
Abstract
Older adults living with HIV (OALHIV) (i.e., age ≥50) now constitute over 50% of all people accessing HIV treatment in British Columbia (BC), Canada. As OALHIV age, the need for supportive care in non-acute settings, including home and community care (HCC), is increasing. The Thrive research project was co-created alongside OALHIV in BC to support people to thrive with a good quality of life (as contrasted with just surviving). Phase 1 of the project linked treatment and demographic records for 5603 OALHIV accessing care in BC. Phase 2 took a community-based research approach with semi-structured interviews to understand obstacles and pathways experienced by 27 OALHIV in accessing HCC. This article summarizes previously published Phase 1 findings and explores Phase 2 findings in-depth. On the HCC journey traveled by OALHIV in BC, there are four main junctures at which obstacles and pathways appear: (1) before referral, (2) during the referral process, (3) at the assessment, and (4) while receiving services. Obstacles are largely related to fluctuating HCC priorities and funding cuts tied to election cycles, requiring systemic and policy changes to enable positive outcomes and impacts in the provision of HCC services. These obstacles can be transformed into pathways through public policy and client-centered, culturally safe care.
Introduction
Older adults living with HIV (OALHIV) (i.e., persons living with HIV/AIDS [PLHIV] age ≥50) now constitute over 50% of all people accessing HIV treatment in British Columbia (BC), Canada. 1 While access to publicly funded treatment and advances in combination antiretroviral therapy (cART) mean OALHIV in BC are approaching life expectancies of the general population, 2 many health and social challenges persist.3-5 OALHIV experience higher rates of comorbidities than HIV-negative individuals, and these conditions can be worsened by persistent inflammation and chronic immune suppression. 6 Sociostructural inequities associated with HIV also have cumulative effects on mental, emotional, and physical health.7-9 The healthcare needs arising from these distinct challenges have implications for the provision of aging-related health services.3,9,10 There is a growing need to appropriately support the unique psychological and psychosocial challenges associated with HIV and aging (e.g., long-term cART toxicity, dementia, menopause, mobility challenges) and to understand the impacts these demands have on available healthcare and ancillary services,11-20 in urban, rural, and remote areas.
As PLHIV grow older, it is more likely they will need to access supportive care in non-acute settings, including home and community care (HCC). 21 In BC, publicly funded HCC services include home support, community nursing, community rehabilitation, assisted living (AL), and long-term care (LTC). A 2016 study found that BC had the highest prevalence of HIV among home support clients—0.49%, over double the 0.21% prevalence of HIV in the general Canadian population—when compared with Manitoba, Ontario, Nova Scotia, and the Yukon. 10 These HCC services may not be designed to encompass the unique healthcare needs, family, and support structures of the populations most affected by HIV in BC (i.e., gay, bisexual, or other men who have sex with men; people who use substances; people of African-Caribbean descent; and Indigenous individuals). Despite the role HCC may have in the healthcare experiences of OALHIV as they age and require higher levels of formal care, 22 this field remains relatively unexplored, particularly in Canada and BC’s context of fluctuating HCC priorities and funding cuts.23-28 This research aims to address this gap and encourage other researchers, policymakers, and service providers to build upon this research for implementation in HCC services.
Methods
The Thrive research project was co-created alongside OALHIV in BC to support people to thrive during all stages of life. Thrive was a 3-year, community-based research study focused on OALHIV accessing HCC in BC, led by the BC Centre for Excellence in HIV/AIDS. Thrive’s purpose was to evaluate the impact of shifting priorities and funding for HCC on the health outcomes and health care experiences for OALHIV. The study’s mixed methods design included: Phase 1, a quantitative arm that leveraged administrative data to monitor trends in health and healthcare utilization among a cohort of OALHIV compared to the general population in BC; and Phase 2, a qualitative arm exploring obstacles and pathways experienced by OALHIV accessing HCC services in BC. Following the guidance of the team’s Indigenous peer research associate, we use the terms “obstacles” and “pathways” instead of “barriers” and “facilitators” to decolonize research language. Ethics approval was received by the University of British Columbia/Providence Health Care Research Ethics Board.
Data and Procedure
Using data from the STOP HIV/AIDS® cohort from 2005 to 2015, which includes linked treatment and demographic records for PLHIV accessing care in BC, Phase 1 of the study compared OALHIV who did and did not access HCC services. Adjusted odds ratios (aORs) were estimated for factors associated with HCC service utilization using logistic regression for sex, self-identified risk factor (e.g., history of injection drug use), having a general practice visit, CD4 count at cART initiation, and Charlson comorbidity index. For Phase 2, a coding framework was co-developed based on priori categories to inform the interview guide focusing on the social, structural, and spatial dimensions of aging with HIV and accessing HCC. Recruitment posters were distributed at AL and LTC facilities, permanent supportive housing facilities, AIDS service and other community organizations, and health clinics serving older adults in Greater Vancouver, BC, Canada. The peer research associates—OALHIV trained in qualitative research methods—and the study coordinator co-conducted 27 semi-structured interviews with OALHIV (n = 27) in the Vancouver Coastal Health and Fraser Health regions. Interviews were conducted over the phone from July to December 2020, with the exception of 7 in-person interviews conducted in February 2020 prior to the onset of the COVID-19 pandemic. Interviews with service providers (n = 10) were conducted over the phone from January to June 2021, including perspectives from social workers, HIV specialists, and peer navigators on how their clients learn about, are referred to, are assessed for, and receive HCC services. The team piloted the codebook by coding an interview transcript together in NVivo to facilitate immersion into participant stories and determine a coding approach, including emergent categories that arose from the data. The semi-structured interviews (N = 37) were then analyzed thematically in two streams: pathways and obstacles in accessing HCC services experienced by OALHIV.
Results
The results summarize previously published Phase 1 findings 1 and explore Phase 2 findings in-depth. Phase 1 included 5603 OALHIV aged ≥50, 837 (14.94%) of whom accessed HCC services between 2005 and 2015. Community nursing (8.98%, n = 503) and rehabilitation (7.73%, n = 433) HCC services were most commonly used, followed by home support (5.85%, n = 328), LTC (1.84%, n = 103), AL (0.36%, n = 20), emergent care (0.34%, n = 19), convalescent care (0.25%, n = 14), and respite care (0.12%, n = 7). 1 Some OALHIV accessed more than one HCC service. Those who received HCC were more likely to be female (aOR = 1.56, 95% Confidence Interval [CI] = 1.24, 1.98), have a history of substance use (aOR = 1.88, 95% CI = 1.57, 2.25), have a higher Charlson comorbidity score (aOR = 1.11, 95% CI = 1.07, 1.15), and have visited a general practitioner in the past year (aOR = 2.17, 95% CI = 1.77, 2.67). 1 The Phase 1 results highlighted the need to explore obstacles and pathways in accessing HCC for OALHIV in Phase 2.
For Phase 2, of the 27 OALHIV interviewed, 15 had used HCC services and 12 had not, including three people who had applied for and were denied services. More than half of the OALHIV participants (59%, n = 16) reported two or more comorbidities. The three most common comorbidities were chronic obstructive pulmonary disease (37%, n = 10), arthritis (26%, n = 7), and hepatitis C (19%, n = 5). On the HCC journey traveled by OALHIV in BC, there are four main junctures at which obstacles and pathways appear: (1) before referral, (2) during the referral process, (3) during the assessment, and (4) while receiving services. The most commonly identified obstacles for accessing HCC services are the referral and assessment processes. Participants described accessing HCC services as “not easily accessible,” “with so many different hoops and red tape,” “bureaucratic,” and/or “hard to navigate.”
Before Referral
Before a person can begin the referral and assessment process, they first need to know where to find this information. HCC services information is often not easily accessible, such as where to find it, who to contact, or what the eligibility criteria is. As a result, people often contact the wrong agencies. Additional reasons that may preclude OALHIV from being referred to HCC services included: (a) fear of stigma and discrimination from HCC workers and in AL and LTC facilities and (b) residing in rural and remote locations. OALHIV who knew about HCC services before their referral reported that they were either well-informed through their volunteer work or by being an active participant at an AIDS service organization.
Referral
There is a stark contrast between referrals from within the community versus following an acute incident and/or hospitalization. Referral from within the community is commonly supported by several professionals (e.g., physician, social worker, peer navigator) or via a community health clinic or specialized HIV/AIDS clinic where multidisciplinary teams help with referrals and assessment. Most OALHIV participants had extra help in seeking and securing HCC services and believe their efforts would not have been successful without the help of a social worker, outreach worker, peer navigator, or their doctor. As this participant explained: If I didn’t have a team behind me to help me navigate, I probably would have a harder time doing it. . .The process is a little bit long. The wait is long. Anything that needs to be done has to go through so many different processing hoops and red tape that sometimes it feels almost like you’re better off not even starting. (OALHIV participant C)
In contrast, acute incidents and hospitalizations prompt HCC referral and assessment at discharge. Paperwork is completed by professionals in the hospital, supporting the client with the HCC referral. Although this usually happens, some OALHIV participants did not receive HCC services because services were denied (i.e., assessed as ineligible), the client was not assessed for HCC services following an acute incident and hospitalization, or family members intervened despite the client’s wishes to receive HCC services at home. Common obstacles experienced through both referral routes (community and acute incident/hospitalization) included: (a) unclear communication pertaining to eligibility criteria; (b) long wait times during the referral process; (c) advocacy fatigue experienced by individuals, family, friends, and other informal caregivers; (d) and in some cases, the convergence of HIV/AIDS diagnosis, poverty, homelessness, and/or substance use obstacles to accessing stigma-free care.
Assessment
The point of assessment, guided by the contact person conducting the assessment, is a crucial step in receiving HCC services and determining what kinds of services will be granted. Some OALHIV participants were denied HCC services or had their services discontinued following funding cuts. This finding parallels the conclusion of the 2020/2021 Annual Report by the Office of the Seniors Advocate, which states that “access to home health and home support services including limited hours of care and inconsistent scheduling of service” is one of the systemic gaps in senior services. 28
“Taking the time” while conducting the assessment was cited as one of the prerequisites for a proper assessment. Some OALHIV participants shared positive interactions with their assessor, emphasizing the importance of thoroughness and attentiveness to the individual’s needs and surroundings. As one OALHIV participant put it, “[the assessor] did a pretty good job seeing what was needed in my home to keep my independence.” Other participants described unsatisfactory assessments, characterized by “a tick mark questionnaire,” “not very appropriate,” “very heavy top down,” “bureaucratic,” and “not fair.” As a family physician shared, he needed to advocate for a patient with deteriorating health, who was declined HCC services by an assessor after a 15 to 20-minute assessment. Notably, the HCC Services Policy Manual suggests “collaboration between the assessor and primary physician.” 29 Yet, service providers (e.g., physicians, peer navigators, social workers) reported a lack of collaboration between themselves and individuals assessing their patients/clients for HCC services. At the opposite end of the spectrum of taking the time was taking too much time and involving too many different entities in the assessment process. As an OALHIV participant shared, “I broke my arm, and they were supposed to come and give me a hand. But by the time they were showing up, my cast was off. It took a very long time. It took over 6 weeks for them to get back to me” (OALHIV participant Q). This was especially pronounced when services were sought for a chronic condition or if additional services were needed outside the scope of the HCC services.
Intersectional obstacles can also present challenges to OALHIV in accessing HCC services due to stigma and discrimination, including but not limited to socioeconomic means, ethnicity, gender, sexual orientation, and comorbidities (see Figure 1 for intersectionality stories from OALHIV). For example, episodic disability, where an individual experiences periods of ill health interspersed with times of being well, is a common condition among PLHIV. 30 Some OALHIV participants shared how they presented better or worse during the time of assessment and how that affected the outcome. In some cases, OALHIV participants were fortunate because the assessors were understanding and flexible. On the other hand, some OALHIV participants did not receive services because they were more mobile at the time. An OALHIV participant recalled being denied services because he was not immobilized, even though immobilization is not a requirement for HCC in BC (having a life-limiting illness, recently being discharged from a hospital for acute care, and/or requiring care to reduce/prevent the need for hospitalization or admission to LTC are the eligibility criteria). Further, homelessness and precarious housing were identified as obstacles in the assessment process, with unclear guidelines on what conditions were considered safe or unsafe for HCC workers. As a service provider participant explained, “There are people who live in very precarious housing situations or are homeless. How do they get these services? It’s pretty impossible if you don’t have a decent place to receive them.” As such, intersectional obstacles need to be considered to enable more equitable access to HCC.
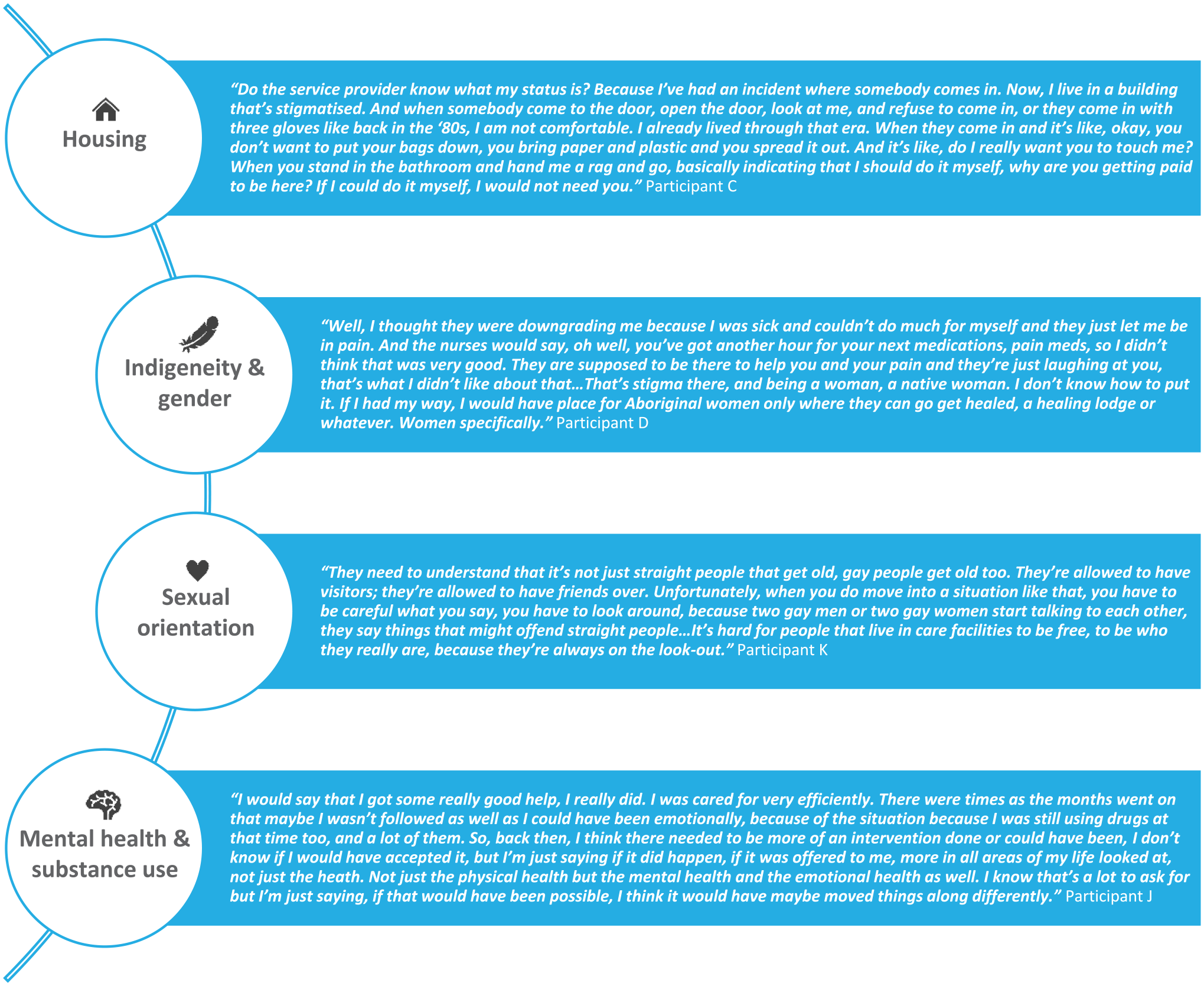
Intersectionality stories from OALHIV.
Receiving HCC Services
HCC services provided to OALHIV participants commonly included bathing and grooming. OALHIV, particularly those without informal caregivers, commonly also require meal preparation, cleaning, laundry, and support to conduct errands (e.g., grocery shopping, medication pick-up/delivery), which are unmet needs by current HCC services. These services are necessary to enable independence and aging with dignity for those who desire to live at home (versus LTC). When these needs are not provided by HCC services, it requires people to pay out-of-pocket. Some OALHIV cannot afford out-of-pocket payments, commonly paid to informal caregivers, due to Canada’s disability benefit and Canada Pension Plan amounts, which are set below the poverty line. From being denied basic services (e.g., requesting a bath more than once a week) to last-minute rescheduling, various OALHIV noted a decline in the quality of services tied to election cycles and shifting priorities, with fewer services now offered. When OALHIV participants received excellent care, they credited HCC workers who love their job and provide care in a relational manner. This underpins the importance of HCC workplace cultures that attract, recognize, and retain exceptional staff.
Scheduling conflicts in HCC workers’ shifts were commonly observed by OALHIV participants. Examples included last-minute service cancelations, incomplete services due to juggling several clients and transportation time, and rotating HCC workers. As shared by an OALHIV participant: “It was usually a different person. I had a different person come three or four times a week.” As such, scheduling conflicts present unstable environments for both HCC workers and their clients when services can not be completed in the allotted time, particularly when rotating HCC workers are juggling several non-regular clients and need more time at the beginning of the appointment to understand the client’s service needs. Furthermore, previously, clients received regular communication and follow-up calls from a HCC services case manager. A “twice-removed” phenomenon appears to have contributed to a lack of communication and follow-up calls. This generates uncertainty in how to issue a complaint.
Discussion
Community nursing, rehabilitation, and home support were the most commonly accessed HCC services amongst OALHIV in BC. Across these and other HCC services, obstacles and pathways appear at four main juncture points: (1) before referral, (2) during the referral process, (3) at the assessment, and (4) while receiving services. The HCC provisions framework in Figure 2 shows recommendations for BC. This framework can be used by other regions and countries to identify public policy and HCC care recommendations for the four main junctures at which obstacles and pathways appear. This research and framework begin to address the need for research and policy development on HCC services implementation for OALHIV and other populations living with complex health conditions and comorbidities.

Public policy and client-centered, culturally safe care framework for HCC provision: BC recommendations example.
By definition, HCC services in BC are designed to “complement and supplement, but not replace, your efforts to care for yourself with the assistance of your family, friends and community.” 31 This presents an obstacle for some OALHIV because they do not always have care support from family, friends, and community. For example, friends may have passed away, family might live in another country, peers may need to redirect attention to their own care needs, and some families withhold support based on stigma. As such, some OALHIV turn to informal caregivers to supplement services that are not provided through HCC, yet are essential to survival (e.g., grocery shopping). OALHIV may be denied HCC services because they receive some support from informal caregivers. Some OALHIV participants also shared stories that signaled commodification of relationships with their informal caregivers (e.g., when grocery shopping would be done only in exchange for money, food, or shelter). Such commodification can make any older adult vulnerable to abuse, and OALHIV who are often marginalized by sociostructural inequity and experience higher rates of poverty and isolation, are perhaps more at risk of being subject to such abuse.
HCC services, and healthcare more broadly, require an intersectional understanding to support client-centered care for OALHIV and BC’s other aging populations. This includes diverse sociodemographic characteristics, such as ethnicity and Indigeneity, all gender identities and sexual orientations, religious practices, socioeconomic factors (e.g., housed versus unhoused or under housed, education, occupation), and comorbidities (e.g., episodic disability and medication side effects, substance use, etc.), to name a few. 32 From before referral through to receiving HCC services, public policy development and client-centered, culturally safe care improvements are vital in the HCC provision to OALHIV and the general population. These public policies and HCC services require a sustainable foundation and multigenerational strategy that withstands election cycles and shifting political priorities.
Conclusion
OALHIV (i.e., age ≥50) now constitute over 50% of all people accessing HIV treatment in BC, Canada. 1 As OALHIV age, the need for HCC is increasing. On the HCC journey traveled by OALHIV in BC, obstacles and pathways appear: (1) before referral, (2) during the referral process, (3) at the assessment, and (4) while receiving services. To transform HCC obstacles into pathways, policy development and client-centered, culturally safe care are required in the provision of HCC services. When OALHIV are supported by pathways along their journey to access HCC, they can thrive and age with dignity.
Footnotes
Acknowledgements
The authors acknowledge with gratitude the OALHIV and service providers that made this research possible through their participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research’s (CIHR) Community-Based Research Operating Grant.