
Abstract
Background
In light of the accelerated growth of China's digital economy and the ongoing enlargement of the older adults population obsessed with chronic ailments, the ramifications of the digital divide on the quality of life of urban older adults with chronic diseases have emerged as a significant concern. This study seeks to elucidate the manner in which the digital divide influences the quality of life of urban older adults with chronic diseases.
Method
This study employs the Chinese Older Adults Social Tracking Survey (CLASS2020) dataset and a multivariate ordinary least squares (OLS) regression model for statistical analysis. In this study, quality of life is employed as the dependent variable, while digital access and digital use of the digital divide are utilised as core explanatory variables. The pertinent indicators are weighted using the CRITIC weighting method to construct a composite indicator of quality of life and digital use.
Result
Study findings show that digital access boosts urban older adults’ quality of life with chronic conditions, but overuse could reduce it. Social support mediates this relationship, with formal support being most effective. Accessibility of community services and facilities have a negative moderating effect on this influence: they decrease the positive impact of digital access and reduce the negative effects of digital use. Notably, Accessibility of community services enhances quality of life by offering care and activities, showing a “replenishment” effect. It is suggested that the government promote the inclusion of smart older adults care through state subsidies and tax credits.
Conclusion
This study highlights the importance of social support and community environment in improving the quality of life for older adults with chronic diseases in the digital economy. It suggests that policymakers should focus on reducing the digital divide and enhancing accessibility of community services to support these individuals. Additionally, the potential mental health issues arising from digital use should be recognized, requiring appropriate digital education and psychological support for older adults.
Keywords
Introduction
Presentation of problem
The scale of China's digital economy continues to expand at a considerable rate, as does the information industry. In 2023, China's digital economy is projected to reach 50.2 trillion yuan, representing 41.5% of the country's gross domestic product (GDP). 1 The digital economy is becoming an increasingly significant component of the Chinese economy. Concurrently, the Internet is experiencing a rapid increase in popularity in China. As of June 2024, the number of Chinese netizens has reached 1.09967 billion, representing an increase of 7.42 million from December 2023. Furthermore, the Internet penetration rate has reached 78.0%. The Internet has become an integral and indispensable aspect of modern life, permeating various aspects of human activity, including education, work, and personal interactions. Conversely, the popularisation of the Internet will result in a significant demographic imbalance by 2023. It is estimated that 62% of non-Internet users in China will be aged 60 and above, while 55.7% of non-Internet users in rural areas will also be above this age. Furthermore, the distribution of Internet users across China is uneven, with significant regional imbalances.
In line with the ongoing and accelerated growth of the economy and society, the health threat model of Chinese residents has also undergone a transformation. Chronic diseases have emerged as the primary determinant of health outcomes among Chinese residents.2,3 The prevalence of chronic diseases among the older adult population is high and shows a continuous growth trend. 4 The data from 2011 and 2015 indicated an increase in the prevalence of chronic disease comorbidities among older adults aged 60 years and above, from 85.96% to 92.24%. 5 As the population of older adults with chronic diseases in China continues to grow in size with the ageing of the population, it is imperative to seek solutions within the context of the information society.
Since the concept of the digital divide was first proposed in 1989, its connotation has continued to expand. Initially focusing only on the differences in access to information and communication technology (ICT),6,7 it has since come to encompass multiple dimensions, it has developed inequality in skills and use (Level 2 digital divide)8,9 and inequality in outcomes (Level 3 digital divide).10,11 The report of the 20th National Congress of the Communist Party of China proposed the implementation of a national strategy to actively respond to the ageing of the population, with the objective of elevating the development of the older adults care industry to an unprecedented strategic height. 12 Concurrently, the State Council released the “Overall Layout Plan for the Construction of Digital China,” underscoring that the development of Digital China serves as a pivotal driver for modernization and a source of policy backing for intelligent older adults care services. 13 Nevertheless, the implementation of smart older adults care is confronted with a number of challenges, including digital exclusion, resource mismatch, and digital anxiety in actual application. 14 In essence, the digital divide hinders active ageing among older adults. Older adults residents are already constrained by the digital divide, which is influenced by factors such as health level and cognitive ability. Older adults patients with chronic diseases encounter greater challenges in navigating the digital divide. Concurrently, despite the considerable advancement in digital infrastructure in urban areas, older adults in urban settings still confront the challenge of inadequate digital integration and a conspicuous digital divide. In light of the aforementioned analysis, this study will examine the population most affected by the digital divide: the quality of life of urban older adults with chronic diseases. It will also investigate the mediating and moderating effects behind this phenomenon. The study employs the most recent CLASS2020 dataset and the OLS regression model for data processing.
The rapid expansion of the digital economy and aging populations with chronic diseases pose dual challenges globally. 15 While digital technologies promise enhanced access to healthcare and social connectivity, older adults—particularly those with chronic conditions—face systemic exclusion due to the digital divide. 16 This study addresses three critical questions: (1) How do digital access and usage disparities impact the quality of life of urban older adults with chronic diseases? (2) What mediating roles do formal and informal social support systems play in this relationship? (3) How do individual behaviors and community-level factors moderate these effects?
Literature review and research framework
A substantial body of research has been conducted by the academic community on the factors affecting the quality of life of patients with chronic diseases. In terms of positive factors, patients who do not smoke, have regular physical examinations and exercise have been found to have a higher quality of life. 17 Similarly, self-efficacy has been identified as having a positive impact on the quality of life of patients. 18 Furthermore, patients with good social support and caregivers have been found to have a higher quality of life.19,20 In comparison to residing in rural areas, residing in urban areas has been demonstrated to enhance the quality of life of patients. 21 Patients with superior health literacy have been shown to exhibit a higher quality of life.22,23 Patients with medical insurance and access to timely medical services have been found to have a higher quality of life. 24 Patients with effective disease management have been observed to have a higher quality of life. 25 In terms of negative factors, patients with multiple chronic diseases have a diminished quality of life, particularly when they also suffer from common chronic diseases such as hypertension, diabetes, and coronary heart disease.26,27 Patients of an advanced age have been found to have a lower quality of life.28,29 Furthermore, female patients have been observed to experience a worse quality of life than their male counterparts. 30 Additionally, patients with low income, low educational attainment, and those who are unemployed or retired have been found to have a poor quality of life31–33; depressive symptoms have a significant negative impact on the quality of life of patients with chronic diseases. 34
Age is a significant factor influencing the quality of life of patients with chronic diseases. Older adults with chronic diseases tend to experience more severe health challenges. From an individual perspective, a favourable lifestyle, self-management proficiency and comprehensive medical service modalities can enhance the quality of life of older adults with chronic diseases.35–37 Older adults with chronic diseases who are older and have lower educational attainments exhibit a diminished quality of life 28 ; Factors such as living status and pre-retirement occupation also have a significant impact on the quality of life of older adults patients with chronic diseases 38 ; Economic income, the number of hospitalisations and the years of illness have an impact on quality of life scores in multiple areas of chronic diseases in the older adults.38–40 From a social perspective, the level of social support and the ability of family members to provide support are significant factors in improving the quality of life of older adults with chronic diseases.41,42 Strengthening the prevention and treatment of chronic diseases and improving primary medical and health services, as well as implementing health education and other measures, are crucial to improving the quality of life of older adults with chronic diseases.43–45
The digital divide poses a relatively severe adverse impact on the mental health of the older adults. As mental health constitutes a critical component of life quality for the older adults,46,47 it is essential to examine the specific manifestations of this negative effect. The detrimental influence of the digital divide on the mental health of the older adults primarily manifests in two aspects: acting as a barrier to accessing electronic health resources and exacerbating psychological distress through social isolation. Regarding the former, the older adults often struggle to effectively utilize digital health services due to insufficient digital skills, leading to unmet healthcare needs and heightened psychological stress. 48 In South Korea, the older adults facing the digital divide demonstrate a significantly increased risk of depression due to limited access to health information. 49 Similarly, the older adults in rural China experience anxiety stemming from their inability to manage chronic diseases via smart devices, a consequence of inadequate digital literacy. 50 Concerning the latter, the older adults lacking digital competencies or devices face difficulties in maintaining social connections through tools such as email, social media, and video calls. This technological divide increasingly marginalizes the older adults in the digital society, severing communication channels with family and friends and intensifying social isolation.50,51
The preceding article addressed the factors influencing the quality of life of older adults with chronic diseases. However, it did not integrate the implications of the information society and the digital divide. The digital divide is a significant factor influencing the health and well-being of older adults, with health being a crucial element of the overall quality of life. The following section will describe the impact of the digital divide on the health of older adults. The current research posits that the impact of the digital divide on the health of older adults can be considered from two perspectives. Firstly, the lack of Internet access and usage skills hinders older adults from utilising online health services, thereby limiting their capacity to obtain health information and manage their own health. 52 Secondly, the digital divide can also be seen to affect the efficacy of digital health technologies, with older adults facing challenges in operating digital equipment, poor information transmission and a lack of trust in new technologies. 53 Furthermore, older adults encounter numerous obstacles when utilising digital health technologies, including difficulty in operating equipment, poor information transmission, and scepticism towards novel technologies. 53 Consequently, older adults are at a disadvantage in reaping the benefits of the digital dividend due to the digital divide, which negatively impacts their health status. 54 Conversely, it has been observed that as the number of older adults who utilise the Internet to obtain information increases, so does the prevalence of poor mental health. This may be associated with the information asymmetry and social isolation resulting from the digital divide. 55 The older adults’ perception of powerlessness and frustration when confronted with digital technology may further exacerbate their psychological distress, thereby influencing their overall health. 50
In conclusion, the digital divide exerts a dual influence on the physical and mental health of older adults. The SF36 scale 56 is a valuable instrument for assessing quality of life, taking physical and mental health into account. However, current research has not yet addressed the impact of the digital divide on the quality of life of urban older adults with chronic diseases.
The level of social support has been demonstrated to exert a significant influence on the quality of life of older adults with chronic diseases.
41
According to the sources of social support, the academic community classifies social support into formal social support and informal social support.
57
According to the functions of social support, the academic circle divides social support into instrumental support and emotional support.
58
Among them, the formal social support involved in this study is all instrumental support, including pensions (reflecting institutional economic security) and number of formal security (reflecting the comprehensive institutional benefits that can be enjoyed). Informal social support encompasses both instrumental support and emotional support. The former includes intergenerational economic support and intergenerational household support, while the latter refers to the frequency of face-to-face interactions between children and their parents and the frequency of communication between children and their parents. Formal support encompasses pensions, pension insurance, retirement benefits, and other benefits provided through formal channels. Informal support, on the other hand, is primarily provided by children and includes intergenerational economic support, intergenerational care support, and intergenerational emotional support. The digital divide can be bridged to enable older adults with chronic diseases to obtain health and policy information, which is conducive to their acquisition of formal social support. Instant messaging software can also be used to facilitate contact between older adults with chronic diseases and their children, allowing them to obtain information and emotional support from their children, that is, informal social support. Based on the above analysis, this study proposes Hypothesis 2a and Hypothesis 2b:
The evidence indicates that smoking is a significant risk factor for a range of chronic diseases, including cardiovascular diseases and respiratory diseases.
59
Furthermore, there is a growing body of research suggesting that smoking may also lead to an exacerbation of existing conditions and increased mortality in older adults with chronic diseases.
60
In light of the aforementioned evidence, this study posits that smoking should be considered a marker of poor lifestyle habits. In the context of the government's active promotion of the community home care model, it is imperative to examine the impact of the community on older adults with chronic diseases. Community-based services for older adults can significantly enhance the quality of life and self-management abilities of older adults with chronic diseases. This is achieved through the provision of personalised nursing interventions, health education, psychological support and other services.
61
Additionally, these services can effectively control disease progression,
62
psychological state,
63
and disease-related knowledge,
43
thereby reducing the incidence of adverse drug reactions.
64
This has a positive impact on older adults with chronic diseases. The ageing-friendly design of community public facilities provides older adults with significant opportunities for health training and social interaction, thereby enhancing their self-care abilities and reducing the care burden on families and society. This is achieved by lowering the incidence of hospitalisations and reducing medical and health expenditures.
65
In 2024, accessibility measures such as facilities, optimised lighting and pavement were implemented to reduce the risk of falls for older adults and increase opportunities for social interaction. This has been shown to improve the social adaptability and life satisfaction of older adults.
66
Based on the above analysis, this study proposes Hypothesis 3a, Hypothesis 3b and Hypothesis 3c:
Figure 1 presents the concepts and research framework of this study, which is used to investigate the impact of the acquisition and utilization of digital technology on the quality of life of older adults with chronic diseases in cities. Based on the theory of social support, this study explores the mediating effect of formal and informal social support, which plays a buffering role 67 in pressure condition. This study explored the moderating effects of community service availability, community facilities and tobacco use. Based on the main effect model, 68 the first two can directly promote the quality of life of the older adults, while tobacco use may weaken the buffering effect of social support and overall damage the quality of life of the older adults, thereby reducing the enabling effect of digital technology itself on the quality of life of the older adults. Meanwhile, this study also focused on the potential heterogeneity of digital access and digital use in empowering the quality of life of the older adults.

Research framework on the impact of the digital divide on the quality of life of urban older adults patients with chronic diseases.
Method
Data
This study is a secondary analysis using cross-section data (CLASS). The China Longitudinal Aging Social Survey (CLASS) is a nationwide, continuous, large-scale social survey project. By regularly and systematically collecting social and economic background data of the older adults population in China, we can understand the various problems and challenges faced by the older adults in the aging process, evaluate the actual effects of various social policy measures in improving the quality of life of the older adults, and provide important theoretical and factual basis for solving China's aging problems. CLASS2020 was implemented in 2020. The survey covered 134 counties in 28 provinces in China. Samples were selected through a stratified multi-stage probability sampling method.
Variables
Table 1 presents a composite index system with two main categories: “Quality of life” and “Digital Use.” Under “Quality of life,” variables such as “General health” (weight: 0.313913) and “Social Function” (weight: 0.243041) have the highest weights, while “ADL” (weight: 0.046557) has the lowest. In the “Digital Use” category, “Internet Intensity” (weight: 0.365772) and “Number of Internet access purposes” (weight: 0.365814) are the most weighted variables.
Index system.
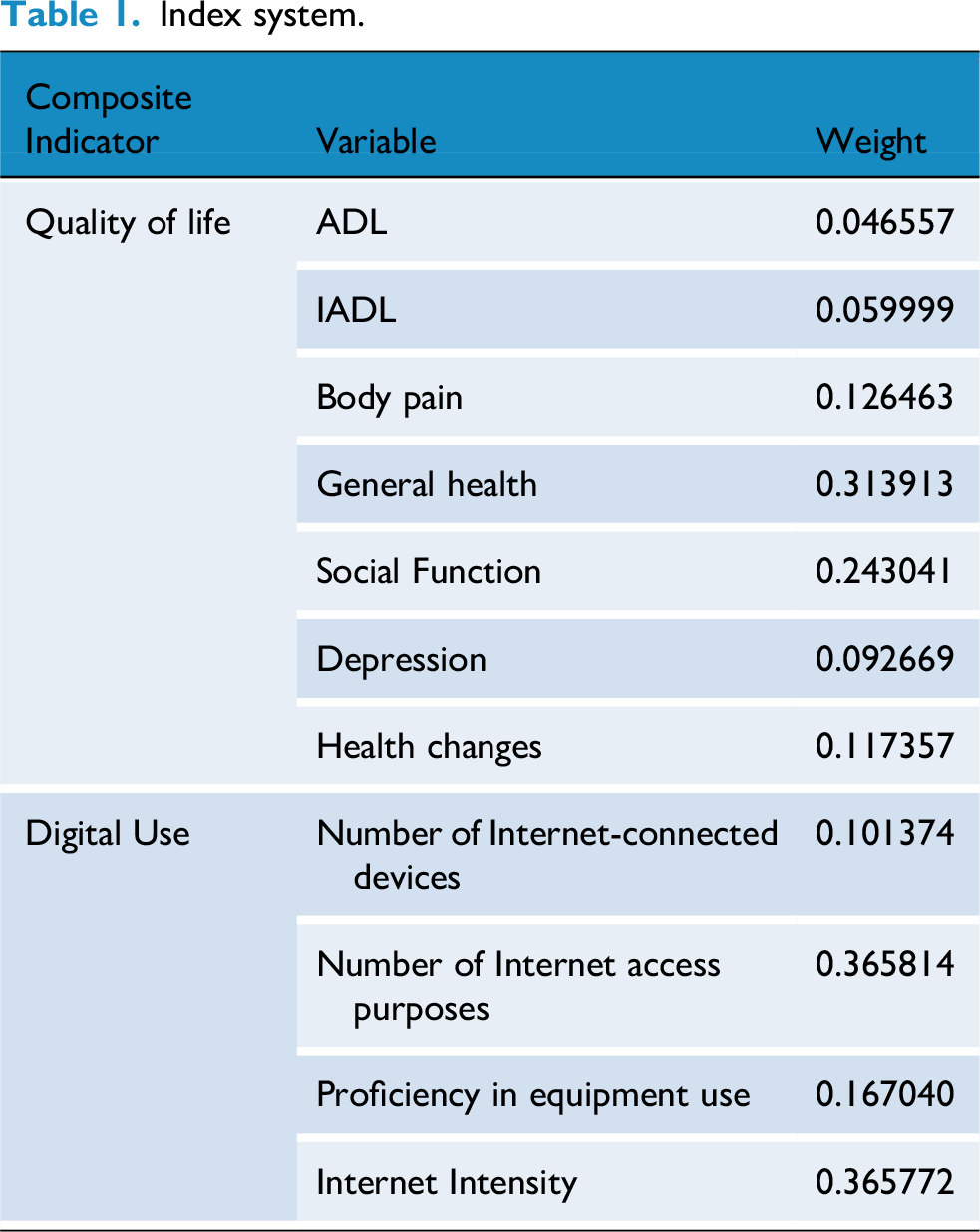
The following section presents an explanation of the variables under consideration. The central focus of this study is the quality of life of older adults patients with chronic diseases. The academic community typically employs the SF-36 scale to assess the quality of life of individuals. This scale comprises nine indicators and 36 questions pertaining to respondents’ physiological function (ADL), physiological function (IADL), physical pain, general health status, energy, social function, emotional function, mental health and health changes. While the CLASS questionnaire does not include the SF-36 scale, a substantial number of the items included in the SF-36 can be found in the CLASS scale. Accordingly, the Critic method is employed to assign weights to the items based on the SF-36 scale, thereby constructing a composite indicator of the quality of life of urban older adults patients with chronic diseases.
The following variables are used for explanatory purposes: The central explanatory variable of this study is the digital divide. In accordance with the findings of previous studies, 69 the digital divide is gauged using two key indicators: digital access and digital use. In accordance with the CLASS questionnaire, the question “Do you use mobile phones/computers to access the Internet?” is employed to ascertain whether the individual in question has digital access. In the event that any of the items is answered in the affirmative, digital access is assigned a value of 1, whereas if none of the items is used, it is assigned a value of 0. The answer to the question “Do you go online?” is then used to assign values from “never go online” to “every day” on a scale of 1 to 5. It is thus evident that the higher the value, the higher the intensity of online access. Finally, the answer to the question “What device do you mainly use to go online?” is used to assign values from 1 to 5. The number of online devices used by respondents is evaluated based on their responses to the question “How proficient are you in using these devices?” Values ranging from “very unskilled” to “very skilled” are assigned from 1 to 5, with higher values indicating greater proficiency in using online devices. The number of online purposes is determined based on the respondents’ answers to the question “What do you usually do when you go online?” Ultimately, the critical method is employed to assign weights to the number of online devices, the number of online purposes, the proficiency of device use, and the intensity of online access, thereby constructing a composite index of digital use.
Control variables: The dependent variables are gender (male = 1, female = 0), ethnicity (Han = 1, ethnic minorities = 0), marital status (married = 1, single, widowed or divorced = 0), and religious belief (having religious belief = 1, not having religious belief = 0). Political status (party members are assigned a value of 1 and others are assigned a value of 0); number of people living together; number of older adults-friendly service facilities in the community; whether taking part in exercise (taking part in exercise is assigned a value of 1 and not taking part in exercise is assigned a value of 0).
The role of mediating variables is to facilitate the understanding of the relationship between two or more variables. Formal social support is divided into two categories: pension and the number of formal security. The former is assigned a value of 1 if the respondent has a pension and 0 otherwise. The latter refers to the number of formal social security items besides the pension, including pension insurance, etc. The category of informal social support encompasses intergenerational economic assistance, quantified by the average amount of financial support provided by each child; intergenerational housework support, measured by the average extent of domestic assistance provided by each child; the frequency of face-to-face interactions between children and their parents, expressed as the average number of meetings per child; and the frequency of communication between children and their parents, indicated by the average number of contacts per child.
Moderating variables: This study employs three variables as moderating variables: tobacco use, accessibility of community services for older adults, and community facilities for older adults. The preceding article provided an explanation of the concept of community older adults facilities. The presence of tobacco use choices is determined by the prevalence of smoking (assigned a value of 1) and the absence of smoking (assigned a value of 0). The provision of accessibility of community services for older adults is quantified based on the number of services offered by the community.
Table 2 presents the descriptive statistics for the variables. The study sample focused on urban older adults with chronic diseases, with 879 samples obtained. Notably, the median for digital access is 0, showing over 50% of these older adults are not connected to the Internet. Despite urban digital infrastructure progress, a significant digital divide exists among them. The median of in-room network signal is 1, implying that their lack of Internet use is due to factors like reluctance to adopt new tech or health constraints, rather than digital infrastructure level. The median of community facilities availability for older adults is 2, indicating most urban communities have sufficient facilities for this age group, suggesting positive results from community-level active ageing policies. The median of urban accessibility of community services for older adults is 0, with a mean of 1 and standard deviation of 2.28, showing most communities can't offer adequate services while a few have more capacity, highlighting imbalances and deficiencies in accessibility of community services for older adults.
Descriptive statistics.

Model
In this study, the explained variable is the quality of life of urban older adults patients with chronic diseases. As this is a continuous variable, the multivariate OLS regression model is used for statistical analysis. Concurrently, given the relatively low proportion of older adults with digital access, the digital access and digital use dimensions of the digital divide are analysed separately.


Since several variables in this study were weighted using the CRITIC weighting method, the CRITIC weighting method is introduced below. First, the original data is standardized according to formula (3). If it is a negative indicator, the direction is converted using 1- 

Calculate the information content of the j-th indicator 
This study uses the propensity score matching method for robustness testing. The treatment group (above the mean) and the control group (below the mean) are set according to whether the independent variable is above the mean. In formula (6),
Result
Benchmark regression
Table 3 presents the findings of the baseline regression analysis. Models (1) and (3) respectively examine the impact of digital access and digital usage on quality of life, without the inclusion of control variables. The results demonstrate that digital access can enhance the quality of life of urban older adults with chronic diseases. This is a statistically significant finding at the 1% confidence level. The quality of life of urban older adults with chronic diseases who have achieved digital access is 0.1461 higher than that of their counterparts who have encountered the digital divide and have not achieved digital access. It can be posited that digital usage will have a detrimental effect on the quality of life of urban older adults patients with chronic diseases. For each additional level of digital usage, the quality of life of urban older adults patients with chronic diseases is reduced by 0.0391. The regression results obtained after the addition of control variables (models 2 and 4) are consistent with those of the baseline regression. The extant literature posits that digital usage may diminish the health status of older adults by impairing mental wellbeing. This, in turn, elucidates why a higher degree of digital engagement is associated with a poorer quality of life among urban older adults with chronic illnesses. It is noteworthy that in the regression model between digital access and quality of life, the presence of facilities designed with older adults in mind within the community is associated with a higher quality of life for older adults. This suggests that the positive effect of digital access on the quality of life of urban older adults with chronic diseases may not be due to digital access itself, but rather to the enabling environment that allows older adults to access digital resources.
Benchmark regression.

Note: *,**, and*** indicate significance at the 10%, 5%, and 1% levels respectively, and the robust standard errors in parentheses are the same below.
The results of employing the Poisson model for regression are presented in Models (5) and (6). Given that the dependent variable in this study is both continuous and count-based, the Poisson model was employed for robustness testing. The results are in alignment with the primary conclusions of this study, thereby substantiating the robustness of the study. The first hypothesis is as follows: The digital divide has a deleterious effect on the quality of life of urban older adults with chronic diseases.
Heterogeneity analysis
Table 4 presents the findings of the heterogeneity test. Models (1) to (4) respectively examine the impact of digital access and digital usage on the quality of life of male and female urban older adults patients with chronic diseases. The results demonstrate that, in general, the positive impact of digital access on the quality of life of urban older adults with chronic diseases is more pronounced for women than for men, whereas the negative impact of digital use on the quality of life of men is not statistically significant. This may be attributed to the fact that the average life expectancy and health status of men are lower than those of women. Therefore, older men are in better overall health than women, and thus the negative impact on mental health caused by digital use is less significant. Despite the vulnerability of urban older adults patients with chronic diseases to societal pressures, female urban older adults patients with chronic diseases are particularly susceptible. In conjunction with the aforementioned observation regarding environmental impact, this may signify that female urban older adults patients with chronic diseases who possess digital access are situated within a more advantageous social milieu.
Heterogeneity analysis.

The experience of work has a profound and far-reaching impact on the lives of older adults, influencing the course of their lives in significant ways. Working within the “system” refers to those samples employed in the public sector and relevant departments of the Chinese Communist Party. In China, work within the system has strong stability, low mobility and better social security. Models (5) to (8) respectively examine the impact of digital access and digital usage on the quality of life of urban older adults patients with chronic diseases, both within and outside the system. The impact of the digital divide on the quality of life of urban older adults patients with chronic diseases who were employed within the system prior to retirement is consistent with the baseline regression. However, the impact of the digital divide on the quality of life of urban older adults patients with chronic diseases outside the system is essentially insignificant. This may be attributed to sample selection bias, as the social security and benefits associated with working within the system are more advantageous. Conversely, workers outside the system who lack such welfare and social security may possess certain physical health qualities if they are able to survive to an advanced age. Additionally, the proportion of urban older adults who have worked within the system is relatively high, and the sample size is considerable. This may be attributable to the sample size.
Robustness test
This study employs the instrumental variable method and the propensity score matching method to conduct robustness tests. Instrumental variables need to be correlated and exogenous, the network signal in the room provides convenience for older adults in accessing the Internet, So it's relevant. Yet it does not directly affect the quality of their lives, so it's exogenous. This is consistent with the exogeneity and correlation characteristics of the instrumental variable. Table 5 presents the findings of the instrumental variable test. The results demonstrate that the KP rk LM value is as high as 280 and the Wald statistic is as high as 478, indicating that the network signal in the room is an effective instrumental variable and substantiating the robustness of the positive impact of digital access on the quality of life of older adults. However, as outlined in the descriptive statistics section, the mere presence of an Internet signal in the room does not guarantee its utilisation by older adults. Consequently, this instrumental variable can only substantiate the robustness of the positive impact of digital access on the quality of life of urban older adults with chronic diseases; it cannot be employed to elucidate the impact of digital utilisation.
Instrumental variable test.

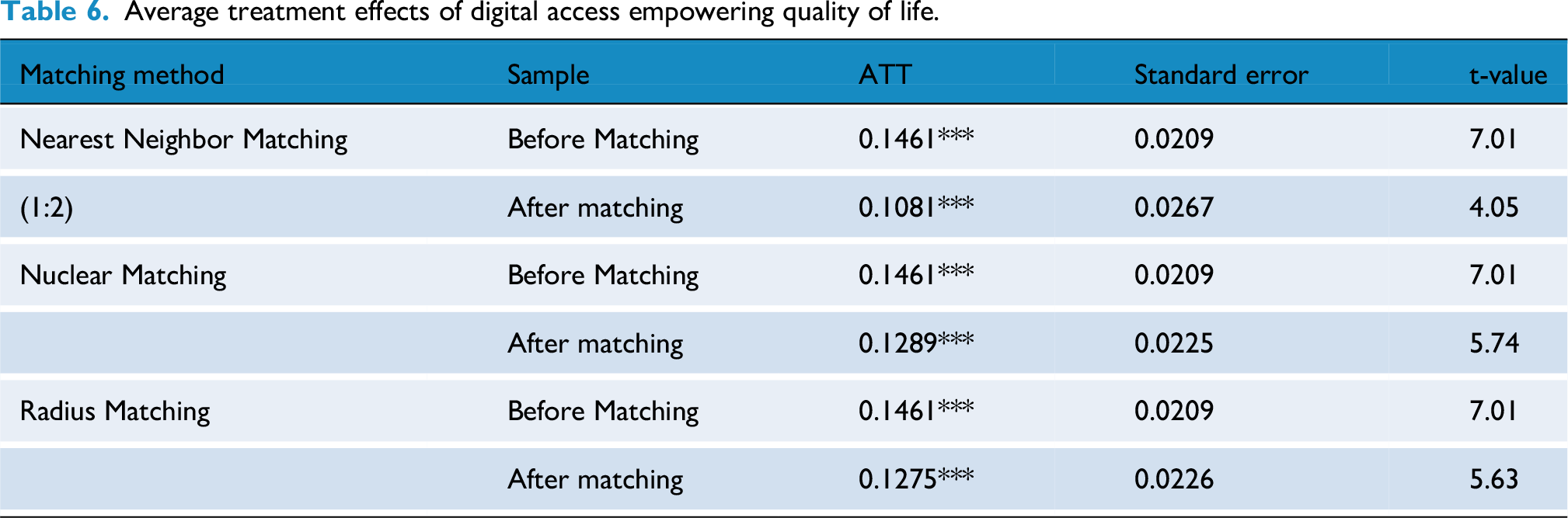
Propensity score value matching is a commonly employed method for identifying causal relationships in social research. Tables 6 and 7 respectively report the average treatment effect of digital access in enabling quality of life and the average treatment effect of digital use in reducing quality of life. In this instance, in-caliper matching is employed. The results demonstrate that the average treatment effect is statistically significant at the 1% confidence level, irrespective of whether nearest neighbour matching, kernel matching or radius matching is employed. This serves to demonstrate the feasibility, scientific rigour and rationality of the propensity score value matching method employed in the present study.
Average treatment effects of digital access empowering quality of life.
Average treatment effect of digital use on reduced quality of life.

Figures 2 and 3, respectively, present the alterations in the standardised deviation of covariates subsequent to kernel matching for digital usage and the modifications in the standardised deviation of covariates following radius matching for digital access. The results demonstrate that the standardised deviations of the majority of covariates exhibited a notable reduction following matching, reaching a final value of less than 10%. This outcome serves to reinforce the reliability of the primary conclusions drawn in this study.

Digital use_change of covariate standardization deviation after kernel matching.

Digital access_change of covariate standardization deviation after radius matching.
Test of mediating variables
In accordance with Hypotheses 2a and 2b, the bootstrap method was employed to assess the mediating influence of formal and informal social support. Table 8 presents the findings of the mechanism test. A 95% confidence interval was observed, and it was noted that the upper and lower bounds of the confidence interval had the same sign. This indicates that the mediating effect of formal social support and informal social support is established. The veracity of Hypotheses 2a and 2b was thus confirmed.
Mechanism test.
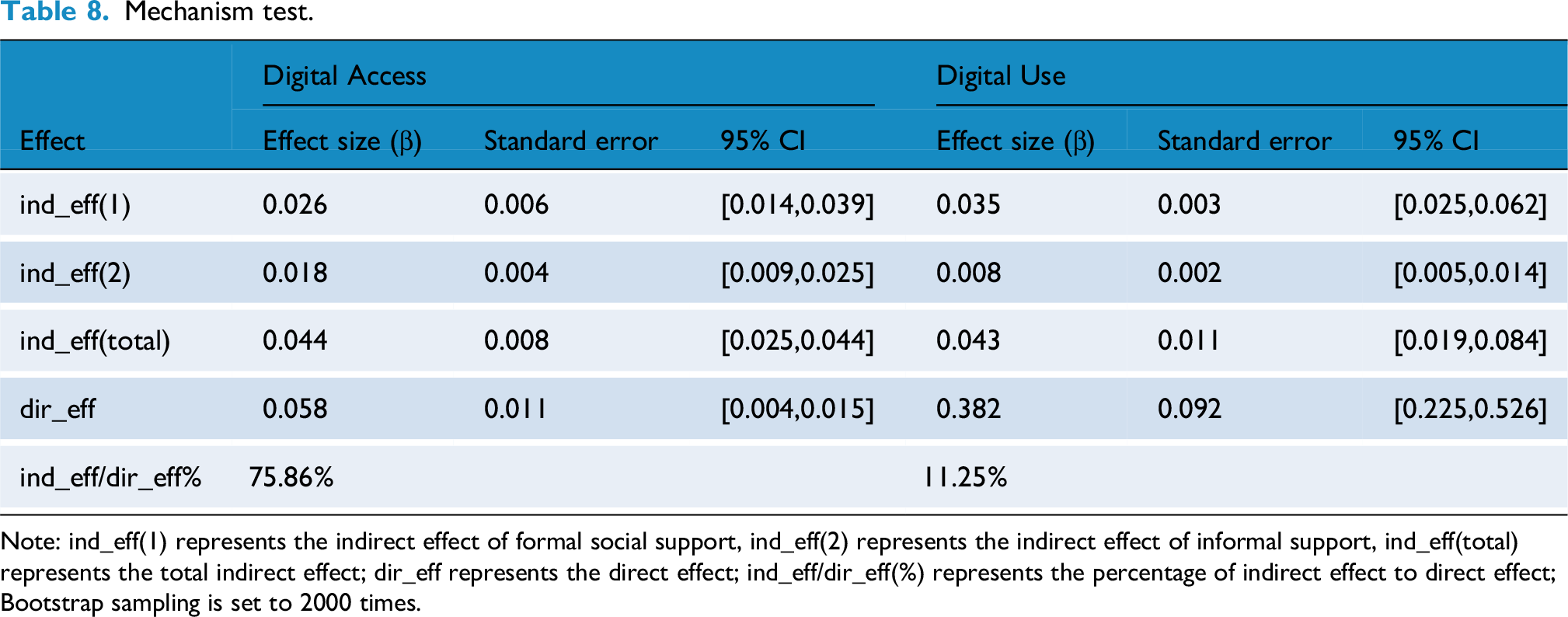
Note: ind_eff(1) represents the indirect effect of formal social support, ind_eff(2) represents the indirect effect of informal support, ind_eff(total) represents the total indirect effect; dir_eff represents the direct effect; ind_eff/dir_eff(%) represents the percentage of indirect effect to direct effect; Bootstrap sampling is set to 2000 times.
The effect sizes indicate that, in terms of the positive impact of digital access on quality of life, the impact of formal social support is more significant than that of informal social support. With regard to the negative impact of digital use on quality of life, the impact of formal social support is markedly greater than that of informal social support, which is almost negligible. In conclusion, the indirect effect of social support on the positive impact of digital access on the quality of life of urban older adults with chronic diseases accounts for 75.86% of the total effect, and is the primary mechanism through which digital access affects the quality of life. Digital access can assist urban older adults with chronic diseases in obtaining health and policy information, as well as facilitating communication with their children. However, it is logical that formal social security, such as pensions and pension insurance, should be determined prior to retirement. In light of the above, it can be posited that the positive impact of digital access on the quality of life of urban older adults patients with chronic diseases is essentially due to the social environment that enables these individuals to cross the digital divide. In conclusion, the indirect effect of social support on the negative impact of digital uses on the quality of life of urban older adults patients with chronic diseases accounts for 1.25% of the total effect, which is relatively minor. In conclusion, the impact mechanism of the digital divide on urban older adults patients with chronic diseases is primarily concerned with the dichotomy of “have or not” rather than the quantity of social support. As long as the digital divide is overcome, it is possible to obtain greater levels of social support. Nevertheless, for urban older adults patients with chronic diseases who have crossed the digital divide, utilising the Internet more frequently does not facilitate the acquisition of additional social support. Such individuals may even possess a more profound comprehension of their own chronic illnesses, having accumulated an excess of health-related data. Such circumstances may precipitate a state of psychological distress and adversely impact mental health.
Test of moderating variables
Hypotheses 3a, 3b and 3c posit that poor lifestyle choices, the availability of community services and the quality of community facilities may serve to mitigate the adverse effects of the digital divide on the wellbeing of older adults in urban areas with chronic health conditions. The pertinent variables are initially centred and subsequently incorporated into the regression model for the purpose of testing the moderating variables. Table 9 presents the findings of the moderator variable test. Model (1) assesses the moderating impact of poor lifestyle habits on digital access. The primary effect is positive and statistically significant, while the cross-term coefficient is negative and statistically significant. The findings indicate that poor lifestyle choices have a beneficial effect on digital access, thereby empowering urban older adults with chronic diseases. The quality of life is found to have a detrimental effect. This is because poor lifestyle choices themselves have a detrimental impact on quality of life. Therefore, although bridging the digital divide can enhance the quality of life of urban older adults with chronic diseases, it has been undermined by poor lifestyle choices. Model 2 assesses the moderating impact of poor lifestyle choices on digital engagement. The primary effect is negative and statistically significant, as is the cross-term coefficient. The findings indicate that poor lifestyle choices have an adverse impact on the quality of life of urban older adults with chronic illnesses who engage in digital activities. The effect is one of weakening. In other words, poor lifestyle choices serve to mitigate the adverse effects of digital engagement on quality of life. The preceding analysis and the conclusions of extant research indicate that the adverse impact of digital use on the quality of life of older adults is primarily exerted through a detrimental effect on their mental health. In this study, smoking was used as a proxy for other unhealthy lifestyle habits. The act of smoking has been demonstrated to have a relaxing effect on the mind and a stress-relieving impact, which may serve to mitigate the negative impact of digital use on quality of life. The third hypothesis was confirmed.
Test of moderating variables.

Model (3) assesses the moderating impact of accessibility of community services on digital access. The primary effect is positive and highly significant, while the cross-term coefficient is negative and highly significant. The findings indicate that accessibility of community services serve to mitigate the impact of digital access on the wellbeing of urban older adults with chronic illnesses. The effect of empowerment on quality of life. This may be attributed to the fact that external factors are constrained in their ability to enhance the quality of life of urban older adults with chronic illnesses. It is evident that the quality of life of this demographic cannot be indefinitely augmented. It can therefore be concluded that if accessibility of community services enhance quality of life, the extent to which the digital divide can positively impact quality of life is minimal. The third hypothesis was confirmed. Model 4 examines the moderating effect of accessibility of community services on digital usage. The primary effect is not statistically significant, while the cross-term coefficient is negative and highly significant. In the event that the main effect is not significant, it is recommended to refer to the baseline regression. The findings indicate that accessibility of community services can mitigate the adverse effects of digital usage on the quality of life of urban older adults with chronic illnesses. This is due to the fact that accessibility of community services has the capacity to enhance the quality of life of older adults, thereby exerting a “replenishment” effect. . Models (5) and (6) respectively test the moderating effect of community facilities on digital access and digital usage, and yield results that are consistent with those observed for accessibility of community services. The veracity of Hypothesis 3C, which will not be discussed in detail here, has been confirmed.
Discussion
This study makes three notable contributions to the field. Firstly, it is the first to explore the impact of the digital divide on urban older adults with chronic diseases from the perspective of quality of life. Secondly, it applies the SF-36 scale structure to digital divide-related fields, and thirdly, it further discusses the influence of the social environment based on the discussion of the impact of social support in existing studies. The results of the mediating variable test indicate that the impact of the digital divide on the quality of life of urban older adults with chronic diseases is achieved through the social support mechanism, including the influence of formal and informal social support. The moderating variables were tested, and it was found that poor lifestyle choices, inadequate accessibility of community services and facilities will diminish the beneficial impact of digital access on the quality of life of urban older adults with chronic diseases, and reduce the positive effect of digital use on the quality of life of this demographic.
Prior research has concentrated on the dual-edged sword effect of the digital divide on the health of older adults. This study demonstrates that the impact of the digital divide on the quality of life of urban older adults with chronic diseases is also two-sided. This duality is evidenced by the disparate effects of digital access and digital use on the quality of life of older adults with chronic diseases. While digital access has been shown to enhance the quality of life of urban older adults with chronic diseases, digital use has been demonstrated to have a detrimental impact on this same quality of life. Despite the prevalence of digital infrastructure in urban areas, with the majority of rooms equipped with a network signal, older adults continue to encounter challenges related to the digital divide. 70 Furthermore, this study revealed that the beneficial impact of digital access on the quality of life of urban older adults with chronic diseases is not solely attributable to digital access itself, but rather to the social environment that facilitates the older adults’ navigation of the digital divide. The moderating effect of community-friendly facilities for older adults and community older adults services also demonstrates the significance of the community environment within the social environment for the quality of life of older adults with chronic diseases. 71
While existing research has emphasised the role of the family environment on the health of older adults and across the digital divide, the impact of formal social support on urban older adults patients with chronic diseases is significantly greater than that of informal social support. 72 This may be attributed to the fact that the life course of older adults in urban society is shaped by significant institutional factors, including a controlled society and a planned economy (over half of the older adults patients with chronic diseases in the sample were employed in the system prior to retirement), which tend to accentuate the role of formal support. Currently, the Chinese government places an emphasis on community-based home care for older adults. Additionally, there is a growing trend in the older adults care system to integrate informal social support with formal social support. Consequently, this situation may undergo a transformation in the future. Conversely, rural areas receive less formal social support. Further research is required to gain a deeper understanding of the impact of the digital divide on older adults patients with chronic diseases in rural areas, as well as to identify the similarities and differences between this group and their urban counterparts.
While our findings are grounded in China's unique socioeconomic context, the dual-edged impact of digital access and usage aligns with global patterns. For instance, longitudinal study in Brazil shows that some older adults are addicted to online social networking, which leads to alienation of real interpersonal relationships, anxiety and hostility. 73 The mediating role of formal social support echoes Germany's emphasis on state-funded older adults care systems, 74 whereas the moderating effect of accessibility of community services resonates with Japan's “Community-Based Integrated Care System”. 75 These parallels suggest that policymakers worldwide must balance technological accessibility with safeguards against digital overuse.
The findings indicate that accessibility of community services play a pivotal role in offsetting the potential adverse effects of digital usage on the quality of life of urban older adults with chronic illnesses. Accessibility of community services can markedly enhance the quality of life of older adults by furnishing them with professional care, support and social activities. This improvement can, to a certain extent, offset the negative effects caused by insufficient or inappropriate use of digital technology. 76 In particular, the “replenishment” effect of accessibility of community services is manifested in the following domains: social interaction and emotional support. Accessibility of community services may assist older adults in establishing and maintaining social relationships, thereby reducing feelings of loneliness and social isolation. This is achieved through the organisation of activities and the provision of communication opportunities. This consequently enhances life satisfaction.77,78 The provision of professional care and support to older adults in the community typically encompasses a range of specialized services, including medical care, rehabilitation, and psychological counseling. Such services are capable of effectively managing the health issues of older adults, providing essential care and support, and enhancing their physical and mental wellbeing, convenience, and personalised service. Community-based older adult care services can provide convenient services to meet the needs of older adults, including home care, regular health examinations, and shopping services.
Conclusion
In light of the social context of the accelerated growth of the digital economy, the information society, the declining birthrate and ageing population, and the expansion of chronic disease groups, this study employed the C LASS2020 data set to investigate the impact of the digital divide on the quality of life of urban older adults with chronic diseases and its underlying mechanisms. The findings were subjected to rigorous robustness tests. The findings of the study indicate that digital access has a positive impact on the quality of life of urban older adults with chronic diseases, whereas digital use has a detrimental effect on the quality of life of this demographic. The results of the heterogeneity analysis indicate that the impact of the digital divide on the quality of life of urban older adults patients with chronic diseases is significant for women and pre-retirement workers within the system, but essentially insignificant for men and pre-retirement workers outside the system.
The use of digital technologies can significantly enhance the quality of life for urban older adults with chronic diseases, while digital use may also have adverse effects. This heterogeneity may stem from deficiencies in the age-friendly design of digital technologies themselves, which consequently prevents some older adults from benefiting from digital tools, while others struggle with digital addiction among older adults. This suggests that policymakers could encourage age-adaptive innovations in digital technologies and implement universal smart care for older adults. For instance, providing national subsidies for purchasing intelligent older adults care devices and offering special tax deduction quotas to manufacturers producing digitally inclusive devices tailored for older adults.
It must be acknowledged that this study is not without shortcomings. Firstly, the instrumental variable of room network signal is only applicable to digital access. This study did not identify an appropriate instrumental variable for digital use, therefore only the instrumental variable test for digital access was conducted. Secondly, the CLASS2020 dataset does not include the SF-36 questionnaire. Despite the development of an indicator system for measuring the quality of life of urban older adults patients with chronic diseases based on the SF-36 questionnaire structure and the CLASS questionnaire, the rigour and completeness of this study remain inferior to those of the SF-36 questionnaire. Furthermore, the CLASS2020 dataset is cross-sectional data. Consequently, despite the implementation of multiple treatments and robustness tests for endogeneity issues, the possibility of residual endogeneity remains.
Future research could use panel data to conduct cohort studies looking at the long-term impact of the digital divide on the quality of life of older adults; Or COX proportional risk models can be used to observe the effect of digital divide on disability risk in older adults.
Footnotes
Acknowledgements
Thanks to the Aging Research Base of Lanzhou University for their help in this study.
Ethics considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Authors’ contributions
Zhang Chi: Conceptualization, Funding acquisition, Writing, Methodology, Project administration, Visualization; Longxuan Lin: original draft, Writing, review & editing.
Funding
This work was supported by the Fundamental Research Funds for the Central Universities (2024lzujbkyqk006). Gansu Province Philosophy and Social Science Planning Project (2024QN005). The research is also supported by Ministry of Education Humanities and Social Sciences Research Project, Grant No. 25YJC840028.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability and consent statement
The data used in this study are from the China Longitudinal Aging Social Survey (CLASS2020), which is a publicly available dataset. Data acquisition platform for figshare (DOI: 10.6084/m9.figshare.29051138), during the data collection and use the data set has passed the formal academic channels open sharing, without access to individual level of informed consent. The research team strictly adheres to the terms of service and data usage norms of the figshare platform. All data operations comply with academic ethics requirements.
Guarantor
Not applicable.
AI disclosure statement
The conception, data processing, analysis and writing process of this research manuscript were all independently completed by the authors, without using any artificial intelligence (AI) tools for content generation, editing or data processing. This is hereby declared.