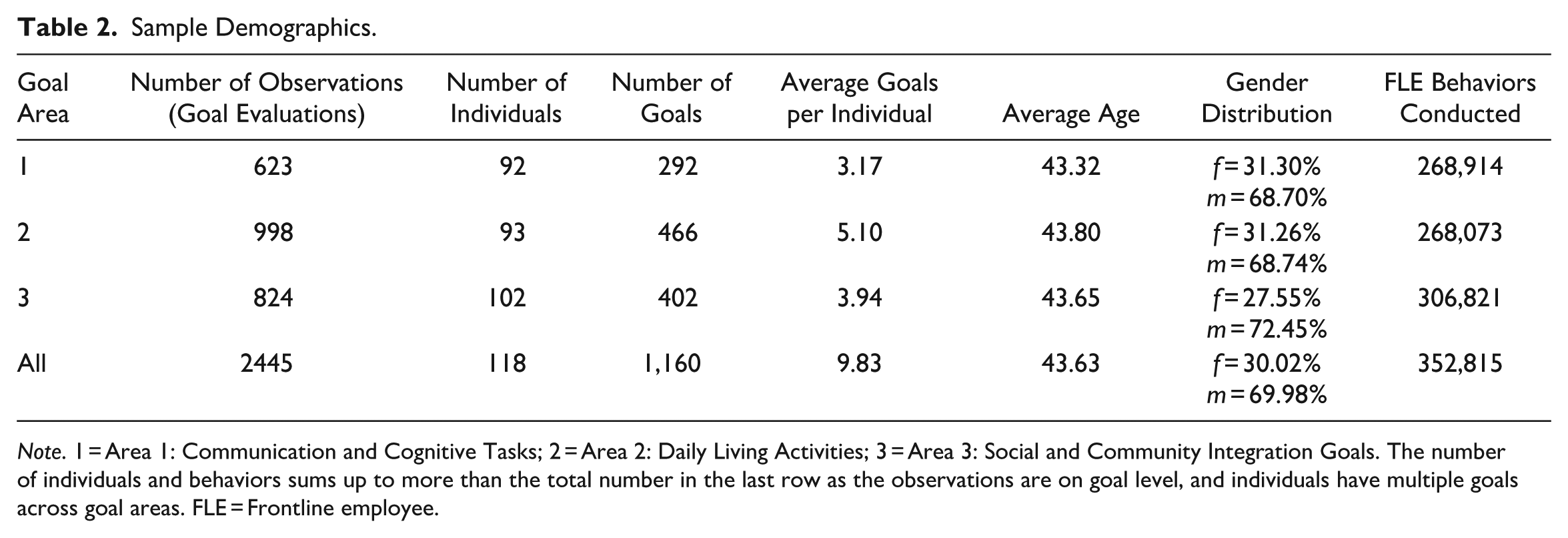
Note. 1 = Area 1: Communication and Cognitive Tasks; 2 = Area 2: Daily Living Activities; 3 = Area 3: Social and Community Integration Goals. The number of individuals and behaviors sums up to more than the total number in the last row as the observations are on goal level, and individuals have multiple goals across goal areas. FLE = Frontline employee.
Adherence Measure
We operationalized adherence through improvements in individualized treatment goals (Ley and Putz 2024). This approach was chosen for three key reasons. First, these improvements reflect individuals’ progress toward personalized well-being-related goals, moving beyond standardized symptom reduction. Given the heterogeneity of mental disorders and disabilities, adherence should not be evaluated through a uniform clinical lens. Instead, tracking improvements in individually defined medical and behavioral goals offers a more meaningful, context-sensitive measure of treatment effectiveness (Berry and Bendapudi 2007). As one FLE manager from our partner organization remarked: “The support plan is built upon everyday experiences from the first few weeks [of stay] and then the diagnoses become secondary.” This perspective aligns with patient-centered care principles, which emphasize personalized goal-setting as a core element of effective treatment, and also reflects a recovery-oriented approach that emphasizes autonomy and participation in the care process (Bray 2021; NSW Health 2022). Second, empirical evidence supports the notion that mental healthcare interventions are often more successful in facilitating personal goal attainment than in achieving symptom relief (Boeykens et al. 2022; Lindhiem et al. 2016). Third, goal-setting as a therapeutic strategy has been demonstrated across a wide range of mental health conditions (Stewart et al. 2022). Therefore, our adherence measure—based on goal evaluations—captures both the complexity of mental health care and the value of individualized, goal-based progress.
The goals in our sample covered both behavioral change and maintenance (Yang, Stamatogiannakis, and Chattopadhyay 2015), with 56.97% classified as change-oriented and 43.03% as maintenance-oriented. These categories reflect that both small improvements and maintaining stability can be a significant achievement in long-term mental health care (Götz, Gosling, and Rentfrow 2022; World Health Organization 2003). Each goal was assessed using a three-point scale (1 = not achieved, 2 = in progress, 3 = achieved). Importantly, the primary caregivers, that is, FLEs who provided direct care and adherence evaluation, were not the same FLEs who interacted with the individuals on a daily basis, although they were fully informed about the individual goals. This separation of roles reduces the risk of common method bias in our data. We defined adherence as a binary outcome based on sequential goal evaluations: a value of 1 indicated an improvement from time t − 1 to time t, while 0 indicated no improvement. Overall, 7.03% of all goals showed improvement during the study period, with an average improvement duration of 8.6 months.
Goal Domains
Each evaluated goal was linked to one of nine goal domains, as defined by the WHO International Classification of Functioning, Disability and Health (World Health Organization 2001). Following the structure of the WHO Disability Assessment Schedule (WHO DAS) (World Health Organization 2010), these nine domains were grouped into three overarching areas of functioning: Area 1 comprises Communication and Cognitive Tasks (including goal domains focused on Learning and Knowledge, General Tasks, and Communication). This corresponds to body functions and structures in WHO DAS. Area 2 covers Daily Living Activities (including goal domains focused on Mobility, Selfcare, and Domestic Life), reflecting the activities dimension of WHO DAS. Area 3 encompasses Social and Community Integration (including goal domains focused on Interpersonal Relationships, Meaningful Areas of Life, Community and Social Life). These domains align with the participation component of WHO DAS. Together, these areas provide a framework for evaluating long-term care needs and improvements.
Operationalizing FLE behaviors
Over the 12-month observation period, each individual experienced between 2,500 and 3,000 documented interactions with 21 different FLEs (caregivers) on average. For the analysis, behaviors were operationalized as the cumulative frequency of each type of behavior type recorded in the daily logs up to the point of each evaluation. In our data, we specifically cover the following behaviors: ensuring/screening, observation, request, intervention, giving medication (instrumental support); instruction/guidance, reminder, indicating/hinting, repeating/practicing (informational support); motivation, reflecting/giving feedback, listening/active conversation (emotional support); and accompany (integrational support). Detailed definitions and corresponding NIC codes for each behavior are provided in Supplemental Appendix B. To enhance interpretability, all behavior measures were standardized. 7 Multicollinearity was ruled out based on variance inflation factors, which were uniformly <5.
Analysis
To assess the impact of FLE behaviors on adherence, we utilize a split hazard regression model, which has two distinct components (e.g., Prins and Verhoef 2007; Schmidt and Witte 1989; Sinha and Chandrashekaran 1992). First, the logit component estimates the probability of goal improvement due to various FLE behaviors while controlling for individuals’ age, gender, diagnosis, and goal type (change vs. maintenance) as well as goal domain (within the specific area). This part of the model accounts for the likelihood that a goal will improve. Second, the hazard component models the time to improvement using a Weibull distribution, which is well-suited for capturing varying hazard rates over time and aligns with the dynamic nature of adherence. This part of the model estimates the timing of improvement for those goals that do eventually improve, accommodating right-censored data, and recognizing that improvements might take place beyond the time window of our research. In addition, the Weibull distribution allows for different shapes of hazard functions (Chintagunta and Dong 2006). By integrating these two components, our approach provides a comprehensive analysis of both the probability and timing of goal improvement (Figure 1).
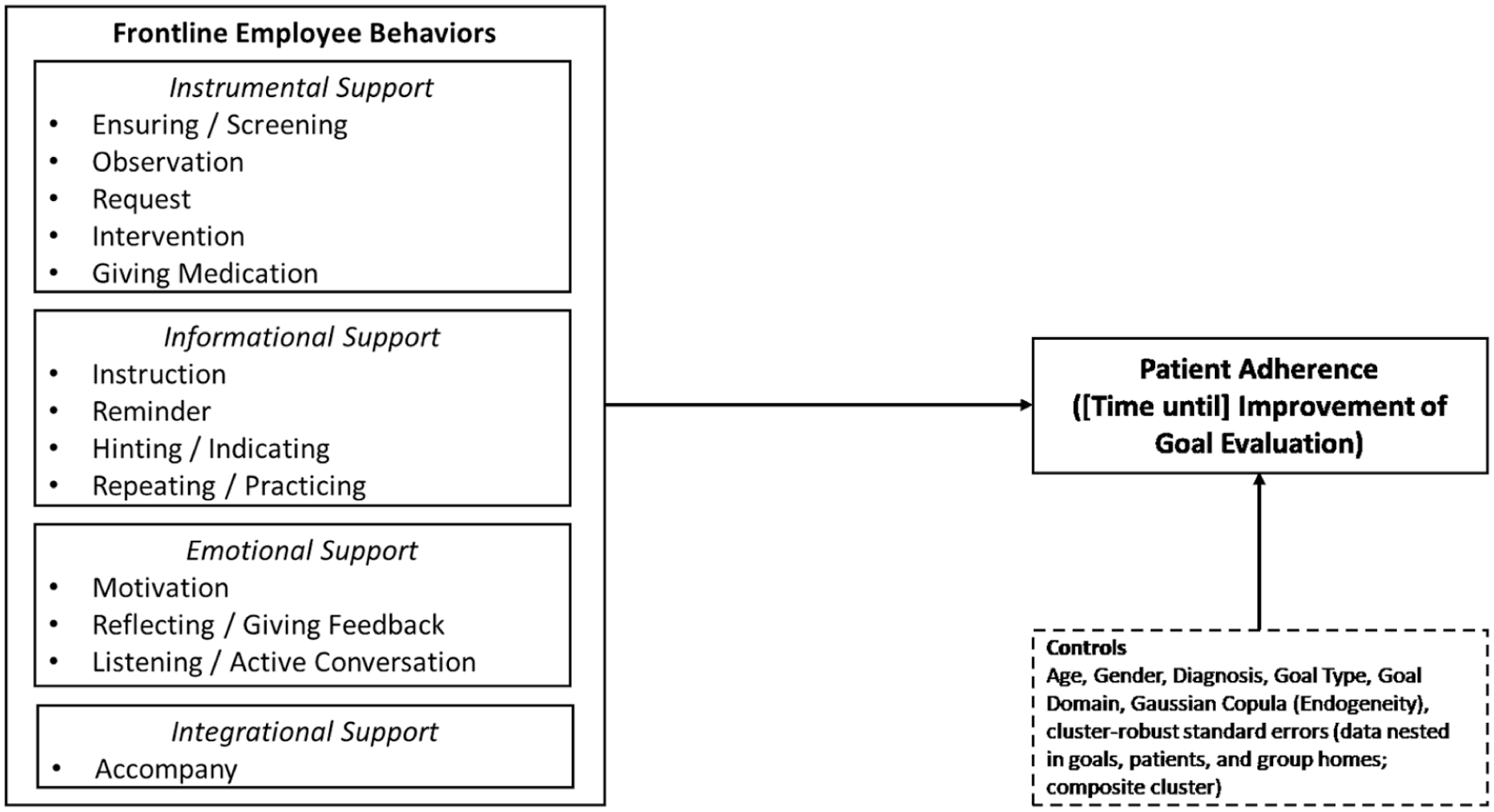
Conceptual framework.
Selection
We conduct separate analyses for the goal area clusters described above. As the three samples are subsets of all group home residents, we applied a two-stage Heckman correction (Heckman 1979). In the first stage, we model the probability of selection of an individual for our sample as a function of age, gender, diagnosis, and number of side diagnoses. Next, we calculated the inverse Mills ratio (IMR) for all observations and included the values as an additional explanatory variable in our subsequent analyses.
Endogeneity
To rule out endogeneity concerns from omitted variable bias, we utilize a Gaussian copula approach, after testing the assumptions of non-normally distributed regressors (Papies, Ebbes, and van Heerde 2017; Park and Gupta 2012). We first included Gaussian copulas for all frontline behaviors, as these are potentially prone to endogeneity due to simultaneity with individuals’ actions. To reduce model complexity, we later removed copula terms that were not significant.
Model
Because goal evaluations are nested within goals, which, in turn, are nested within individuals, all residing within group homes, we incorporated cluster robust standard errors based on the composite clusters. This strategy allows us to capture correlations within and between different levels of the data hierarchy. The model is specified as follows:


where
Results
Tables 3 through 5 provide an overview of our findings. The correlations between all variables included in our analysis can be found in Supplemental Appendix C. Note that in the split hazard regression, the estimated coefficients indicate the impact of the variables (a) on the probability of the event (logit, stage 1), and (b) the impact of the variables on the timing of the event (hazard, stage 2). As the split hazard model is parameterized, positive coefficients indicate an increase in the mean time until improvement, which is the opposite of the interpretation in the Cox hazard regression, in which a positive coefficient implies a positive impact on the hazard and a reduction in the mean time, for example, until adoption (Mallapragada, Grewal, and Lilien 2012; Sinha and Chandrashekaran 1992). To facilitate interpretation, we exponentiate the standardized coefficients to obtain effect sizes of odds ratios (ORs) for the logit stage and time ratios (TRs) for the hazard stage. These ratios show how much the odds or time change when a behavior increases by one standard deviation.
Results of Split Hazard Regression for Communication and Cognitive Task Goals (Area 1).
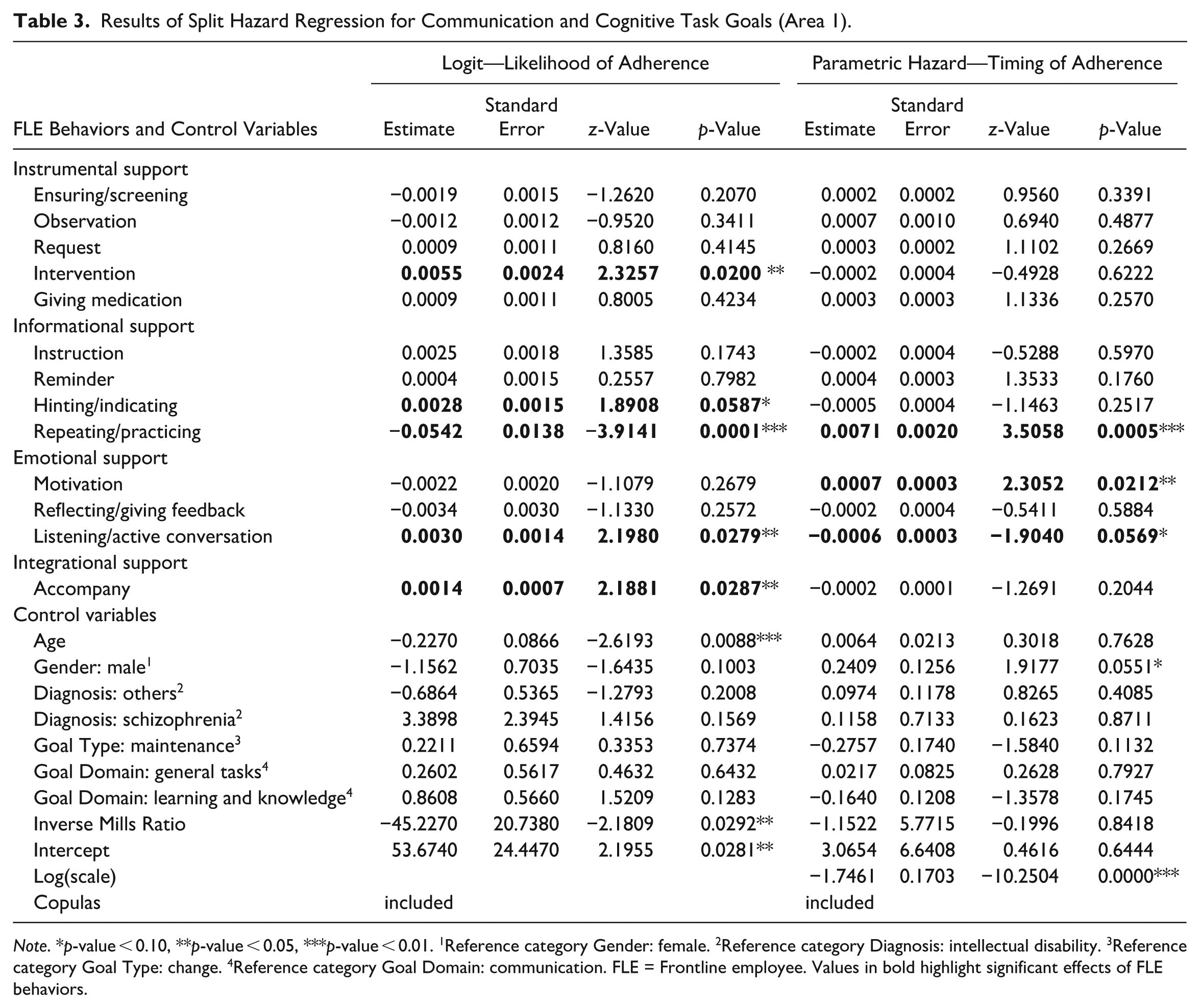
Note. *p-value < 0.10, **p-value < 0.05, ***p-value < 0.01. 1Reference category Gender: female. 2Reference category Diagnosis: intellectual disability. 3Reference category Goal Type: change. 4Reference category Goal Domain: communication. FLE = Frontline employee. Values in bold highlight significant effects of FLE behaviors.
In the first goal area, Communication and Cognitive Tasks, intervention (β = 0.0055, OR = 1.006, p < 0.05 (two-tailed)), hinting/indicating (β = 0.0028, OR = 1.003, p < 0.10), listening/active conversation (β = 0.0030, OR = 1.003, p < 0.05), and accompanying (β = 0.0014, OR = 1.001, p < 0.05) have a positive effect on improvement likelihood, while repeating has a negative effect (β = −0.0542, OR = 0.947, p < 0.01) per equation 1. In the parametric hazard model (Equation 2), we find that while listening/active conversation (β = −0.0006, TR = 0.999, p < 0.10) marginally reduces the time until improvement, repeating/practicing (β = 0.0071, TR = 1.007, p < 0.01) and motivation (β = 0.0007, TR = 1.001, p < 0.05) increase the time until improvement occurs (see Table 3 for details).
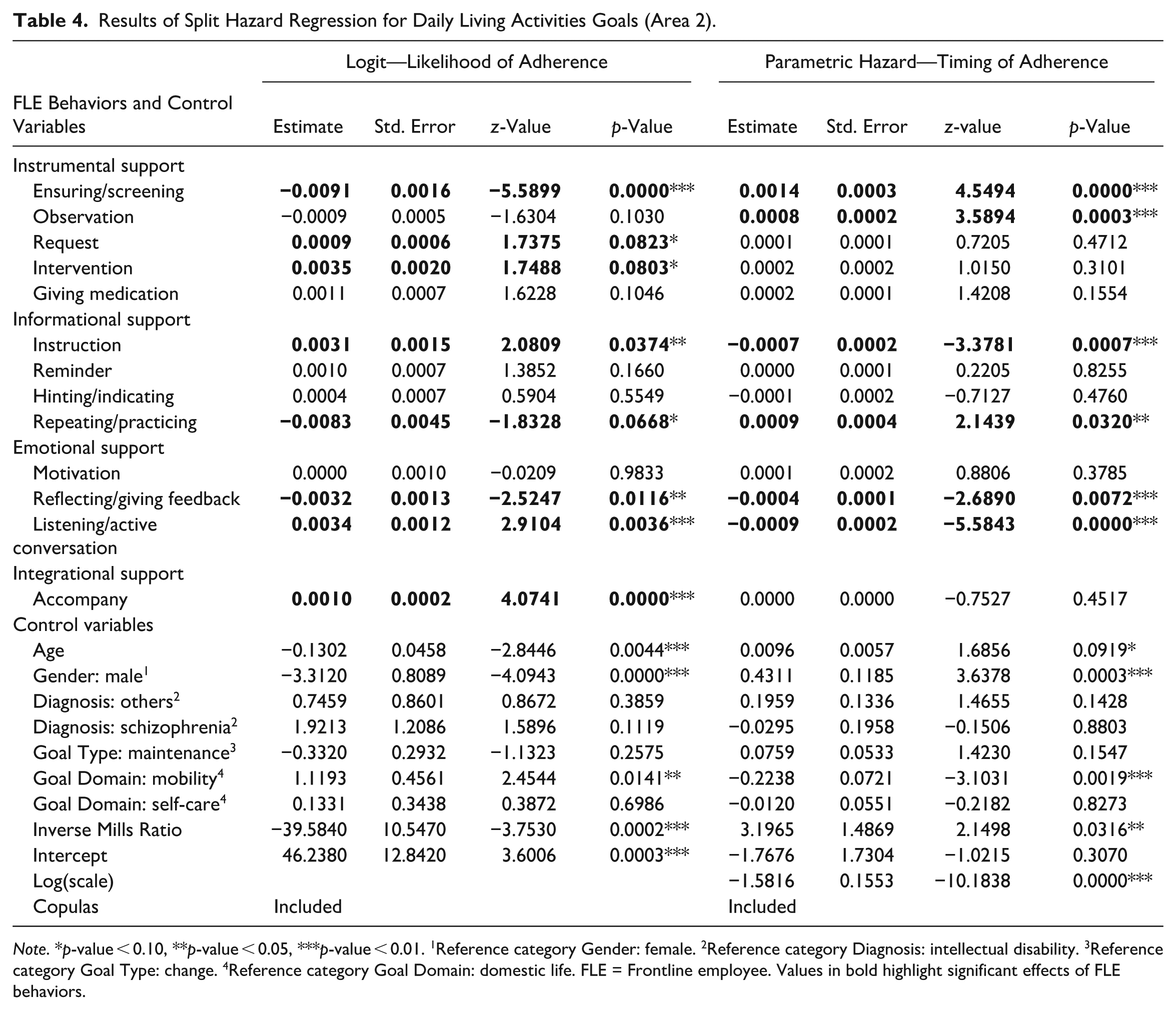
The second area, encompassing goals related to Daily Living Activities, we find that on the one hand, requests (β = 0.0009, OR = 1.001, p < 0.10), intervention (β = 0.0035, OR = 1.004, p < 0.10), instruction (β = 0.0031, OR = 1.003, p < 0.05), listening/active conversation (β = 0.0034, OR = 1.003, p < 0.01), and accompanying individuals (β = 0.0010, OR = 1.001, p < 0.01) increase the likelihood of improvement. On the other hand, ensuring/screening (β = −0.0091, OR = 0.991, p < 0.01), repeating/practicing (β = −0.0083, OR = 0.992, p < 0.10), and reflecting/giving feedback (β = −0.0032, OR = 0.997, p < 0.05) decrease the likelihood of improvement. The parametric hazard model shows that instruction (β = −0.0007, TR = 0.999, p < 0.01), reflecting/giving feedback (β = −0.0004, TR = 0.999, p < 0.01) and listening/active conversation (β = −0.0009, TR = 0.999, p < 0.01) reduce the time until improvement occurs, while ensuring/screening (β = 0.0014, TR = 1.001, p < 0.01), observation (β = 0.0008, TR = 1.001, p < 0.01), and repeating/practicing (β = 0.0009, TR = 1.001, p < 0.05) increase it (see Table 4 for details).
Results of Split Hazard Regression for Daily Living Activities Goals (Area 2).
Note. *p-value < 0.10, **p-value < 0.05, ***p-value < 0.01. 1Reference category Gender: female. 2Reference category Diagnosis: intellectual disability. 3Reference category Goal Type: change. 4Reference category Goal Domain: domestic life. FLE = Frontline employee. Values in bold highlight significant effects of FLE behaviors.
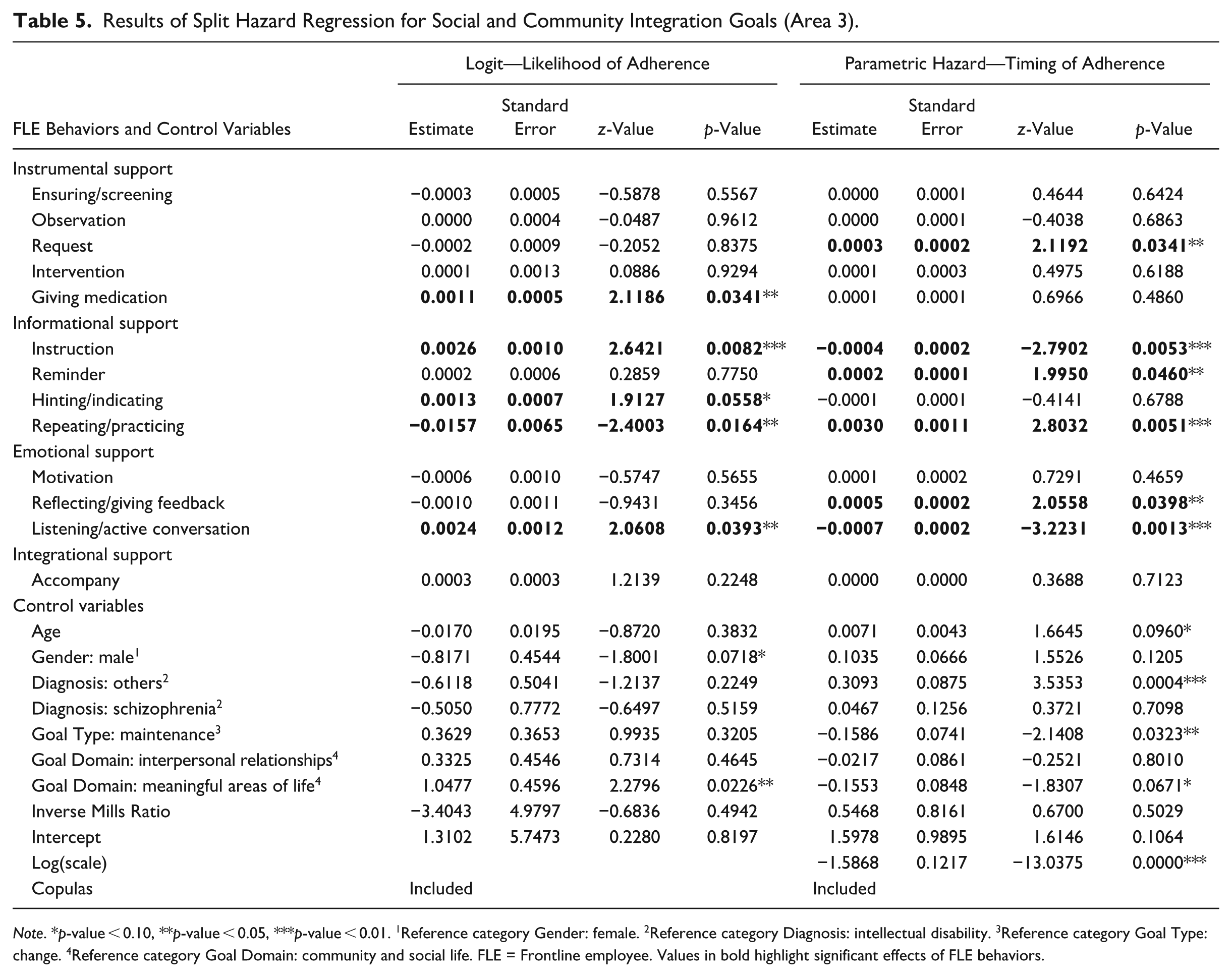
Lastly, in area three, which focuses on the improvement of goals related to Social and Community Integration, again listening/active conversation positively affects the likelihood of improvement (β = 0.0024, OR = 1.002, p < 0.05), as well as giving medication (β = 0.0011, OR = 1.001, p < 0.05), instruction (β = 0.0026, OR = 1.003, p < 0.01), and hinting/indicating (β = 0.0013, OR = 1.001, p < 0.10). On the contrary, repeating/practicing, as in the other two areas, reduces the likelihood of improvement (β = −0.0157, OR = 0.984, p < 0.05). In the parametric hazard model, instructions reduce the time until improvement (β = −0.0004, TR = 0.999, p < 0.01). In addition, as is the case in all other areas, listening/active conversation reduces the time until improvement occurs (β = −0.0007, TR = 0.999, p < 0.01). However, for requests (β = 0.0003, TR = 1.0003, p < 0.05), reminders (β = 0.0002, TR = 1.0002, p < 0.05), repeating/practicing (β = 0.0030, TR = 1.003, p < 0.01), and reflecting/giving feedback (β = 0.0005, TR = 1.001, p < 0.05) we see an increase in the time until improvement (see Table 5).
Results of Split Hazard Regression for Social and Community Integration Goals (Area 3).
Note. *p-value < 0.10, **p-value < 0.05, ***p-value < 0.01. 1Reference category Gender: female. 2Reference category Diagnosis: intellectual disability. 3Reference category Goal Type: change. 4Reference category Goal Domain: community and social life. FLE = Frontline employee. Values in bold highlight significant effects of FLE behaviors.
Table 6 summarizes our results and thus provides a comprehensive overview for the discussions of our findings.
Summary of Split Hazard Regression Results.
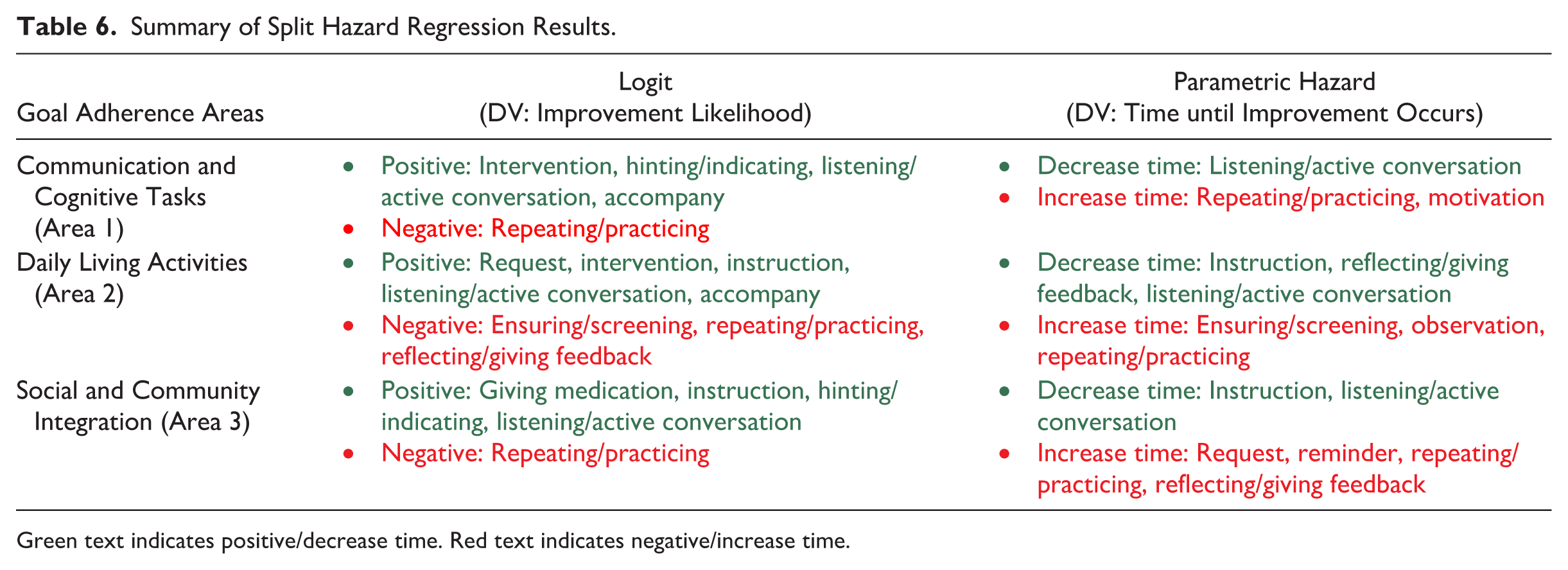
Green text indicates positive/decrease time. Red text indicates negative/increase time.
Discussion
FLEs play a pivotal role in determining treatment success and overall progress toward improved well-being for individuals with mental illness (Allen, Sugarman, and Wennerstrom 2017). The behavior of healthcare providers, especially those who interact directly with patients, substantially influence adherence, emotional recovery, and broader therapeutic outcomes (Brady and Cronin 2001; Di Mascio 2010; Hausman 2004). In what follows, we first discuss the consistent positive and negative effects of FLE behaviors across goal domains, and then examine how specific behaviors operate within distinct functional areas.
Listening and Active Communication as Catalysts for Adherence
Our findings highlight the consistent positive influence of FLE listening and active conversation across all care domains. These behaviors foster trust, validate individuals’ experiences, and cultivate a sense of psychological safety—factors critical to supporting vulnerable populations (McCabe and Priebe 2004). Their impact is robust regardless of whether interactions center on basic care tasks or more complex relational needs. This aligns with prior work emphasizing the foundational importance of trust and strong consumer–provider relationships in service delivery (Bradley et al. 2013; Di Mascio 2010).
Risks of Authoritarian Communication
In contrast, behaviors characterized by excessive repetition or pressured communication tend to diminish autonomy and provoke resistance, thereby impeding progress across domains. As one manager in our partner organization noted: “Especially in areas for people with mental disabilities, frequent ‘reminding’ can be ‘annoying,’ leading to people tuning out.” This observation resonates with Wampold (2015), who argues that therapeutic environments must safeguard individuals’ sense of agency and avoid coercion. Interestingly, these results diverge from findings in general healthcare contexts, where emphasizing negative consequences may promote adherence (Seiders et al. 2015). In mental healthcare, however, such strategies can backfire, underscoring the need for context-sensitive communication that respects psychological autonomy.
Communication and Cognitive Tasks
In the realm of Communication and Cognitive Tasks, behaviors offering supportive interventions, such as offering hints or accompanying individuals during tasks were most effective in promoting learning and information exchange. These actions reflect constructive forms of guidance that align with prior research highlighting the benefits of supportive advice in improving therapeutic outcomes (Seiders et al. 2015). By contrast, motivational strategies rooted in coercion or pressure were detrimental, impeding progress in communication and cognitive functioning.
Daily Living Activities
When dealing with Daily Living Activities, direct support in everyday tasks—such as providing structured instructions or physical accompaniment—proved beneficial when it fostered a sense of structure and competence (e.g., Marinova, Singh, and Singh 2018; Sirdeshmukh, Singh, and Sabol 2002). Nevertheless, over-involvement, such as constant supervision or intrusive monitoring, had adverse effects. Such overreach may be perceived as infantilizing or controlling, reducing autonomy, and potentially exacerbating symptoms. These findings are consistent with self-determination theory (Deci and Ryan 2000), which emphasizes autonomy as a core psychological need. Reflective practices were also beneficial when targeted and purposeful but counterproductive when excessive, as unfocused reflection may devolve into rumination, which has been linked to adverse mental health outcomes (Nolen-Hoeksema 2000).
Social and Community Integration
FLE behaviors that promote gradual, structured Social and Community Integration, such as giving instructions or providing cues, proved most effective. These actions support community participation without overwhelming individuals, consistent with findings from broader service research (Gremler and Gwinner 2008; Sirdeshmukh, Singh, and Sabol 2002). Individuals also reported valuing medication support in this domain, as it enhances their sense of stability and enables them to focus on reintegration efforts. Conversely, behaviors involving reminders, requests, or excessive reflection slowed progress, particularly as individuals grew more confident and autonomous. These findings reinforce the importance of adaptive, flexible care that evolves as individuals become more confident and independent. Importantly, our data indicate that the need for integrational support diminishes as individuals become more socially integrated and self-sufficient. As a manager from our partner organization observed: “In participation planning, this is often justified by increased independence. These are [the individuals’] own plans and implementations.” This trajectory aligns with broader recovery frameworks that view psychological improvement as a process of increasing self-efficacy and social connectedness (Anthony 1993). Nonetheless, consistent with prior work (Cruwys et al. 2014), our findings suggest that accompaniment remains valuable in early adherence stages, particularly in the domains of communication, cognitive tasks, and daily functioning.
Overall, the behaviors of frontline healthcare employees have a profound impact on the treatment trajectories of mentally ill individuals. Our findings demonstrate that empathetic communication, especially active listening and engaging dialogue, enhances adherence and accelerates recovery across domains. Conversely, directive or authoritarian behaviors, even when well-intentioned, can inhibit progress and reduce adherence. Thus, frontline interventions must be tailored to individuals’ needs, emphasizing autonomy, trust, and gradual reintegration into community life.
Research Implications
To the best of our knowledge, no prior research has systematically examined the effectiveness of FLE interactions with individuals suffering from mental disorders or disabilities, particularly with respect to the critical outcome of adherence. By introducing this underexplored yet vital topic, our study advances our understanding of how FLE support influences the well-being of vulnerable consumers and extends research in TSR, adherence, and frontline interaction literature.
Consistent with TSR principles, we explicitly recognize individuals with mental illness as vulnerable consumers warranting focused scholarly attention. The chronic, multifaceted nature of mental health conditions underscores the need for longitudinal service research capturing ongoing relational processes rather than episodic encounters in this unique service interface (Singh et al. 2017). Our research responds to calls in the TSR literature to prioritize services for disadvantaged and vulnerable populations (Boenigk et al. 2021; Danaher and Gallan 2016; Ostrom et al. 2015), particularly in behavioral and mental health.
By positioning adherence as the focal outcome variable, we address one of the key challenges in both healthcare and service research—how to effectively foster and sustain consumer progress toward their treatment goals (Wang and Yim 2019; Yang, Stamatogiannakis, and Chattopadhyay 2015). Through the lens of social support theory, we conceptualize FLE behavior as a multidimensional influence on adherence, identifying four distinct support types: instrumental, informational, emotional, and integrational. This framework builds on existing literature acknowledging the significance of patient-provider interactions in shaping adherence outcomes (DiMatteo 2004), while extending it by articulating how specific FLE support behaviors shape measurable patterns of continuity and persistence. Methodologically, our use of objective, longitudinal data provides a precise lens for examining real-world FLE interactions and adherence trajectories, offering a model for future service research beyond self-reports investigating dynamic, temporal patterns in frontline-consumer interactions (Kahn and Luce 2003).
Within healthcare, our findings extend adherence and patient-provider interaction research by incorporating integrational support, which remains underexplored compared with instrumental, informational, and emotional support. We demonstrate that integrational support, facilitating patients’ reintegration into social networks and community life, is theoretically distinct yet essential for long-term adherence and well-being (Cruwys et al. 2014). This highlights the social mechanisms driving sustained adherence and calls for research on how integrational support interacts with other support types to shape recovery in chronic mental health.
Beyond healthcare, our study contributes to broader service research by demonstrating how FLEs dynamically tailor multiple forms of social support to optimize consumer outcomes. Integrational support, in particular, highlights the importance of relational and social integration processes that can enhance continuity and persistence across service contexts. Future research could explore how support dimensions operate in diverse service environments—such as education, social care, or financial services—and how contextual moderators (e.g., service intensity, emotional labor, or stigma) influence the effectiveness of each support type over time.
In summary, our research pioneers the investigation of FLE behaviors and their influence on adherence among mentally ill individuals—a population that has received limited attention in service literature. By bridging theoretical and empirical gaps, we extend social support theory in healthcare and offer a framework for improving service delivery to vulnerable consumers. These principles—empathetic listening, adaptive support, and tailored interactions—are equally relevant in social services and community programs for elderly or socioeconomically disadvantaged clients. We hope these insights inspire future research and practical interventions that foster more empathetic, adaptive, and effective frontline care.
Implications for Practice
Our study leverages real-life quantitative data to offer actionable insights into the effects of FLE behaviors on adherence, which are summarized in Table 7.
Summary of Managerial Implications.
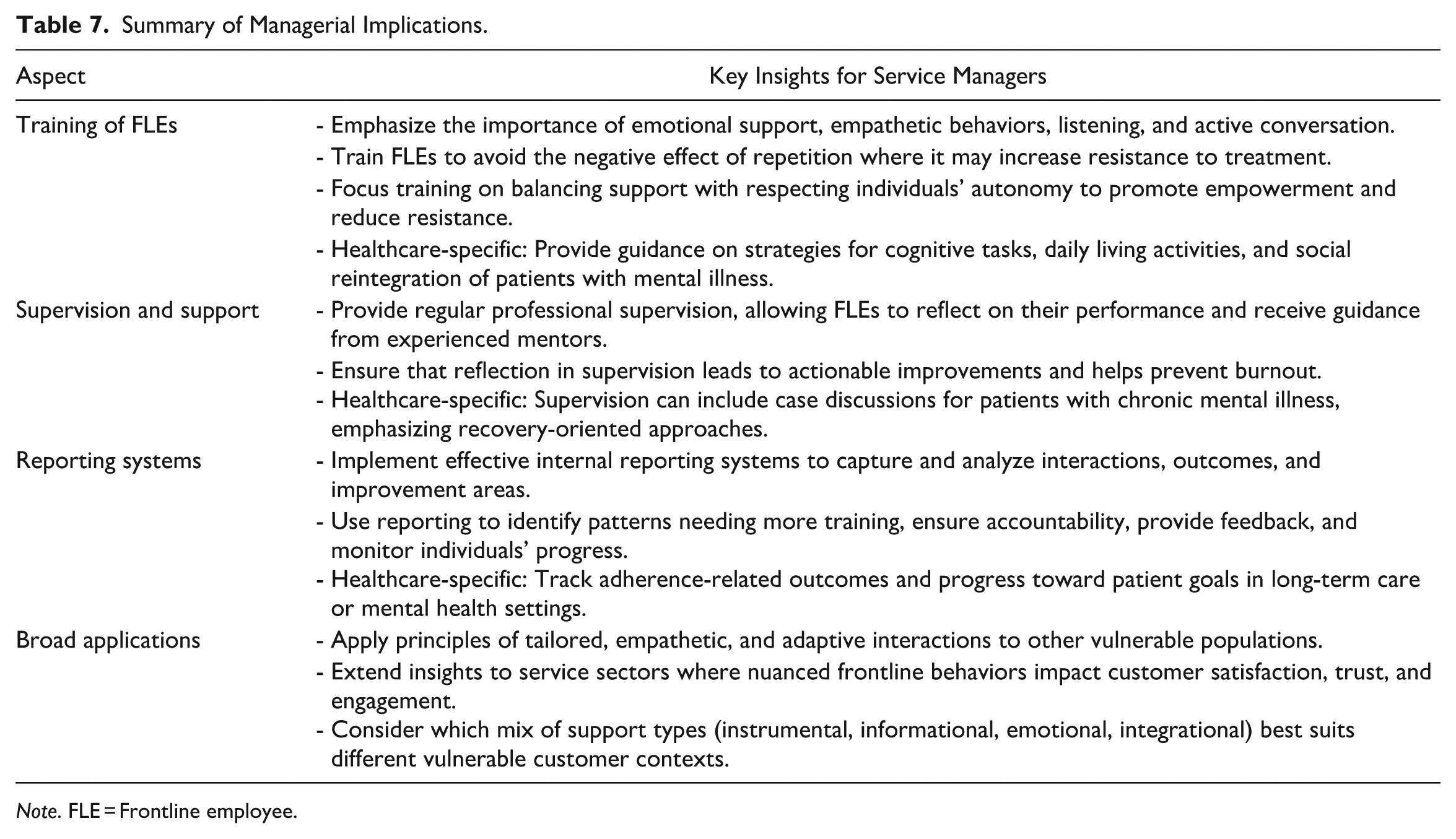
Note. FLE = Frontline employee.
Implications for Mental Healthcare Services
As primary contacts, FLEs shape the therapeutic environment, making their behavior especially consequential in mental healthcare, where sensitive and complex needs of individuals require a nuanced and empathetic approach. Given the unique challenges associated with mental illness, we recommend that healthcare institutions implement targeted FLE training programs focused on adaptive behavioral strategies, consistent with the World Health Organization (World Health Organization 2025a).
Training should emphasize the development of emotional support skills, particularly the ability to engage in empathetic, genuine conversations. Coaching FLEs to actively listen and manage conversations with sensitivity fosters trust and strengthens the therapeutic alliance, both essential for improving adherence. These practices are especially impactful in mental healthcare settings, where feelings of safety and validation boost individuals’ outcomes.
Equally important is discouraging excessive repetition, particularly when providing informational support. A one standard deviation increase in repetition is associated with a 5.28%, 0.83%, and 1.56% decrease in the likelihood of goal improvement across the three areas studied. Repetitive instructions can feel overly directive, diminishing autonomy and increasing resistance. FLEs should tailor communication to individual preferences to promote empowerment and collaboration (Davidson, Rakfeldt, and Strauss 2010).
Training should help FLEs balance instrumental, informational, emotional, and integrational support, tailored to individuals’ functional needs. For instance, instrumental support guides practical tasks, informational support provides clear guidance without overloading the individual, emotional support builds trust and validation, and integrational support facilitates social participation. Balancing these supports helps optimize adherence while promoting autonomy and long-term well-being. FLEs should support individuals in achieving personally meaningful goals, fostering autonomy and recovery. Tailored communication and adaptive support help individuals progress toward objectives that matter most to them, rather than merely following prescribed treatment protocols. In the realm of cognitive tasks, FLEs should provide engaging low-pressure support- offering hints, being present, and facilitating open communication without applying motivational pressure. Creating a calm, supportive environment helps maintain a healthy flow of information. In areas requiring practical guidance, FLEs should be careful not to “breathe down the individual’s neck.” Over-observing or micromanaging can be counterproductive. Reflecting too much on individuals’ progress can also hinder improvement, but when done purposefully and in moderation, it can foster well-being. When it comes to situations regarding social integration, structured, task-oriented activities are needed. FLEs should be trained to use a “nudging” approach without overwhelming individuals. This includes offering clear instructions, necessary interventions, or even medication when needed, but without constant reflection, requests, or reminders. The goal is to avoid overwhelming individuals while maintaining focus on improvement without distractions.
Implications for Service Practice
Although derived from the mental health domain, the underlying principles of listening and adaptive support extend to other vulnerable populations, including the elderly, individuals with chronic conditions, and those facing socioeconomic challenges, for example, refugees and homeless. These groups often encounter similar difficulties, such as communication barriers (Mende et al. 2024) and can benefit from tailored, autonomy-respecting care strategies.
Beyond healthcare, sectors serving vulnerable consumers—such as those experiencing financial hardship or language barriers—can apply the principles of tailoring interactions to individual goals to prioritize empathy, clear communication, and problem-solving support, ultimately improving customer satisfaction and trust (Wirtz and Lovelock 2021). Managers should support their FLEs in determining the appropriate mix of instrumental, informational, emotional, and integrational support, tailored to individual needs, to keep frontline interactions adaptive and autonomy supportive. Supervision and reporting systems can help monitor outcomes, identify training needs, and ensure consistent application.
Limitations and Future Research
While our study provides valuable insights into FLE behaviors and their influence on adherence, several limitations should be acknowledged, opening avenues for future inquiry.
First, our data are derived from system entries reflecting ex-post assessments of interactions. Although this method provides structured documentation, it lacks the immediacy and contextual richness of real-time data. Future research would benefit from incorporating even more granular or immersive methods, such as ethnographic fieldwork. These approaches could reveal more nuanced understandings of FLE behavior and allow researchers to examine how interactions unfold in the moment and affect adherence directly.
Second, our 12-month observation window 8 enables the analysis of mid-term behavioral changes (World Health Organization 2003) but future research should consider extended study periods, particularly since behavioral changes may unfold gradually and be shaped by diverse long-term factors (Kazdin 2007).
Third, our study primarily takes the lens of improvements in adherence. Future studies could examine whether certain interaction styles, such as overly directive or emotionally detached behaviors, may have unintended negative consequences on adherence or resistance. Relatedly, scholars should explore the emotional labor of FLEs, including how sustained emotional demands affect both patient outcomes and employee well-being, and what factors foster stable, long-term relationships with vulnerable individuals.
Fourth, while our study examines different FLE interaction styles across mainly three broad groups of diagnoses, future research could take an even more granular approach, exploring micro-level differences within interaction styles with various patients through qualitative methodologies. Understanding subtle variations in FLE behavior could support the development of more effective, individualized treatment approaches (Insel 2010).
Fifth, although our study is confined to mental healthcare, the integration of vulnerable consumers into social life extends beyond this domain. Future research could investigate similar dynamics in other service contexts, such as retail or social care, to better understand how consumer–provider relationships shape long-term well-being and social integration.
Lastly, as our data stem from one healthcare provider in a single country, limiting generalizability, future research should extend these findings across different cultural and healthcare system contexts. Cross-country comparisons could identify how systemic and cultural factors shape the effectiveness of frontline interaction strategies.
In conclusion, as one of the first studies to integrate mental illness diagnoses into the service literature within the framework of TCR and TSR, we hope to inspire future research focused on the lived experiences of vulnerable consumer populations and the critical role of frontline service employees. Table 8 presents a structured roadmap for future research, outlining key themes, questions, and suggested methodological approaches for advancing this field.
Future Research Themes, Questions, and Methodologies.
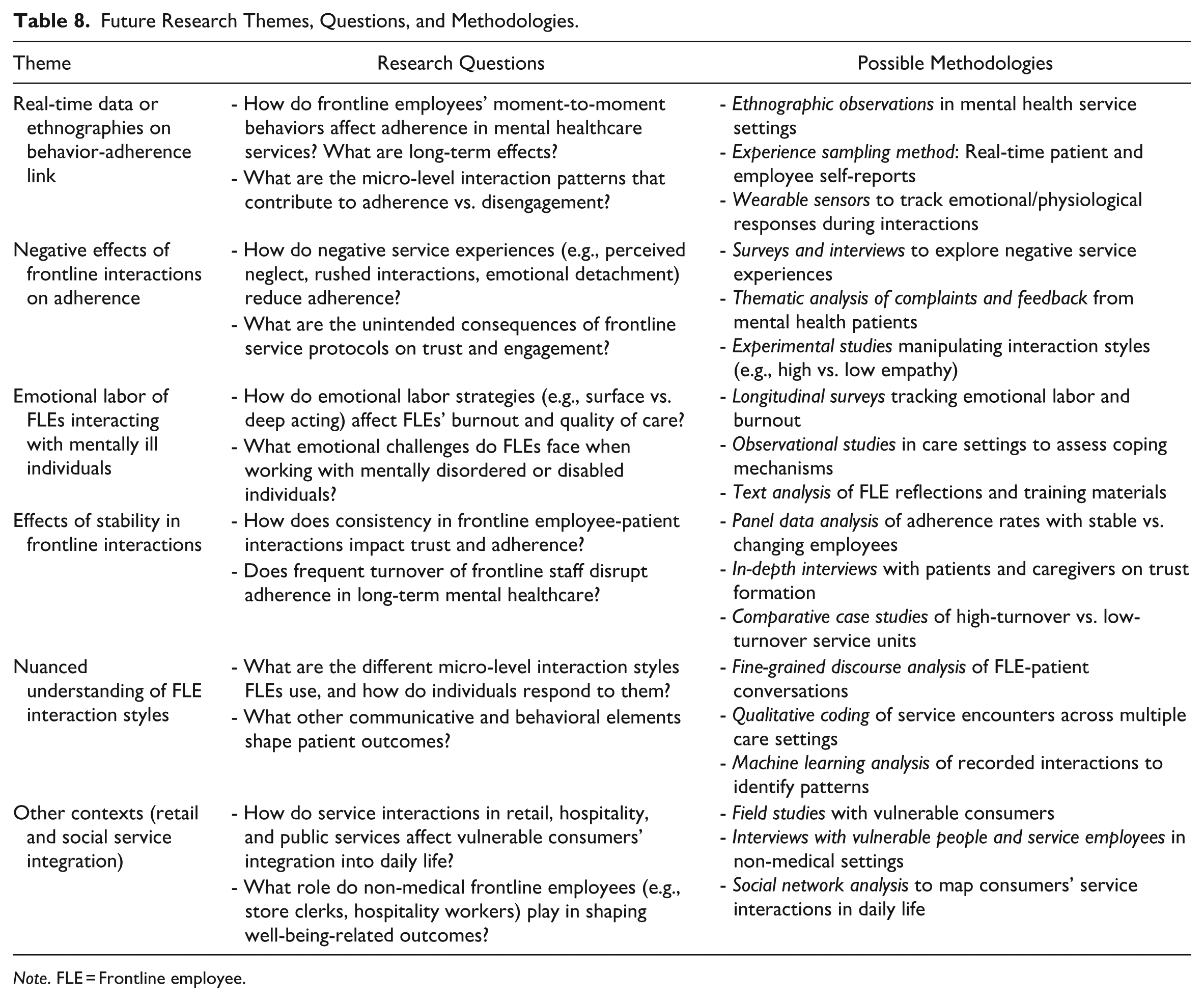
Note. FLE = Frontline employee.
Supplemental Material
sj-pdf-1-jsr-10.1177_10946705251410017 – Supplemental material for Adherence in Mental Healthcare: The Role of Frontline Employee Behaviors
Supplemental material, sj-pdf-1-jsr-10.1177_10946705251410017 for Adherence in Mental Healthcare: The Role of Frontline Employee Behaviors by Victoria Kramer, Janina Wiebringhaus, Detelina Marinova and Manfred Krafft in Journal of Service Research
Footnotes
Acknowledgements
We thank the collaborating health care provider for the provision of access to the data used for this study. We acknowledge feedback from participants of the EMAC Doctoral Colloquium 2023 as well as the AMA Marketing Strategy Consortium 2024. Finally, we are grateful for the constructive guidance and feedback by our review team.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.