
Abstract
The eye is a unique sensory structure, which must be evaluated for toxicity to determine the safety of drugs, industrial chemicals, and consumer products. Changes in the structure and/or function of ocular tissues following systemic administration of a potential new drug in preclinical animal models can result in significant delays in the development of a new therapeutic and in some cases lead to termination of the development. The ability to detect and characterize ocular toxicity in preclinical models and to predict risk in patients is critically dependent on the preclinical testing strategy, the availability and use of state-of-the-art ocular safety assessment tools, and the knowledge of drug mechanism of action and the current regulatory environment. This review describes the design and execution of toxicity studies with the incorporation of current methods for in vivo assessment of ocular toxicity, including methods for detecting early changes in the eye. In addition, anatomical differences among laboratory animals, preparation of globes for examination, and iatrogenic and spontaneous ocular findings are described that can affect interpretation of toxicological findings. Finally, the correlation between nonclinical outcomes and clinical evaluations is discussed in terms of expected therapeutic uses, indications, and regulatory consequences of ocular effects.
Introduction
Eyes are finely tuned, specialized transducers of the visual world and are critically important to overall health, function, and well-being. Disease, injury, environmental stressors as well as drugs can disrupt the delicate anatomy and physiology of the eye and cause adverse effects on vision.1,2
The drug development process generally follows a logical progression, although different pharmaceutical companies can take somewhat different approaches for entry into early clinical trials. Unwanted ocular side effects of the drugs are typically not the most common safety issue in drug development programs, but findings of ocular toxicity in nonclinical studies can be a major barrier to further clinical development. Depending on the nature of the findings, these side effects may stop the development of a potentially important new drug, impact the label and use of a drug, reduce the return on investment for the drug sponsor, or in a worse-case scenario, may adversely impact the health and well-being of the patient. Therefore, drug companies rely on various methods and strategies to identify, assess, and if necessary, remove potential new drugs with ocular safety risks from their pipelines. 3 The earlier in the drug development process these risks are detected and evaluated the better in order to lower costs and conserve resources by removing higher risk compounds from development, that is, if a drug is to fail, it is hoped that it would fail early.
It is not always easy to identify drugs with ocular safety risks, especially early in the development process. Questions that often arise during development include whether the ocular finding is truly different from background, the relevance to humans or the animal model, the reversibility of the ocular finding, and maybe more importantly, the ability to monitor the findings in the clinic. In addition to these fundamental and basic issues, questions arise regarding the dose (exposure) at which the effect occurs and whether a reasonable safety margin is expected in clinical trial patients. At the end of the safety assessment, the more critical question would be whether the potential benefit of the therapy outweighs the potential risk.
The toxicologist has to be aware of methods, tools, and models that may be employed to detect and assess the changes in the visual system. Selection of an appropriate and relevant animal model is critical. In general toxicity studies, the dog and albino rat are the more common test species. However, should the albino rat be used considering that the eye of the human is pigmented? The albino rat is susceptible to light-induced retinal degeneration that may complicate the ability to detect drug-induced ocular toxicity. 4 Differences in ocular toxicity between the albino and the pigmented rat have been seen for some drugs 5 but not for others, based on a hypothesis related to melanin binding.6–8 On the other hand, the dog eye contains the tapetum, an anatomic structure that is not present in humans making tapetal findings in dogs unlikely to be relevant to humans. 9
This review is based on a symposium entitled Ocular Toxicity from Systemically Administered Xenobiotics: Considerations in Drug Development presented at the annual meeting of the American College of Toxicology (Phoenix, AZ, 2011). The symposium was developed to discuss the design, execution, and interpretation of toxicity studies that incorporate current methods for in vivo assessment of ocular toxicity, and how those methods can be used to detect early changes in the eye that inform risk assessment decisions. In addition, detecting microscopic findings due to ocular toxicity are described, and these histopathological changes can be affected by, for example, anatomical differences among laboratory species, preparation of globes for examination, and iatrogenic and spontaneous ocular findings, and so forth. Finally, the correlation between nonclinical outcomes and clinical evaluations is discussed in terms of expected therapeutic uses, indications, and regulatory consequences of ocular effects.
Noninvasive Measures of Structure and Function in Ocular Toxicology and Drug Discovery
“First, do no harm” is a guiding principle for bringing any new therapy to the patient. This principle applies also to the tools and assays used to evaluate the efficacy or toxicity of compounds in patients and when possible, should guide the use of laboratory animals. The globe of the eye is a unique organ in which many of its structures are assessable by noninvasive means. The main function of the eye is to regulate and focus light from the environment onto the retina where it is absorbed and converted into action potentials for processing by the brain. There are very few functional parts to consider in this chain of events and includes extraocular muscles that facilitate the movement of the globe within the eye socket, constriction of the pupil that regulates the amount of light entering the eye, processing of light by the neural retina, and detection of the retinal signal by various areas of the brain dedicated to vision.
Invasive or terminal assays such as histology and tissue dissection that are widely used in the laboratory setting are not typically applicable when examining the patient. The eye presents a unique situation where the target tissues are readily accessible and are open to noninvasive means for the determination of viability, potential toxicity of xenobiotics, and efficacy of treatment. In addition, the eye is unique because the retina is part of the central nervous system, and its function can be compromised by a myriad of conditions from physical damage of surrounding tissue, degeneration of the retinal neurons, or distorted function without physical change. For example, compounds such as sildenafil 10 can transiently interfere with the process of absorbing light by the retina, resulting in a decrease in retinal function, without a detectable change in the cell structure.
Abnormal control of extraocular muscles in patients and some animals can be evaluated by moving a target within the field of view and observing the smooth or abnormal tracking movement of the eye. It is rare, however, that a disease or adverse drug interaction would be limited to affecting only these muscles. For example, nervous system depressants such as barbiturates or alcohol will alter normal eye movement and will also affect cognition and retinal function. 11 The involuntary reflex of pupil constriction in response to light can be observed during an undilated ocular examination, and the timing and the extent of the pupil reflex can be measured using a pupilometer. Abnormal pupil dilation can be a symptom of brain injury, retinal degeneration, compromised muscle or nerve conduction, or many other conditions. In the conscious animal, pupil reflex can be altered if the animal is under stress and not first acclimated to the examination; anesthetics can suppress the pupil reflex as well. 11
Through the use of direct observation, biomicroscopy, specialized imaging, electrophysiology, and visual acuity (VA) assessments, it is possible to evaluate both the structure and the function of ocular tissues without causing harm to patients or laboratory animals. In this section, several noninvasive methods are reviewed, which are used to examine the ocular tissues in the laboratory and directly translate to methods used in the clinic.
Imaging
The most important tool ophthalmologists have at their disposal is their own eyesight. Inspection of ocular tissues such as eyelids, cornea, iris, lens, lacrimal complex, and conjunctiva for signs of inflammation, irritation, or other abnormal appearance can be done with a simple pen light and a magnifying lens or loupe. Detailed visualization of the anterior structures such as cornea, lens, and iris can be conducted through a slit lamp biomicroscope to magnify and enhance particular features. Examination of posterior structures or the ocular fundus including the retina, optic nerve, macula (in primates), choroid, and retinal vasculature requires additional lenses or a fundus camera to compensate for the optics of the eye. In addition, technology such as optical coherence tomography (OCT) imaging can extend the examination further by providing a noninvasive cross-sectional image of the tissues similar to histology and greatly enhanced diagnostic capabilities (see below).
Slit Lamp Biomicroscope
The slit lamp consists of a high-intensity multicolored light source that can be cropped to form a thin beam of light and is mounted on a 180° articulating arm (Figure 1, left). This device can be coupled with a digital imaging system to provide documentation of regions of interest. Although the normal or affected cornea is typically transparent with direct illumination, indirect or off-angle illumination with a narrow beam of light takes advantage of internal scattering properties of the cornea and provides an easy visual inspection of the corneal layers for damage or swelling (Figure 1, right). Off-angle illumination can also provide examination of the anterior chamber depth and accent pathology in the iris, conjunctiva, aqueous humor, and lens not readily visible with direct illumination. For example, intraocular inflammation can result in the accumulation of proteins in the anterior chamber, which cause a cloudy appearance in the aqueous fluid. When viewed directly, the eye appears milky or opaque, but with lateral illumination it is possible to differentiate between anterior chamber cloudiness (flare) and corneal opacity. 12
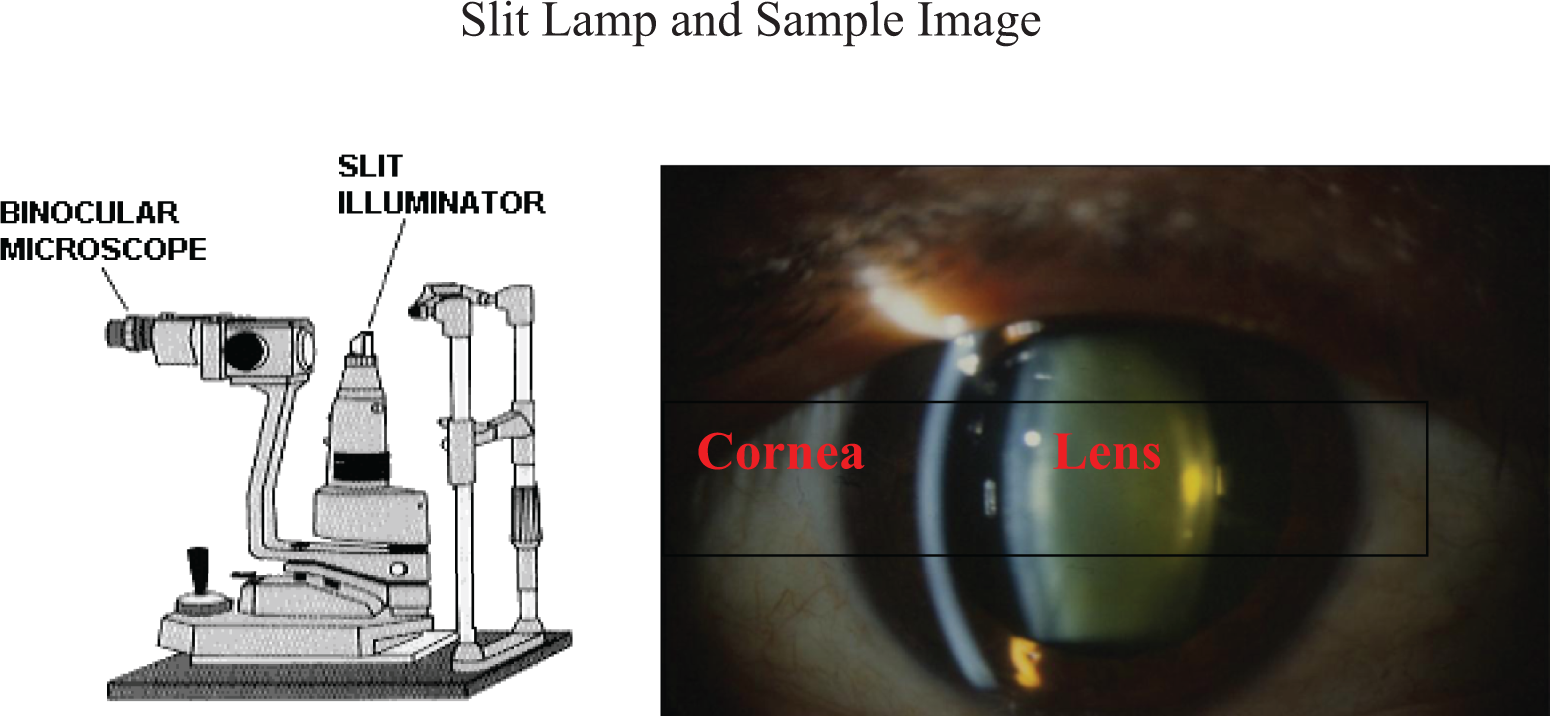
Binocular microscope with slit illuminator (left) and a normal eye with slit illumination showing the cornea, anterior chamber (AC), and lens (right).
With the slit beam in the wide-open position, direct inspection of the external features of the eye can be undertaken to include lashes, lids, cornea, and conjunctiva for inflammation (conjunctivitis and blepharoconjunctivitis) and pigment changes. Breakdown of the corneal epithelium, suspected abrasions, and abnormal tear distribution due to toxicity from, for example, β-blockers, antidepressants, or antihistamines can be highlighted using fluorescein dye. 13 The slit lamp can also be fitted with a tonometer to measure the intraocular pressure (IOP) in humans. A handheld tonometer is typically used in animals. Finally, although it is possible to inspect features at the back of the eye such as the optic nerve head, macula, and fovea using a condensing lens, typically this inspection is done using an ophthalmoscope or fundus camera to image such features.
Ophthalmoscope
Light entering the eye is reflected out along the same path it enters. Therefore, in order to visualize the fundus, it is necessary for the observer to be in line with the source of light. 14 The direct ophthalmoscope is a handheld device with a mirrored aperture by which the examiner can be in line with the light source. This method provides a magnified view of the fundus and also requires the ophthalmologist to be in close proximity to the patient’s eye. This can be difficult with some laboratory species. The indirect ophthalmoscope uses the same mirrored aperture but includes a convex lens to allow for a greater field of view and can be used at arms length. Direct or indirect ophthalmoscopy requires cooperation of the patient or the animal to achieve the best field of view. For some laboratory animals, sedation is often required. Ophthalmoscopy is both clinically and nonclinically the most common examination used to inspect the features of the fundus and make a diagnosis of normality or pathology. Results of the examination are typically documented with detailed notes, but to capture pictures for follow-up and presentation of results, a fundus camera operating on similar principles is required.
Fundus Camera
In many cases, it is important to document the pathology of the eye whether to track the progression of disease or to provide images to an independent reading center. The fundus camera uses the same principle as ophthalmoscopy in that the image capture device must be in line with the light source. In general, there are 2 types of fundus photography, flash photography that uses a bright flash to capture a color image and confocal scanning laser ophthalmoscopy (cSLO) that uses a scanning laser to collect a high-resolution monochrome image of the fundus (Figure 2). Flash photography has the advantage of reproducing exactly what an examiner would see using an ophthalmoscope. However, the cSLO can produce more detail and focus through the retina into the choroid. In addition, for standard fundus imaging, the cSLO uses an “invisible” infrared laser that is more comfortable for patients and can better penetrate opaque media. Most commercial flash photography cameras are designed for the human eye and can be easily used in large animals for standard fundus imaging. For small animals, an additional condensing lens is often required. The cSLO does not require an additional lens when imaging animals although the lack of color information can make it difficult to document pathology in some animals such as a change in tapetum color seen in dogs and cats with ocular stress.
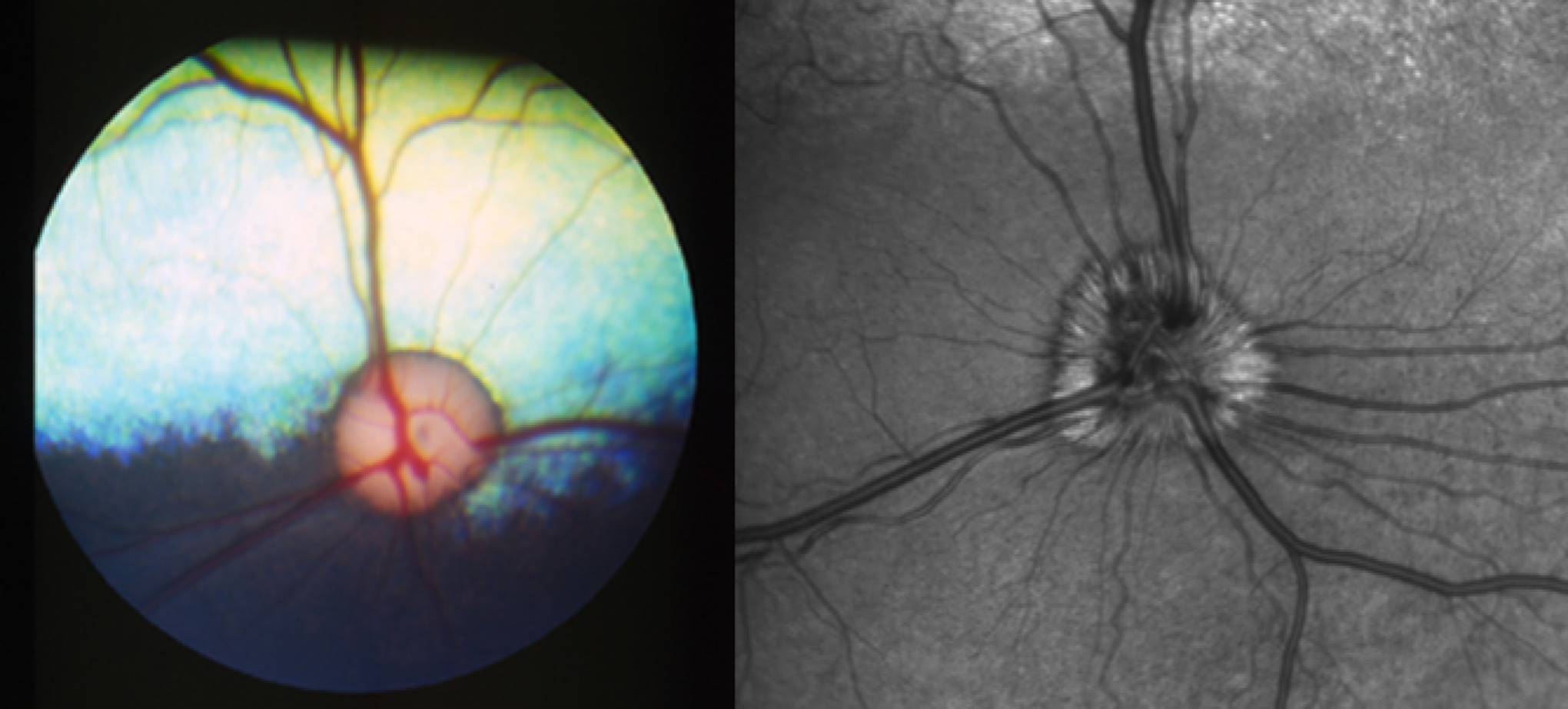
Color fundus photographs of a normal dog with normal bluish tapetum (left) and normal dog optic nerve head imaged using cSLO (right). cSLO indicates confocal scanning laser ophthalmoscopy.
Angiography
An important feature of modern fundus cameras is the ability to image the retinal and choroidal vasculature. The retinal vasculature lies between the front of the eye and the retina and is visible during the fundus examination although the dynamics of blood flow are not easily discernible. Fluorescein angiography (FA) involves the intravenous injection of a fluorescent contrast agent to visualize the pattern of retinal vasculature filling and can identify areas of nonperfusion or ischemia as well as regions of excessive blood flow or leakage. For example, in advanced diabetic retinopathy, it is possible to observe both pooling of fluorescein dye around new and leaking vessels and areas of ischemia with insufficient blood flow and fluorescein signal (Figure 3). 15
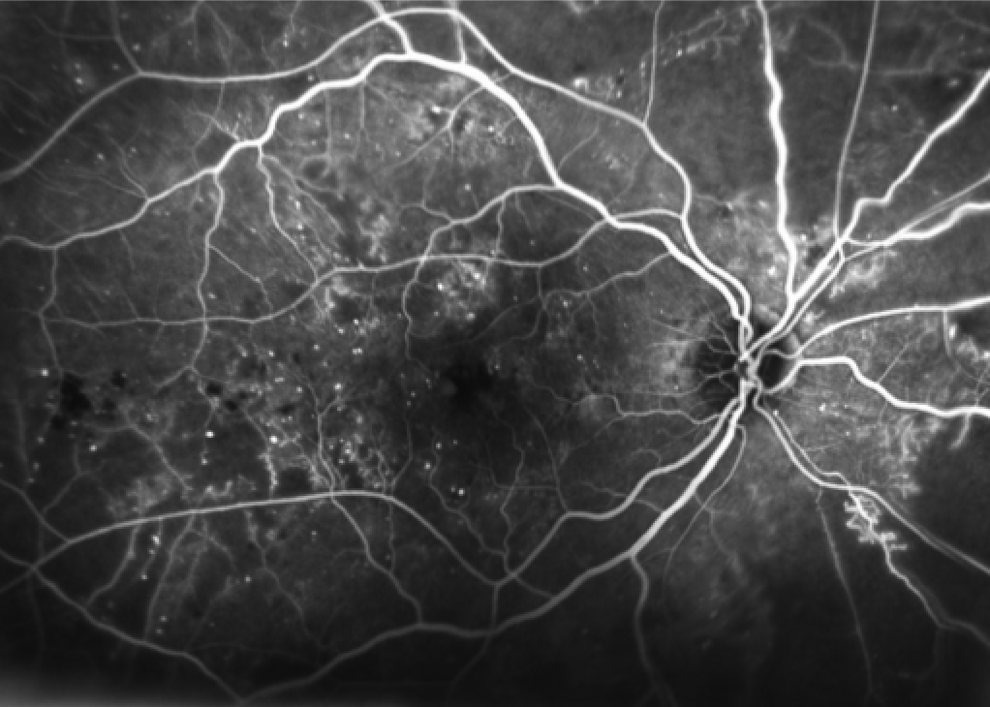
Fluorescein angiogram of a patient with advanced diabetic retinopathy. Fluorescein is pooling as small bright dots indicating microhemorrhages, while the dark regions indicate restricted blood flow and ischemia.
The choroidal vasculature is located behind the retina and the pigment-dense retinal pigment epithelium (RPE). Fluorescein emits light in the green spectrum, which is easily absorbed by the pigment in the intact RPE. The choroid can only be visualized under certain circumstances using FA. For example, a break in Bruch membrane and RPE can result in vessel growth from the choroid into the retina. This new vessel growth, choroidal neovascularization (CNV), can be easily visualized with FA. 16 Degeneration of the tight junctions between RPE cells can be caused by local or systemic toxicity and can result in a “window” effect, where the fluorescein-filled choroid can be seen through defects in the RPE.17,18 In addition, fluorescein can be used to visualize the choroid in albino animals that are devoid of retinal pigment or animals with a tapetum such as dogs which have a nonpigmented RPE in front of the tapetum. 19 Imaging of the choroid with an intact pigmented RPE is done using the infrared light emitter indocyanine green (ICG). Infrared light is not absorbed by the RPE and can help diagnose the conditions such as retinal detachment or early CNV. 16
Optical Coherence Tomography
The OCT is an imaging method, which uses a broadband near-infrared laser that is split with one beam targeted at the target tissue and the other down a reference path that is at equal distance from the camera as the target tissue. The beams are reflected back to the camera and reconstructed into a cross-sectional image of the target tissue. 20 Multiple cross-sectional images can be taken in close proximity to create a 3-dimensional volume image. This method works best on tissues with distinct boundaries and reflectance, such as tumors, blood vessels, or parts of the eye such as the retina, cornea, and anterior segment (see retina in Figure 4A). Under ideal circumstances, some have reported up to 3 µm resolution in humans, which is sufficient to diagnose retinal disorders such as edema, detachment, and thinning due to cell death in various layers of the retina. The thickness of the human retina varies from approximately 210 to 340 µm depending on where in the retina (fovea, macula, and periphery) the image is taken, whereas the mouse retina has an average thickness of 209 µm.21,22
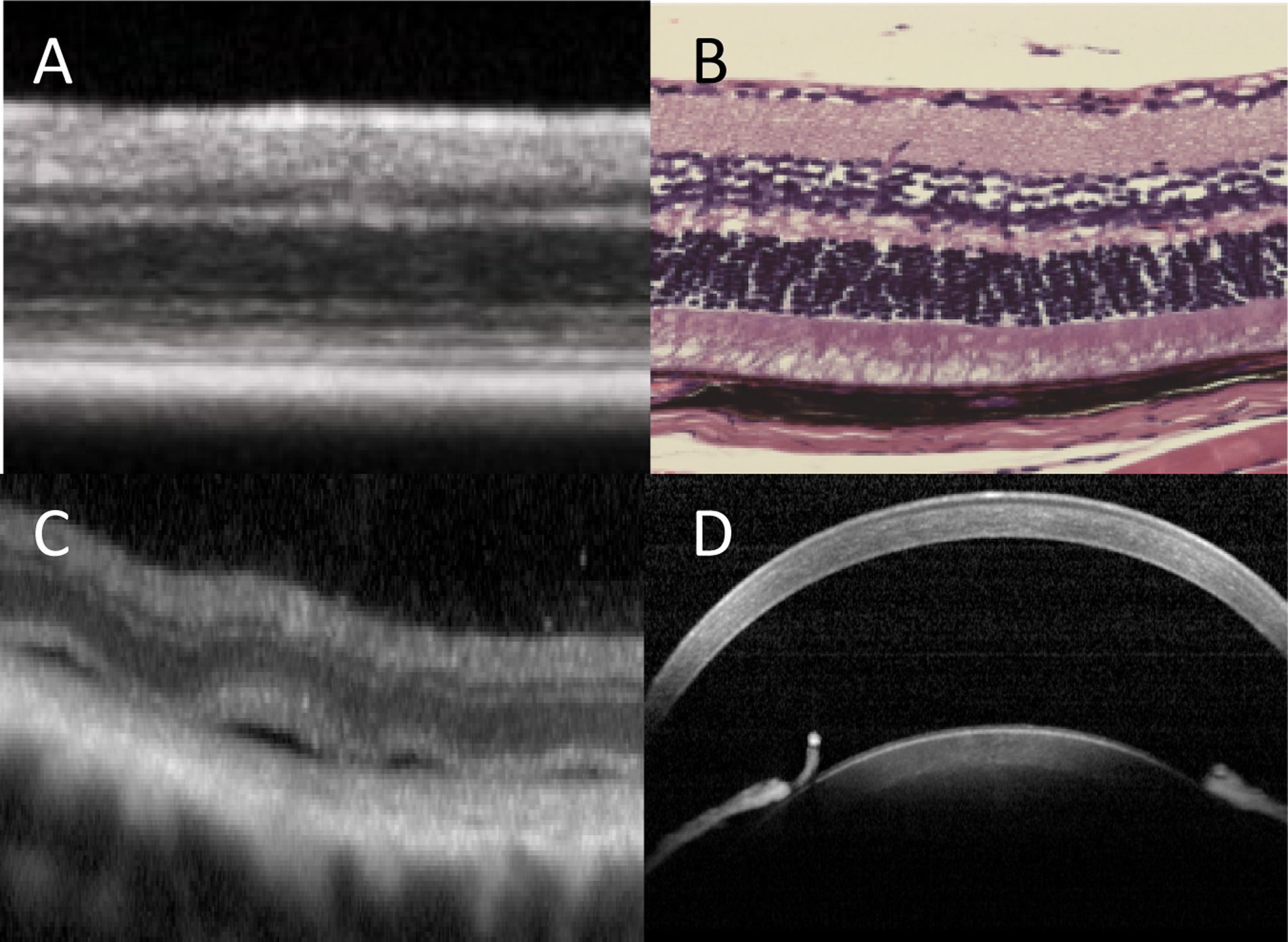
A, The OCT image and (B) histology section from a C57BL/6 mouse retina at a similar area of the retina. There is no perfect alignment of all retinal layers, because the images are from different animals and likely different areas of the retina. C, The OCT image of a dog retina with multiple small retinal detachments. ICG angiography (not shown) helped direct where to look for detachments. D, The OCT image of a normal rat cornea (top), lens, and iris (bottom). ICG indicates indocyanine green; OCT, optical coherence tomography.
The OCT imaging is being used more often in animal testing as an alternative to histology and as a method to track retinal and corneal changes without sacrificing the animal thereby allowing for the changes to be followed over time. Figure 4A and B shows a side-by-side comparison of an OCT image and histology of the retina of a c57BL6 mouse. Although there is no perfect correlation between images, the differences are likely due to changes in tissue thickness during histology processing and selection of image location. The OCT imaging has a distinct advantage of capturing features such as small retinal detachments that can often occur when doing toxicology screening. Using ICG angiography to highlight the location of detachments and following with OCT imaging, it is possible to diagnose the small features that are difficult to detect with histology or a fundoscopic examination. Figure 4C shows an example of an OCT image, where small retinal detachments are evident, which were not seen during the fundoscopic examination. The normal anterior segment of the rat is shown in Figure 4D.
Electrophysiology
The functional measurement most people are familiar with is the eye chart, where patients are asked to report the smallest images they can see. This threshold of perceivable vision is visual acuity (VA), and while this is the standard of care for patients, it is difficult with current technology to reliably measure VA in animals. Instead, the electrical activity in response to visual stimulation of the retina and brain can be measured using procedures such as the electroretinagram (ERG) and the visual-evoked potential (VEP). The ERG is the most commonly used tool to evaluate the function of the retina in patients that cannot easily read an eye chart, for example, infants and laboratory animals. 23 The examination is similar to an electrocardiogram such that electrodes are placed around the target tissue to measure the passive or induced electrical response.
The retina comprises 3 distinct layers—photoreceptor, bipolar, and ganglion cell layers. Light is absorbed by photoreceptors, amplified and processed by bipolar cells, and ultimately converted into action potentials by ganglion cells for transmission to the brain. Vertebrate animals have 2 classes of photoreceptors—rods and cones. Rods are highly sensitive to very low levels of light and provide “starlight” vision but are easily saturated with a small background light. Cones provide color and daytime vision and are not easily saturated and provide vision over a broad range of light intensities from twilight to full sun. Once the patient is sufficiently dark adapted, the rod or scotopic system produces up to a 5-fold larger ERG response compared to the cone or photopic system. For diurnal animals or patients, 60 minutes of dark adaptation is usually sufficient for dark adaptation, while nocturnal animals such as rodents can take up to 12 hours for complete dark adaptation.
The ERG encompasses a broad spectrum of examinations all of which probe some aspect of retinal function. The most common full-field ERG stimulates the entire retina with a uniform or Ganzfeld field of light. The intensity, color, or shape of the light pulse can be altered to probe various cell types. For example, a dim light under completely dark conditions can elicit a response (b-wave) that originates from bipolar cells. Brighter stimuli are used to record photoreceptor function, and a background light will saturate the rod pathway and isolate cells in the cone pathway. The amacrine cell response can be seen as an oscillating signal found on the leading edge of the b-wave and can be isolated with filtering techniques.
For toxicology studies or initial screening of patients with potential pathology, a 4-flash full-field ERG series is recommended. 24 Once dark adapted (1) a moderate flash intensity is used to elicit a rod b-wave followed by (2) an increase in flash intensity to evoke a rod a-wave and b-wave; oscillatory potentials from the inner retina can also be electronically filtered from this response. The patient is then light adapted to a background that is sufficiently bright to saturate the rod activity. Subsequently, (3) with the same flash intensity as used in (2) above, the cone a-wave and b-wave are recorded followed by (4) the response to a flickering light (frequency is species dependent) to probe the cone pathway inner retinal function. 25 This paradigm can be altered if a compound is suspected to affect a retinal function not captured with the above paradigm.
Since the full-field ERG stimulates the entire retina uniformly, it is not possible to distinguish between an event that comprises a discrete area of the retina or the retina as a whole. For example, a 30% decrease in ERG amplitude could be due to a 100% loss of 30% of the retina (laser burn, ocular tumor, and isolated blood vessel rupture) or a 30% loss from 100% of the retina (pan-retinal photoreceptor degeneration). A secondary examination such as fundus photography with OCT imaging can help distinguish between these events, or focal and multifocal ERGs can be used to record from distinct regions of the retina. 26 The ERGs from small patches of retina will result in reduced signal size and decrease the signal-to-noise ratio making the results more difficult to interpret.
For both structural and functional reasons, it is difficult to isolate the small ganglion cell response from the full-field ERG dominated by other cellular potentials. The scotopic threshold response (STR) is a dark-adapted ERG signal recorded with very dim light stimuli and can reflect both ganglion and amacrine cell function, but the ratio varies by species. The STR has a very small amplitude, requires considerable averaging of signals, and is sensitive to the level of dark adaption thus making it difficult to use as a robust clinical end point. The photopic negative response (PhNR) following the cone b-wave has been shown to be diminished with glaucoma or compounds that block ganglion cell activity. However, a definitive link is yet to be demonstrated between the severity of glaucoma and a progression of PhNR loss.
If the ERG examination appears normal and the patient still experiences visual deficits or the laboratory animal is suspected to have vision loss, it is possible that transmission of the retinal signal to the brain is compromised. For example, undetectable ganglion cell loss can occur in early glaucoma or with optic nerve damage following a concussion, traumatic brain injury, or an ocular tumor. The VEP is a specialized electroencephalogram where 1 to 3 electrodes (dependent on species) are placed at the back of the skull over the occipital lobe, and the brain response to an alternating pattern of light is recorded. 27 The VEP signal is very small (5-10 µV) but is relatively free of artifacts with proper electrode placement.
Visual Acuity
The VA is a primary end point for determining the threshold of the visual system to perceive and process light stimuli in the external environment. As important as VA measures are in patients, there is a paucity of methods to assess similar visual function in laboratory animal models. The VA is the threshold of an ability to recognize the objects of decreasing size (spatial resolution) or the difference in luminance between the objects (contrast sensitivity). Measurement of VA encompasses all parts of the visual system, from light passing through the cornea, absorption of light by the retina, signal transduction to the brain, and finally, cognitive recognition followed by a behavioral response by the patient.
The most widely used method for evaluating VA in the laboratory is an optokinetic response (OKR). This measure is based upon a reflex action of the patient to a moving stimulus. One issue with OKR is that it does not necessarily require the entire visual system. As a reflex, the measure does not require the visual cortex or integrative systems of the brain. It does, however, involve integrated function of the retina and is a useful tool to evaluate the visual function in conscious patients.
Prusky and colleagues have used an OKR system in mice and rats, which generates a virtual rotating cylinder on 4 computer monitors.28–31 These screens surround a platform on which the unrestrained animals are placed. The animal reacts to the “rotating” grating with small head and neck movements that are tracked by the experimenter. The grating spatial or contrast resolution can then be reduced to determine the threshold of OKR. Species/strain differences in VA have been observed,28,31 and loss of OKR contrast threshold after experimental induction of diabetes in rats has been noted as well. 32 Although the system has demonstrated utility in evaluating the aspects of VA, it requires significant technician training and has low throughput.
Another family of methods used to determine the visual function in rodents is a maze or water-escape procedure in which animals are required to make decisions based on visual stimuli. For example in a Y-maze, the animals must travel down a long “stem” of the Y, and based upon visual stimuli at the end of each arm, select one arm for behavioral reinforcement. 33 The reinforcement can be in the form of a food reward or if the maze is filled with water, an escape platform. Similarly, an open pool of water (Morris water maze) can be used with visual stimuli showing the location of the escape platform. Static or moving gratings can be used to determine spatial or contrast resolution threshold. These maze procedures have an advantage compared with the OKR in that the entire visual system, including decision making, is required to locate the reward, but these methods are also labor intensive and have low throughput.
A system that appears to combine the aspects of both the OKR and the maze systems is an operant conditioning procedure reported by Carlsson and Swedberg. 34 In this study, rats were trained to differentially respond on levers based upon visual stimuli presented via a computer monitor in order to obtain a reward. This procedure can be automated, reducing the need for constant technician interaction with the animal and by employing multiple systems high throughput can be achieved with a single technician. This capability permits repeated measures of VA over time in the same subject, and data from this assay are consistent with reports in OKR and maze methods.
Microscopic Findings in Ocular Toxicity Studies
The detection of morphologic changes in ocular tissues resulting from systemic toxicity involves clinical ophthalmic examination and microscopic examination. 3 ,35 –37 For the toxicologic pathologist, successful identification of toxicologic microscopic changes in ocular tissues not only requires an understanding of the differences in ocular anatomy among laboratory animals but also an understanding of clinical ocular findings, tissue artifacts, and spontaneous ocular findings. 38
At necropsy in toxicology studies, the globes should be enucleated as soon as possible after death to minimize postmortem autolysis, especially of the retina. 39 Globes should always be handled as gently as possible with minimal tension to avoid morphologic artifacts, such as retinal detachment and artifacts in the optic nerve. The retrobulbar optic nerve should remain attached to globes of all animals in order to obtain a cross-section of the optic nerve for the examination of axons of ganglion cells. Ocular sections should generally be along a plane that is through the pupil. With few exceptions, the extraocular tissues, including lacrimal glands, should be carefully removed from the globe to enhance fixation and visualization of landmarks used for trimming. Globes need to be identified as right (oculus dexter [OD]) or left (oculus sinister [OS]) after enucleation, and the identification should be maintained throughout the entire preparation process.
The purpose of fixation is to preserve ocular tissues, but all fixatives have advantages and disadvantages that are important to understand. If using a fixative for the first time, it is highly recommended to ensure the fixative is appropriate and functions well—do a pilot study! Regardless of the fixative, 48 to 72 hours should be allotted for complete fixation of nonrodent globes and at least 24 hours for rodent globes to avoid artifacts, especially during trimming. 40 Commonly used fixatives include glutaraldehyde and fixatives containing glacial acetic acid (eg, Davidson or modified Davidson fixatives).40,41 Fixation of nonrodent globes with glutaraldehyde is facilitated by use of intravitreal injection or the creation of a small (∼5mm) window after a short (5-30 minutes) period of immersion fixation. If technical holes are created during fixation, they should not be located in the desired plane of section. 40 One potential disadvantage of glutaraldehyde (especially for rodent globes) is a distorted shape associated with osmolarity. 42 A potential disadvantage of fixatives containing glacial acetic acid is excessive cell swelling that causes artifacts (eg, clefts in the corneal stroma, vacuolation of corneal endothelial cells, and swelling of lenticular fibers, especially in the lens of monkeys).40,43 Following fixation, the globes are trimmed in a posterior-to-anterior direction using a long, sharp blade and using the optic nerve and the long-posterior ciliary artery as landmarks. Trimmed globes should be put into megacassettes for processing and then embedded and sectioned by an experienced histotechnologist. 44
Terms used to describe clinical and microscopic ocular findings should be specific in order to ensure accurate communication between the pathologist, toxicologist, and maybe more importantly, the sponsor. Since the cornea and lens are normally transparent, any interference with transparency may be referred to as an opacity. Focal clinical opacities in the cornea may microscopically correlate with deposits (eg, mineral) or fluid (eg, edema). Focal opacities in the lens may correlate with focal accumulation of lens epithelial cells, swelling of lens fibers, or degenerative changes. Truly degenerative (nonreversible and permanent) changes in the morphologic appearance of the lens may be referred to as cataract, but not all diffuse lenticular opacities are permanent opacities and, therefore, not cataracts. Reversible opacification of the lens may be induced by various stimuli including drugs (eg, opioids), cold temperature (ie, cold cataract), anoxia, asphyxia, dehydration, arrest in blinking, and stress.45,46
Since ocular structures, such as the retina, are composed of different cell types, terminology used to identify a finding should be as specific as possible. The term retinal degeneration is a vague term that needs to be defined as to the cell type (eg, photoreceptor) and area (eg, outer sensory retina) involved. When identifying an ocular finding, the most specific term (eg, single-cell necrosis or layer thinning) should be used. Once an ocular finding is detected, it needs to be accurately classified as a background (ie, iatrogenic or spontaneous) or a treatment-related finding and labeled with the proper diagnostic term. Iatrogenic findings may be associated with a test method, such as orbital inflammation from retrobulbar venipuncture in rodents. 47
Spontaneous background findings occurring in the ocular structures of laboratory animals are well referenced in the literature.48–50 Spontaneous alterations may be congenital, inflammatory, hyperplastic, or neoplastic and may be associated with inherent specifics of the test animal, such as strain, pigmentation, age (eg, senile retinal atrophy), environmental conditions (eg, light-induced retinopathy), or nutrition.51–53
A condition that is generally protected from occurring by the presence of melanin is phototoxic or light-induced retinopathy. 54 The primary ocular mechanism for controlling light exposure is constriction of the pupil by the pigmented iris and absorption of light by the iris, but light-induced retinopathy has been reported in pigmented rats when pupils are dilated, especially with constant illumination.55,56 Natural exposure to light may contribute to a gradual slow loss of photoreceptors through the aging process, but short exposure of high levels of light intensity may cause a severe loss of photoreceptors. 51 The severity of the degeneration is related to the distance from the light source. Therefore, photoreceptor degeneration will be more severe in albino animals in cages close to the room light source (generally those on the top of the cage rack), even if the overall room light intensity is within the acceptable limits.51,52,57–59 In addition to light intensity, other factors that influence the development of light-induced retinopathy in albino rodents include wavelength, duration of exposure, length of time for dark-adaptation, age of initial exposure, maturity of the retina, gender, diet including a deficiency of nutrients, and so forth.60,61 For example, in albino rats, females have a tendency to be more affected than males. 51 Generally, retinal findings of light-induced retinopathy are characterized by a decrease in the thickness of the outer nuclear layer (ONL; normally thicker than the inner nuclear layer), disorganization and thinning of the layers of outer segments and inner segments, and possibly the presence of displaced photoreceptor nuclei.
Some corneal findings, such as subepithelial calcification, may be a spontaneous finding (eg, corneal dystrophy in rodents) or a treatment-related finding.62–68 Other treatment-related ocular findings may be secondary to changes in other ocular structures. For example, keratoconjunctivitis sicca may develop following a treatment-related decrease in precorneal tear film. 69
Some findings are an exaggeration of a normal process, such as displacement of photoreceptor nuclei. This represents a gradual loss of photoreceptors that occurs with age in the retina of humans and laboratory animals.70,71 The displaced photoreceptor nuclei may be detected when they are observed in the inner and outer segment layer (ISL and OSL) of the retina. Displaced photoreceptor nuclei generally have a normal density of chromatin, although pyknotic nuclei are occasionally observed, especially when an intravitreal injection has occurred.
The predicative value of ocular findings in laboratory animals may vary between rodent and nonrodent species and between animals and humans. 72 Ocular findings in animals may be difficult to correlate with ocular findings in humans, since some drugs that cause retinal lesions in laboratory animals do not appear to cause retinal changes in humans. 73 One reason may be binding of the compound to melanin.6–8,74 Treatment-related ocular findings may also occur in ocular structures that are not present in the human eye (eg, Harderian gland in rodents and tapetum lucidum in dogs). 9 These findings are generally considered nonrelevant in regard to human toxicity.38,75–78 Some treatment-related ocular findings, such as phospholipidosis, are considered to be potentially reversible and, therefore, the biological importance may be questionable.79–86 Unfortunately, other treatment-related ocular findings can be quite serious because the target cell has limited or no capability for regeneration in the human eye (eg, human corneal endothelial cells and photoreceptors).87,88 Additional aspects of toxicologic ocular pathology are well referenced in the literature.73,89,90 The effects of compounds on the RPE have been thoroughly reviewed by Mecklenburg and Schraermeyer. 91
Case Study: Ocular Toxicity of an Oncology Therapeutic—Obstacles and Impact to Development
The previous sections described different techniques used for the assessment of ocular toxicity in experimental animals. Furthermore, it was shown that many of the noninvasive methods also have use in human medicine. Therefore, the results from toxicity studies using a primarily noninvasive technique, for example, OCT imaging and ERG, can potentially translate to human safety. In spite of this ability, understanding the potential mechanism of pharmacodynamics can further provide data for determining the potential risk to patients, or whether the drug has sufficient “viability” to proceed in clinical development. The impact of the resulting data on the key considerations for drug development is discussed in the next section including patient safety and quality of life, relevance and feasibility of predictive monitoring, and potential regulatory concerns.
To provide patients with terminal cancer faster access to new and innovative drugs, oncology drugs that meet certain criteria are developed under the purview of ICH S9 guidance for nonclinical safety testing. 92 In essence, ICH S9 takes a more risk-tolerant approach to drug testing than the more traditional ICH M3(R2). Nevertheless, ocular toxicity can profoundly affect clinical development of even these higher risk oncology drugs. To illustrate the impact of this, the specific case of PF847, a heat shock protein (HSP90) inhibitor for use in patients with late-stage terminal cancer, is discussed. Data essential for decisions addressing the viability of the program are presented including data generated during the standard preclinical safety studies and investigative studies to partially elucidate a mechanism for this toxicity.
Several antitumor agents are currently being developed based on their targeted activity to the HSP90 class of molecular chaperone.93–97 The HSP90 is a compelling target for oncology indications because HSP90 is required by many kinases known to drive oncogenic growth. Some of these kinases (eg, EGFR, HER2, RAF, CDK4) have been the direct target of kinase-inhibitory therapeutics because of their known central role in tumor growth. These targeted kinase inhibitors have been highly effective in modulating tumor growth. Whether due to the genetic unstable nature of tumors and/or the relatively rapid proliferation of these cells, tumors appear to be uniquely dependent on HSP90 protein expression for growth. Inhibiting HSP90 interaction with these client proteins can potentially inactivate a spectrum of key oncogenic drivers and has been an active and popular tumor control strategy.
PF847 was a compound selected to advance into preclinical safety studies over several candidate molecules. Toxicology studies exploring the effects of repeated doses of PF847 over the course of 1 week indicated that the most affected organs were the gastrointestinal tract and the bone marrow (lymphoid and hematopoietic toxicities) of rats and dogs. For these early exploratory safety studies, ocular assessments were not performed. PF847 was chosen over similar candidates, in part, because of better tolerability in these short-term repeat dose studies, good efficacy in preclinical models, and its good oral bioavailability. These properties made PF847 a good candidate for advancement to the next stage of drug development including the regulatory-focused studies necessary for an investigational new drug (IND) filing. Two of these IND-enabling studies were a 1-month rat (Wistar-Han) study and a 1-month dog (Beagle) study.
In both 1-month toxicology studies, gastrointestinal and hematopoietic toxicities were observed that were similar to the findings in the 1-week exploratory safety study, although the effects in rats were observed earlier during treatment and at higher doses. Doses in the 1-week study were up to 50 versus 20 mg/kg in the 1-month study. The high-dose group dogs in the 1-month study also had a novel finding that occurred concurrently with the onset of the gastrointestinal toxicity. Initially, it was noted that the dogs were walking into objects and displayed other indications of possible compromised vision. In dogs administered PF847, these functional visual deficits became evident beginning on day 10. Subsequent ophthalmologic examinations showed bilateral mydriasis, diminished direct pupillary light reflex (PLR), and diminished menace reflex. Bilateral, mild tapetal hyperreflectivity, and mild narrowing of the retinal vasculature were noted in individual animals at the end of the dosing period. Due to the severity of the gastrointestinal toxicity, the high-dose male dogs were euthanized approximately 14 days into the planned 1-month study. Dogs in the male recovery group were taken off the planned dosing regimen at this earlier time and were started on a 1-month recovery period. Similar but milder findings were noted in female dogs in the high-dose group and were dosed a full 30 days. Following 1 month of recovery, the findings in the high-dose male dogs did not reverse completely; mildly diminished bilateral PLR with menace reflex, narrowing of the retinal vasculature, and tapetal hyperreflectivity were noted. These results suggested the dogs had recovered some of their sight, but that some damage to the retina persisted. These ocular findings were observed in the high-dose group only. There were no similar ocular findings in the rats, although gastrointestinal effects were quite evident at the high dose.
Upon microscopic evaluation of the eyes, a severe retinal degeneration was found in the eyes of male and female high-dose dogs only (Table 1). Retinal degeneration, characterized primarily by a disorganization and decreased thickness of the ONL due to decreased numbers of photoreceptor nuclei, particularly near the outer limiting membrane, was noted in dogs from the high-dose group (Figure 5). Based on histological assessment, the rod photoreceptor cells appeared to be predominantly affected. Other features of degeneration included decreased thickness, sometimes with accompanying disorganization, of the photoreceptor ISL and OSL and photoreceptor nuclei in the ISL and/or OS.
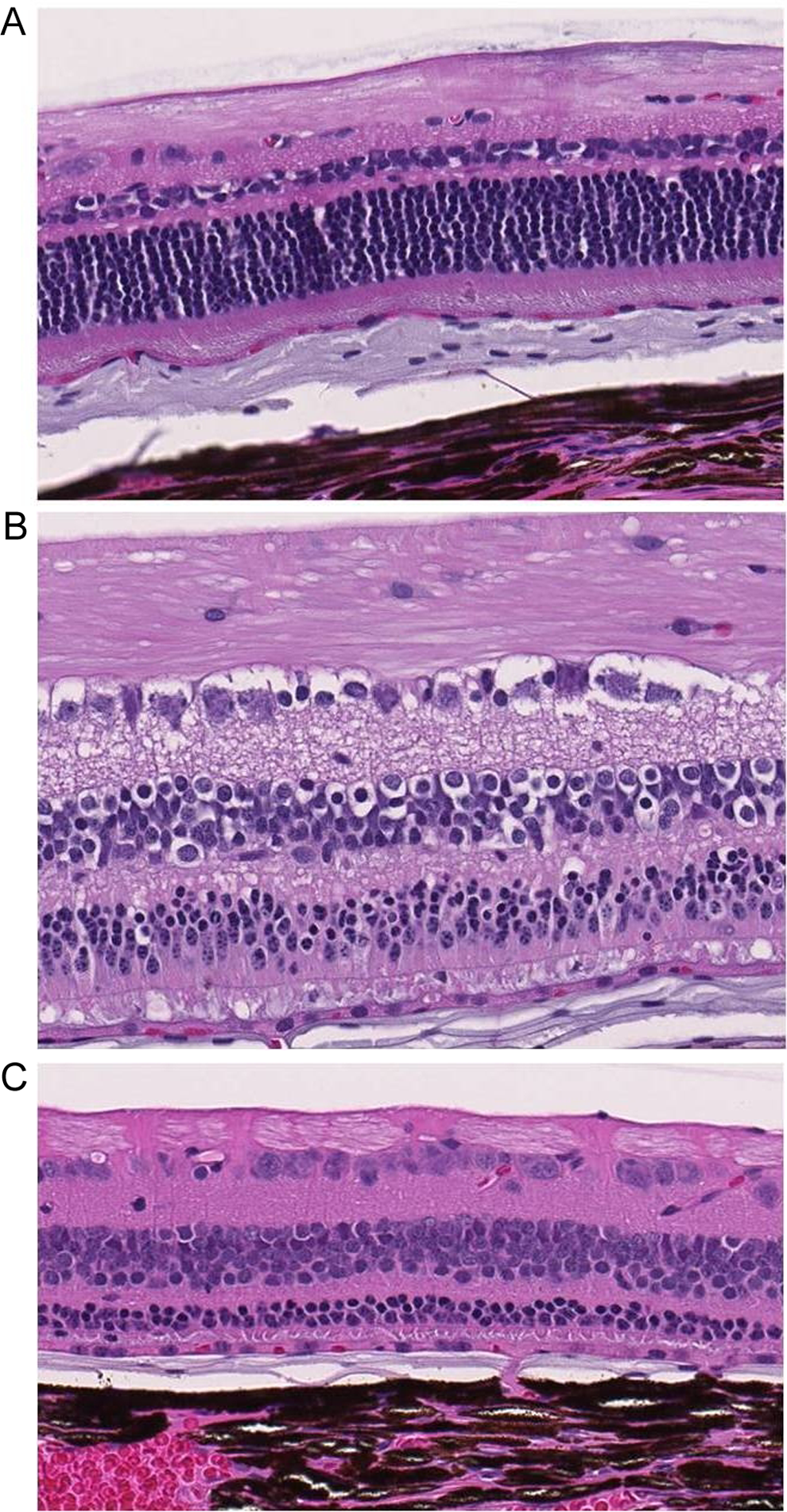
Retinal changes following administration of PF847 before and after a 1-month recovery period. Control dog retina (A). Cellular toxicity was apparent after 12 days of PF847 administration to dogs (B), most notably in the photoreceptor layer. After a 1-month recovery period (C), the retinal layer had a diminished outer nuclear layer and diminished photoreceptor inner and outer segments indicating irreversible loss of photoreceptors. Magnification ×200.
Incidence and Severity of the Microscopic Lesions in Dogs Treated With PF847 for 14-30 Days.a
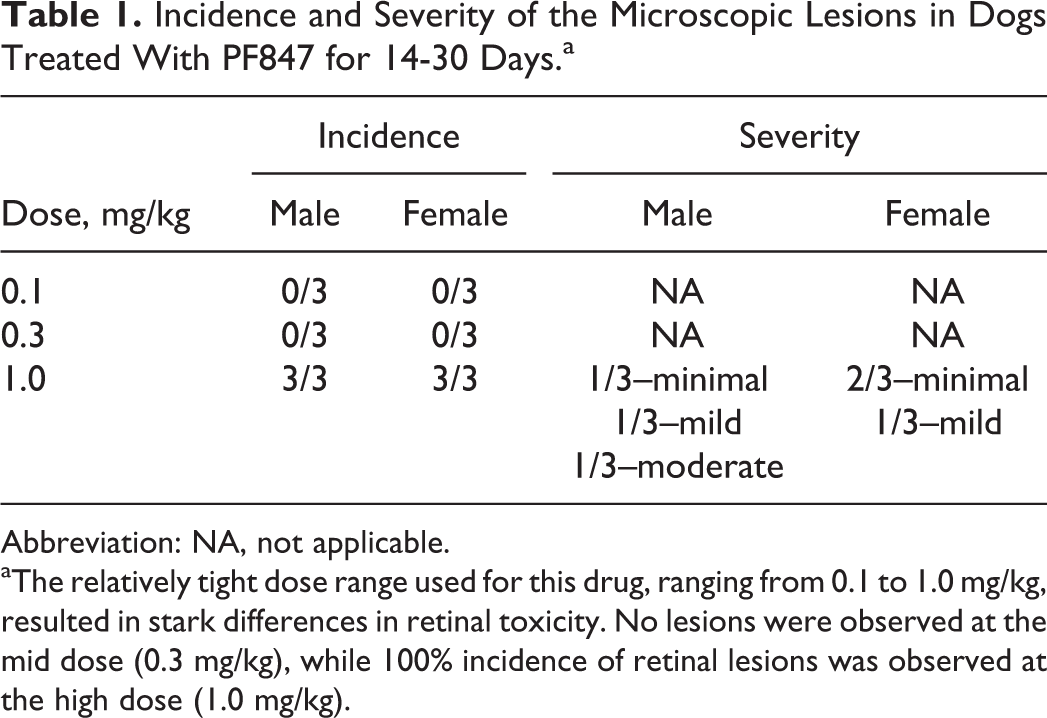
Abbreviation: NA, not applicable.
aThe relatively tight dose range used for this drug, ranging from 0.1 to 1.0 mg/kg, resulted in stark differences in retinal toxicity. No lesions were observed at the mid dose (0.3 mg/kg), while 100% incidence of retinal lesions was observed at the high dose (1.0 mg/kg).
There was no indication of subtle or early signs of retinal degeneration in the lower dose levels, and no ocular findings were observed in rats at any dose level. In summary, the findings were considered to be of significant concern and were investigated further. Based on reproducibility and the close association of the ocular findings with the projected efficacious doses in the clinic, these findings were considered test article related and potentially target related. Pigmented rats (Long Evans) were used in an attempt to reproduce the ocular findings seen in the dog, but the retina from rats in these studies was also unaffected at levels producing gastrointestinal and hematopoietic toxicities. It was not certain why the dog was more sensitive to PF847 compared with the rat.
Although PF847 was intended as a therapeutic for late-stage, terminal cancers, where patients and physicians are more tolerant of adverse effects, ocular toxicities were evaluated for whether the risk to patients’ remaining duration and quality of life would be considered reasonable. Blindness is considered an unacceptable risk of potentially modest life extension for many patients. This later consideration factored into the strategy of how to best mitigate the risks associated with this drug if it was to be considered for clinical trials. Since blindness was considered an unacceptable clinical outcome for patients with cancer, and the preclinical toxicology studies demonstrated toxicity only after irreversible damage had been done to the photoreceptors, a more effective assay would be needed in the clinic. Specifically, an assay was required that predicted the onset of any photoreceptor toxicity early enough so that treatment could be stopped and allow for recovery of the retina.
The ERG was considered a sensitive measure of retinal function and therefore a potentially appropriate assay, although implementation of ERG monitoring in the clinic can be quite challenging. The OCT is potentially capable of detecting retinal toxicity but would likely detect existing damage rather than predict an onset. A positive OCT “signal” may occur too late to be clinically useful. For ERG acquisition, a logistical challenge appeared to be finding an ERG-capable clinical facility near the desired patient population. It was also unclear whether an ERG would be sufficiently sensitive to distinguish PF847-induced retinal changes from individual variability in patients or even preclinical study species. To determine whether ERGs could be considered a predictive monitoring tool, ERG capabilities under laboratory conditions in the dog were investigated. The goal, as it applied to potential clinical administration of PF847, was to determine whether the changes in retinal functional capacity, as measured by ERGs, would precede the structural damage that had been observed in the toxicology studies. If the ERG demonstrated that functional changes predict future structural damage before that damage occurs and becomes irreversible, then theoretically clinical therapy could be suspended in ERG-monitored patients to allow the retinas to recover and thereby eliminate the risk of blindness as a result of therapy.
To determine whether an ERG measure of retinal function was sensitive enough to detect retinal changes within the 14 to 30-day time frame consistent with those changes observed in the toxicity studies, 4 male dogs were administered daily doses of PF847 throughout a 12-day study and examined for ERG changes at days 4 and 11. Both scotopic (dark adapted) and phototopic (light adapted) luminance response were examined. Reproducible ERG waveforms were acquired from all 4 dogs prestudy. Amplitudes of a- and b-waveforms were very consistent across dogs and demonstrated luminance responses to increasing light levels consistent with ERG responses reported previously in dogs. 98
Under scotopic conditions, dogs treated with PF847 showed a dramatic reduction in waveform amplitudes (Figure 6). There was an ∼50% to 60% reduction in the amplitudes of a- and b-waves recorded 6- to 9-hour postdose (PM) on day 4. Interestingly, these decreases were smaller or absent in dogs recorded 2- to 5-hour postdose (AM) on day 4. By day 11, a- and b-wave amplitudes were reduced ∼80% to 90% in both AM and PM recording sessions. Under photopic conditions, b-wave amplitudes were reduced ∼50% to 60% in dogs administered with PF847 as early day 4 and continuing through day 11. The a-wave amplitudes were not detectable under photopic conditions.
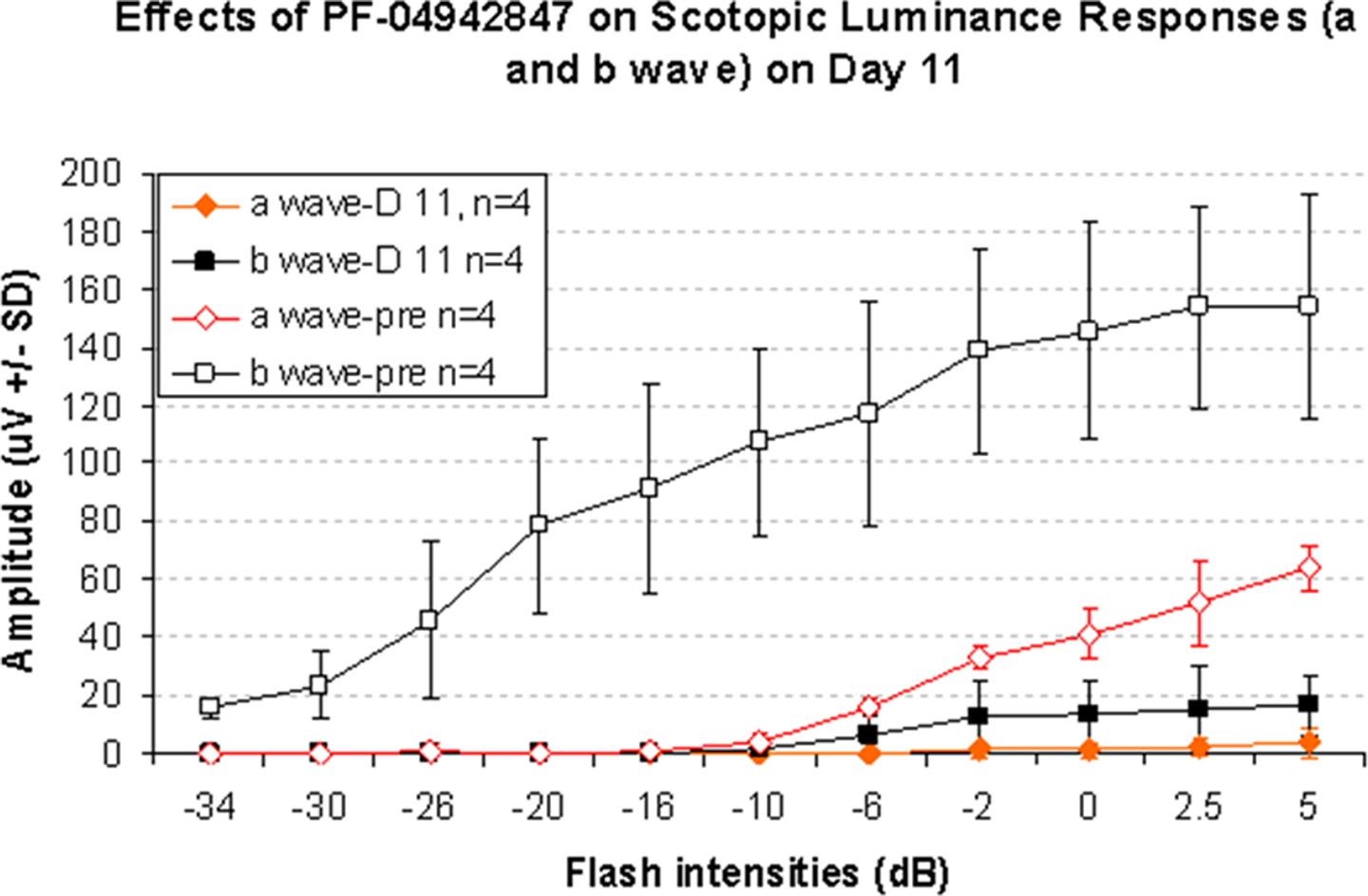
Dark adapted (scotopic) luminance responses following 11 days of PF847 administration.
These results clearly indicated that ERG assessment was sufficiently sensitive to measure perturbations in retinal function as a result of PF847 administration at doses sufficient to cause a histopathological effect. The detection of significant changes as early as 4 days is potentially useful for clinical monitoring. Although progressively more severe changes are observed at 11 days in this study, the fact that earlier detection was possible suggests functional changes in the retina early in the dosing regimen. Theoretically, retinal function can be used to predict the onset of more serious structural damage to the retina, specifically photoreceptor loss. Before this could be considered clinically useful, more definitive studies would need to be performed to address the timing of the functional changes and how these relate to discrete events resulting in damage to retinal tissue with an essential focus being structural changes to the photoreceptor layer.
Ultimately the decision was made to terminate the development of PF847, with the detection of ocular toxicity in the preclinical toxicology studies weighing heavily into that decision. The risk of loss of eyesight presents formidable physical and psychological challenges and is considered unacceptable by many patients, oncologists, and sponsors. Gross photoreceptor loss could be reasonably expected to result in an additional burden to patients and caregivers by limiting the patient’s ability to care for oneself.
Although a potentially useful clinical monitoring assay was identified in the ERG monitoring protocol, the ERG results also underscored the significance of the ocular toxicity. It was unclear that the desired efficacious doses can be achieved while safely managing the ocular toxicity caused by PF847 administration. The detection of toxicity at 4 days suggests that presumably after some accumulation of the drug or metabolites in the retinal tissue, the effects of HSP90 inhibition are relatively acute, limiting the potential dosing duration. It is possible that alternate, perhaps less frequent, dosing regimens may provide a better toxicity to efficacy ratio. Other molecules may have a more favorable therapeutic index depending on their individual chemical properties. For PF847, however, the toxicity appeared to closely follow projected efficacious doses and a daily or twice weekly dosing regimen was strongly desired to provide sufficient dosing flexibility in the clinic.
Additional considerations that impacted the development of this drug include the regulatory risk associated with ocular toxicity. Because oncology drug products are used to treat life-threatening cancers, a certain degree of toxicity can be acceptable as long as the benefit, usually considered an increase in life expectancy, outweighs the risk. Despite this relatively risk-tolerant approach to oncology drug development, ocular toxicity is a signal of concern. Of particular concern is the irreversible nature of photoreceptor loss and the relative steep dose–response curve of the ocular toxicity. In this case, the ability to monitor PF847 needs additional characterization and as of this writing the mechanism is not fully understood. Furthermore, even if these issues were addressed, there would likely be labeling implications for the drug that would last the life of the product, through development and marketing. Although potentially a manageable risk, the concern is that the therapeutic would appear to represent an unnecessary risk in a competitive market.
For the reasons stated above, PF847 was removed from the drug development track. Ocular toxicity, while not the only concern, was a prominent concern in this case with adverse clinical implications for patient’s quality of life and disease management even in the dire case of late-stage terminal cancer treatment. 99
Clinical and Nonclinical Correlates of Ocular Toxicity: Evaluation and Regulatory Considerations
This section of the review explores the relationship between ocular findings in nonclinical studies and the occurrence or lack of occurrence of those findings in the clinical setting. The following scenarios are presented:
Drugs that showed findings in both the nonclinical and the clinical settings.
Drugs that showed findings only in clinical or in nonclinical settings.
Drugs for which the development program was terminated based on the nonclinical findings.
Although several of the drugs described below also produced nonocular toxicities that were taken into consideration in the assessment of benefit/risk, the focus of the review was on the ocular findings. The information presented for all drugs was obtained primarily from public information (www.accessdata.fda.gov/scripts/cder/Drugsatfda).
There are some recognized class effects that generally, although not always, show good correlation between animals and humans. Corticosteroids, for example, are known to induce the formation of cataracts and increase IOP in both animals and humans.100–102 Increased IOP may lead to the onset or worsening of glaucoma. The anticholinergics and adrenergics may cause mydriasis in animals and in humans that could potentially lead to increased IOP in susceptible individuals.103–106 For these 3 classes of drugs, the ocular effects may be observed after systemic or topical ocular administration. The prostaglandin F2-α analogs are well known to cause iris pigmentation in both monkeys and humans after chronic topical administration to the eye. 107
Voriconazole is a triazole antifungal agent with recommended treatment duration of at least 7 to 14 days. In rats and dogs, there was no ocular toxicity in chronic systemic toxicity studies. With longer treatment in the 2-year rat carcinogenicity study, however, there was a slight reduction in the thickness of the ONL of the retina in females at a dose that was ≤2-fold the human dose. Overall, the animal studies did not show strong evidence for potential adverse effects in the eyes. Clinical studies showed abnormal vision, color vision change, and/or photophobia. These findings were generally mild and rarely resulted in discontinuation of treatment. A 28-day study of retinal function in healthy patients showed reversible decreases in waveform amplitude in the ERG and visual field and alteration in color perception. Given the findings in humans and the lack of findings by ophthalmology and histopathology evaluations in animals, a follow-up study was conducted in dogs to look at ERG changes to further explore the effects of voriconazole in the retina. This study showed ERG changes consistent with those reported in the clinic and at plasma levels similar to those of affected humans.
Given that voriconazole demonstrated significant benefit in the treatment of invasive aspergillosis, a condition that has high morbidity and mortality, it was decided that the benefit of the drug outweighed the risks. The drug was approved with the ocular findings acknowledged in the label. In addition, the label recommends ocular monitoring if the drug is used beyond 28 days, since reversibility for ocular effects with longer treatment duration was unknown. In subsequent postmarketing reports, optic neuritis and papilledema were observed with treatment duration of ≥28 days but given the significant benefit of the drug product in treating invasive aspergillosis, the decision was to keep the drug on the market and acknowledge the postmarketing findings in the label.
Voriconazole therefore provides a good example where ERG evaluation offered a good correlation to the toxicity findings in humans, whereas no effects were observed by ophthalmology and histopathology in animals (under the conditions used in the study) to prompt a clinical concern.
Vigabatrin is a γ-aminobutyric acid transaminase inhibitor approved for refractory complex partial seizures in adults who have inadequately responded to several alternative treatments and infantile spasm in children aged 1 to 2 years. In animal models, vigabatrin produced retinal degeneration in albino rats of both sexes and albino female mice at doses less than or equal to the human dose. These lesions were described as focal, multifocal, or occasionally diffuse disorganization of the ONL, with displacement of the nuclei into the rods (rats) or as mild focal loss of rods and rod nuclei from outer retinal layers (mice). In another rat study, the lesions were described as loss of the rod and cone layer and disorganization of the ONL. A similar effect was not observed in chronic studies in pigmented rats, dogs, or monkeys. Due to the lack of histologic effects in pigmented animals, the retinal findings were attributed to vigabatrin exacerbation of light-induced retinal toxicity in the “overly sensitive” albino retina. Although no concern for such ocular effects emerged from the clinical trials conducted in the United States, renewed interest in the retinal findings in rodent resulted from reports to the European Medicine Agency (EMA) of visual field defects, sometimes severe. In response, the sponsor reevaluated the original eye tissue sections from previously completed animal studies (confirming a lack of adverse effects) and conducted investigational studies to further assess the mechanism of the retinal toxicity.
Although the efforts were still ongoing during the regulatory review to clarify the mechanism of the retinal toxicity, given the severity of the indication and the lack of other therapies in the case of infantile spasm, it was determined that the benefit justified the risks. The drug was approved with a black box warning in the label. Because of the risk of permanent vision loss, vigabatrin is available only through a special restricted distribution program. Periodic vision monitoring is required for all patients treated with vigabatrin.
Vigabatrin is an example where nonclinical studies predicted clinical adverse effects, and interestingly, the albino animal species predicted clinical outcome. However, the data were unclear as to whether there was any relationship in the mechanism of retinal toxicity between the nonpigmented (albino rat) and the pigmented eye (human).
Sildenafil is a phophodiesterase type 5 (PDE5) inhibitor indicated for male impotence. Sildenafil can also inhibit PDE6, although with a 10-fold lower selectivity compared to PDE5. PDE6 is involved in phototransduction in the retina. Knowledge of this pharmacological activity prompted the sponsor to study the effects of sildenafil on the retina. Slowing of the repolarization to blue light challenge was observed in vitro in the dog retina, and increased ERG a- and b-wave implicit time was observed in vivo in dogs. Inhibition of pupillary reflex was observed in a 14-day intravenous study in dogs at ≥3-fold the human dose. However, this was not observed with 4 weeks of treatment at a similar dose. No ocular effects were reported after chronic dosing in rats (albino) or dogs, although conjunctival redness was observed in dogs at a dose 3-fold the human dose. The redness was attributed to the vasodilatory properties of sildenafil. In the clinical trials, temporary changes in color vision were observed (ie, difficulty in telling the difference between blue and green objects or objects that appear to have a blue-colored tinge). The ERG clinical assessment showed a reduction in the amplitude of the response to blue and orange light, consistent with the findings observed in dogs. Given that the findings were mild and transient, the decision was to approve the drug with the ocular findings acknowledged in the label. Sildenafil provides an example where knowledge of secondary target expression and function in the eye helped design studies to investigate a potential effect. The affinity for PDE6 is thought to be the basis for the abnormalities related to color vision in the clinic.
Linezolid is an oxazolidinone antibiotic indicated for the treatment of serious infections caused by gram-positive bacteria, including some vancomycin- and methicillin-resistant strains. The recommended treatment duration ranges from 10 to 28 days. Based on ophthalmology or histopathology evaluations, no ocular findings were apparent in animal studies of up to 3-month duration in rats (albino) and dogs. However, in postapproval reports, optic neuropathy was observed primarily in patients treated for longer than the maximum recommended duration of 28 days. A 6-month follow-up study in rats showed optic neuropathy in 2 males. A direct relationship to treatment was equivocal because of the acute nature of the finding, asymmetrical distribution, and comparability to spontaneous unilateral optic nerve degeneration reported in aging rats. Given the efficacy and indication, the original label was revisited, and the clinical and nonclinical findings were acknowledged in the label. In addition, the label includes recommendations for prompt ophthalmic evaluations if vision is affected and monitoring if the treatment duration is 3 months or longer and in all patients reporting new visual symptoms regardless of the length of therapy.
Other examples of therapeutics that resulted in ocular effects in patients that were not observed in nonclinical studies included:
Tamsulosin HCl—intraoperative floppy iris syndrome has been a complication observed in patients that undergo cataract surgery.
Denileukin diftitox—loss of VA and color vision has been observed in humans.
Ciclesonide—cataract development has been observed in humans, which is an expected class effect.
In these 3 cases, no adverse ocular findings were observed in the nonclinical studies. In all cases, the clinical benefits of the drug products were considered to outweigh the risks, and the decision was to acknowledge the findings in the label with appropriate precautions. For denileukin diftitox, the label contains a black box warning for potential loss of VA and color vision.
Aripiprazole, a 5HT1A/D2 receptor partial agonist and 5HT2A receptor antagonist, is indicated for bipolar disorder and schizophrenia. Retinal degeneration was observed in the albino rat in 6-month toxicity and 2-year carcinogenicity studies at doses 14- and 7-fold greater, respectively, than the human exposure at the maximum recommended human dose (MRHD). No ocular findings were reported in toxicology studies in monkeys with dosing up to 1 year or in a mouse (albino) carcinogenicity study. The sponsor attributed the finding to the drug exacerbating a light-induced retinopathy. In clinical trials, blurred vision was observed. However, no other major ocular pathology was identified to indicate an effect on the retina. Given the indication and the lack of identification of any major ocular pathology in the clinic, the drug was approved. The blurred vision observed in humans and the rat findings were acknowledged in the label. As a postapproval commitment, studies focusing on the reversibility and mechanism of retinal degeneration in rats were requested. If light induced, the finding would be considered of minimal relevance to humans.
Verapamil, indicated for angina, arrhythmias, and essential hypertension, showed lenticular and/or suture line changes in beagle dogs at 2- to 4-fold greater than the human dose and frank cataracts at 7- to 14-fold higher than the human dose. No findings were observed in rats. However, cataracts have not been reported in man in the ∼30 years since approval.
In the following examples, development of 3 drugs was terminated because of severe ocular toxicity at exposures similar to that expected or observed in humans or a no-observed adverse effect level (NOAEL) was not identified.
In the first case, drug A, irreversible findings were observed and consisted of white spots in the vitreous of albino rats and fundus hemorrhage in dogs after chronic dosing. The safety margin on the human dose was low, that is, 1- to 4-fold the MRHD. For drug B, hypertrophy and sloughing of the RPE were observed after 3 months in albino rats (irreversible and severe) at exposures overlapping humans and after 28 days of administration in dogs (minimal). For the third case, drug C, cataracts or associated lenticular findings were present at all dose levels within 6 months of treatment in dogs. The lowest dose of drug C assessed in dogs was 30-fold the human dose. The sponsor was asked to provide evidence that the finding can be avoided or is unlikely to occur in humans (eg, determination of a NOAEL). However, the application was withdrawn.
In summary, the examples presented showed that in certain cases animals can predict clinical findings. In other cases, animal data did not predict clinical outcomes. Many factors can contribute to the ability of animals to predict clinical outcome, and these include differences in target expression responsible for exaggerated pharmacology as well as targets responsible for toxicity. In addition, differences in pharmacokinetics may explain the lack of nonclinical and clinical correlation, since there may be differences in the amount of drug and/or active metabolite that reach the eye as well as the period of time the drug is retained in the eye, particularly if the drug binds to melanin. Differences in anatomy or physiology may potentially lead to a lack of nonclinical and clinical correlations. For example, a higher sensitivity to light-induced damage is seen in the albino rat retina, toxicity observed in the retina may be secondary to toxicity in the tapetum of dogs, and smaller vitreal volume and decreased retinal vascularity observed in the rabbit may lead to an increased susceptibility for adverse effects after intravitreal injections, and so forth. In other cases, the finding may not be feasibly detected in animals (eg, blurred vision). These and other factors highlight the importance of careful consideration of species selection to ensure the species will be adequate to identify risks relevant to humans.
In addition to species selection, the examples presented highlight the importance of careful consideration of the battery of testing. For both voriconazole and sildenafil, ophthalmoscopy and histopathology evaluations in animals showed no adverse effects under the conditions of the studies. In these examples, ERG evaluation was found to be a more sensitive parameter to predict clinical outcome. Knowledge of ocular expression and function of a target is also an asset to help design proper studies to investigate a potential effect, as was the case with sildenafil.
Together, well-designed and thoroughly planned nonclinical and clinical studies contribute to maximize the potential to identify risks. When adverse nonclinical findings occur, the decision to continue development depends on the potential risk and the ability to manage that risk in the clinic. When risk is identified or confirmed in clinical studies, a benefit to risk ratio assessment drives further drug development decisions. It should also be realized that the assessment of risk improves as more individuals receive the drug product, and usually, the full risk profile is not completely known until after the drug is marketed.
Summary and Conclusions
The English proverb, “the eyes are the window to your soul”, captures the unique structure and function of the eye. Its transparent nature enables relatively easy, noninvasive examination of the tissues (eg, blood vessels and nervous system) not normally accessible from outside the body. Although not critical to life, its function of capturing and processing images of the external world is clearly critical to the quality of life. Therefore, disruption of the ocular structures or processing of visual images can be a devastating outcome to healthy individuals and to patients being treated with pharmaceuticals.
In drug development, the toxicologist and pathologist, along with the aid of specialists like veterinary ophthalmologists, are charged with careful and thorough evaluation of experimental animals, and data to ensure that drug administration does not represent an unacceptable risk to patients. With improvements in technology, noninvasive methods are being developed and used for detecting early changes in ocular structures and function. Although these technologies can clearly help the toxicologist understand onset, reversibility, and translatability, they must still be used in conjunction with complete and robust histopathological end points. Early screening of compounds for potential ocular toxicity with the use of in silico models as well as in vitro methods with ocular cells was not discussed here but continues to receive significant attention.3,108 Although in silico models have proved useful for the prediction of varying toxicological end points (eg, genotoxicity and carcinogenicity), the use of these models for the prediction of ocular toxicity has been limited due to the lack of complete validation against in vivo outcomes. Improvements in this technology are continuing.
In vitro tissue assessments for ocular effects have been particularly valuable for early screening and also for mechanistic-based research into drug toxicity. The use of lens and corneal tissue cell systems for assessing cataract or opacity potential of pharmaceuticals has shown great promise as drug screening methods. Mecklenburg and Schraemeyer 91 provided a good overview of the use of RPE cell systems as a means for examining the mechanism of ocular toxicity of xenobiotics. These in vitro/in silico systems are considered to represent a future of early screening for ocular toxicity of xenobiotics. However, these methods are not easily developed within laboratories, and the translation of the results to human medicine is still problematic.
In clinical practice, the ophthalmologist has several “tools” to evaluate the structure and function of the eye of a patient including VA tests, imaging, direct examination, and so forth. Since some of these clinical tests rely on verbal instructions from the ophthalmologist or verbal response from a patient, they are obviously of no practical use in a nonclinical setting. However, the ability to use the same or similar test in the clinic and in nonclinical test species has the advantage of improving our ability to predict the translation of an ocular safety risk to patients. Methods of clinical importance have been introduced that have shown great promise in a nonclinical setting including ERG and OCT imaging. Yehoshua et al 109 and Bearelly et al 110 reported the use of OCT imaging for the evaluation of geographic atrophy associated with age-related macular degeneration. These investigators showed very detailed morphological changes with imaging that was previously not always possible in patients. As described above, this method has proven to be a very useful tool in nonclinical studies, particularly with nonhuman primates. Although the resolution of the scans does not allow a detailed description at the cellular level, this noninvasive technique provides an opportunity to examine the same animal over the duration of a nonclinical study for the evaluation of changes at the supracellular level. Moreover, these clinically useful tools permit a “structure–function” evaluation in the animal that can be potentially directly translatable to patient safety. Similarly, other clinical tools continue to show promise and use within the nonclinical laboratory (ERG and VEP) with the results also considered to be predictive of human outcomes. Despite these advances, there remains a critical need for more research and development of preclinical and clinical biomarkers for ocular toxicity.
In spite of these technological advances in noninvasive methods, histopathological evaluation currently continues to be, from a regulatory perspective, a more definitive determinant of ocular toxicity with recognition that not all histopathological findings are predictive in humans (eg, tepetum in dogs). In addition, some animals have a higher background incidence of ocular lesions (eg, light-induced ocular degeneration in albino rats) that must be considered in determining risk to patients.111,112
With greater understanding of nonclinical results using the methods described here, the risk of adverse ocular outcomes in patients can be better managed because of the increase in scientific understanding and also because of the direct translation of the results to patient safety. Since drug development is a resource-intensive enterprise, sponsors are often times reluctant to terminate a drug development program, particularly if the drug in development is the only “asset.” Therefore, further development proceeds “at risk” for regulatory scrutiny or adverse clinical outcomes that ultimately lead to drug development termination. In all, the toxicologist in collaboration with the pathologist, ophthalmologist, and other principle scientists play a key role in evaluating the nonclinical data toward recommending drug development progression or termination.
Footnotes
Acknowledgments
The authors (VT, CJS) wish to acknowledge Chang-Ning Liu (electroretinography), Kate Muravnick (retinal histopathology), and John Marcek and Ted Schmahai (toxicology studies) for their expertise and technical assistance with the conduct of the PF847 studies.
Authors’ Note
The opinions of the author (MIR) expressed in this manuscript do not necessarily reflect the views or policies of the US Food and Drug Administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.