
Abstract
Safe medication management is crucial for maintaining health and well-being, particularly among older adults who often take multiple medications prescribed by different healthcare providers. The aim of this study was to identify factors related to medication safety among older adults using the Safe Medication Assessment (SMA) tool during home visits conducted by mobile care teams in the western part of Sweden. A quantitative pilot study was conducted. Safe Medication Assessment was used at baseline (n = 18) and follow-ups at 1 month (n =13) and 3 months (n = 13) to measure medication management. The study presented numbers and proportions (%) of identified similarities and differences in medication management among participants. The study identified several common risk factors associated with unsafe medication management among older adults, for example taking 5 or more medications (95%), having prescriptions from different prescribers (70%), and dealing with the complexity of medication management (39%). Protective factors that contributed to safe medication management included use of methods to remember medication schedules (95%), securely storing medications (95%), and having knowledge about prescribed drugs (77%). Implementing Safe Medication Assessment (SMA) during home visits offers a proactive approach to enhancing safe medication management among older adults living at home. Addressing risk factors such as polypharmacy, comorbidities, and cognitive function, along with use of protective factors like medication storage and patient education, can optimize medication therapy, minimize risks, and enhance treatment outcomes. Mobile care units play a vital role as a bridge for integrated care between different care providers, facilitating improved treatment outcomes for older adults managing complex medication regimens at home.
Keywords
Background
Mobile teams perform home visits as a working approach to improve continuity of care for older adults following hospitalization. The current study aims to develop knowledge regarding factors related to medication safety among the elderly using an instrument for drug assessment, Safe Medication Assessment (SMA), during home visits.1 -3 By considering various factors such as age-related physiological changes, comorbidities, polypharmacy, and cognitive function, healthcare professionals can minimize the risk of adverse drug events and optimize therapeutic outcomes. 4 Therefore, reviewing medications based on their indication, dosage regimen, potential drug interactions, and any adverse effects is significant, particularly after discharge from hospital where new or changed prescriptions are common.5,6 Aging leads to changes in organ function, such as decreased renal function and liver metabolism, as well as alterations in body composition and metabolism, which can affect drug clearance, concentrations, and side effects, highlighting the need for dosage adjustments. 7 Another important consideration is the presence of comorbidities among older adults, with multiple chronic conditions often requiring pharmacological treatment. Therefore, it is crucial to consider interactions among prescribed medications to prevent complications. 8 Moreover, polypharmacy, the use of multiple medications, is common among older adults and increases the risk of adverse drug events, drug interactions, and non-adherence.
Regularly reviewing medication lists is necessary to identify unnecessary or duplicative medications and optimize treatment.9,10 Cognitive impairment, such as dementia or mild cognitive impairment, can also affect older adults’ ability to follow medication regimens and recognize drug reactions or interactions. 11 Empowering older adults in medication management is stressed to enhance safety and adherence. Nursing interventions, such as providing clear and accessible information about prescribed medications (including instructions for use and side effects), can increase compliance by facilitating informed decision-making and self-management. Nursing support also includes monitoring older adults’ medication management to detect side effects, failures, or changes in health and well-being, and then making necessary adjustments. Safe medication assessment requires a multifaceted approach encompassing age-related changes, comorbidities, polypharmacy, cognitive function, patient education, and support from healthcare professionals, such as nurses. 12
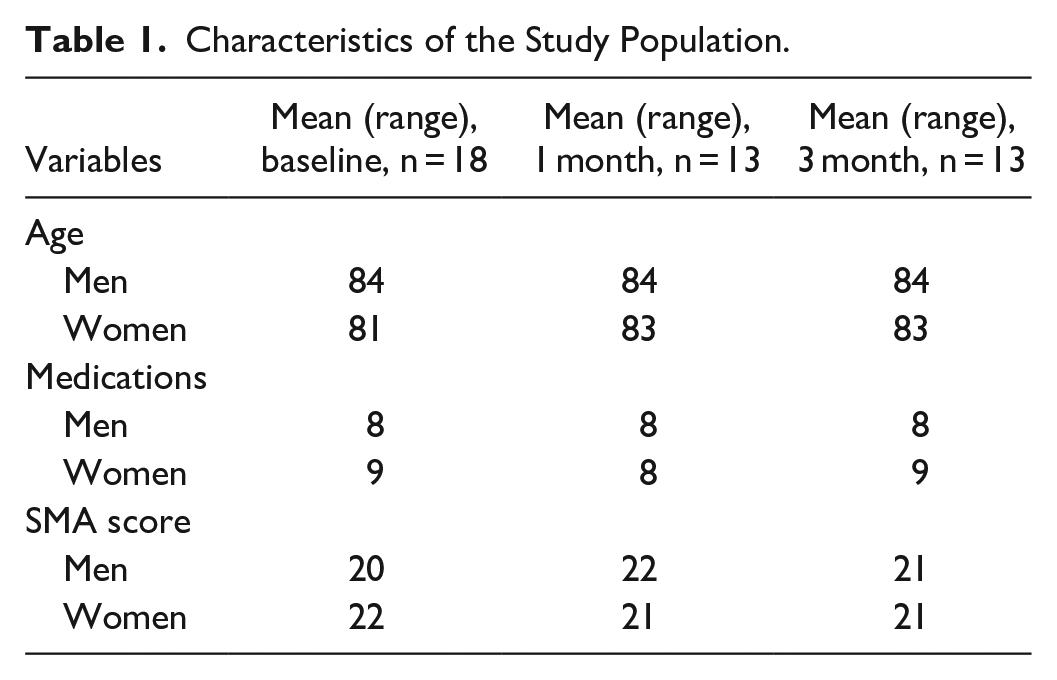
The demographic profile of Sweden indicates a growing population with an average life expectancy of 84 years for women and 81 years for men, resulting in a shortage of caregivers for older adults needing support in daily life. The Swedish National Healthcare Services, predominantly publicly managed, are provided by county councils, local authorities, or municipalities. Private healthcare services are often contracted by these entities, resulting in similar healthcare costs (whether public or private). Primary care offers basic health and medical services (general practitioners, specialist nurses, physiotherapists, occupational therapists, dentists) for common conditions and illnesses. 13 Hospitals provide highly specialized care, for example, Sahlgrenska University Hospital. One part of this hospital, Sahlgrenska Home, offers healthcare at home to avoid unnecessary hospitalization, complementing emergency and/or geriatric clinics and collaborating across organizational boundaries based on individuals’ needs and situations. 14 Additionally, each municipality organizes elderly care, either in private homes or elderly care homes. Both public and private providers offer home help services and elderly care homes. 13 Safe Medication Assessment (SMA), a systematic protocol for assessment, activities, and communication, is used in Swedish primary healthcare to monitor older adults’ drug treatment. It includes information about prescribed medications to avoid unsafe medication management, such as double dosing due to newly prescribed or expired drugs. SMA is considered a tool for safe medication management, particularly regarding polypharmacy (using more than 5 medications) among older adults living in private homes.2,3 Limited knowledge of prescribed medications can lead to poor compliance with prescriptions, underscoring the importance of clear and updated drug prescriptions to ensure patient safety. 15 Another issue is the lack of information transfer, which often occurs when older adults transition between care providers, such as moving from hospital care to home healthcare provided by the municipality. This lack of transfer can result in uncertainty regarding medication management. 16 To our knowledge, there is limited information about the use of systematic approaches like SMA to safeguard medication management for older adults at home. Therefore, the aim of this study was to identify factors related to medication safety among older adults using the Safe Medication Assessment (SMA) tool during home visits conducted by mobile care teams in the western part of Sweden
Methods
Setting
The university hospital in the western part of Sweden employs approximately 17,000 individuals across 120 departments spread across 4 different hospitals. The hospital where the study took place includes an emergency department, intensive care unit (ICU), operating theatre, wards, and various day care units. Patients experiencing ill-health are provided with different care pathways based on their health status, including admission to wards or transfer to primary or community care providers. Mobile care units associated with the hospital perform drug utilization reviews for older adults who have been hospitalized previously or have visited for day care. 14
Design
Descriptive statistics 17 were used to analyze current pilot study with data collected at baseline, 1 month, and 3 months using Safe Medication Assessment (SMA) protocols consisting of twenty items.2,3 Four of these items focused on prescription details, including routes of administration, potency, dosage, and whether assistance in dispensing medications was required. The remaining 16 items assessed medication safety, such as reporting/showing prescribed medications, medication clarity, and cognitive/memory problems (Supplemental Appendix).
Data Collection
A strategic sampling method was used to the pilot study. 17 A researcher (registered nurse from a mobile care unit in the western part of Sweden) collected data using the SMA protocol2,3 for drug reviews among older adults aged 65 years and above residing in private homes. Inclusion criteria were former patients (hospital stay or day care) over the age of 65 who could understand and speak Swedish and lived in private homes receiving home visits from a mobile care team associated with a university hospital. Exclusion criteria included adults younger than 65 years and older adults living in nursing homes. The first 18 persons (Table 1) approached to participate in the study (from February to April 2023) were included (10 former inpatients, 5 emergency department users, 2-day care unit attendees, 1 ambulance transport recipient). During the initial home visit (baseline), participants received oral and written information about the study’s aim, methodology, forthcoming results, and were assured of anonymity and voluntary participation.18,19 Before follow-up visits at 1 and 3 months, the nurse called several days in advance to confirm voluntary participation. Five out of the initial 18 participants dropped out before the first follow-up at 1 month, resulting in 18 participants at baseline and 13 participants at the follow-ups. Data collection took place from February to August 2023, with 1 researcher (CS) using the SMA protocol.2,3
Characteristics of the Study Population.
SMA Protocol
The SMA protocol2,3 consisted of 20 items, with 4 items (yes/no) focusing on prescription details according to overview of medication management (prescription, drug used, dosage, support) and 16 (0-2 = 0-30) on medication safety aspects for example reported drugs, number of drugs and cognitive ability (Supplemental Appendix). Participants were asked to show and describe their prescribed medications, and questions were posed in line with the SMA protocol regarding medication management at home, including assessments of cognitive impairment, swallowing difficulties, and language barriers. Each item represented a potential risk factor and was assigned points (0-30), with higher points indicating safer medication management.
Data Analysis
A pilot study using quantitative methods was conducted. 17 Outcome measures included the number of drugs and potential drug-related problems. Descriptive statistics 17 based on the SMA protocol2,3 was used to identify factors related to medication management among older adults. Data from the protocol were analyzed using Microsoft Office to present numbers and proportions. An overall mean was calculated based on 3 assessments (baseline, 1 month, and 3 months) to identify similarities and differences in medication management among participants.
Ethical Considerations
Ethical approval for the study was obtained from the mobile team unit managers. According to Swedish regulations, 20 ethical approval is not mandatory for quality improvement studies that do not pose harm to individuals, as was the case in this study related to medication management. However, respect for participants was a primary concern throughout the study, following the principles of the Declaration of Helsinki 19 and national ethical considerations. 18 All participants were informed about the study’s aim, and voluntary participation was emphasized at all data collection phases (baseline and follow-ups). Written informed consent was obtained before data collection, ensuring no harm and voluntary participation. To maintain anonymity, no personal identification was used in the presentation of results, which were presented using tables and numbers.
Results
Safe Medication Assessment: Mobile Teams Toward Continuity
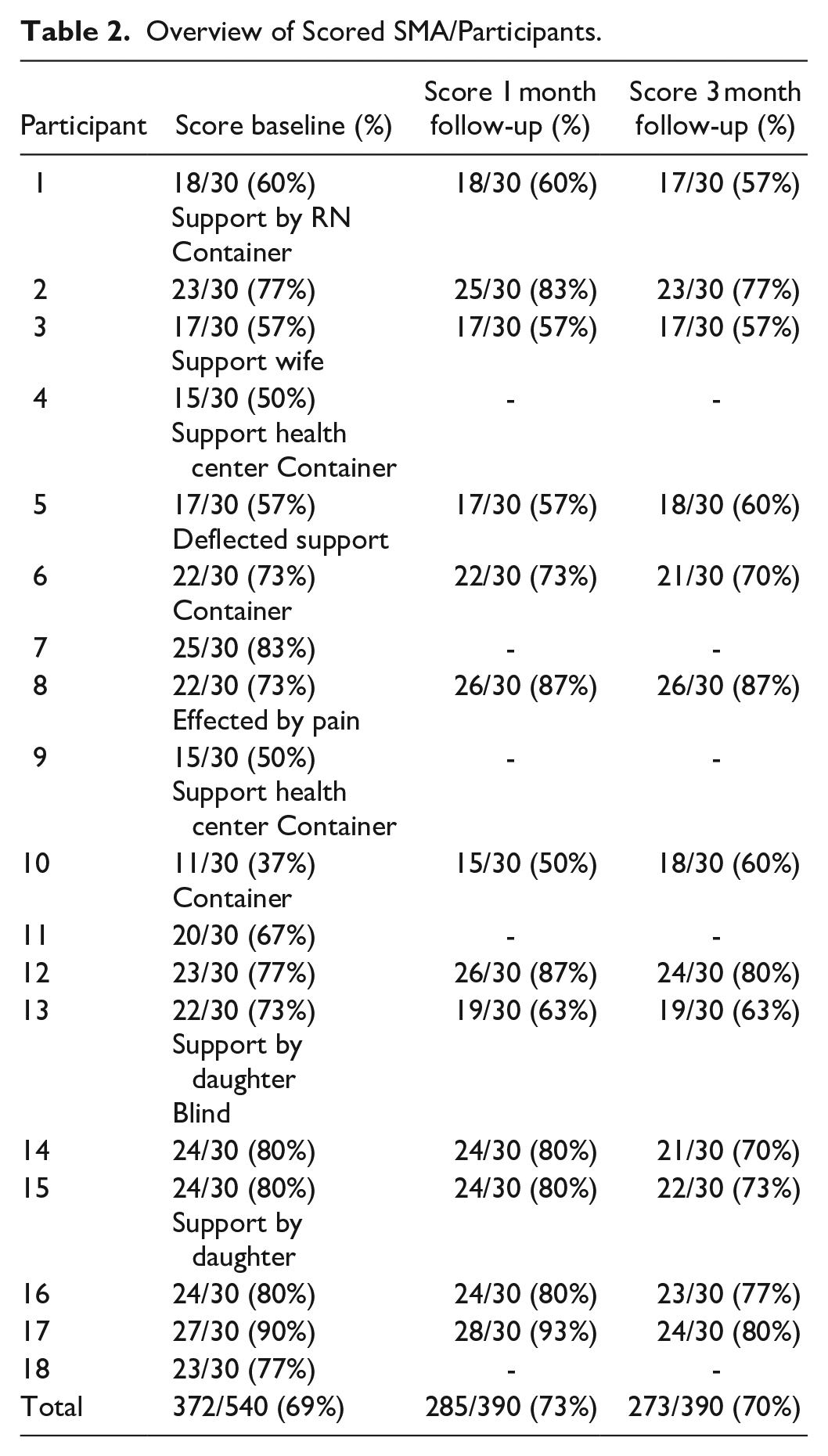
Medication assessments conducted using the Safe Medication Assessment (SMA) revealed that all participants were able to provide descriptions of their prescribed medications. During the initial visit, 3 out of 18 participants (17%) managed their medications independently using containers or dose dispensers, while 2 participants received assistance from relatives, and 1 participant used a dosing aid (Table 2). By the first follow-up visit (1 month), 1 out of 13 participants (8%) had received assistance from relatives or nurses until they received containers or dose dispensers, highlighting the importance of planning for safe medication management. Assistance from healthcare professionals or relatives with dispensing drugs remained low, and the use of containers or dose dispensers also remained infrequent (baseline 17%, follow-ups 8%)
Overview of Scored SMA/Participants.
The nurse conducting medication assessments via SMA identified the 5 most common risk factors related to unsafe medication management (Table 3) as the use of 5 or more drugs (95%), involvement of multiple prescribers (70%), complexity of medication management (39%), deliberate alteration of prescribed doses (23%), and side effects (20%). Drug interactions (11%) were also identified as a risk factor. However, swallowing difficulty (0.5%) and misunderstanding risks (0%) were minimal, with all participants being native Swedish speakers. Additionally, a decrease in deliberate use of doses other than prescribed without consulting prescribers was noted from baseline (33%) to follow-ups (1 month = 8%, 3 months = 15%). Alcohol did not emerge as a risk factor in this pilot study.
Responses to Individual Items Safe Medication Assessment Tool.
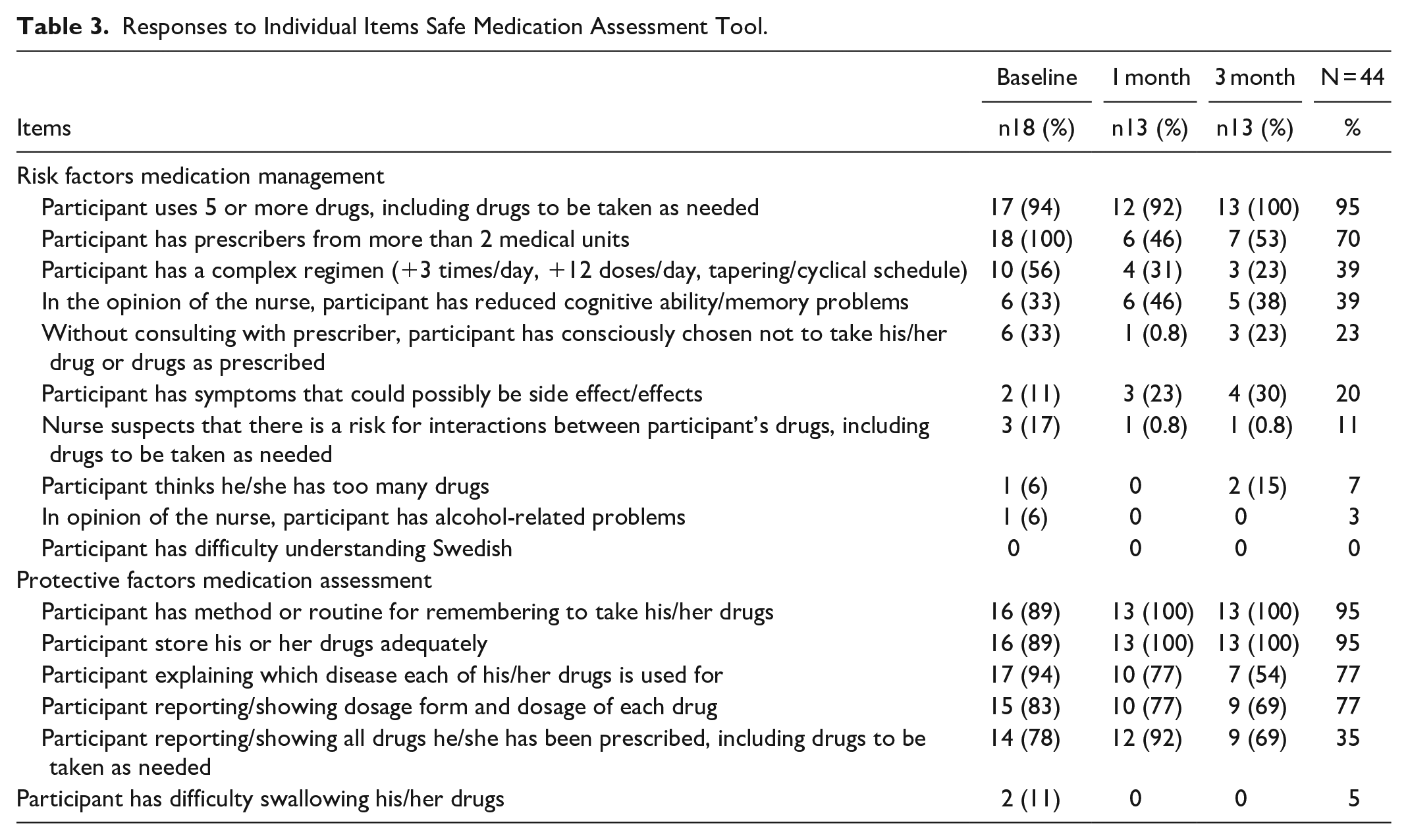
The results also revealed protective factors (Table 3). For instance, 95% of participants had developed their own methods to remember when and how to manage medications. Furthermore, medications were stored securely and safely at home. Additionally, 77% of participants understood the purpose of their prescribed drugs, and the same percentage could describe and/or show the dosage of each drug. Interventions to enhance safety and quality of medication, such as drug dispensers (20%), were noted. Home visits conducted by nurses could be described as nursing interventions, facilitating safe use of prescribed medications by providing structured information and education related to the treatment of ill-health following SMA protocols.
Discussion
The study aimed to identify factors related to the safety of medication among older adults using the Safe Medication Assessment (SMA) instrument during home visits, and this aim was achieved. The results demonstrate the use of the SMA instrument during home visits in Sweden, systematically addressing factors related to medication safety among older adults. By using SMA, registered nurses (RNs) working in various healthcare settings (hospital, home health care) can systematically evaluate medication management dimensions such as appropriateness, adherence, and potential risks associated with polypharmacy and drug interactions among older adults to enhance health and well-being.
Based on the identified medication management risk factors, several conclusions can be drawn. The use of 5 or more drugs (risk of polypharmacy) was a significant risk factor for medication management among older adults, particularly when including drugs taken as needed, which can lead to drug interactions, side effects, and non-compliance/adherence.12,21 Using SMA2,3 offers a structured and systematic approach independent of the healthcare professional conducting home visits, focusing on function and tasks rather than individual health professionals’ approaches. SMA’s structured approach ensures that well-known risk factors such as age-related physiological changes, comorbidities, polypharmacy, and cognitive function are not overlooked, reducing side effects and improving compliance.4,9,10 Mobile teams 1 conducting home visits can also improve continuity of care by bridging the gaps between different healthcare providers from healthcare and social services, reducing communication gaps, duplicative prescriptions, and conflicting treatment plans to ensure older adults’ safety and treatment outcomes. This is especially important given the complexity of medication regimens, frequent dosing, high daily doses, or tapering/cyclical schedules. RNs conducting home visits may face challenges related to adherence, which increases the risk of dosing errors, missed doses, and medication mismanagement.22,23 Additionally, nurses’ observations of reduced cognitive abilities or memory problems can be visualized through SMA, allowing for professional management of concerns about older adults’ capacity to manage their medications safely and effectively, reducing the risk of medication errors, accidental overdoses, and missed doses.23,24 During home visits, discussions about non-adherence behaviors, such as deviating from prescribed medications without consulting prescribers, can be conducted by visiting RNs in a calm and familiar home environment, enhancing health outcomes.23,24 Symptoms attributed to medication side effects during home visits indicate a need for closer monitoring and evaluation of the individual’s medication regimen.25,26 Failure to address these symptoms may lead to medication-related complications or discontinuation of necessary treatments, resulting in further ill health requiring hospitalization. 25
Implementing SMA during home visits facilitates comprehensive assessment of medication-related factors, enabling healthcare professionals (prescribers, RNs) to identify potential safety concerns, prevent side effects, and improve health and well-being. By evaluating medication treatment within the context of individuals’ needs and home health circumstances, SMA provides structured and systematic support to improve patient safety through medication compliance, persistence, and continuity of treatment. 24 SMA addresses specific medication-related issues such as simplifying complex regimens, adjusting dosages, and providing patient education to enhance safe medication management.2,3 Another conclusion drawn from the results is that SMA aligns with person-centered care principles, involving older adults in a calm, safe, and private environment.24,26 By conducting repeated home visits, RNs can continue discussions and decisions in partnership with patients and other team members (hospital, primary care, home health care), fostering collaborative shared decision-making processes and empowering older adults to be involved in their health and well-being.24,27,28,29
The results demonstrate protective factors in medication adherence, as older adults have established methods or routines for remembering to take medications, suggesting a proactive approach that enhances medication compliance and effectiveness.30,31 Moreover, appropriate medication storage at home is maintained to ensure drug efficacy and safety, which is crucial for optimal treatment outcomes. However, these results differ from other studies 32 showing more problematic situations at home due to inappropriate medication storage. This discrepancy may be attributed to the tradition of purchasing medication without a prescription at pharmacies or receiving leftover medications from relatives and friends. In Sweden, most medications require a prescription from a physician, making direct purchase from pharmacies impossible. Therefore, older adults’ knowledge of prescribed medications likely stems from information provided by prescribers and other healthcare professionals, including RNs during hospital or home health care treatments, demonstrating attentiveness to medication details. In accordance with a person-centered approach, actively involving older adults in their treatment plan based on their health status and informed decision-making can significantly enhance their health and well-being. Openness and collaboration in medication management, supported by home visits, serve as a cornerstone for developing a seamless and integrated healthcare system.24,27,33 In summary, based on the observed behaviors related to medication management, the participants demonstrate engagement and responsibility in adhering to their treatment regimens, contributing to improved medication adherence, treatment effectiveness, and overall health outcomes. However, ongoing support and monitoring may still be needed to ensure sustained medication adherence and optimal therapeutic benefits.
Limitations
There are limitations to this pilot study. 17 The sample size is small and limited to a specific setting (home visits in the western part of Sweden associated with 1 university hospital). However, validity and reliability are assured as the same participants were included in all 3 data collections, using a previously validated protocol in primary care, collected in a trusted environment (private homes) by a researcher with knowledge and experience in home visits and medication assessment. Data analysis was performed using established scientific methodology 17 by 2 authors (junior and senior researchers). Although the study adhered to ethical considerations 18 following the Declaration of Helsinki, 19 such as voluntary participation and anonymity, the results require further development due to the limited data collection (pilot study) within 1 setting. Future studies are needed to confirm these findings.
Conclusions
Implementation of Safe Medication Assessment (SMA) during home visits in Sweden represents a proactive and effective approach to improving safe medication management among older adults living at home. The identification of well-known risk factors such as polypharmacy, comorbidities, and cognitive function highlights the importance of conducting comprehensive assessments, close monitoring, and coordinated care to optimize medication therapy, minimize risks, and enhance treatment outcomes. SMA provides a systematic evaluation of medication-related factors and allows for tailored interventions based on individual needs within the context of integrated care across various healthcare settings. Strategies such as medication reconciliation and simplification of medication regimens, supported by education from mobile team units during home visits, can enhance medication adherence using a person-centered approach that fosters open communication among older adults, healthcare providers, and formal/informal caregivers. Implementing SMA during home visits enhances continuity of care by providing a holistic and systematic view of older adults’ medication management across different healthcare settings. This approach ensures that medication-related issues are identified and addressed proactively, ultimately improving patient safety, treatment adherence, and overall health outcomes. In summary, the use of SMA in home visit settings in Sweden demonstrates a commitment to enhancing the quality of care for older adults by focusing on safe and effective medication management within the broader context of integrated healthcare delivery.
Supplemental Material
sj-pdf-1-hhc-10.1177_10848223241257498 – Supplemental material for Ensuring Safe Medication Assessment for Older Adults: A Pilot Study
Supplemental material, sj-pdf-1-hhc-10.1177_10848223241257498 for Ensuring Safe Medication Assessment for Older Adults: A Pilot Study by Kristina Rosengren and Charlotta Szemberg in Home Health Care Management & Practice
Footnotes
Acknowledgements
The authors would like to acknowledge participants (patients) that shared their experience with us as well as the Sahlgrenska University Hospital, Department of Geriatrics, Mölndal, Sweden, and University of Gothenburg Centre for Person-Centred Care (GPCC), and Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.