
Abstract
Introduction:
The aim of this study is to examine the association between social support and quality of life among older adults receiving home care services and to identify the key variables with the most impact on the quality of life (QOL).
Methods:
Cross-sectional data were collected in Finland from older (aged 65 and over) home care recipients and merged with administrative data (n = 442). The analysis was done using multiple linear regression.
Results:
The findings showed that having more social support was positively associated with increased QOL (p < .001). The presence of adequate help and support (p < .001) and higher education (p < .034) were significantly associated with better QOL. Depressed older home care recipients were more likely to experience a lower QOL (p < .001).
Conclusions:
The findings highlight the essential role of social support in promoting older adults’ possibilities to live at home meaningfully. When developing home care services, more attention is needed in recognizing and addressing older care recipients’ social needs alongside health-related tasks.
Introduction
Quality of life (QOL) is a concept directly related to a person’s physical health, social relationships, psychological well-being, level of dependence, and how they relate to the environment. 1 The World Health Organization has described QOL as an individual’s view of their position in life through the lens of their culture and value system according to their goals, standards, concerns, and expectations. QOL is considered objective and subjective, with numerous dimensions of health and well-being, including social, mental, psychological, and environmental, that can be positive or negative to an individual. 2
In old age, QOL is negatively impacted by difficulties with activities of daily living (ADL) and instrumental activities of daily living (IADL), impaired cognition, depression, poor health, lack of social networks and lack of social support.3-8 Moreover, the provision and perceptions of good care are known to positively impact overall QOL among older adults.9-11
Social support refers to the availability of people on whom individuals can rely on to receive care, love and the feeling of being valued. 12 Barrera 13 has suggested three types of social support including social embeddedness (evaluates frequency of contacts), received support (quantifies actual support received) and perceived support (estimates subjective exchanges in support and subsequent satisfaction). Much of the existing literature highlights the major role of the family in providing social support in old age. 14 While formal care services are provided by social and health care professionals, family members are still the most important providers of informal support and are actively involved in providing care. 15
The Finnish home care system has gone through several transformations over the years, resulting in more targeted and selective services to the frailest and oldest old.9,16 Building on aging in place policies the aim has been to encourage and support older adults to live at home for as long as possible.17,18 In 2022, just over 100,000 older home care clients were visited regularly, and more than half of these (59%) were visited at least once a day. 19 Currently, the Finnish home care system is faced with challenges like shortage of personnel and limited resources to respond to the increased care needs of the older population.20,21 According to national surveys, 34% of older home care recipients experience loneliness, 22 which is significantly more compared to the older population in general. 23
In other countries such as Canada, a study found home care users having lower emotional, tangible, and emotional support than non-users of home care services. 24 Likewise, a study in the US reported that home care clients who lacked social support were at higher risk of suicide. 25 The overarching outcomes of past studies point to the challenges faced by older adults receiving home care services and the effects on their QOL. Despite this, research examining older home care recipients’ QOL has remained scarce. To increase understanding of QOL in home care settings, the current study aimed to:
(i). Examine the association between social support and quality of life among older adults receiving home care services and
(ii). Identify the key factors with the most impact on the quality of life of older adults receiving home care services.
Materials and Methods
This study used combined data obtained from the Old-age social exclusion in home care – prevalence, meanings & intervention (SOLDEX) project. The data consisted of cross-sectional survey data collected from home care services recipients and administrative data accessed via the Finnish Social and Health Data Permit Authority (Findata). The administrative data consisted of information extracted from national care registers (Hilmo, Avohilmo, and Sosiaalihilmo) and the Residential Assessment Instrument (RAI) register. 26 Cross-sectional study design was used as it is suitable for collecting data on multiple variables simultaneously among hard-to-reach target groups.
Participants
Survey data were collected in Finland at two study sites in 2022. The study sites included one municipality and one joint municipal authority responsible of organizing publicly provided home care services in Northern and Eastern parts of Finland. Inclusion criteria were age 65+ and receiving home care services on a regular basis (at least once a week). Based on these criteria 2284 older home care clients received an information letter, questionnaire, consent forms, and pre-paid envelopes in early May 2022. Two reminder letters were sent; after 2 and 4 months. Overall, 559 responded, with a response rate of 24.5%, which is close national surveys conducted among the target group. 27
About half of the respondents were assisted in filling in the survey by a family member, friend, researcher, home care worker, or others. The help offered included reading the questions and filling in the survey but not responding on behalf of the participant. Six participants were excluded since they had not answered the questions by themselves. Participants (n = 111) not assessed by the RAI instruments were also excluded. Finally after this, 442 participants were included in the study (Figure 1).
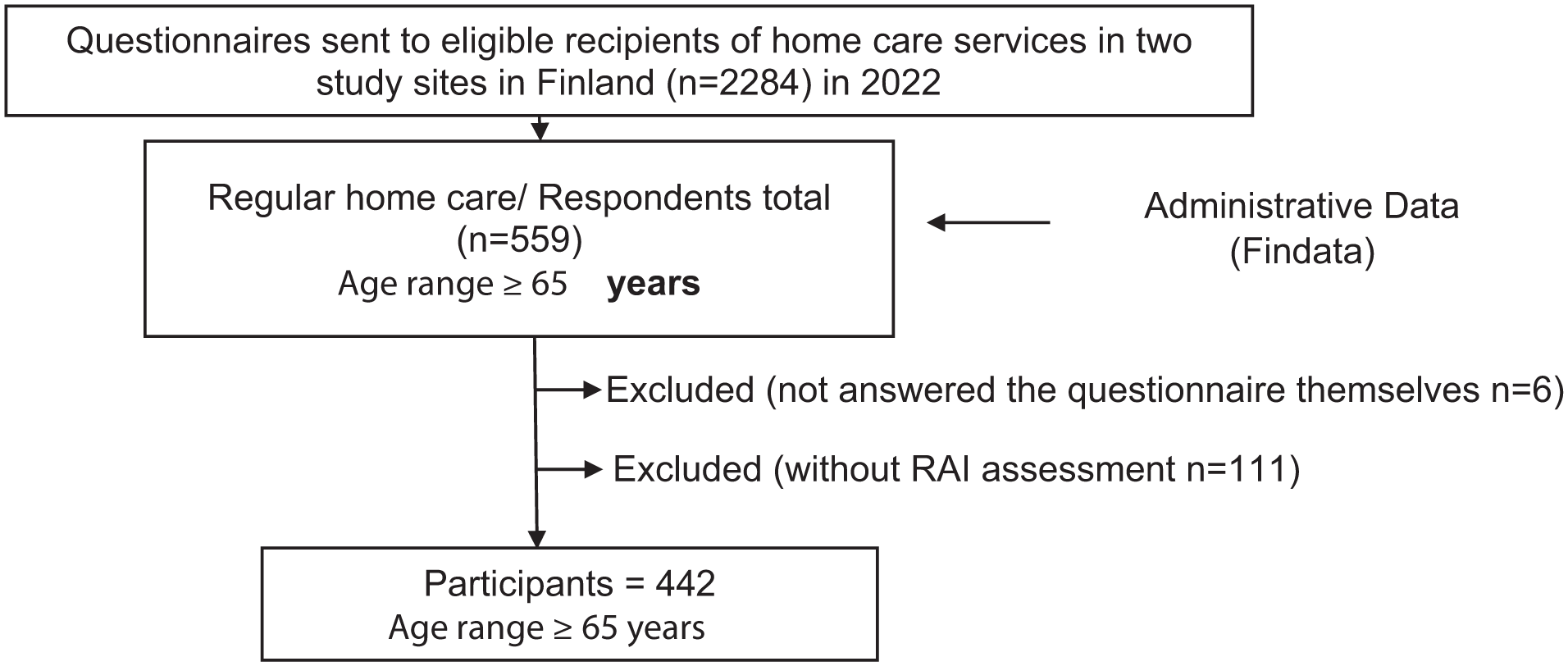
Flow chart showing the selection of participants.
Measures
Independent Variable
Social Support
The modified Medical Outcomes Study Social Support Survey (mMOS-SS) from survey data was used to measure perceived social support. The mMOS-SS scale was derived from the 19-item, self-administered social support survey developed in the Medical Outcomes Study (MOS). 28 The items within the mMOS-SS concern instrumental support and emotional/informational support. The total mMOS-SS score was computed by calculating the average score of the 8 items and then transforming to a (0-100) scale. 29 The mMOS-SS had good internal reliability and consistency with Cronbach’s Alpha .88, showing that the mMOS-SS items measured similar construct reliably.
Outcome Variable
Quality of Life
European Health Interview Survey-Quality of Life (EUROHIS-QOL) 8-items scale from survey data was used to measure quality of life. The EUROHIS-QOL 8-item measure was derived from the WHOQOL-100 and the WHOQOL-BREF.1,30,31 The 8 items were summed and averaged, with higher scores showing a higher quality of life. The Cronbach alpha for the scale was .81, showing good internal consistency of the EUROHIS-QOL 8 items.
Co-Variates
Cognitive Status
Cognitive status was measured using the Cognitive Performance Scale (CPS) from RAI register data. The scale ranged from 0 (intact) to 6 (very severe impairment). The scale includes items assessing the level of consciousness, memory impairment and the executive function of an individual to give scores reflecting cognition. The CPS scale has been validated against the Mini Mental State Examination in various studies.32,33 Cognition was dichotomized into 2 categories: no or low impairment (0,1) and moderate or high impairment (2+).
Depression
Depression Rating Scale (DRS) from RAI register data measures the symptoms of depression. The DRS has been validated against the Cornell Scale for Depression and the Hamilton Depression Rating Scale. 34 The scale scores range from 0 (no mood symptoms) to 14 (all mood symptoms present in the last 3 days). We recoded the DRS variable into 2 categories: not depressed (<3), and depressed (≥3).
Activities of Daily Living
Activities of Daily Living Long Form Scale (ADL) from RAI register data was used. The scale includes the sum of activities that show an individual’s ability to function in daily living activities such as moving in bed, walking/moving, dressing, eating, using the toilet, and personal hygiene. The scale ranges from 0 to 28, where the higher the values, the worse the individual’s ability to function in daily activities. 35
Instrumental Activities of Daily Living
Instrumental Activities of Daily Living Scale (IADL) from RAI register data measures 7 daily instrumental activities: preparing meals, doing ordinary household chores, using the phone, managing finances, taking medication, shopping, and using transportation. The scale is from 0 to 21, with lower scores indicating more independence and higher values showing the need for help in IADLs.
Other co-variates from survey data included the following variables. Age in years was calculated from birth dates and used as a continuous variable. Gender categories were male, female, and other, but there were no responses to the option of other. Marital status was recoded into 3 categories: widow, married/in partnership (married or registered partnership/common law marriage/in partnership but living separately), and not in partnership (single or unmarried/separated or divorced). Education was recoded into 3 categories: basic (primary school), secondary (vocational school/high school/community college), and higher level (university of applied sciences degree/master’s degree/doctoral degree). The ability to make ends meet was recoded into 2 categories: with difficulty (with great difficulty, with some difficulty) and easily (fairly easily, easily). Residential area was recoded as urban area (city center/suburb) or rural area (village/countryside). Study sites were (Site 1 and Site 2). Adequacy of help and support was recoded as inadequate (less than you need) and adequate (as much as you need, more than you need).
Overall, the co-variates were classified into biological factors (age, gender), socio-economic factors (marital status, education), functional ability and cognitive factors (cognition, depression, ADL, IADL), environmental factors (residential area, study site), and adequacy of help.
Statistical Analysis
Descriptive statistics of the variables were performed to obtain frequencies, percentages, means, and standard deviations. We then utilized bivariate analysis using the Pearson correlation to check the association between social support and QOL. Normality assumption tests were done for the quantitative variables using histogram charts and skewness coefficients. Multivariate linear regressions were conducted to examine the associations between social support (independent variable) and QOL (outcome variable). The bias was controlled by adjusting for potential confounding variables (covariates) found in the literature.3-8 Simultaneously, the association between covariates and quality of life was examined.
Hierarchical method was used in adding variables to multivariate linear regression models. The order of variable entry was determined based on predefined theoretical model structure.2,36 Five models were constructed as follows. Model 1 included social support and biological factors (gender, age) as independent variables. Socioeconomic factors (marital status, education) were added to Model 2. Model 3 consisted of variables on functional ability (cognition, depression, ADL, IADL) in addition to the variables in models 1 and 2. Environmental variables (residential area, study site) were added to Model 4, and lastly, Model 5 added adequacy of help. There was no multicollinearity between the independent variables because the variance inflation factor was between 1.09 and 1.79 among the individual variables, with an overall mean VIF of 1.27. The Stata 16 program was used for the analysis. A value of P ≤ .05 was regarded as statistically significant.
Results
Characteristics of the Study Sample
Table 1 shows the descriptive statistics of the participants. The average age was 85.7 (SD 7.5), ranging from 65 to 101. The majority of participants were female (73.0%). Over half of the participants were widows (55.8%). Over half of the participants could make ends meet easily (52.7%), while 47% were unable. Altogether, 18.4% of the participants reported having inadequate help. Most participants lived alone (83.7%). Urban areas had slightly more residents (58.9%) than rural areas (41.1%). A slightly bigger proportion of the participants lived in suburbs (34.8%) as compared to a village or conurbation (31.8%), whereas 24.1% lived in the city center. In contrast, only 9.3% lived in the countryside or scattered settlements.
Descriptive Statistics of the Study Participants.
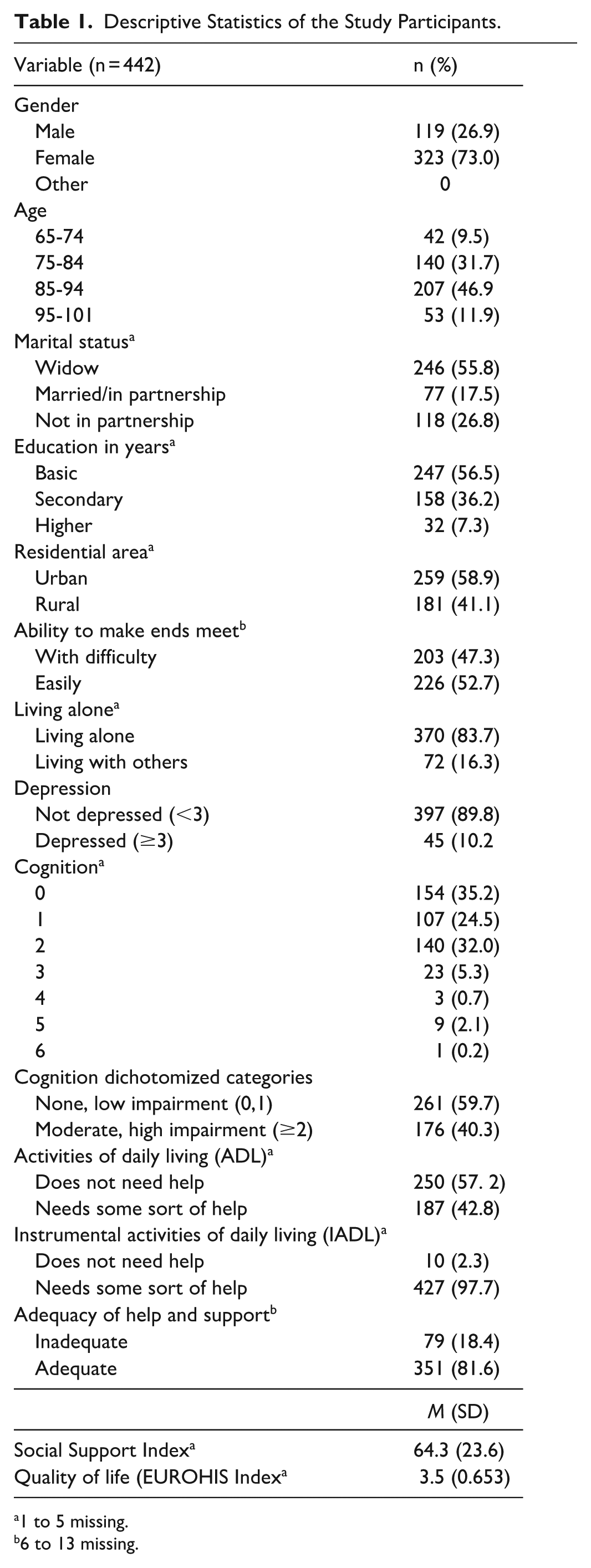
1 to 5 missing.
6 to 13 missing.
Functional Ability and Cognitive Characteristics
In the overall sample, 59.7% reported no or low impairment regarding their cognition, and the rest had moderate/high impairment deficiencies. A minority (10.2%) reported being depressed. Most participants did not need help with ADL (57.2%), while the rest required some help with ADLs. Regarding IADL, there was a greater demand for assistance, and only (2.3%) reported not needing any help, while the rest needed some sort of help at different levels.
Association Between Social Support and Quality of Life Among Home Care Recipients
Table 2 presents the association between social support and the QOL of older adults using home care services. First, the Pearson correlation coefficient showed a positive correlation between social support and the QOL of older adults, r(424) = .253, p < .001. The linear regression indicated that having more social support was positively associated with better QOL (p < .001), which was evident in all 5 models after adjusting for covariates (Table 2).
Multiple Linear Regression Models for the Association Between Social Support and QOL.
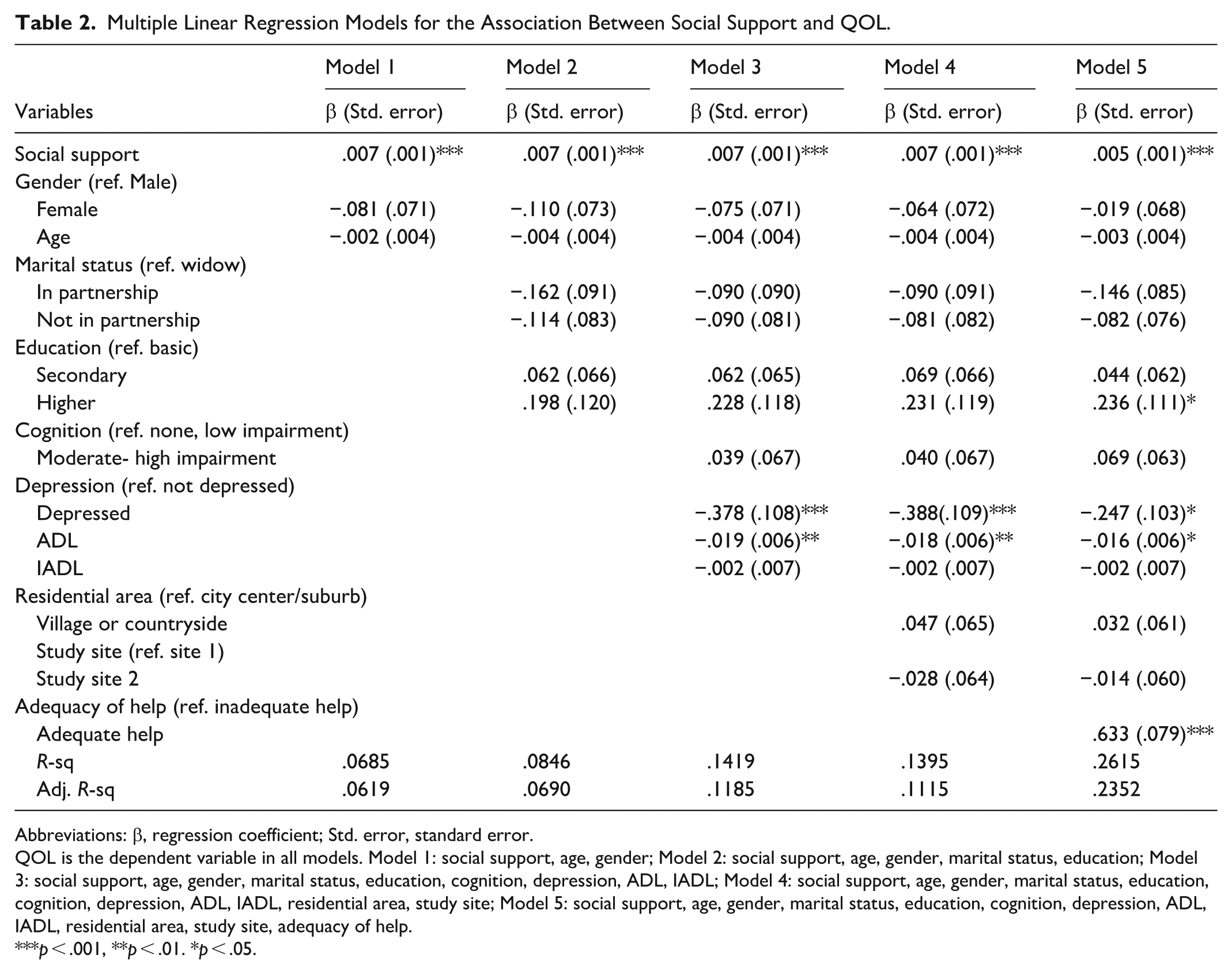
Abbreviations: β, regression coefficient; Std. error, standard error.
QOL is the dependent variable in all models. Model 1: social support, age, gender; Model 2: social support, age, gender, marital status, education; Model 3: social support, age, gender, marital status, education, cognition, depression, ADL, IADL; Model 4: social support, age, gender, marital status, education, cognition, depression, ADL, IADL, residential area, study site; Model 5: social support, age, gender, marital status, education, cognition, depression, ADL, IADL, residential area, study site, adequacy of help.
p < .001, **p < .01. *p < .05.
Other Factors Associated with Home Care Recipients’ Quality of Life
Following the second aim of the study, the variables with the most impact on QOL were observed. Having adequate help and support (p < .001) and having higher education (p < .034) were significantly associated with the likelihood of better QOL in Model 5. With regard to functional ability factors, being depressed had a negative association with QOL, indicating that depressed older adults were more likely to experience lower QOL than those without depression (p < .001 for models 3 and 4; p < .017 for Model 5). Activities of daily living (ADL) were associated with QOL (p < .006) in models 3 and 4; p < .001 in Model 5), suggesting that individuals who need help in their daily activities experience lower QOL. Biological factors did not show a significant association with QOL in this study.
Discussion
This study aimed to examine the association between social support and QOL among older adults receiving formal home care services. Focusing on the study’s first research question, the results suggest that having more social support is associated with a better QOL for older adults receiving home care services. The adequacy of help was a significant determinant of QOL outcomes: where those that received enough support reported increased QOL, while those with less support than needed suffered lower QOL. Social support included instrumental support, such as having someone to help with daily chores or getting to the doctor, and emotional support, such as having someone to love or who understands your problems. The findings suggest that while offering social support to older adults is required, it is even more crucial that the social support provided is adequate if the quality of life of older adults is to be impacted.
The findings attest to the essential role of social support in promoting QOL among older adults who receive home care services and are in line with previous literature confirming the positive relationship between social support and QOL among older adults.8,37,38 For example, in a study done in England, Finland and Austria, home care users who had frequent social contact and support reported higher QOL. 39 However, most of the previous literature has focused on specific interventions or different contexts regarding the association between social support and QOL among older adults, such as among older adults receiving cognitive behavioral therapy 40 or in nursing homes. 41
Further, the results indicate the relevance of promoting psychological well-being, such as reducing depression among older adults, and enhancing functional abilities, such as activities of daily living (ADL), in order to improve QOL. Difficulties with ADL were associated with a decline in QOL, as stipulated in previous literature. 4 Focusing on the role of education, the positive relationship between higher levels of education and increased QOL shows the importance of high education levels in shaping QOL in later life, as reported by research focusing on older adults in general. 37
Focusing on the second research aim seeking to identify the key factors with the most impact on QOL, the results suggest that social support, depression, activities of daily living (ADLs), and education stood out as the most significant factors for QOL among the study sample. It may be that since QoL embodies components of the functional status of an individual, qualities like higher education level which raises the decision-making capacity, while presence of social support lowers stress, 42 ultimately contributing better quality of life. In contrast, depression has been closely tied to physical comorbidities like cardiovascular illnesses and higher health care costs 43 consequently lowering quality of life. Unlike, findings from previous literature,44,45 gender and age did not have a significant influence on the QOL of older home care recipients. This may indicate among older adults with care needs, QOL is not merely influenced by biological factors, but rather by a number of factors including functional dependency and perceived socio-psychological wellbeing. 46
Limitations
The results are based on cross-sectional data, which does not allow conclusions to be drawn regarding the causal direction of the variables’ relationship. Also, the study population is relatively small and collected from two specific study sites and therefore the findings are not nationally representative. Moreover, it is likely that there is some bias in participation as responding to the survey requires adequate functional capabilities and the ability to give informed consent. Hence, older adults with severe functional or cognitive decline are likely to have been excluded from the study. The findings may also have been impacted by the measurements and analysis methods used. In this study, we were not able to examine from whom social support is received. Also, our analysis did not focus on different dimensions of social support separately. Both QoL and social support are subjective and multidimensional concepts with diverse meanings for different people. There may also be cultural variation in how both concepts are understood. Thus, future studies could replicate this study to investigate the association between social support and QOL among older home care recipients in other populations and cultures to further understand its impact on those living with care needs. Also, more evidence-based knowledge is needed on how to support older adults QOL in diverse home care settings. 47
Conclusions
This study advances the understanding of the association between social support and quality of life of older adults using home care services. The results suggest that higher QOL is achieved by a number of factors like psychosocial wellbeing, and not only biological factors. When developing home care services, special attention is needed to recognize and address older care recipients’ social needs alongside health-related tasks. Home care professionals play an important role in providing and ensuring adequate social support for community-dwelling older adults living with care needs.
Footnotes
Ethical Considerations
The study was pre-assessed and approved by the research ethical committee of the University of Eastern Finland. Permission for research from both study sites was applied for and received before the data collection process. Participation in the study was voluntary.
Consent to Participate
Study participants gave informed consent in written format.
Consent for Publication
Permission to publish research results was included in the informed consent given by the study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has been financially supported by the European Union’s Horizon 2020 Research and Innovation Program under Marie Sklodowska-Curie (Neuro-Innovation, grant number 101034307) and the Research Council of Finland (Soldex, grant number 342267).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.