
Abstract
Lanthionine synthetase cyclase-like receptor 2 (LANCL2) is a novel therapeutic target for Crohn’s disease (CD). BT-11 is a small molecule that binds LANCL2, is orally active, and has demonstrated therapeutic efficacy in 3 validated mouse models of colitis at doses as low as 8 mg/kg/d. Exploratory experiments evaluated BT-11 in male Harlan Sprague Dawley rats with a single oral dose of 500 mg/kg and 80 mg/kg/d for 14 days (n = 10 rats dosed/group). Treated and control rats were observed for behavioral detriments, and blood and tissues were collected for clinical pathology and histopathological examination. A functional observational battery demonstrated no differences between treated and control groups over multiple times of observation for quantal, categorical, and continuous end points, including posture, in cage activity, approach, response to touch, weight, grip strength, body temperature, and time on a rotarod. Histopathological examination of the brain, kidney, liver, adrenal gland, testes, stomach, small and large intestines, duodenum, pancreas, heart, lungs, spleen, thymus, and rib found no significant differences between the groups. Plasma enzymes associated with liver function were transiently elevated 2 to 4 days after the 500 mg/kg single dose but returned to normal values by 8 days and were not observed at any time in rats given 80 mg/kg/d for 14 days. One hour after oral administration of a single dose of 80 mg/kg, BT-11 had a maximal concentration of 21 ng/mL; the half-life was 3 hours. These experimental results demonstrated that BT-11 is well tolerated in rats, and, with further testing, may hold promise as an orally active therapeutic for CD.
Keywords
Introduction
According to the Crohn’s and Colitis Foundation of America, inflammatory bowel disease (IBD) afflicts over 1.4 million people in North America and 4 million worldwide. This widespread and debilitating illness results in decreased quality of life and significant health care-related costs. 1 In addition, intestinal inflammation caused by the 2 clinical manifestations of IBD, ulcerative colitis and Crohn disease (CD), increases the risk for developing colon cancer, especially at early ages (<30 years). 2
Even though current treatments for IBD have improved, 3 -5 they are only modestly successful for chronically managing the disease and result in significant adverse side effects, including a diminished ability of the immune system to mount protective responses against pathogens and malignancies. The current treatment paradigm for IBD includes aminosalicylates, corticosteroids, immunomodulators, antibiotics, and biologics (eg, anti-tumor necrosis factor α [TNF-α] monoclonal antibody). 5 Thus, there is an unmet clinical need for developing safer and more effective therapeutics for IBD.
One such approach is described here. Lanthionine synthetase cyclase-like receptor 2 (LANCL2) has emerged as a promising therapeutic target for chronic inflammatory, metabolic, and immune-mediated diseases such as IBD. 6 It is expressed in the hematopoietic system, specifically in neutrophils, monocytes, and splenocytes, as well as locally in gut CD4+ T cells and colonic epithelial cells. Abscisic acid (ABA) binds to LANCL2, leading to elevation in intracellular cyclic adenosine monophosphate, activation of phosphokinase A, and suppression of inflammation. 7 We identified PubChem compound CID247228, 8 N 1,N 4-bis(3-(1H-benzo[d]imidazo-2-yl)phenyl)terephthalamide, the parent compound of BT-11, piperazine-1,4-diylbis((6-(1H-benzo[d]imidazo-2-y)pyridin-2-yl)methanone), as a ligand of LANCL2 and a potent oral anti-inflammatory therapeutic in mice with colitis. 9 Biotherapeutics Inc (Blacksburg, VA) developed libraries of new chemical entities based on derivatives and analogs of ABA and CID247228. 10 Screening for LANCL2 binding and lead optimization based on efficacy, selectivity, local activity in the gut, and safety resulted in the selection of BT-11 as a top lead compound for CD treatment.
Oral treatment of mice with BT-11 demonstrated a 90% reduction in gut inflammation combined with a 4× reduction in colonic lesions with doses efficacious at 80 mg/kg and at doses as low as 8 mg/kg. These histological improvements observed in 3 mouse models of colitis correlated with decreased numbers of inflammatory F4/80+ CD11b+ macrophages and effector T helper 1 (Th1) cells in the gut mucosa. BT-11 also increased the levels of anti-inflammatory (FOXP3)-expressing CD4+ T regulatory cells in the colonic lamina propria, spleen, and mesenteric lymph nodes (MLNs) and decreased the levels of Th1 cells and Th17 cells in the spleen and MLN, respectively. 9 Furthermore, oral administration of BT-11 upregulated the colonic expression of interleukin 10 and LANCL2 and downregulated the expression of TNF-α in a dose-dependent manner. The present study investigated the exploratory profile of BT-11 in rats in preparation for investigational new drug (IND)-enabling Good Laboratory Practice studies in rats and dogs.
To further support the development of BT-11 as an orally active, locally acting small-molecule drug for CD, initial exploratory pharmacokinetic (PK) and exploratory safety studies were conducted in male Sprague Dawley rats, as this species provides the most common rodent model for in vivo preclinical studies used to support an IND application that are recommended by the International Conference for Harmonization. 11,12 The single-dose study used a high dose to approach the maximal tolerated dose and to facilitate the design of repeated dose studies. Initial PK studies were also done after single-dose administration, with blood concentrations measured 0.5 to 48 hours following oral administration. Results contributed to choice of dose for a 14-day exploratory repeated-dose study, which should provide indication of capability for the test agent to be tolerated for longer periods of time. For these single- and repeated-dose studies, behavioral and physiological effects were evaluated along with pathological effects. The results of the experiments described suggest that BT-11 is well tolerated in rats and that further more comprehensive studies would be warranted to position this test agent as a potential therapeutic agent.
Materials and Methods
Preparation and Purification of the Test Compound (BT-11)
The test compound, piperazine-1,4-diylbis((6-(1H-benzo[d]imidazo-2-y)pyridin-2-yl)methanone), is a bis(benzimidazolylaryl) heterocycle with structural similarity to N 1, N 4-bis(3-(1H-benzo[d]imidazo-2-yl)phenyl)terephthalamide, which is the chemical identified by PubChem as CID247228 and which has other identifiers, including NSC61610. 8 -10
Purification of BT-11 (1.46 g) was done from powder dissolved in hot dimethyl sulfoxide (DMSO; 90°C, 30 mL). After cooling overnight, the precipitate was centrifuged at 3,200g for 1 hour. The supernatant was removed and the solid was again redissolved in hot DMSO (20 mL). The precipitate was centrifuged at 3,200g for 1 hour. The supernatant was discarded and the pellet was resuspended in acetonitrile (CH3CN), vortexed, and centrifuged. The supernatant was discarded and the white solid was dried under high vacuum (recovery 870 mg or 60%). Purity was >98% as determined by nuclear magnetic resonance.
For these studies, the test compound was administered by oral gavage as a suspension in a pharmaceutical grade vehicle (Ora Plus; Perrigo, Dublin, Ireland). A suspension of 100 mg/mL was used to provide the dose of 500 mg/kg and a suspension of 20 mg/mL was used for dosing 80 mg/kg. Control animals were given equivalent volumes of the suspending vehicle. The suspension concentrations were chosen to provide volumes acceptable to Virginia Tech’s Institutional Animal Care and Use Committee (IACUC protocols 14-065 and 14-178) for oral administration of the mg/kg dosages to the rats.
Single- and Repeated-Dose Studies: Dosing and Sample Collection
All studies used adult Sprague Dawley male rats 200 to 250 g (>46 days old; Harlan Laboratories, Dublin, Virginia). Rats were group housed (2 per cage) on diamond dry cellulose bedding (Harlan Laboratories) and provided with a standard pelleted rat chow and water ad libitum until 12 hours before dosing. During the 5- to 7-day quarantine period, rats were adapted to a reverse light cycle (lights on at 9:00
Physiological end points (body weight) and behavioral end points (a Functional Observation Battery [FOB] that evaluates general appearance, mobility, and nervous system functioning) were done before and at multiple points after dosing (noted in Functional Observational Battery section). The number of rats in each group was sufficient to provide statistically significant behavioral data (n = 10, except n = 8 for day 21).
Additional treated animals were terminated (n = 3/treatment/time point, n = 4 for controls) to perform clinical pathology studies and histopathological observations. For the single-dose study (500 mg/kg), these were at 2, 4, 8, and 14 days postdosing. For the repeated-dose study, these were at 4, 8, 14 (day of the last dose), and 21 days.
Pharmacokinetic Study: Dosing and Sample Collection
For the PK study, 12 adult male Sprague Dawley rats (Harlan Laboratories) arrived with indwelling jugular catheters. They were individually caged on diamond dry cellulose bedding (Harlan Laboratories) and given a standard pelleted rat chow and water ad libitum. Rats were allowed to acclimate for 5 days prior to dosing, during which they were monitored for postoperative health issues and had their catheters checked for patency. Following 12-hour fasting, all rats were administered 80 mg/kg of the test agent by oral gavage. Blood samples were taken from a minimum of 3 rats at 0.5, 1, 2, 4, 8, 12, 16, 20, 25, and 48 hours after dosing. Catheterized rats were bled (0.5 mL) more than once but no more than twice within a 24-hour period based on IACUC recommendations. Test agent concentrations in plasma were determined by liquid chromatography–mass spectrometry (LC–MS/MS).
Plasma Sample Preparation and LC–MS/MS Analysis for PK Studies
Blood samples were collected with heparinized syringes via the exteriorized ends of the jugular vein catheters. The samples were transferred to BD Microtainer blood collection tubes (Becton Dickinson, Franklin Lakes, New Jersey) with EDTA and centrifuged to separate the plasma. The plasma supernatant was removed and stored in Eppendorf tubes at −20°C.
Purified test compound BT-11 and reserpine (MP Biomedicals LLC, Santa Anna, California) were used as standard and internal standard, respectively. BT-11 was accurately weighed and transferred into a 5-mL volumetric flask. The analyte was completely dissolved in 5 mL of 10% formic acid (FA) in acetonitrile (CH3CN; standard solution 1 [SS1]). Then, 10 μL of SS1 was diluted 1,000 times in CH3CN. This solution was used to prepare all standard solutions. For internal standard preparation, 2.0 mg of reserpine was dissolved in 10% FA in CH3CN (2 mL) and mixed thoroughly internal standard solution #1 (ISS1). Then, 10 μL of ISS1 was diluted to 10 mL with CH3CN (internal standard solution #2 [ISS2]). This solution was used to spike all samples. The BT-11 calibration curve was obtained from 7 standard solutions containing plasma (100 μL) ranging from 0.5 to 15 ng/mL. The lowest level of quantitation was 0.2 ng/mL (200 ppt).
Before injecting for analysis, plasma (100 μL) was mixed with ISS2 (10 μL) and CH3CN (200 μL). The solution was centrifuged at 12 000 rpm for 10 minutes. The supernatant was transferred to a clean tube. CH3CN (100 μL) was added to the pellet. After vortexing and centrifugation, both supernatants were combined. After evaporation of CH3CN, 50%/50% (H2O/CH3CN) (1 mL) was added. The solution was vortexed and centrifuged for 2 minutes. The solution was transferred into a high-performance liquid chromatography (HPLC) glass vial for analysis.
Blood plasma samples were run in duplicate using an HPLC column from Phenomenex (Luna C18 150 × 2.1 mm, 3 μm; Torrance, California). The flow rate was set at 0.2 mL/min and the injection volume at 50 μL (into a 20-μL loop). The mobile phase consisted of a mixture of A (H2O with 1% FA) and B (CH3CN with 1% FA), with gradients alternating 3 times between 95% A:5% B and 5% A:95% B over 15 minutes. For MS/MS analysis, the LC column effluent was pumped directly into the Thermo Instrument TSQ triple quadrupole mass spectrometer (Thermo Finnigan, San Jose, California) equipped with an electrospray ionization source. The instrument was calibrated with a solution of polytyrosine according to the manufacturer’s recommendation. Optimal parameters were obtained with the BT-11 standard (10 ng/μL) flowing at a rate of 10 μL/min into 50%/50% (A/B) of mobile phase at a rate of 0.2 mL/min to achieve reasonable MS sensitivity in multiple reaction monitoring. The MS parameters for detection were spray voltage 4,500 V, sheath gas pressure 45 psi, auxiliary gas pressure 55 psi, capillary temperature 300°C, parent ion 265.0 ([MH2]2+) for test compound BT-11 and 609.0 for internal standard reserpine ([MH]+), monitored product ion 193.9 for test compound BT-11 and 195.0 for internal standard reserpine, and positive polarity. In order to keep the MS clean, the divert valve was used to transfer the column effluent to the MS from 8.0 to 9.3 minutes. From 0 to 8.0 minutes and 9.3 to 15 minutes, all the column effluent was transferred to waste.
Determination of PK Properties
The PK calculations used a simple average obtained from results of duplicate analyses for blood from each of 3 rats at each time point for n = 3. Data generated were based on medians and geometric means, with both suggesting that the data followed an approximate 1-compartment model. The median-based curve was smoother and was subsequently used in downstream analyses as appropriate. Median plasma concentrations were entered into PKSolver (an add-in program for PK and pharmacodynamics data analysis in Microsoft Excel) for the determination of elimination rate constant (kel), apparent volume of distribution (Vd), clearance (Cl), and half-life (T1/2). 13 The maximal concentration (Cmax) and the time to Cmax (Tmax) were estimated from observing the graph of median plasma concentrations versus time. The absorption rate constant (ka) was generated by fitting a 1-compartment mathematical model to the data using JMP Pro version 11.2.0 (Cary, North Carolina). Although area under the curve was calculated, it could not be used to determine bioavailability (F) because the test compound was too insoluble to administer by the intravenous (IV) route and no comparison could be made.
Functional Observational Battery
The FOB was performed using the standard operating procedures of the Laboratory for Neurotoxicity Studies at Virginia Maryland College of Veterinary Medicine, which follows the template of Moser. 14 A baseline assessment was made prior to dosing (study day -3 or -4), and then assessments were performed at 4 hours and 1, 7, and 14 days after dosing for the single-dose study and at 3, 7, 14, and 21 days during the repeated-dose study.
For each assessment, rats were first observed in their home cage for posture, clonic, and tonic involuntary movements, vocalizations, respirations, and activity level. Following that, rats were observed during handling for cage removal ease, lacrimation, salivation, piloerection, palpebral closure, palpebral reflex, pupil size and general handling reactivity, as well as pupil light, oculocardiac, and visual placing responses. Next, rats were placed in an open field for 3 minutes and observed for clonic and tonic involuntary movements, gait, mobility, arousal, stereotypy, and bizarre behavior along with counts of rearing, fecal boluses, and urine pools. Animals were then tested for the following reflexes: approach, touch, click and tail pinch responses, and righting and tail–limb reflexes. The FOB was concluded by taking the following physiological measurements: body weight, body temperature, time on an accelerating rotarod, forelimb and hind limb grip strength, and landing foot splay distance following a 30-cm drop.
Pathological Procedures
Rats were euthanized at sacrifice by intraperitoneal injection of 200 mg/kg of sodium pentobarbital. Blood was collected from the inferior vena cava for complete blood count and clinical chemistry (n = 3-4/group). Blood samples were analyzed using standard end points for hematology and blood chemistry, as conducted for patient samples submitted to the Clinical Pathology Laboratory of the Veterinary Medicine Teaching Hospital. These analyses include red blood cell concentrations, hemoglobin, hematocrit, mean corpuscular volumes, mean corpuscular hemoglobin concentration, cell hemoglobin concentration, platelet number, mean platelet volume, reticulocytes, white blood cell count and differential, glucose, blood urea nitrogen, creatinine, phosphorus, calcium, sodium, potassium, chloride, carbon dioxide, anion gap, cholesterol, total protein, albumin, globulins, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin (BILI).
The following tissues were collected and immersion fixed in 10% neutral-buffered formalin for histopathological examination: brain, kidney, liver, adrenal gland, testes, stomach, small and large intestines, duodenum/pancreas, heart, lungs, spleen, thymus, and rib (including hematopoietic tissue of marrow). Rib samples were decalcified overnight using decalcifying solution with FA and formalin (EDF; Medline, Mundelein, Illinois) prior to all tissues being trimmed and submitted to the Histopathology Laboratory of the Veterinary Medical Teaching Hospital. The samples were dehydrated, cleared, and embedded in paraffin. The samples (n = 3) were then sectioned at 5 μm thickness, stained with hematoxylin and eosin, and examined by light microscopy by a board-certified veterinary pathologist in a nonblinded fashion.
Statistics
The rat FOB included measurement of quantal, categorical, and continuous end points. Quantal end points (identified as either present/normal or absent/abnormal) were piloerection, palpebral reflex, pupil light response, oculocardiac reflex, visual placing, tail–limb reflex, vocalization, and normality of respiration. Categorical (scored) end points of the FOB included posture, in cage activity, handling reactivity, in cage arousal score, response to approach, and response to touch. Quantal and categorical end points were summarized as contingency tables and compared between treatment groups at each time point (1 outcome at a time) using Fisher exact test (single-dose experiment) or the Mantel-Haenszel χ2 test (repeated-dose experiment). The Mantel-Haenszel test was selected for the repeated-dose experiment because the rats were processed in 2 blocks. Continuous end points were weight, body temperature, number of rears during observation period, seconds on a rotating rod, foreleg grip strength, hind leg grip strength, and landing foot splay. Normal probability plots showed that all continuous end points followed a normal distribution. Subsequently, continuous end points were summarized as means ± standard deviation. At baseline, treatment groups were compared (separately for each outcome) using 2-sample t tests (single-dose experiment) or mixed-model analysis of variance (repeated-dose experiment). During follow-up (for both single-dose and repeated-dose experiments), the treatment groups were compared using mixed-model analysis of covariance, with baseline measurements as covariates. The linear models specified baseline measurements, treatment group, time, and the interaction between treatment group and time as fixed effects, with Kenward-Roger as the denominator degrees of freedom. Random effects were rat identification within treatment group (both single-dose and repeated-dose experiments) and block (repeated dose experiment). To specifically compare treatment groups at each follow-up time point, the slicediff option of proc GLIMMIX was applied to the interaction between treatment group and time. Clinical pathology also provides continuous end points; these were evaluated using 1-way analysis of variance. Statistical significance was set to P < 0.05. Analyses for quantal, categorical, and continuous end points were performed using SAS version 9.4 (Cary, North Carolina), whereas clinical pathology continuous end points were analyzed using JMP Pro version 11.2.0.
Results
Single-Dose Study, 0 or 500 mg/kg, FOB
No obvious behavioral evidence of detrimental effects was seen over the 2 weeks these animals were observed. Referring specifically to the FOB end points that were quantal (yes/no), categorical (scored), or continuous, the following statements can be made. First, there were no differences in quantal end points between treated and control groups for piloerection, palpebral reflex, pupil light response, oculocardiac reflex, visual placing, tail–limb reflex, vocalization, or normality of respiration. These were identified as either present/normal or absent/abnormal (data not shown because all animals had the same response). Second, for categorical end points, compared at each time point using Mantel-Haenszel test, the control and treatment groups did not differ at time points beyond baseline. However, a significant difference was observed between the 2 groups for touch response at baseline (P < 0.0406). It is the only significant finding for all comparisons within all FOB end points. Finally, for continuous end points, no statistical differences between control and treated groups were noted at any time, with the exception of weight and hind grip strength (Figure 1). For weight on day 14, as illustrated in Figure 1, the least squares (LS) mean for the 500 mg/kg BT-11 group was lower than the LS mean for the vehicle control group (LS means 254.71 vs 264.46; P = 0.0006). The groups did not differ for weight at any other time points. For hind grip strength, the LS mean for the 500 mg/kg group was lower than the LS mean for the control group on day 1 (LS means 0.40 vs 0.46; P = 0.0272). It is noteworthy that the differences for hind grip are really small, despite reaching statistical significance. The groups did not differ at other time points.
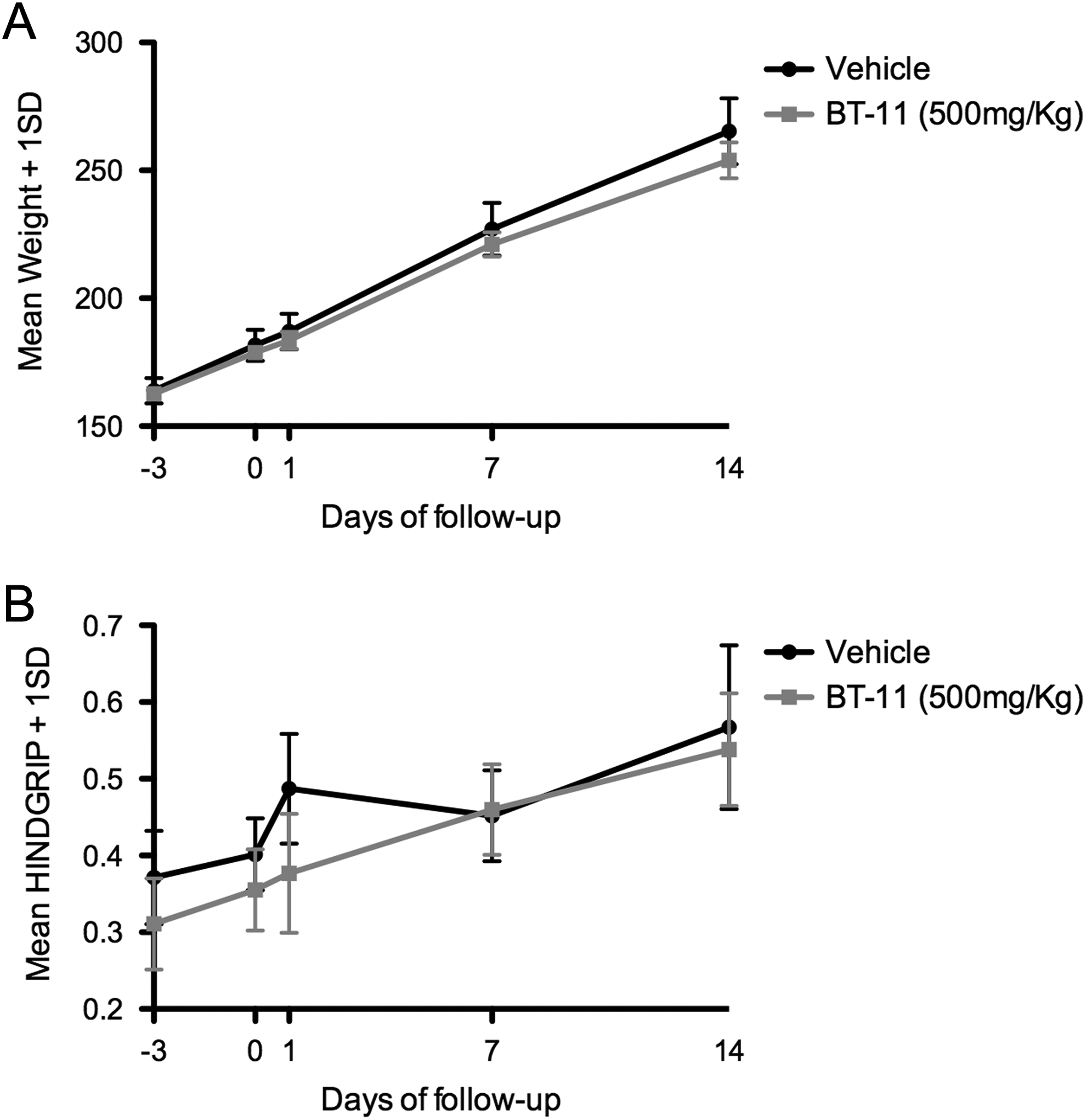
Time related measurements of weight (Fig 1A) and hind grip strength (Fig 1B) 2 to 14 days after a single oral dose of 500 mg/kg BT-11. Results expressed as mean ± standard deviation (n = 10). Statistical differences between groups were seen with weight at 14 days and with hind grip strength on day 1.
Single-Dose Study, 0 or 500 mg/kg, Pathological Assessment
Histopathological comparison was made between vehicle control and BT-11–exposed animals. No significant differences were noted between the 2 groups at any of the postdosing intervals (2, 4, 8, or 14 days). Some findings were noted in all animals, such as mild deep mucosal–submucosal eosinophilic infiltrates in the stomach, the presence of small numbers of mast cells in perivascular regions in the myocardium, and hepatic portal infiltrates of lymphocytes along with occasional eosinophils and neutrophils. These are considered as normal features of these animals and not related to test article exposure.
Blood samples that underwent analyses in the Clinical Pathology Laboratory showed clinically significant increases in markers of hepatocellular injury (ALT, AST) and cholestasis (alkaline phosphatase [ALP], total bilirubin [tBILI]) on postdosing day 2 (ALT, AST, ALP, and tBILI) and postdosing day 4 (AST and tBILI). However, these changes were not statistically significant (Table 1). The changes in blood values did not persist, as samples taken on days 8 and 15 were not clinically or statistically different from control values. The reversibility of these effects associated with the very high dose given reduces the significance of these findings. Other end points evaluated were not clinically significant, as blood samples from controls and treated rats demonstrated similar results.
Select Mean Plasma Chemistry Results From Control Rats and Test Rats 2, 4, 8, and 14 Days After Oral Administration of BT-11 at a Single Dose of 500 mg/kg.a
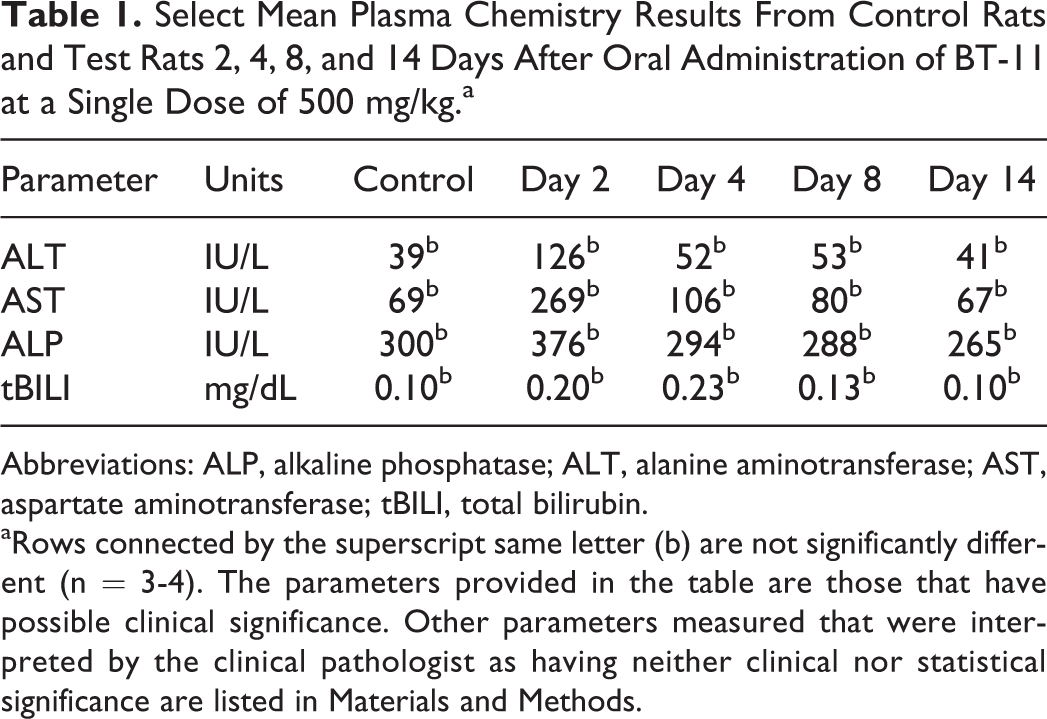
Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; tBILI, total bilirubin.
aRows connected by the superscript same letter (b) are not significantly different (n = 3-4). The parameters provided in the table are those that have possible clinical significance. Other parameters measured that were interpreted by the clinical pathologist as having neither clinical nor statistical significance are listed in Materials and Methods.
Pharmacokinetic Experiment, Single 80 mg/kg Oral Dose
The test compound could be detected at very low ng/mL (ppb) levels. The plasma samples obtained at 24 to 48 hours had very low but still measureable levels (1-2 ng/mL). For analytical procedures associated with PK studies, the biological samples (0.5-1 mL blood) were extracted and purified as described in Methods section. results of the chemical analysis of blood plasma are provided in Table 2.
Plasma Concentrations of BT-11 in Samples Taken After Administration of Test Compound.
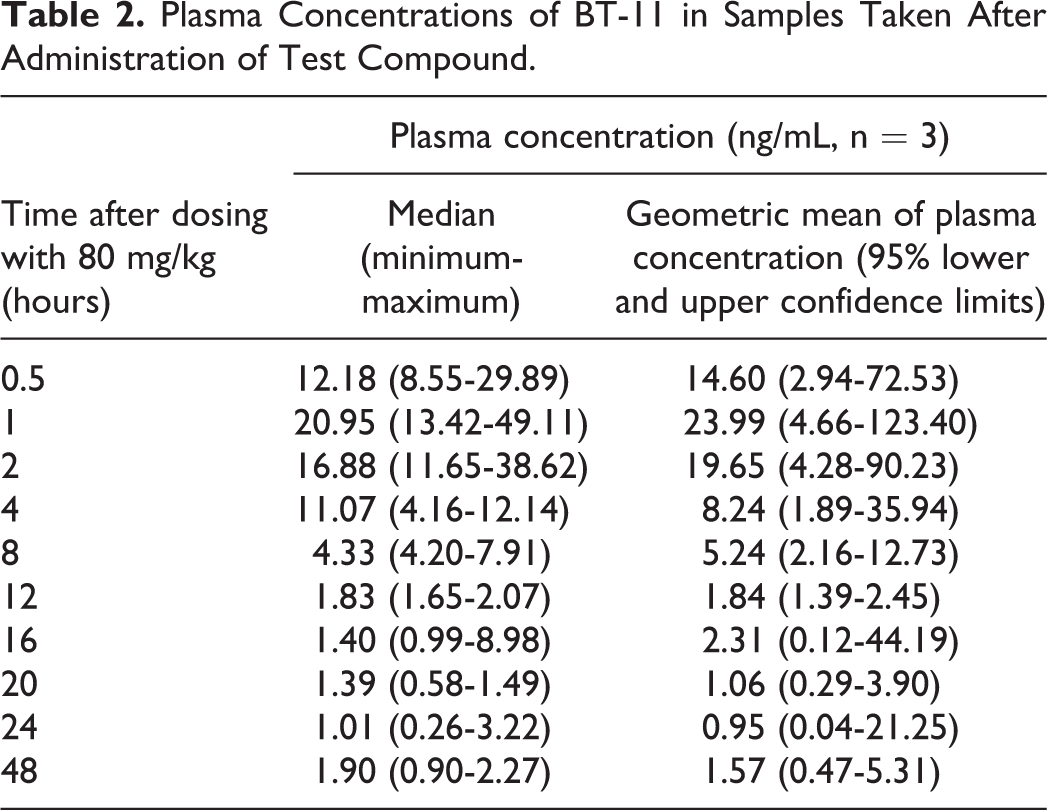
Because plasma concentrations of the test agent were no longer decreasing by 12 hours after administration, median values for 0.5 to 8 hours were used for calculation of PK parameters. Original plasma concentration (Cpo) was extrapolated by the computer from the straight line on a log scale of elimination that ran through the highest concentration (Cmax), so the following parameters could be provided as:





The graph depicted in Figure 2 provides visualization of the PK data. The y-axis on this graph gives the data in ng/mL (ppb). By inspecting this graph and data in Table 2, Cmax was estimated as 21 ng/mL at a time after dosing (Tmax) of 1 hour.
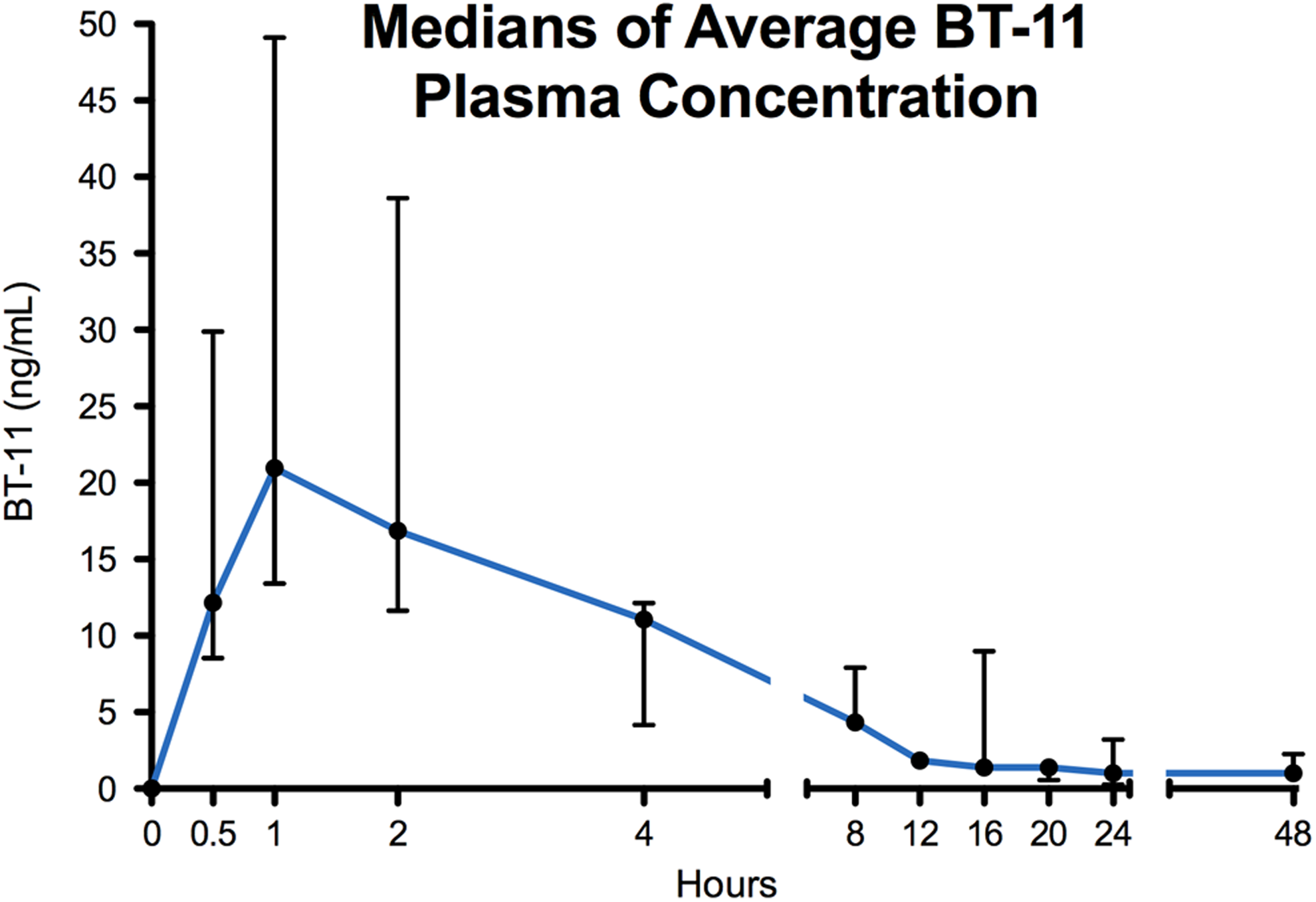
Plot of plasma concentrations of BT-11 at various times after a single oral dose of 80 mg/kg, arithmetic y-axis. This plot was used for the estimation of Cmax and Tmax. Values depicted are expressed as median with errors bars representing the minimum and maximum at each time point (n = 3).
From the data obtained and analyzed after rats were given a single 80 mg/kg oral dose, and assuming single-compartment, dose-independent PKs, time to steady state (97% level) after repeated dosing would expect to occur at 5× T1/2, or approximately 15 hours. Usually, the apparent Vd is determined from PK parameters calculated after IV injection of test compounds. This alleviates the confounding associated with drug absorption kinetics. As BT-11 is relatively insoluble at concentrations required to provide the test dose in an appropriate volume, IV administration was not feasible here, so an attempt was made to estimate an apparent Vd after oral administration.
Although not designated a PK study, some blood samples were collected from rats given the high dose (500 mg/kg) to evaluate a general time course of blood concentrations of BT-11. Concentrations were 32, 3.1, and 13 ng/mL in samples taken at 2 hours, 17, 15, and 6.7 ng/mL in samples taken at 4 hours, and 3.0, 9.6, and 3.3 ng/mL in samples taken at 22 hours.
Repeated-Dose Study, 0 or 80 mg/kg, FOB
No behavioral evidence of detrimental effects associated with oral BT-11 treatment was observed over the 2 weeks of treatment or the 1-week postdosing period. No quantal differences were noted between controls and BT-11–treated rats at any time data were collected. The groups did not differ for the vast majority of categorical comparisons, with the exception of significant differences for the following outcomes: posture at baseline and on day 21 (P = 0.0235, P = 0.0339, respectively), cage removal ease at baseline (P = 0.0285), and response to touch on day 7 (P = 0.0285). These differences were likely variations within degrees of normal behavior. For continuous end points, the groups were balanced at baseline, and at time points after dosing, the groups did not differ. The only exception was a significant difference for rears during the observation period on day 14 (Table 3); LS mean for dose 0 was greater than the LS mean for the 80 mg/kg/d dose of BT-11 (P = 0.0273). This was a single difference that only appeared once during the course of observations. Furthermore, end points that changed with a single dose of 500 mg/kg (Figure 1) were not altered in rats given 14-day treatment with 80 mg/kg/d (Figure 3).
BT-11: Example of a Continuous FOB End Point for Male Rats Given Repeated Doses of 80 mg/kg BT-11 for 14 Days.
Note: The number in bold indicates statistical significance, p < 0.05.
Comparison of weight and hind grip in control and BT-11–treated rats before and after the initiation of 14 daily oral doses of 80 mg/kg. Day 21 is 7 days after dosing ceased. Values are expressed as mean ± standard deviation (n = 8-10). In contrast to what was seen with the 500 mg/kg acute dose (Figure 1), there were no significant differences between control and treated rats.
Repeated-Dose Study, 0 or 80 mg/kg, Pathological Assessment
Clinical pathology and histopathology
No test article-associated lesions were noted in animals administered this agent, and none were seen in the vehicle control group. The conclusion is that no histopathologic evidence of toxic injury was observed in rats given 80 mg/kg/d of BT-11 over a period of 14 days. Clinical pathological examination of blood samples taken at various sacrifice days did not reveal any clinical or statistical differences when samples from control and test rats were compared.
Discussion
The results of behavioral and pathological experiments presented here indicate that BT-11 appears to be well tolerated when administered orally to adult male rats over 14 days at 80 mg/kg (cumulative dose 1,120 mg/kg) or as a single oral bolus of 500 mg/kg. Experiments were designed to include end point determinations 7 to 14 days after dosing to evaluate reversibility of any detriments. The only statistical difference noted 14 days after treatment ended was a weight difference of <4% when the high bolus dose was given, even though weight differences were not evident until that time nor did weight differences appear between control and treated rats given multiple 80 mg/kg doses of BT-11.
Although clinical pathology end points suggestive of transient liver effects were noted in early (2-4 days postdosing) blood samples collected after bolus oral administration of 500 mg/kg BT-11, no such effects were seen at later time points. Nor were any of these end point changes noted when blood samples were collected during or after the repeated-dose experiments. Oral administration results in drug in the blood going to the liver before it enters general circulation, where first-pass elimination is possible. In experiments with 500 mg/kg BT-11, the liver was exposed to a bolus, high concentration of the product. 15 This may have contributed to the transient response observed. Note that plasma concentrations of BT-11 at 2 hours after 500 mg/kg were between 3 and 39 ng/mL and concentrations 2 hours after 80 mg/kg were between 12 and 39 ng/mL. The dose of 500 mg/kg was considered very high, as it was over 60× a low-effective pharmacological dose for treating IBD in mice (8 mg BT-11/kg/d), 9 and yet it did not cause any long-lasting detriments.
The rat FOB is a thorough and quantitative way to measure behavioral effects of new drugs in intact laboratory animals. 14 It provides numerous time-related end points, allowing observers to document changes relevant to general and nervous system-specific toxicities. Following oral BT-11 administration, the general appearance and behavior of the rats were normal, and both controls and treated rats gained weight. Biologically significant effects of BT-11 on weight or weight gain, sensitive indicators of general toxicity, were not seen with any of the rats in any of the experiments conducted as part of this study.
For this study, we developed the analytical method for plasma detection of BT-11 and found it useful for the detection of plasma concentrations as long as 48 hours after a relatively high efficacious dose (80 mg/kg). We assume that this method can be adaptable for lower plasma concentrations associated with lower dosing paradigms, but studies using the minimal efficacious dose (8 mg/kg) remain to be done. Plasma samples collected after oral administration of 80 mg/kg BT-11 in the present study indicated that it could be orally active and systemically absorbed by this route. Current therapeutic agents used to treat IBDs, including glucocorticoids for CD, may be given orally, locally (by rectal administration), or by the IV route. 5 However, even locally applied drugs need some systemic absorption in order to exert anti-inflammatory effects. The PK profile of BT-11 in the present experiments suggests rapid absorption and rapid elimination with the possibility of limited systemic absorption as well as local delivery to the lower gastrointestinal tract, a therapeutic benefit similar to the commonly used IBD treatment, mesalamine. 5 Although the BT-11 used in these experiments was insufficiently soluble to be given IV, future studies are planned after development of a more aqueous soluble formulation so bioavailability can be determined by comparing blood levels after IV and oral dosing.
The analytical method used to analyze plasma concentrations for BT-11 was very sensitive and capable of determining low plasma levels after oral administration during PK experiments. The PK parameters calculated in this study were used to extrapolate useful information. For example, the high apparent Vd, which is greater than blood volume of the test animal, suggests either (1) that the test compound is being distributed outside the blood because a Vd > 1 L/kg suggests that the drug could be sequestered in tissue outside body water or (2) a considerable amount of the test agent is not being systemically absorbed but is instead being eliminated prior to absorption (eg, through the liver and/or feces) and acting locally in the gut. 15 The latter possibility is more likely for BT-11 due to the consistent 90% reduction in gut inflammation observed in animal pharmacology studies using 3 validated mouse models of IBD. 9 Although the product used for these studies was relatively insoluble, a more soluble form of BT-11 is under development so future experiments could provide additional PK data comparing a more soluble BT-11 (given IV, so Cpo does not have to be estimated) and oral BT-11. It is recognized that the use of different pharmaceutical preparations, vehicles, and/or different concentrations of test compound could have a significant role in the PKs of the test agent. 16 Of note, however, is that BT-11 is being proposed as a treatment for CD, where a local effect in the gastrointestinal tract is preferred over high systemic distribution after oral administration.
The overall conclusions from the results presented here are that oral administration of BT-11 to rats leads to relatively rapid but limited absorption from the gastrointestinal tract and relatively rapid removal from the plasma. Furthermore, oral BT-11 administration at the doses tested in the rat did not cause histopathological or behavioral effects.
Footnotes
Acknowledgments
The authors wish to acknowledge Mehdi Ashraf-Khorassani, Chemistry Department, Virginia Tech, for operating the LC–MS/MS.
Author Contributions
Marion Ehrich contributed to conception and design and contributed to acquisition, analysis, and interpretation. Philippe Bissel, Bernard S. Jortner, and Geraldine Magnin-Bissel contributed to conception and design and contributed to analysis and interpretation. Katie Boes contributed to design and contributed to acquisition, analysis, and interpretation. Jonathan Hinckley and Stephen R. Werre contributed to design and contributed to acquisition and interpretation. Adria Carbo and Raquel Hontecillas contributed to conception and design and contributed to acquisition and interpretation. Casandra Philipson and Noah Philipson contributed to conception and contributed to acquisition. Richard D. Gandour contributed to conception and design and contributed to acquisition and analysis. Josep Bassaganya-Riera contributed to conception and design and contributed to acquisition, analysis, and interpretation. All authors drafted the manuscript, critically revised the manuscript, gave final approval, and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Drs Carbo, Philipson, Hontecillas, Philipson, Gandour, and Bassaganya-Riera were employed by or consulted for Biotherapeutics Inc at the time this work was done.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Virginia Biosciences Health Research Corporation and NIH SBIR/STTR funds (1R43DK097940 and 1R41DK099027).