
Abstract
It is well accepted that the preferred place of care for many people is in their own homes and that home care services have the potential to allow people to remain in their own homes for as long as possible. This narrative review aimed to summarize the existing literature on person-centered practices in home care and develop a conceptual framework, based on The Health Information and Quality Authority’s (HIQA) standards development principles, to achieve high-quality person-centered home care. A narrative review was conducted using the academic databases Embase, APA PsychInfo, Social Services Abstracts and CINAH. A qualitative content analysis was used to analyze and synthesize the findings. In total 39 studies were included in this narrative review. This review emphasizes four key principles for person-centered home care. A human-rights based approach ensures care is delivered with dignity, respect, and non-discrimination, guaranteeing equitable access for all. The safety and wellbeing principle focuses on preventing health decline and harm, while promoting the overall well-being of the care recipient. Responsiveness centers on how staff identify and address individual needs, with their skills and competencies playing a crucial role. Finally, the accountability principle underlines the importance of strong leadership, clear governance, and effective collaboration between home care and other services. The approach of using principles as a framework to underpin this study can inform policymakers, home care providers and others in good practice in upholding person-centered care during the development of home care policy and care delivery.
Introduction
It is well accepted that the preferred place of care for many people is in their own homes, for as long as is possible. 1 Demographic challenges, trends towards increasingly complex care and support being provided in the home, and the need to focus on a person-centered care approach that facilitates autonomy and choice, underline the need to develop alternative models of care and support to meet the needs of this population.1,2 Home care services provided by formal carers, which refers to paid care provided by home support providers, 3 have the potential to allow people to remain in their own homes for longer and also has added protections in the context of prevention of infection.1,4 A person-centered care approach has service users at the core of the service, and can be achieved by “actively involving them in the provision of care”. 5 This includes respecting their preferences, needs and values, and ensuring that service users receive high-quality, safe care that is consistent and coordinated. 5 Research has shown that the provision of home care services that meet the services users’ needs minimizes the decline of health and function, increases independence, and promotes quality of life.6 -8
Within the health and social care sector, there is a clear move in a number of countries towards setting out guiding principles for regulatory frameworks. These principles can be understood as fundamental values or goals that are needed to underpin person-centered care, regardless of the service setting or type. 5 In line with emerging international evidence, the Health Information and Quality Authority (HIQA) has developed a set of core principles informed by an evidence review to use as a framework to develop all national standards for health and social care services in Ireland.5,9 The set of four principles—a human-rights based approach (HRBA), safety and wellbeing, responsiveness and accountability—are intended to work together, and collectively describe how health and social care services provide person-centered, safe, consistent, and integrated care and support. 9
Increased knowledge of these principles in the context of home care services will inform policymakers, health and social care professionals and home care providers on the creation of safe, consistent, and coordinated home care services, where people and their families are involved in decisions around their care and support, and organizations and individuals work towards achieving the best outcomes for the person using services.5,10 This narrative review aimed to summarize the existing literature on person-centered practices in home care and to develop a conceptual framework, to achieve high quality person-centered home care. This narrative review was guided by the research question: What evidence from the literature identifies characteristics of good person-centered practices in home care services, where people experience safe, high quality outcomes from the care, and support they receive in their home?
Methods
This narrative review is part of the evidence review developed by HIQA to inform the development of National Standards for Home Support Services. HIQA’s evidence synthesis procedure is published in the Evidence Synthesis Process: Methods in the development of National Standards, Guidance and Recommendations for the Irish Health and Social care Sector. 11
Search Strategies
The research question for this narrative review was guided by the PICo framework (population, phenomenon of interest, and context). 12 The search was limited to published studies from 2010 to early 2021, to build on the previous systematic review published by Genet et al 4 in this area, which reviewed studies up until 2010. The literature search was conducted in May 2021 using the academic databases Embase, APA PsychInfo, Social Services Abstracts, and CINAHL and updated in February 2023; findings and conclusions were adjusted as appropriate.13,14 The returns were catalogued according to the type of article and the source of the article. A combination of search terms was used; these related to the population (e.g., “adult,” “aged,” “older,” “elderly,” “service-user”; setting (e.g., “household,” “domestic,” and “community”) and the topics of interest (e.g., “homecare,” “home support,” and “home help”). The full list of terms used to search the academic databases is presented in Supplemental Appendix A. All results derived from the search strategy were imported to the Covidence systematic management software for the screening phase.
Eligibility Criteria
This narrative review included quantitative, qualitative, and mixed methodologies. The following exclusion criteria were applied at three stages of study selection (screening by title, screening by title and abstract, and during the assessment of the full text), documents focusing on settings outside of scope (e.g., hospital settings), documents focusing on developing countries, books, book reviews, editorials, and letters. This narrative review inclusion and exclusion criteria are presented in Supplemental Appendix B. In the screening phase, five researchers (CB, MW, YK, JG, and DM) conducted initial title and abstract screening for potential inclusion, using a researcher agreement chain, where one researcher reviews articles for initial inclusion. Articles marked as “unsure” were independently reviewed by a second reviewer before a decision was made. Any outstanding conflicts were then resolved by a third reviewer. 12
Data Analysis
The software Microsoft Excel was used to record the data extracted, which contained information of interest, such as the authors, publication date and country, study aim, study design, population, principles, and related concepts. In this narrative review, we used a predefined framework to code relevant data from the selected articles, which reflect the principles used by HIQA to underpin all national standards. The researchers (CCB, MW, DM, and YK) mapped the data according to these principles of a Human rights based approach, safety and wellbeing, responsiveness and accountability, and recorded it in the data extraction table. Once completed, the data extraction was reviewed by another researcher (JG) to ensure that they reflected these principles in the context of home care services. Once mapping was completed, a narrative synthesis approach was used to identify patterns and connections in the coded data.15,16
Results
Search Results
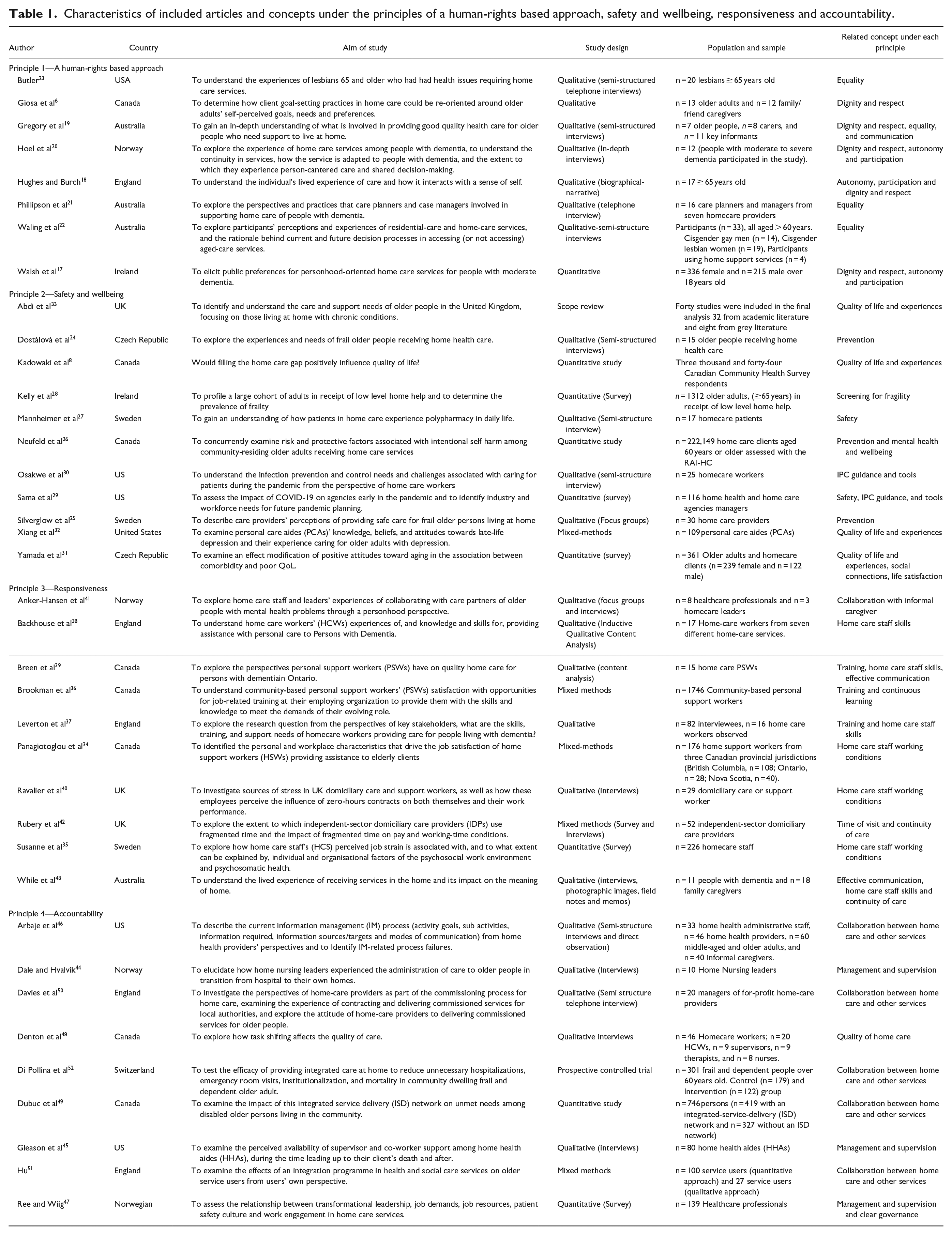
A flow chart of the selection process for relevant literature is presented in Figure 1. From the database search 25,454 articles were returned. Following the removal of duplicates, 20,127 documents were identified for inclusion in the screening phase. Eight papers were identified from citation searching and included in the full text screening phase. A total of 39 articles were identified for inclusion in this narrative review following a review of full texts. The characteristics of the included articles and related concepts under each principle are presented in Table 1.
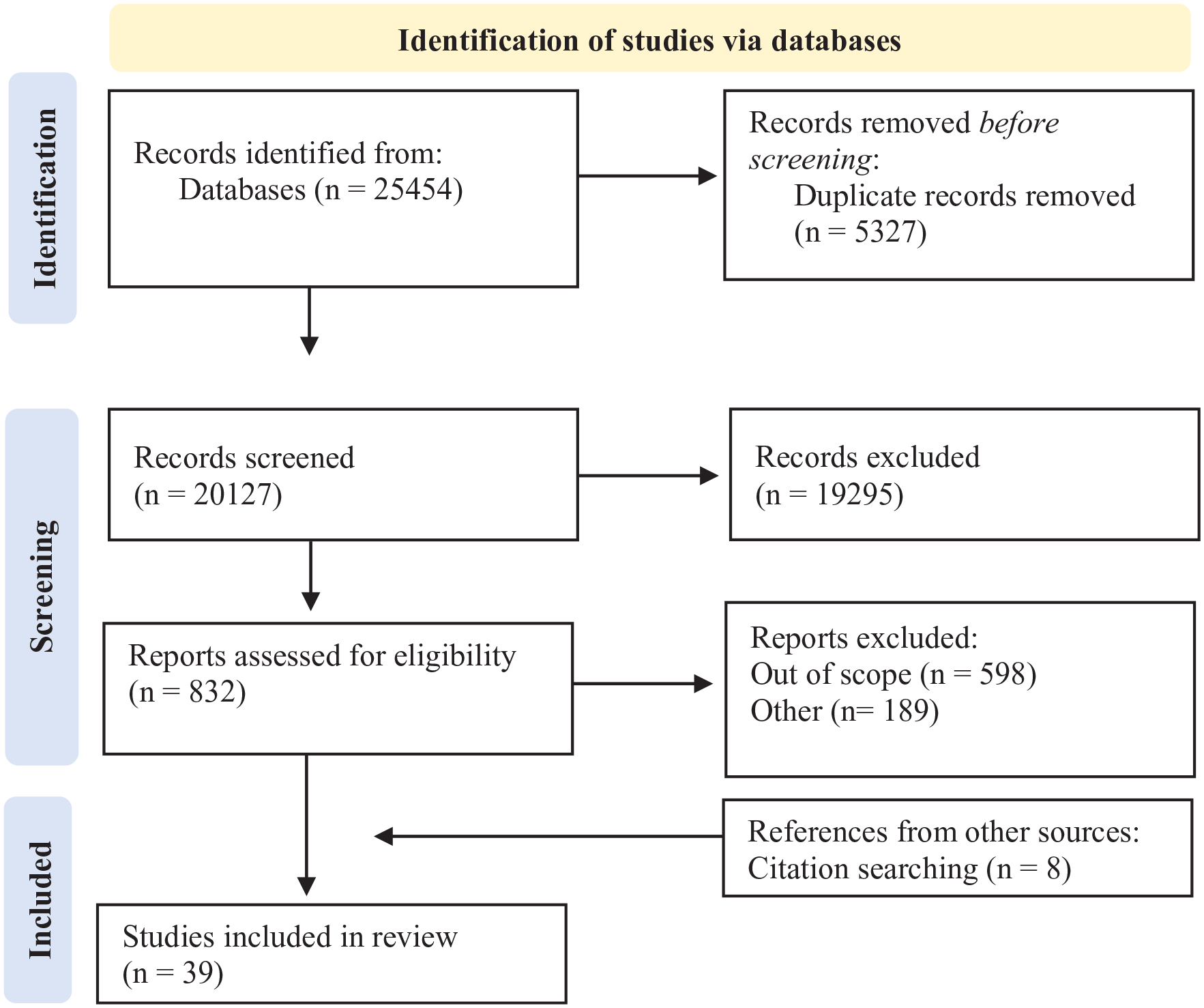
Flow chart of the included articles.
Characteristics of included articles and concepts under the principles of a human-rights based approach, safety and wellbeing, responsiveness and accountability.
A Human Rights-Based Approach in Home Care Services
It is widely recognized that applying a HRBA to home care promotes a person-centered, safe and quality service.17 -19 Eight studies were categorized under the HRBA principle in this narrative review. The literature shows that within the principle of a HRBA, dignity and respect are at the core of person-centered care.17 -19 In home care services, dignity and respect means incorporating service users’ knowledge, values, beliefs and cultural backgrounds into their care planning and delivery of care.6,20 However, three studies reported challenges in fully involving service users in their own care, particularly those with functional or cognitive impairments.19 -21 These studies suggested that this might be due to a lack of appropriate information that meets service users’ needs 20 and time constraints. 19 According to Giosa et al 6 respect and dignity can be protected by avoiding ageism and ensuring effective communication during care planning, focusing on goal-setting to protect older people’s capacity and promote their independence. 6 In addition, presenting clear options of care to those with dementia can also improve the design of a care plan. 21
Autonomy as a HRBA to care is defined as having control over one’s life and day-to-day living. Hughes et al 18 described autonomy as both “decisional” which refers to the ability to make decisions independently and “executional” which is the ability to carry out these decisions independently. 18 Home care services can support and promote both aspects of service users’ autonomy and participation by involving them in decisions regarding their care plan and facilitating their independence. 19 However, studies have reported situations where home care workers complete a task on behalf of the person, as opposed to supporting the person to do the task themselves.17 -19
Studies also highlighted the importance of equality in home care provision and that service providers need to create a culture of non-discrimination.19,22,23 Studies showed that ethnic minority populations 19 and lesbian women aged over 60 years 22 face significant challenges in accessing home care services for a variety of reasons, including for example language barriers, a lack of accessible information, low health literacy or lack of trust in the services. 19
Safety and Wellbeing in Home Care Services
Safety and wellbeing as a principle relates to safeguarding the service user, the prevention of harm, and the quality of life of a person while they are accessing home care services. 5 The literature relating to “safety and wellbeing” consisted of 11 studies. Studies emphasized that to provide safe home care services, there is a need to understand and assess service users’ underlying physical and psychological condition, including multiple comorbidity, cognitive impairment, and polypharmacy.24 -27 An Irish study that associated frailty levels with a greater number of home care hours recommended incorporating frailty measures into community services, including home care services and re-ablement services, to detect and prevent deterioration at an early stage. 28 Studies that explored the experiences and needs of frail older people receiving home care services reported that participants associated safe home care with staff education and experience, their ability to provide health information and advice, and continuity of care.24,25 However, service users, home care providers, and staff faced challenges during the Covid-19 pandemic, including a lack of infection prevention and control (IPC) guidance, tools, and training tailored for the home care sector, leading to unmet service user needs, greater burnout of informal caregivers, and feelings of unsafety by both home care staff and service users.29,30 In addition, the mental wellbeing of the person receiving home care services may also pose a threat to their personal safety. Studies have highlighted the importance of identifying patterns and risk factors associated with intentional self-harm or suicidal behavior in clients.31,32
Home care services can have a significant impact on service users’ wellbeing. For instance, being able to maintain social connection and activities is a key component of healthy ageing and increased quality of life. 31 As people begin to experience physiological limitations such as sight loss, hearing loss, difficulties with memory or limited mobility, they tend to lose the ability to sustain relationships and become increasingly dependent on their close relatives and carers for daily socializing and mental stimulation. 33 In addition, a Canadian study showed that older adults whose home care needs were being met, had significantly higher levels of life satisfaction, and lower levels of loneliness and stress, compared with older adults whose home care needs were not being met. 8
Responsive Home Care Services
In total 10 studies were categorized under the principle of responsiveness. The principle of responsiveness was identified in the literature as the way in which home care staff respond to a person’s needs, and how their abilities, duties and competencies facilitate this. However, the evidence shows a high turnover of home care workers due to low job satisfaction and working conditions, such as zero-hour contracts and irregular work hours.34,35 In addition, home care worker’s skills and knowledge emerged as a challenge in the provision of person-centered care.36,37 The lack of training and qualification requirements for home care workers leads to high staff turnover, a breakdown in continuity of services, and a reduction in the quality of care provided, especially for people with dementia.37 -39 According to Leverton et al, 37 to assist people with dementia, home care workers need skills and training on how to manage challenging behaviors, and dealing with complex attachments such as lack of professional boundaries between home care workers and service users and their family, and effective communication. 37 In addition, shortage of home care workers, coupled with a lack of qualification requirements for the role, leads to employees being recruited at short notice without proper examination of their competence and skills, and without providing sufficient training or induction to their role. 40 Time constraints also emerged as a barrier to delivering a high quality and responsive home care services.41,42 In addition, timing of home care visits was found to be crucial to the quality of care and the level of satisfaction of the person using the service, and a poorly-timed visit or missed appointment could have negative impacts on the person’s day, quality of care delivery and their continuity of care. 42
Effective communication and collaboration play a crucial role in ensuring responsiveness in home care services. This requires home care staff to communicate openly and transparently with the people receiving the service and their families while working together. In addition, the literature also described the potential barriers that professionals face in collaborating with people receiving care and support at home, for example a situation where a service user or family member may be rude, aggressive, or even violent. 40 However, poor communication practices at the organizational level can also lead to dissatisfaction and unmet needs among individuals receiving care at home. 43 Studies showed that the relationship between formal and informal caregivers can be conflicting. This is due to a lack of communication and deficiencies in providers’ flexibility and structure for collaboration with informal carers, resulting in unmet expectations. 41
Accountable Home Care Services
Under the principle of accountability 10 papers were identified. Accountable home care services should have a clear vision for their work. They should support their staff to deliver on this vision, work well with other relevant services, and regularly assess the impact of their work on those they are caring for and supporting. 9 In home care services, managers and supervisors are responsible for the coordination and quality of the care and support provided.44 -46 However, in a study of 226 home care workers, the majority reported that they did not have sufficient support from management to develop their skills. They also reported that managers had no interest in their health and wellbeing, which in turn was associated with higher job strain. 35 Studies highlighted that the role of manager and supervisor extends beyond personnel and financial management.44,45,47,48 Managers are also responsible for creating relationships and motivation among home care workers, 47 strengthening the service’s quality and culture, encouraging and supporting teamwork, and supporting home care workers emotional health.35,45
Home care providers must be able to collaborate with a range of services and health and social care professionals.46,49,50 In this context, home care providers and other health and social care services should be open to developing structures and systems that improve information management and the sharing of service users’ data confidentially within and between services.46,49 However, the variation across services and the transition of care from hospital to home may lead to inconsistent and inefficient information sharing between services. 51 This can result in unmet needs for service users, avoidable hospitalization or re-hospitalization, increased visits to hospital emergency departments, premature nursing home placement and consequent increase of healthcare costs. 52
Conceptual Framework
Based on the findings from this narrative review, a conceptual framework of how to achieve person-centered care in home care services was developed (Figure 2).
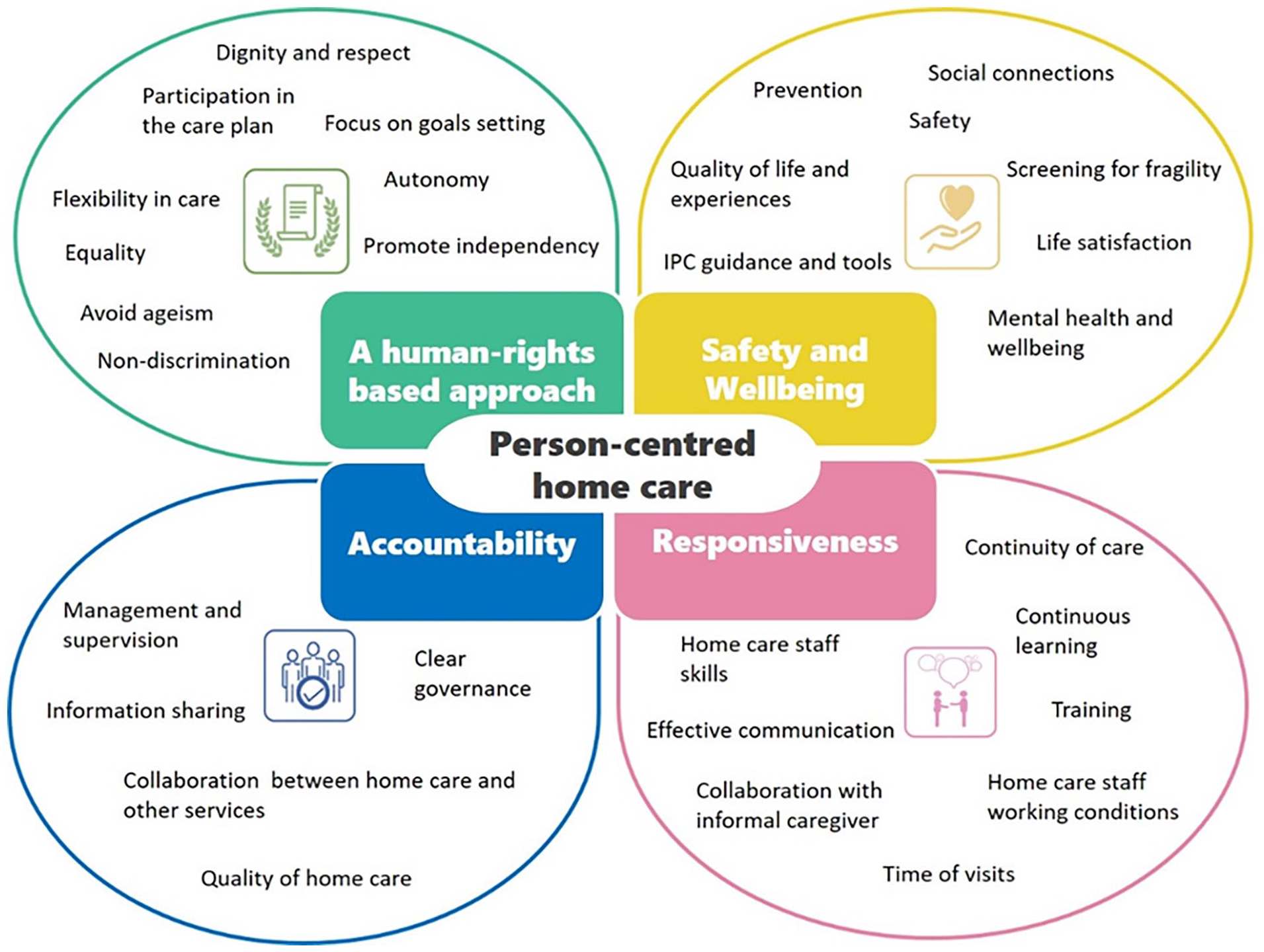
Conceptual framework of how to achieve person-centered care in home care services.
The concepts underpinning the principle of a human rights based approach emphasize the importance of dignity, respect, autonomy, participation, and non-discrimination in the delivery of person-centered care. Service users’ values, beliefs, and cultural background are central to care planning and delivery. Communication is clear, respectful, and avoids ageism.
In terms of safety and wellbeing, the literature highlighted the importance of preventing health deterioration, focusing on preventative measures to reduce the risk of acute illness or injury caused by fragility. The ability to remain socially connected was also emphasized.
Characteristics of responsive and person-centered home care services include having competent staff who are skilled and who collaborate and communicate openly with families and people receiving support, in order to bring about the best outcomes for them. Staff training is provided, especially in dementia care. Flexible visiting times are offered to meet the service users’ needs.
The principle of accountability emphasizes the importance of having a clear vision and mission to guide service delivery. Managers should cultivate a positive work environment and teamwork, and ensure that staff receive adequate support for professional development. Ongoing monitoring and evaluation are crucial for continuous quality improvement.
Overall, the framework aims to ensure home care services empower individuals, promote their independence and wellbeing, and uphold their human-rights. Strong leadership and governance structures are essential for organizations that provide person-centered home care services.
Discussion
This narrative review aimed to synthesize characteristics of person-centered practices in home care services and to develop a comprehensive conceptual framework based on HIQA’s set of four principles—a HRBA, safety and wellbeing, responsiveness, and accountability. This narrative review highlighted how these principles provide a consistent and meaningful framework to improve the quality of care throughout the home care sector. This involves respecting service users’ dignity, creating flexible care plans, involving people, and their families in decisions around their care and implementing clear governance.
However, the literature highlighted challenges to achieving person-centered home care, such as challenges faced by home care workers in fully involving service users in their care planning and delivery, due to workload, time constraints and lack of training, education, and skills. The working conditions for homecare staff and the shortage of home care staff also negatively impact the ability of home care services to meet service users’ needs. Studies suggested that workforce planning and staff retention are essential for delivery and sustainability of person-centered home care services. This can be achieved through professional regulation, access to training, and flexible care delivery models.34,40,53,54 In addition, research has shown that home care managers and supervisors play a key role in developing staff skills, supporting their health and wellbeing and encouraging the positive organizational culture which is associated with high-quality delivery of care.44,48
It emerged from the literature that home care workers often experience constraints relating to duration and timing of visits, which might lead to a task oriented model of care, resulting in poor quality of care and unmet service users’ needs.41,42,55 -57 Similarly, Hughes et al 18 suggested that inflexible care and task-centered services were often perceived as rushed, with carers having little time to actually chat to the person, leaving the service user with a sense of being undervalued and hindering their sense of autonomy. 18 To provide person-centered home care it is essential to provide sufficient time for visits, enhancing communication and collaboration between home care staff, service users and family care. While involving the family of the person receiving care and support at home may help with responsiveness, the relationship between formal caregivers and family members can sometimes be challenging. 41 Thus, there is a need to create a structure for collaboration with informal carers and ensure that the care provided by formal and informal caregivers complement each other, to enhance the quality of life for service users and their families.41,55
This narrative review also highlighted that there is inconsistent and inefficient collaboration between home care services and other health services. Similarly, an integrative review that evaluated the discharge communication between the hospital and home healthcare agencies reported limitations such as issues with discharge documentation (e.g., too much or too little information), lack of trust between services and lack of mutual communications. 58 Perhaps these findings highlight the need for a clear governance framework that facilitates open communication between organizations, working together with professionals from other disciplines and inter-agency collaboration. 33 This governance framework includes the collection, organization, and communication of the service users’ needs, health status and care plans.33,46
Overall, person-centered home care should create equal opportunities for all people using the service, allowing them to remain socially connected to their community, family, and friends, which positively impacts their safety and overall wellbeing. Efforts to maximize a service user’s quality of life should not just focus on enabling them to perform routine tasks independently within their homes, but should also focus on maintaining their social connectedness. Conversely, if people were treated in a manner they perceived as being “demeaning,” with lack of regard for the person’s individuality, this resulted in de-personalized care. 18 Therefore, just because care is delivered in the home does not mean that it should immediately be assumed to be “person-centered” without regard for the individuality of the person. 18
Before drawing a conclusion, the study’s strengths and limitations must be considered. A particular strength of the study was the systematic approach used to search and screen the literature for this narrative review. One limitation is the risk that relevant articles may be omitted. While the focus of the review is not on exhaustiveness, efforts were made to reduce this risk by utilizing multiple sources to identify articles. In addition researchers whose knowledge base is the development of standards and guidance, interacted regularly with subject matter experts. This interplay, along with the iterative and learning nature of the preliminary scoping assessment, adds to the robustness of the decision-making in developing the conceptual framework for the literature review and, ultimately, the final set of included articles that form the evidence-base for the standards.
Implications for Policy and Practice
This narrative review examined the experience of individuals who receive and provide home care services. The implementation of regulations and national standards that support providers to develop and update their policies, procedures, and guidance to ensure a holistic, person-centered home care is essential for the sector. A person-centered service should focus on quality, be integrated, needs led, and inclusive of complex care, without barriers, or gatekeepers to access home care services. Furthermore, the fundamental principles of a HRBA, safety and wellbeing, responsiveness, and accountability—should underpin the legislation, standards, and regulation of this sector. This is an opportunity to incorporate a consistent and meaningful framework throughout the home care sector, ensuring high-quality of care and support for service users and their family. In addition, strong and effective governance arrangements are required at national, regional, and local service-delivery levels, to ensure that people using home care services receive consistent, safe, and coordinated care.
Conclusion
Applying the principles of a HRBA, safety and wellbeing, responsiveness and accountability to home care services can inform policymakers, home care providers and others of good practice in upholding person-centered care during home care policy development and delivery. Home care providers need to recognize and acknowledge the values and preferences of service users. Person-centered home care must be provided by skilled care staff who collaborate and communicate openly with families and people receiving care and support to bring about the best health and personal outcomes. Systems and structures to support collaborative working and communication between home care services and other health and social care services are needed, to ensure that people get the integrated care and support they need and that the information required to drive quality and safety is available when and where it is required.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223241267874 – Supplemental material for How to Achieve Person-Centered Care for People Using Home Care Services: A Narrative Review
Supplemental material, sj-docx-1-hhc-10.1177_10848223241267874 for How to Achieve Person-Centered Care for People Using Home Care Services: A Narrative Review by Carolina Bassul, Judy Gannon, Yvonne Kelly, Michelle Williams, David Morrissey, Joyce McKee, Niamh O’Rourke and Rachel Flynn in Home Health Care Management & Practice
Footnotes
Authors Contribution
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.