
Abstract
Although researchers have studied dyslexia for over a century, there is still much debate about how dyslexia differs from other reading difficulties and how to support students labeled dyslexic. Nevertheless, dyslexia policy and practice are steeped in authoritative discourse that speaks of a definitive definition, unique characteristics, and prescribed intervention programs that are not well supported by research. In Texas, and increasingly in other states, only educators trained in these programs are considered qualified to provide intervention for students identified as dyslexic. In contrast to earlier research, which found that the word dyslexia decreased teachers’ confidence and feelings of self-efficacy, the dyslexia interventionists we interviewed expressed a high degree of confidence and certainty about dyslexia and the interventions they used. Bakhtin’s notion of authoritative and internally persuasive discourse helped us think about the reasons for these findings and how to initiate a broader and more inclusive conversation about dyslexia.
Recently, there has been a vast increase in attention to dyslexia in policy, practice, and the media. Although researchers have studied dyslexia for over a century, there is still much debate about how it differs from other reading difficulties and how to support students identified as dyslexic. Some children struggle to decode print, which is the central issue in what is termed dyslexia. However, researchers have failed to consistently identify characteristics or patterns of reading that distinguish dyslexia from other decoding difficulties (Elliott & Grigorenko, 2014; Vellutino, Fletcher, Snowling, & Scanlon, 2004). Some academics question whether the term is useful as it is not clearly defined and does not provide clear guidance for instruction (Elliott & Grigorenko, 2014; Scanlon, 2016; Stanovich, 1994). Nevertheless, the current discourse of dyslexia that saturates policy and practice speaks of a unique set of characteristics and a specific form of intervention (Worthy et al., 2017).
In 1985, Texas passed the nation’s first dyslexia legislation, requiring screening and treatment. More recent laws concern instructional accommodations, technology integration, and educator preparation. The Dyslexia Handbook, originally written in 1986 and updated multiple times, provides guidelines for school districts regarding identification and instructional services that are aligned with the Texas Education Code and Texas Administrative Code (Texas Education Agency [TEA], 2014). The Dyslexia Handbook also specifies licensing regulations for dyslexia “practitioners” and “therapists” (p. 47) and requirements for “training” of K-12 educators in “the components and delivery of dyslexia instruction” (p. 39). Many states have followed Texas’s lead; as of March 2018, 41 additional states had dyslexia-specific laws (Youman & Mather, 2018).
Part of the definition of dyslexia in Texas law, and in 14 additional states, is that “it should be unexpected in relation to the student’s other cognitive abilities” (TEA, 2014, p. 67). This language explicitly separates students identified as dyslexic from other students with reading difficulties. This separation is also evident in state policies that govern who is qualified to provide intervention for dyslexia and what type of instruction is sanctioned. In a study of Texas elementary educators, Worthy and colleagues (2016) noted distinct differences in the ways dyslexia interventionists—educators with training in dyslexia-specific programs—and classroom teachers talked about dyslexia. For example, although most of the classroom teachers felt confident in providing instruction for students with reading difficulties, the label dyslexia negatively affected their confidence. In contrast, the dyslexia interventionists spoke assuredly about the definition and characteristics of dyslexia and the effectiveness of dyslexia intervention programs.
These emergent findings and the limited number of interventionists among the participants led to the current study. We examined the following question: What are the perspectives, understandings, and experiences of dyslexia interventionists?
Theoretical Framework
We used Bakhtin’s (1981) notion of “authoritative discourse” as a theoretical frame for this research. As humans develop their worldviews (what Bakhtin calls “ideological becoming”), they encounter various points of view, expressed as sometimes-competing discourses. One kind, internally persuasive discourse, is grounded in multiple perspectives, exploration of ideas, and negotiation of meaning. Internally persuasive discourse is characterized by questioning rather than certainty (Bakhtin, 1981). Here we focus on authoritative discourse (AD), which has a single, static, inflexible meaning and “demands our unconditional allegiance” (p. 343). Because AD is not open to questioning or change, it limits possibilities for multiple perspectives.
Matusov and von Duyke (2009) illustrated the impact of AD in their analysis of an online discussion among teacher candidates. The candidates were responding to a classroom dilemma—what to do about students’ “foul language” in school (p. 175). Early in the discussion, some participants responded with “a clichéd authoritative discourse” (p. 176), invoking traditional “social taboos” that frown on cursing in school (p. 182). They used “language walls,” a form of AD, that blocked discussion (Matusov & von Duyke, 2009, p. 183). For example, one participant wrote that using foul language “is obviously inappropriate” (p. 182), leading some of the participants to accept the point being made and refrain from challenging it.
AD is common in discussions surrounding learning differences. In special education, learning differences are commonly framed as intrinsic disorders (Connor, 2014; Reid & Valle, 2004). This perspective reflects medical terminology describing the identification and instruction of students with learning disabilities (LDs)—including diagnosis, symptoms, and treatment—and in the characterization of LD as having a neurological origin. Such authoritative language can silence and intimidate families and educators, leading them to defer to people who bill themselves as experts (Baglieri, Valle, Connor, & Gallagher, 2011; Bishop, 2013). These perspectives and terminology also apply to dyslexia discourse.
Morson (2004) asserted, “The basic power of an authoritative voice comes from its status as the one that everyone hears” (p. 320). In Texas, and increasingly in the rest of the United States, that voice includes a set of “generally acknowledged truths” (Bakhtin, 1981, p. 344) about dyslexia (Worthy et al., 2017). These ideas and language are recirculated in legislation and policy, through dyslexia advocacy organizations (e.g., the International Dyslexia Association [IDA]) and the media, and are rarely questioned. Other examples of dyslexia discourse, common in popular media but unsupported by research, are that 15% to 20% of the population is dyslexic (Vellutino et al., 2004) and that dyslexic individuals are unusually intelligent (Thomas, 2000).
Dyslexia Research and Legislation
Early researchers and educators believed dyslexia resulted from visual deficits characterized by letter and word reversals, which are now known to be common in inexperienced readers. Many researchers now agree that the predominant challenge in dyslexia is accurate and fluent decoding, caused by phonological processing deficits (Bradley & Bryant, 1983; Vellutino et al., 2004). This agreement is reflected in definitions from the IDA and the National Institutes of Health (National Institutes of Neurological Disorders and Strokes, n.d.). The identification of dyslexia, like other LDs, has historically been based on a discrepancy between intelligence (IQ) and achievement (Stanovich, 1994). Although the U.S. Department of Education (n.d.) discourages the use of a discrepancy model in the identification of specific learning disability (SLD), common definitions continue to include the notion of unexpectedness.
These definitions also describe dyslexia as “neurobiological” (IDA, n.d.-a) or “brain-based” (National Institutes of Neurological Disorders and Strokes, n.d.), and studies exploring connections between dyslexia and the brain are plentiful (Barquero, Davis, & Cutting, 2014). Using imaging techniques such as functional magnetic resonance imaging (fMRI), researchers have examined brain structure and activity during reading tasks, as well as differences in the brain after interventions. Such research has contributed to increased understandings of reading and language processes, and there is potential for productive “interdisciplinary conversation” (Hruby & Goswami, 2011, p. 169). However, there are limitations of this research, including differing interventions and methodologies, inconsistencies in participant selection, and small sample sizes (Bishop, 2013; Eklund, Nichols, & Knutsson, 2016; Ramus & Szenkovits, 2008). Furthermore, because participants must remain still during imaging (Varma, McCandliss, & Schwartz, 2008), the reading measures employed are far removed from meaningful reading. The tasks include identification of correctly spelled and misspelled words, discriminating between pseudowords and real words, phoneme–grapheme matching, and phonemic awareness activities (Barquero et al., 2014). Accordingly, many researchers question the practical implications of imaging research, cautioning that findings should be considered exploratory (Barquero et al., 2014; Hruby & Goswami, 2011; Richlan, Kronbichler, & Wimmer, 2009).
For decades, researchers have searched for distinctions between learners identified as dyslexic and other students with reading difficulties. In research comparing the spelling and reading of these two groups of students and “normally achieving” students matched for achievement level, researchers have not been able to consistently identify “idiosyncratic processes” or signature patterns in reading, spelling, brain structure, or brain function unique to dyslexia (Cassar, Treiman, Moats, Pollo, & Kessler, 2005; Ramus & Szenkovits, 2008; Tanaka et al., 2011). In fact, a diagnosis of dyslexia, like one of other LDs, depends on the assessment measures used and their interpretation, which can differ by region, by state, and even within districts (Moats & Lyon, 1993; Shaywitz, Morris, & Shaywitz, 2008; Vellutino et al., 2004).
Relatedly, there is wide consensus that dyslexia is “not an all or none phenomenon” (Shaywitz, Escobar, Shaywitz, Fletcher, & Makuch, 1992, p. 149) but that decoding proficiency exists along a continuum, with no clear cutoff point for a dyslexia diagnosis (Shaywitz et al., 1992; Vellutino et al., 2004). Another consensus is that students with decoding difficulties, including those identified as dyslexic, benefit from targeted decoding instruction. However, researchers from a variety of perspectives agree decoding instruction should be only one component of a comprehensive, responsive, meaning-based approach to reading instruction and that there is no best teaching method, including for students identified as dyslexic (International Literacy Association [ILA], 2016; Scanlon, 2016; Scanlon, Anderson, & Sweeney, 2017; Shaywitz et al., 2008). Yet, some sources, including the IDA (n.d.-c) and state guidelines (Youman & Mather, 2013, 2015), assert that only explicit, systematic, decoding-focused reading programs are effective for dyslexia.
Such programs are consistent with the Orton-Gillingham, or OG, approach (Gillingham & Stillman, 2014), which is a “systematic, sequential, multisensory, synthetic and phonics-based approach to teaching reading” (Ritchey & Goeke, 2006, p. 171). In a review of intervention research with OG and OG-based programs, Ritchey and Goeke (2006) found only 10 published studies and two dissertations that met their minimal criteria for sample size and study design. The researchers cautioned that even the studies reporting effectiveness must be viewed with caution because of design and implementation issues, concluding, “Despite widespread use by teachers in a variety of settings for more than five decades, OG instruction has yet to be comprehensively studied and reported in peer-refereed journals” (p. 181). Similar results were found in a review by What Works Clearinghouse (WWC; 2010), which included 31 published reports focusing on OG-based interventions, none of which “met WWC evidence standards with or without reservations” (p. 2). The WWC excluded 25 of those published studies because they were not focused on the effectiveness of an intervention, they did not include a comparison group, or less than half of the participants were identified as learning disabled. Of the remaining six studies, none met the WWC standards for evidence-based research either because of nonequivalent intervention and comparison groups or because “the measures of effectiveness cannot be attributed solely to the intervention” (p. 2). More recent studies have found mixed results or small effect sizes or have had methodological limitations (Hwee & Houghton, 2011; Lim & Oei, 2015). Perhaps as important, reading is a highly complex process; all readers, including those identified as dyslexic or struggling, have varied strengths and challenges (Dennis, 2012), and “teaching them is too complex a task for a scripted, one-size-fits-all program” (ILA, 2016, p. 3).
Our review of research supports Nicholson’s (2016) contention that “confusion lies at the heart of dyslexia research and practice” (p. 67). However, despite the limited research consensus around dyslexia, the number of dyslexia laws in the United States has continued to increase.
Dyslexia Legislation and Policy
The Individuals With Disabilities Education Act of 2004 (Council for Exceptional Children, n.d.) discontinued the use of intelligence tests in the identification of SLD, substituting response to intervention (RTI). However, laws in Texas and in a growing number of states (including Louisiana, Arkansas, Iowa, Washington, and Minnesota) stipulate that students who do not qualify for special education services for SLD can still be evaluated for dyslexia and, if identified, must receive accommodations in accordance with Section 504 (Council for Exceptional Children, n.d.). In Texas, the procedures for identifying dyslexia are separate and more flexible than those for SLD; the RTI process is not required, and teachers and parents may request evaluations if dyslexia is suspected (TEA, 2014). Texas law also requires educational regions or districts to provide a “specialized type of intervention program” (TEA, 2014, p. 14), listing components consistent with language in the IDA’s (n.d.-c) guidelines, including multisensory, systematic, explicit, and sequential, and the Dyslexia Handbook (TEA, 2014) specifically differentiates dyslexia instruction from regular classroom teaching: While the components of instruction for students with dyslexia include good teaching principles, the explicitness and intensity of the instruction, fidelity to program descriptors, grouping formats, and training and skill of the teachers are wholly different from core classroom instruction. (p. 26)
There are also regulations for training and certification of dyslexia interventionists, offered mainly outside university teacher education programs (TEA, n.d.-b). Education courses or degrees and teaching experience are not required. These laws create a marked distinction between how expertise in dyslexia and expertise in reading education are recognized. Yet, in schools, dyslexia interventionists and other educators share the responsibility for teaching students identified as dyslexic.
Teacher Knowledge of Dyslexia
In public discourse, teachers are portrayed as lacking knowledge and preparation in dyslexia, as well as empathy for dyslexic individuals (e.g., Macias, 2013). The IDA explicitly questions the knowledge of public school teachers: “In public school settings where many teachers are not knowledgeable about this condition, students with dyslexia may be considered stupid or lazy” (IDA, n.d.-b, para. 3). Research presents a more nuanced perspective.
Research examining teachers’ knowledge and beliefs about dyslexia has found that participants demonstrated a mix of accurate and inaccurate beliefs. Wadlington and Wadlington (2005) found the educators they surveyed understood correctly that intelligence and home environment are not related to dyslexia, but most identified word reversals as the major hallmark of dyslexia. Similarly, in survey studies of preservice and inservice teachers (Washburn, Binks-Cantrell, & Joshi, 2014; Washburn, Joshi, & Binks-Cantrell, 2011), the majority of participants identified dyslexia as a language-based difficulty affecting decoding and spelling but pinpointed a visual perception deficit as the cause. Washburn and colleagues (2011) also examined novice and experienced teachers’ knowledge of basic language constructs considered important for teaching challenged readers. The teachers’ knowledge was variable, but the researchers concluded that most lacked explicit knowledge of some phonology, phonics, and morphology concepts. From a more recent study, “teachers had accurate understandings when asked about reading disability, but misconceptions when asked about dyslexia” (Washburn, Mulcahy, Musante, & Joshi, 2017, p. 169). From these findings, along with the earlier research, the authors concluded, “It appears that there is confusion among teachers about what dyslexia is and what it is not” (pp. 186-187). These studies highlight a misconception among some educators that letter and word reversals are hallmarks of dyslexia. As the authors point out, this misunderstanding may lead some teachers to rely on vision-based therapies over instruction targeted at decoding issues.
The findings of this body of research also underscore a general confusion among educators about the term dyslexia and how it differs from reading difficulties. Considering the research reviewed, this confusion is understandable because dyslexia has not been clearly defined as distinct from other decoding difficulties. The most recent Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, n.d.) no longer lists dyslexia as a separate category from SLD because “the many definitions of dyslexia and dyscalculia meant those terms would not be useful as disorder names or in the diagnostic criteria” (para. 4). Similarly, literacy educators rarely use the term (Harris & Hodges, 1981) because it “carries with it so many empirically unverified connotations and assumptions” (Stanovich, 1994, p. 579). Thus, it is not surprising that teacher education does not present a uniform set of concepts and information about dyslexia. Further highlighting these issues, Gibbs and Elliott (2015) found the way students were labeled (as having “reading difficulties” or as being “dyslexic”) affected teachers’ feelings of efficacy. They also found the term dyslexia “is more likely to evoke aspects of essentialism than ‘reading difficulties’” among teachers, and that distinguishing between the two groups of readers may “obscure information about the specific strengths and weaknesses of individual group members” (p. 334).
In our earlier study (Worthy et al., 2016), we interviewed elementary classroom teachers, reading specialists, and dyslexia interventionists in Texas about their understandings and experiences of dyslexia practices and policies. As previously noted, the findings illuminated a difference between the two dyslexia interventionists and the other participants in their confidence about their knowledge of and instruction related to dyslexia. Most teachers and reading specialists spoke assuredly about their ability to provide instruction for students with reading difficulties; however, like the teachers in Gibbs and Elliott’s (2015) study, the term dyslexia limited their confidence and efficacy beliefs about their ability to support and motivate students identified as dyslexic. The dyslexia interventionists, in contrast, spoke confidently about their knowledge of dyslexia and their ability to provide intervention for students labeled dyslexic. We conducted the current study to further examine these emergent ideas and the perspectives of dyslexia interventionists. We included the two interventionists from the previous study and solicited additional participants to more deeply explore their perspectives and experiences of dyslexia.
Method
Researchers and Positionality
All the authors are former elementary classroom teachers and current literacy teacher educators and researchers. We have worked with many students with reading difficulties. We take their struggles seriously and believe there are no clear truths or single answers to the complex issues surrounding reading difficulties.
We have observed the recent increased attention to dyslexia, and we share a concern about effects on educational practice. In schools, we have observed that educators trained in dyslexia-specific interventions speak with certainty about dyslexia characteristics, identification, and instruction, while many teachers express limited confidence, because they have not received training that is “institutionally-sanctioned” (Brantlinger, 1997, p. 432).
We see teaching as a complex and dynamic practice that requires continuous learning and inquiry, rather than a technical field where teachers are trained to implement programs (Vaughn & Parsons, 2013). We also believe literacy is too complex to be taught with prescriptive programs that minimize the need for teacher expertise. Accordingly, we argue that effective teachers of literacy draw on a range of approaches and strategies. Understanding language structure and how to teach decoding is essential, but effective literacy instruction goes beyond those components. Teachers must also deeply understand assessment and instruction in comprehension, fluency, vocabulary, and reading–writing connections. In addition, educators need to be familiar with a wide variety of texts and understand how to support students in choosing and reading them, and they need to be responsive to learners’ motivations, languages, and backgrounds.
Participants
We employed purposeful sampling to identify potential participants with experience and knowledge about dyslexia (Rubin & Rubin, 2011). We searched the Central Texas school districts’ online directories to find the names of teachers who were identified as dyslexia interventionists. Next, we searched the online registry of Cognitive Academic Language Therapists published by the Academic Language Therapy Association, a nonprofit national professional organization that certifies dyslexia practitioners and interventionists. Through this process, we identified 20 potential participants and contacted them by email, inviting them to participate in a study titled “Deconstructing Dyslexia” focusing on “the perspectives of elementary educators who work with students identified as dyslexic.”
Including the two participants from our previous educator study, 13 interventionists agreed to participate. They worked in two school districts serving linguistically, racially, and socioeconomically diverse communities, and their experience as interventionists ranged from 4 months to 20 years. All participants were female and had previously served as teachers in general elementary education (four), elementary special education (four), elementary bilingual education (two), and middle or high school (two); one had served as a reading specialist. Five participants had master’s degrees in education-related fields, and two had master’s degrees in fields other than education (English Literature and Counseling). Two were enrolled in a special education master’s degree program with a specialization in dyslexia at a regional university, and the others received their training in dyslexia through private dyslexia training centers in Texas. All dyslexia training programs were accredited by the IDA.
Data Collection
We employed an “intensive interview” approach (Rubin & Rubin, 2011), using the same semistructured interview protocol (see Appendix A in the online supplementary archive) and interview procedures as in the previous study of educators (Worthy et al., 2016). We asked participants about their definitions of dyslexia, personal and professional experiences with dyslexia, perceptions of their own knowledge and confidence about dyslexia, and interventions for dyslexia. Interviews were conducted in person by the second author, audio recorded, and transcribed. The interviewer’s beliefs and opinions were not communicated during the interview. The interviewer sent the transcripts to participants for member checking, asking them to review them and to let us know “if there is anything you would like to add or if you feel something in the transcript does not accurately represent your views or beliefs.” Comments and clarifications were added to transcripts and included in the analysis.
Data Analysis
We began with initial coding, reading and recording first impressions of all the transcripts, followed by more focused analysis (Miles, Huberman, & Saldaña, 2014; Saldaña, 2013). We started systematic analysis by examining participants’ responses to questions about two a priori categories corresponding to questions in the interview protocol: (a) Definition and Characteristics of Dyslexia and (b) Instruction for Dyslexia. Within these categories, we unitized the data into meaningful segments and then sorted them inductively into subcategories.
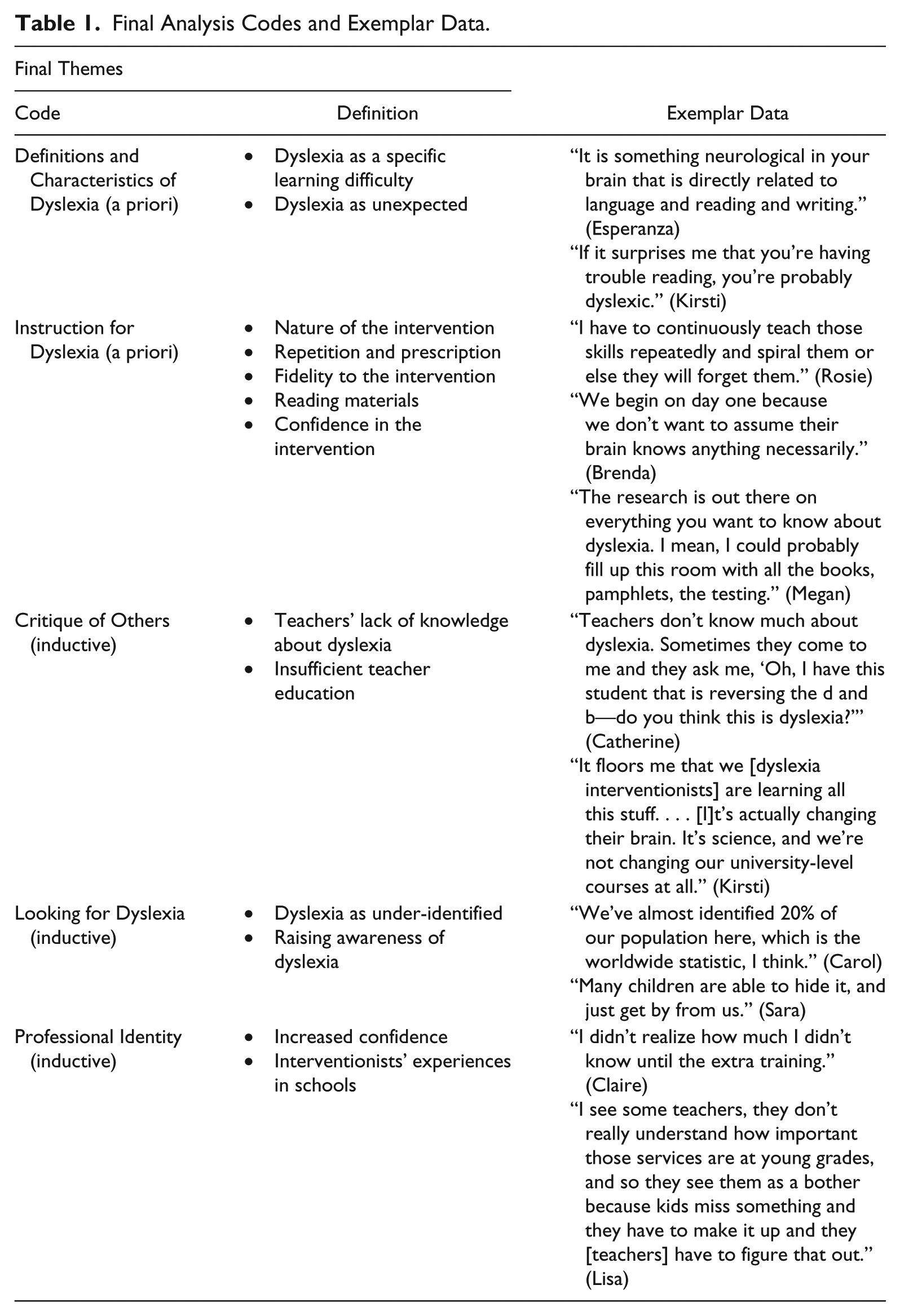
For the remaining data, all researchers inductively analyzed the same three transcripts, writing margin notes about possible categories and patterns. During this process, we each wrote analytic memos that included definitions and descriptions of developing codes, themes, and connections to research and theory, as well as quotes from the transcripts that exemplified themes and represented the range of perspectives (Saldaña, 2013). We shared these in a collaborative online document and in research meetings and continued to negotiate until we agreed on a preliminary set of codes. We then unitized the data into meaningful segments, analyzed the units using the preliminary codes, and combined and refined the codes based on our group discussions. We employed the revised codes to analyze the remaining transcripts. Working from the coded data, we continued looking for ways to collapse the codes into larger categories while writing and sharing analytic memos. After seven rounds of analysis, we reached consensus on three major themes: (a) Critique of Others, (b) Looking for Dyslexia, and (c) Professional Identity. We worked in pairs to identify and describe subcategories within the themes and then returned to the data to recode, refine, and identify examples (see Table 1). After analyzing thematically, we conducted an additional level of analysis employing an AD lens (Bakhtin, 1981), focusing on how responses reflected discourses of dyslexia as well as on how participants expressed their ideas.
Final Analysis Codes and Exemplar Data.
To safeguard the trustworthiness of the study, we kept track of ideas brought up by a small number of participants, as well as negative examples that disconfirmed our emerging hypotheses (Miles et al., 2014; Saldaña, 2013). As an additional means of strengthening credibility, we constructed profiles of each participant and returned to them throughout data analysis to ensure representation of each participant’s major ideas.
Findings
In this section, we present the two a priori themes, followed by the inductive themes, illustrated by participants’ voices. In addition, we highlight examples of institutional discourse, popular discourse, and authoritative language.
Dyslexia Interventionists’ Definitions and Characteristics of Dyslexia
Consistent with research consensus and with the IDA definition, dyslexia interventionists defined dyslexia as an issue with phonological processing and decoding and emphasized that it is not related to vision or letter reversals. Also consistent with the IDA definition, which is included in the Texas Dyslexia Handbook (TEA, 2014), participants defined dyslexia as a neurological issue that is unexpected in relation to other abilities.
Dyslexia as a specific learning difficulty
Dyslexia was described by 12 of the 13 participants as a deficit in phonological processing that primarily affects decoding, spelling, and fluency and that can affect other reading processes. Megan (all names are pseudonyms) explained how she knows when a student should be tested for dyslexia: We are looking for that grapheme/phoneme awareness, the understanding that most kids have by the end of kindergarten that this letter goes with this sound. And when that is missing that is a big red flag. When kids are avoiding reading, that is a big red flag. Processing speed, to be able to rapidly name the letters of the alphabet, is another red flag.
Nine participants said dyslexia is caused by a neurological issue. According to Esperanza, dyslexia is “something neurological in your brain that is directly related to language and reading and writing.” Megan asserted dyslexia is a unique form of reading disability: “It is a disability in reading, but it is a very specific one where we have isolated what exactly is breaking down in the three different loops that are involved in it in the brain.” Megan’s description of finding “exactly” the cause of dyslexia in the brain is an example of a language wall, a type of AD that limits inquiry and exploration around other possible explanations (Matusov & von Duyke, 2009).
Dyslexia as unexpected
A commonly mentioned characteristic of dyslexia was its unexpectedness in relation to other abilities. According to Lisa, It’s about a kiddo who is generally doing well and seems to understand what you’re saying to them . . . but then they can’t learn to read or they can’t learn to decode and sound out words.
Kirsti affirmed the unexpectedness, saying dyslexic students are “smart” and “articulate”: “If it surprises me that you’re having trouble reading, you’re probably dyslexic.” Consistent with the unexpectedness, 10 interventionists said intelligence is an important part of the identification of dyslexia and a characteristic that distinguishes it from other reading difficulties. Several mentioned the use of IQ tests in dyslexia identification, even though researchers have noted the limited connection between intelligence and decoding (Siegel, 1992). Rosie noted, “The IQ does let you know if they are average or above average in intelligence.” Furthermore, she explained, Typically, when you look at a student who did not qualify, it was because they were below average on the IQ. That lets you know that you need to go another route in testing, which is more testing for another learning disability.
Megan asserted that an average to above average IQ was necessary for students to make progress in the dyslexia intervention: “By definition they’re not going to benefit from the intervention unless they have the cognitive ability to benefit.” The phrase “by definition” acts as a language wall that restricts how these ideas might be expanded or questioned (Matusov & von Duyke, 2009).
Consistent with popular notions of dyslexia, several participants described students with dyslexia as having special traits, such as being creative, “out-of-the-box thinkers” (Kathy). Claire said, “People who are dyslexic are often people like Einstein. People who’ve done a lot to change our world.” According to Esperanza, “A lot of successful entrepreneurs and professionals are dyslexic.” These ideas are related to the notion of intelligence but are not supported by research.
Instruction for Dyslexia
According to interventionists, once a student is diagnosed with dyslexia, the district is required to provide intensive intervention 4 or 5 days per week for 45 min. In the districts where our participants worked, intervention was provided in small group pull-out sessions.
Nature of the intervention
Participants said the programs they use are derived from OG and conform to the description of “multisensory, systematic, sequential, explicit” interventions in the Texas Dyslexia Handbook (TEA, 2014). Esperanza described the multisensory component: I’m talking about moveable letters to make a word. I’m talking about tapping the sounds for spelling and reading for the words. I might be teaching them how to visualize a word, read the word, cover the word, write it on the table, use your fingers, use sand.
Repetition and prescription were also cited as common features across all programs, and participants emphasized the importance of these components.
Repetition and prescription
Participants said the intervention is dependent on systematic repetition of skills. Rosie explained, “I have to continuously teach those skills repeatedly and spiral them or else they will forget them.” Referring to the program used in her district, and employing language consistent with AD (“has to be,” and “exactly”), Kirsti said, Take Flight© (The Written Word: Center for Dyslexia and Learning, 2018) is very prescribed. In fact, a lot of times I stop and go back and read to make sure I said exactly everything. It has to be done exactly the same way, exactly the same verbiage. We’ve had to memorize this chart. I mean, we can do it in our sleep. It has this whole long thing and it has to be said exactly the same way. That is part of the power of it, the repetition.
Catherine added that doing the same routine every day “helps the dyslexic student to be more organized in their thoughts and minds.” Brenda provided a detailed example of how repetition works within a lesson: So, the therapeutic aspect of that is when you are saying there is no /l/ [in a word], try again, try again, try again. Okay let’s get a mirror, let’s look at where the /l/ is in your mouth. They look, they say it, they blend it, they name the letters, they write it. So, it’s sort of taking it down to the smallest little bit, and it’s done over and over and over again, until the brain begins to change.
Brenda’s assertion that dyslexia interventions can change the brain was couched in certainty, consistent with AD: My experience is in about three months, do this every single day, the brain begins to change and retain this information. I tell the teachers it takes about three months before you begin seeing change, but it is a permanent change.
Similarly, Megan invoked the authority of research when she said, “We’re looking at all these MRIs with dyslexic students before and after interventions and it’s actually changing their brain.” Although descriptions of “changes in the brain” in RTI are not commonly found in dyslexia legislation and policy, this is a common theme in popular media (Emanuel, 2016), and participants described it as part of their training.
Fidelity to the intervention
Participants stressed the importance of strictly following the scripted program and starting at the beginning with all students. Brenda explained, We begin on day one because we don’t want to assume their brain knows anything necessarily. . . You’re starting with the most foundational aspects of English, so you don’t want to go to anything harder without knowing they have that foundation.
Referring to the OG-based program she uses, Kathy also stressed that starting at the beginning is important because each skill builds on the previous one: “I use the Take Flight program, which kind of assumes that we don’t take anything for granted. All kids start at lesson one and learn the multisensory approach.”
Although participants noted that fidelity to the intervention programs is important, in practice, many found it difficult to conform to all program requirements. Claire said the program her district uses is designed for 1-hr sessions, but constraints of the school schedule made it practically impossible to address all the components: “Scheduling wise, we don’t always have that full hour. And sometimes it really takes longer than an hour if you’re going to really cover it.” She noted comprehension, vocabulary, and writing are the components that she typically skipped.
Although all participants used dyslexia-specific interventions, and all started students at the beginning of the programs, some participants talked about possibilities for instructional flexibility. Although Carol uses her district’s program with fidelity, she said she would prefer to use a mix of dyslexia programs: “I think you can take a little of both, honestly, and use what works.” Claire said she supplements with other phonics programs according to “what fits with what kid.” Similarly, Grace said she mostly follows one program but sometimes pulls words or sentences from other OG-based programs.
Although Angela and Esperanza also used OG-based programs as the core of their instruction, they occasionally added other instructional components. Angela said she tries to include a read aloud, which is not a regular component of the intervention program. After describing what she does in a typical session, Angela said, “And then we do a read aloud. . . It usually only happens on Friday.” Finding time for a read aloud was not always possible because there were so many program components she was required to address. Only Esperanza mentioned giving students opportunities to read books: I had a first grader recently, and it took a while to break the code. Then all of a sudden, things started flowing, and then she wanted to read about a certain author, a certain type of book. I went and got her everything I could find on that author, or a series.
Although a few other participants mentioned that students read texts as part of their instruction, they were limited to decodable materials provided by the intervention programs. Catherine said her district’s program includes “one-page readers,” and that the students are “excited because it’s the only thing they get to read.”
Confidence in the intervention
Using language consistent with AD, interventionists expressed certainty about the research and information on dyslexia they had heard, read, or been explicitly taught in their dyslexia training courses. Grace said, “The research is out there on everything you want to know about dyslexia. I mean, I could probably fill up this room with all the books, pamphlets, the testing.” Megan asserted, “We know what it is, we know the neurobiology of it, we know what works to fix it,” and Esperanza commented, “Each situation is unique, but the dyslexic student, you know for a fact that it is a processing issue that requires building those connections.” Similarly, Kirsti said, “As long as I stick to this [program], I know this works and I know if I make sure to say everything it says to say, then it will all turn out good.”
During the interviews, almost every dyslexia interventionist shared a success story of a student who made a substantial amount of growth, which they attributed to the intervention program. When students did not make progress, extenuating circumstances were cited as the reason for the lack of progress rather than the intervention program. Kirsti shared a story of a student whose progress was not what she had hoped for: “It broke my heart that he didn’t make more progress, but he just, he was dyslexic, he was ESL [English as a second language], he didn’t have home support.”
Critique of Others
Dyslexia interventionists spoke critically of others’ knowledge and actions, including classroom teachers on their campuses. They also criticized teacher educators and the university preparation teachers receive.
Teachers’ lack of knowledge about dyslexia
Ten participants explicitly said teachers were not knowledgeable about dyslexia or prepared to meet the needs of their students identified as dyslexic. Angela said, “I don’t know if teachers even believe it. They don’t even know what it is, really.” She felt teachers needed more information and should attend trainings to learn about dyslexia. She recounted how teachers wanted her to serve their students, but then they refused to attend additional dyslexia trainings: “I know they want their kids getting served by me, but I will say that not really any teachers, very few, only two I know, have been to any extra training.” Catherine asserted that “teachers don’t know much about dyslexia. Sometimes they come to me and they ask me, ‘Oh, I have this student that is reversing the d and b—do you think this is dyslexia?’” Nine of the interventionists were also critical of classroom instruction for students identified as dyslexic. For example, Kirsti spoke of teachers on her campus who taught students letter sounds “incorrectly”: I hear some teachers. . . say, “The sound /w/ says /wuh/,” and I’m like, “no.” And I’m not going to say anything. But, we’re not helping if we’re teaching them the wrong thing.
Insufficient teacher education
Eight participants criticized teacher preparation, blaming teacher educators for what they saw as limited knowledge and preparation of classroom teachers. Kirsti said, “As far as training, none of the teachers at this school were trained to know anything about dyslexia.” Continuing, she said, “It floors me” that university coursework is not adapting coursework to the idea that dyslexia interventions change the brain. She used authoritative language (“It’s science”) to align herself with what she understood to be accepted research findings and in opposition to teacher educators by saying, “It’s science, and we’re not changing our university-level courses at all.” Similarly, Megan pointed out that the state law requires teacher education programs to address dyslexia using ideas and materials sanctioned by the state, but she said, “I’m not sure that is exactly happening at all of our universities yet. I’m not sure that some of our professors even understand that phonics and phonemic awareness might be important.”
Looking for Dyslexia
All participants asserted that dyslexia is under-identified and that teachers need to be able to recognize the signs so they can refer students for testing.
Dyslexia as under-identified
Although there is no research consensus about the incidence of dyslexia, Shaywitz (2003) considered any student reading “below the age, grade, or level of ability” based on a discrepancy between a test of intelligence and reading achievement to be dyslexic (p. 30). A figure of 15% to 20% is commonly cited in the media (IDA, n.d.-b; Reading Horizons, n.d.), and some interventionists, persuaded by the authority of these statistics, saw this as their goal for identifying students. As Sara said, “When I hear dyslexia, I immediately say one in five. . . I do not think it is getting the attention that is needed considering the amount of children it affects.”
Participants spoke with urgency about stepping up identification so that more students could be served. For example, Carol said she is “hoping that, as time progresses, more schools will identify more kids. Because there are so many unidentified kids out there, I believe. It’s really sad because they could have such a better chance at being successful in life.” Kirsti said she worries about students, “especially those dyslexic kids that think out of the box.” She referred to a post about dyslexia on Facebook that posed questions about unidentified students: What if that kid that slips through the cracks is the one with the cure for cancer? What if we’re writing them off or we’re not giving them everything they need to be successful? What if that is the kid who could really change the world?
She said, “That post keeps coming back to me. They’re that talented; it could happen.” Six participants talked about the importance of early identification, noting that waiting for students to fall farther behind is unproductive. As Claire said, In order for them to qualify for dyslexia at the younger ages, they have to be so low. . . Then when there’s a significant gap there, then they’ll qualify. Well, then it’s harder to get them to catch up.
Kirsti was frustrated with kindergarten and first-grade teachers who decide to “wait and see” and vowed, “I’m not going to wait and see anymore.” Sara noted that “many children are able to hide it.”
Two participants described situations in which testing failed to identify dyslexic students. Angela said she believes her son is dyslexic; she requested district testing, but he was not identified. She felt the testing was inaccurate, asserting, “I swear he’s like one to a T, so I don’t know how he manipulated the thing.” Kirsti said she thinks the tests used in her district are “good tests, [but] I don’t think they are broad enough to catch everything,” recalling a case of dyslexia that was not caught. When the district did not identify one of her students as dyslexic, Kirsti encouraged private testing: “I just had one [student] that we had tested outside, because [the district] said he was not dyslexic and the neurologist said, ‘Yes, he is.’” Kirsti’s story is indicative of how medical professionals are held up as authorities, even in education-related contexts (Baglieri et al., 2011).
Raising awareness of dyslexia
Five interventionists said their dyslexia training increased their awareness and made them more attuned to the prevalence of dyslexia. Brenda, who previously taught special education, said, “Three days into the training, I’m realizing that almost all my LD kids are dyslexic and I didn’t even know that’s what it was, but there was a way to fix it.” Claire said the dyslexia training led her to realize that her son is dyslexic: “Had I not gone through all of this, I would not have known to advocate to get him tested.”
Seven participants said the training they provided to teachers on their campuses along with their district’s increased focus on dyslexia was helping to raise awareness of dyslexia in their schools, leading to increased identification. Sara said her school has “a really good climate” regarding dyslexia: “We have people talking about it. We are identifying so many more kiddos.” Brenda told a similar story: Since I’ve been here, every year I do teacher training in the beginning of the year so our teachers have gone from not knowing what dyslexia is to coming to me and saying, “I have one.” . . . So, I would say the teachers are more educated here, very supportive, looking for kids who may need that type of intervention or may be dyslexic.
Seven participants spoke about efforts to increase identification of dyslexia in their schools and districts. Carol said, “We’ve almost identified 20% of our population here, which is the worldwide statistic, I think.” Kathy described her school as “on the lookout for dyslexia,” and Kirsti noted that the first-grade teachers, with whom she had been working closely, “got a lot better at identifying and getting those kids tested.” After “feeling like an army of one,” she said, “the first-grade teachers started to get on board, because they were having to deal with the things that I can fix.”
Professional Identity
From participants’ descriptions, it was clear that their training had a transformative effect on their professional identities. Participants expressed a sense of separateness from other teachers because of their training and because they only served students identified as dyslexic.
Increased confidence
The intensity and focus of dyslexia training, in conjunction with IDA’s materials and Texas policy, appeared to fundamentally affect the interventionists’ confidence in their knowledge of dyslexia and ability to provide effective intervention. Participants talked of being transformed by the training. Rosie explained, “It was two years of talking about nothing but dyslexia. . . It was all I lived and breathed for two years.” Claire said she felt much more self-assured about her knowledge of dyslexia: “I thought I knew a lot before, and I didn’t realize how much I didn’t know until the extra training.” She continued, So, in hindsight, when I go back and I think about what I taught in Special Ed, I think, oh my god, I wish I had known what I know now back then. Because I know there are certain kids I had in elementary, middle, and high school that were severely dyslexic, and I just felt like whatever I was doing with them was not working at all.
The training provided Angela “a deeper understanding of the strengths, and that’s huge, and it just kind of all makes sense. Before I was just, they can’t read, or they’re not going to read, and that’s not true at all.”
Compared with the limited confidence of the teachers in our previous study (Worthy et al., 2016), the dyslexia interventionists expressed a high degree of certainty in their knowledge about dyslexia and in the intervention programs they used. Of the 13 participants, eight expressed unequivocal confidence. Kathy, for example, said she felt “1000% confident.” Four participants who were still in training said they were confident but still had more to learn, and one (Kirsti) said she was confident “as long as I stick to the script.”
Interventionists’ experiences in schools
Most interventionists spoke of themselves as separate from teachers. Angela underscored her feelings of separation, saying, “I haven’t seen a non-dyslexic in a long time.” Rosie, a former classroom teacher, articulated the tension she felt in her professional identity, sharing that her trainings specifically emphasized the message, “Don’t think like a teacher, think like a therapist.” Angela said she pursued training in dyslexia rather than a master’s in literacy because “I’m not a literacy teacher, I’m a reading interventionist, mostly with dyslexic kids, and I couldn’t find anything like that. I didn’t want to learn about literacy in the classroom or. . . any of that.”
Dyslexia interventionists described how others at their schools looked to them as experts with specialized knowledge to help dyslexic students. Brenda explained there was a general understanding at her school that teachers could refer students to her and she would be able to help them: “The teachers are very grateful that there is someone to help them with this. . . to fix it for them and bring them back.” Similarly, some interventionists articulated that their specialized understanding of dyslexia put them in a unique position. Brenda stated with confidence, “So a therapist [dyslexia interventionist] knows all those little things that the brain is having trouble with.”
The interventionists’ views of their roles and responsibilities as dyslexia interventionists sometimes served as sources of tension among staff at school campuses. For example, several interventionists said they felt a lack of support when they pulled students out of regular classroom instruction for intervention. Catherine shared how teachers sometimes “get mad at me because I’m doing my job.” These tensions seemed related to the interventionists’ beliefs that general education teachers were misinformed or uninformed about what students labeled with dyslexia need. Lisa noted, I see some teachers, they don’t really understand how important those services are at young grades, and so they see them as a bother because kids miss something and they have to make it up and they [teachers] have to figure that out.
Discussion and Importance
It was clear the interventionists in our study were committed to the academic growth of their students and firmly believed the programs they used were the only effective interventions for dyslexia, even though research does not support this belief (Ritchey & Goeke, 2006; WWC, 2010). According to our participants, these intervention programs present the same skills, in the same sequence, using the same materials, and all students need to begin at the first lesson regardless of reading skill. These intervention programs focus primarily on decoding, employing repetition and rote learning, and do not include opportunities for students to read trade books or select their own texts. The narrow view of reading inherent in these programs is at odds with a more comprehensive conception of literacy learning that has been found to be effective for all students, including those with reading difficulties (Dennis, 2012; ILA, 2016; Scanlon, 2016).
The concept of AD (Bakhtin, 1981) helps us understand why the dyslexia interventionists are so certain of their beliefs and why other educators are less confident in their own knowledge and self-efficacy regarding dyslexia (Gibbs & Elliott, 2015; Worthy et al., 2016). Common dyslexia discourse, circulated by advocacy organizations and intervention training programs, has been institutionalized in legislation, making the discourse authoritative and unquestionable. The discourse and the law position one group of educators—those with training in dyslexia-specific programs—as more knowledgeable than other educators who may have broader understandings of literacy and experience teaching reading to a range of students. From this perspective, classroom teachers, reading specialists, and special education teachers are unqualified to provide dyslexia instruction unless they have received training approved by the state and by IDA (n.d.-d; TEA, 2014). The IDA also critiques approaches “popularly employed” in schools if they do not conform to IDA guidelines, stating that they are “especially ineffective for students with dyslexia” (IDA, n.d.-c, para. 1).
The participants in our study echoed these criticisms of teachers, teacher educators, and other approaches to reading instruction. They spoke with confidence, employing language walls (Matusov & von Duyke, 2009) such as “We know for a fact,” “A dyslexia therapist knows,” “By definition,” “We have isolated exactly what is breaking down,” “We know what it is, we know the neurobiology of it,” “I can fix it,” and “It has to be done exactly the same way.” They invoked brain research, “science,” and terms commonly associated with the medical field, language that can intimidate and silence open conversation (Baglieri et al., 2011). Considering the time, effort, and money they have invested in their dyslexia training, it is not surprising that the interventionists have strong beliefs about dyslexia and the efficacy of their training. Answers to reading difficulties presented with authority and certainty through trainings and advocacy organizations may be easier to embrace than the ideas that reading difficulties are complicated, that there is no clear definition of dyslexia, and that there is no accepted solution to the reading difficulties faced by students identified as dyslexic. However, in research, as in internally persuasive discourse (Bakhtin, 1981), nuance and uncertainty are the norm. According to Ellis, McDougall, and Monk (1997), “In science, nothing is certain and everything is questionable. In science, there are only hypotheses which enjoy greater or lesser degrees of support at any given moment in time” (p. 13). This view contrasts starkly with AD and with the interventionists’ absolute confidence in their beliefs about dyslexia and the interventions they used.
The AD of dyslexia and its institutionalization in policy has led to an unfortunate separation between dyslexia interventionists and other educators who share the goal of supporting students with reading difficulties. Interventionists should be working together with classroom teachers for the benefit of their students. Instead, the AD of dyslexia positions interventionists as experts who hold the key to “what works.” When students exhibit reading difficulties, the interventionists’ answer is to test, identify, and pull students out of classrooms for remedial instruction that has little basis in research. The certainty of AD leaves little room to question these ideas or to implement alternative forms of instruction that could potentially be more beneficial for students. Because they are positioned as unqualified to serve students labeled as dyslexic, teachers may not feel confident to speak back to AD and to advocate for their students (Gibbs & Elliott, 2015; Worthy et al., 2016).
Limitations and Implications
Texas has a history of dyslexia legislation spanning more than 30 years. While this makes Texas a rich site for research in dyslexia, it also limits the applicability of findings across other contexts. However, the number of dyslexia laws and training programs and the reach of dyslexia organizations is steadily increasing (Youman & Mather, 2018). Thus, the implications of this research may extend to other states.
Regarding implications for research, it would be important to examine the perspectives and experiences of other educators, including special education teachers, principals, and district personnel. Interviews with students identified as dyslexic and observations of interventions and their connections to classroom instruction would also provide valuable perspectives.
From a practice perspective, it is most important to keep in mind that the ultimate goal is supporting students with reading difficulties. Interventionists and teachers, each of whom have specialized knowledge and skills for teaching reading, should work together to ensure that all students who exhibit reading difficulties are provided with effective and meaningful instruction. This will mean moving past AD from all parties—including policy makers, university- and school-based educators, administrators, and researchers—to engage in conversation that focuses on areas of research consensus, including the need for comprehensive, meaning-based, responsive reading instruction for all students with reading difficulties (Compton, Miller, Elleman, & Steacy, 2014; Frankel, Pearson, & Nair, 2010; ILA, 2016).
Supplemental Material
OL_SUPP_APP_A_Worthy – Supplemental material for “We Know for a Fact”: Dyslexia Interventionists and the Power of Authoritative Discourse
Supplemental material, OL_SUPP_APP_A_Worthy for “We Know for a Fact”: Dyslexia Interventionists and the Power of Authoritative Discourse by Jo Worthy, Natalie Svrcek, Annie Daly-Lesch and Susan Tily in Journal of Literacy Research
Supplemental Material
Supplemental_Material_784759 – Supplemental material for “We Know for a Fact”: Dyslexia Interventionists and the Power of Authoritative Discourse
Supplemental material, Supplemental_Material_784759 for “We Know for a Fact”: Dyslexia Interventionists and the Power of Authoritative Discourse by Jo Worthy, Natalie Svrcek, Annie Daly-Lesch and Susan Tily in Journal of Literacy Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.