
Abstract
Background: Physical activity is a safe, evidence-based self-management strategy for older adults (aged 65+) with cognitive impairment. Although homecare occupational therapists (OTs) and physiotherapists (PTs) are well positioned to support the growing number of older adults living at home with cognitive impairment, physical activity is rarely recommended as a strategy to manage cognition. Objective: To increase OTs’ and PTs’ knowledge of physical activity recommendations, as well as increase the range of physical activity recommendations for older adults living at home with cognitive impairment. Methods: This quality improvement project used a pre-post intervention approach. Data was collected through a pre-post clinician survey and pre-post chart audit to evaluate the impact of a multimodal education intervention on OT and PT knowledge and practice. The intervention included educational sessions and the development of four client handouts. Results: Post-intervention, OT and PT survey results showed a non-significant improvement in knowledge, and a greater range of physical activity recommendations. The PT chart audit demonstrated a statistically significant increase in PTs providing education about the role of physical activity in relation to cognitive impairment. For OTs, there was a non-significant increase in physical activity recommendations. Conclusions: This multimodal education resulted in non-significant improvements in knowledge for OTs and PTs, however there were significant practice changes for PTs when providing education to patients about the impact of physical activity on cognition. Future research could refine the targeting of this intervention to better meet the needs of OTs and incorporate an evaluation of patient outcomes.
Keywords
Background
The prevalence of cognitive impairment among older adults (aged 65+) is growing. Mild Cognitive Impairment (MCI) has a similar symptomatology to dementia (also referred to as neurocognitive disorder in the Diagnostic and Statistical Manual of Mental Disorders V1,2) and can be a precursor to dementia and/or Alzheimer’s Disease (AD).3,4 In Canada, there are more than 747,000 older adults living with dementia and AD, 5 with prevalence doubling every 5 years. 6 Not only can the symptoms associated with cognitive impairment (including MCI, AD, and/or dementia/neurocognitive disorder) result in a decreased quality of life, as well as reduced independence in activities of daily living (e.g., bathing), and instrumental activities of daily living (e.g., grocery shopping)5,7, the growing prevalence of cognitive impairment poses numerous challenges for families and the Canadian healthcare system. These include patient safety considerations, such as wandering and responsive behaviors, as well as caregiver burden, and financial strain to families and the healthcare system.8,9
To address the increasing prevalence of cognitive impairment, de Melo Coelho et al. 10 recommend adopting prevention strategies to alter the course or progression of dementia and AD. This is consistent with the Government of Canada’s recent strategy to address the growing prevalence of dementia across the country. 8 Physical activity is an evidence-based, safe, and effective method of slowing the progression of dementia, as well as preventing the progression of MCI to dementia.11 -14 Physical activity can be defined as “any bodily movement produced by skeletal muscles that requires energy expenditure,” 15 therefore, it can include physical exercise (e.g., jogging) and daily activities (e.g., vacuuming). Older adults with cognitive impairment may have difficulty engaging in physical activity due to comorbid conditions (e.g., arthritis), fear of injury, and difficulty understanding instructions.16,17 However, physical activity is particularly beneficial for these older adults as it can improve memory, attention and performance in activities of daily living, as well as reduce caregiver burden.11,18 -20
Occupational therapists (OTs) and physiotherapists (PTs) working in the home and community healthcare sector are well positioned to provide physical activity recommendations to older adults living with cognitive impairment. However, their ability to provide such recommendations is impacted by limited training on individualized approaches and limited clinician awareness of the benefits of physical activity for individuals living with cognitive impairment. 21 Additionally, studies addressing strategies to support increased physical activity for older adults living at home with cognitive impairment are limited.
Aim
The primary aim of this quality improvement project was to increase community OTs’ and PTs’ knowledge of physical activity as an important intervention for older adults with cognitive impairment by 20%. The secondary aim was to increase the range of physical activity recommendations for older adults living at home with cognitive impairment. The need for this project was supported by a local needs assessment at our organization. This assessment showed that physical activity was not being addressed in practice with these clients despite OTs and PTs indicating that physical activity was important for older adults with cognitive impairment.
Methods
Study Design
This quality improvement project utilized a pre-post intervention design guided by the Model for Improvement. 22 The Model for Improvement serves as a simple and useful framework for rapid organizational improvements and improved patient outcomes in health care settings. 22 There are 3 fundamental questions in The Model for Improvement, which will be highlighted in this article22,23:
(1) What are we trying to accomplish?
(2) How will we know that a change is an improvement?
(3) What changes will result in improvement?
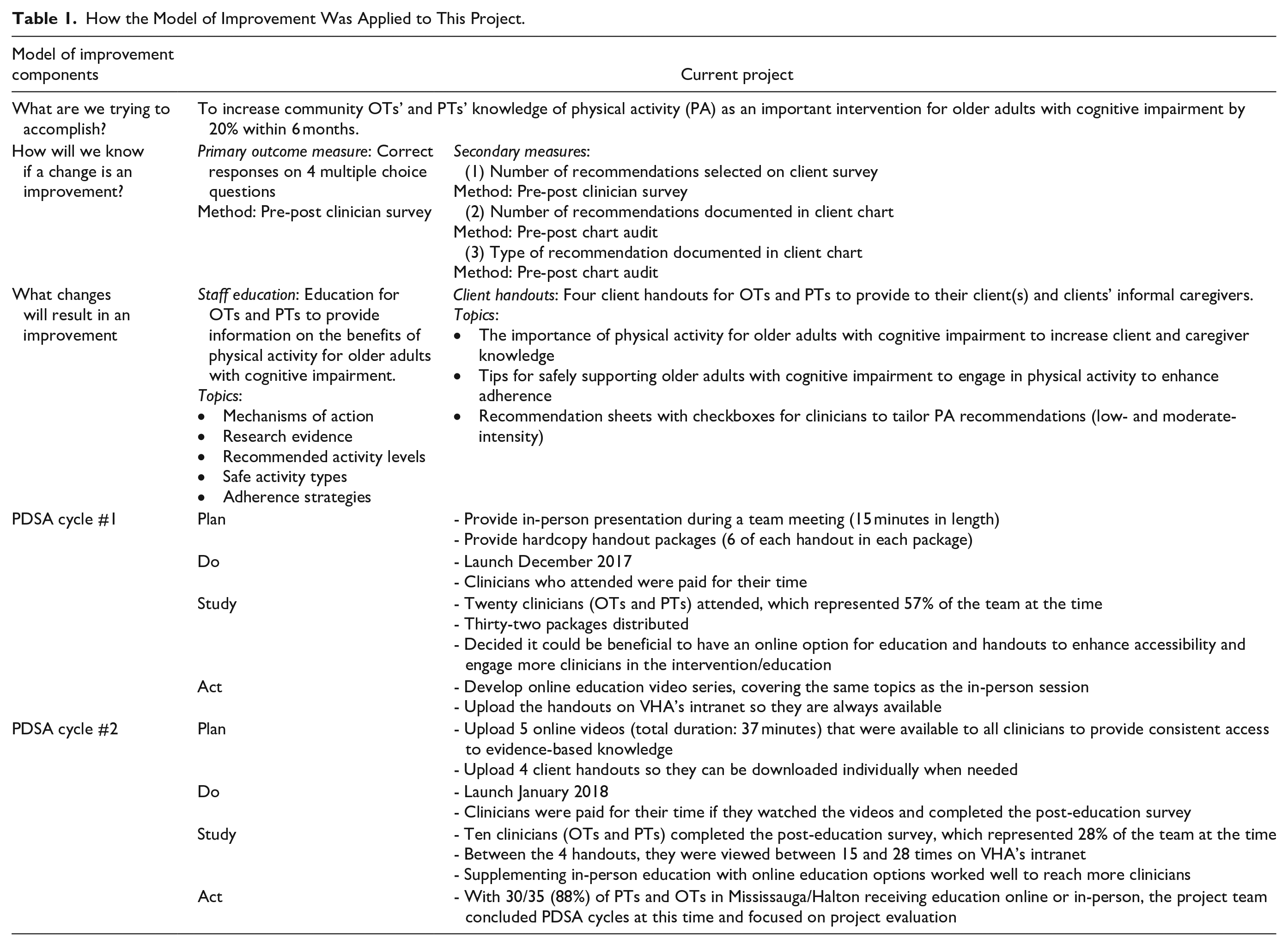
Once improvements, or change ideas, are conceptualized, The Model for Improvement uses Plan-Do-Study-Act (PDSA) cycles as the mechanism to implement rapid change. PDSA cycles are iterative processes, where small improvements are tested and inform future small improvements.20,21 Table 1 summarizes how each of the Model’s components were applied in this project.
How the Model of Improvement Was Applied to This Project.
Setting
The project was conducted at a home healthcare organization that provides homecare support to individuals of all ages and backgrounds with a broad range of medical conditions. This intervention was implemented in an administrative health region that incorporated both urban and suburban neighborhoods within the Greater Toronto Area of Ontario. At the time of project implementation, this region was served by a team of 35 OTs and PTs who collectively visited approximately 3000 clients/month. OTs were typically authorized to conduct 2 to 4 visits with clients, whereas PTs usually had 4 to 6 visits, sometimes with support from a physiotherapy assistant.
Multimodal Education Intervention
A needs assessment was first conducted to identify what type of intervention(s) may help to address the aim. A current state assessment was used to validate the project aims, and to inform change ideas by asking clinicians what would improve their knowledge and support physical activity recommendations. During the needs assessment, OTs and PTs were asked to comment on tools and resources that would be helpful in addressing physical activity with their older adult clients with cognitive impairment. They reported that the most useful tools/resources would be having a list of safe activities they can tailor to clients’ needs, developing a better understanding of the research evidence, and informational handouts for clients and caregivers. Thus, a multimodal intervention was designed to increase OT and PT knowledge and enhance their ability to address physical activity with their older adult clients with cognitive impairment. This intervention consisted of provider education, as well as handouts for clients and families. The handouts developed for this project are included as supplemental materials.
The content for each element of the intervention, summarized in Table 1, was informed by peer-reviewed literature, reputable gray literature (e.g., Alzheimer’s Society Canada, Canadian Society for Exercise Physiology), clinicians, clinical leaders, and/or a client partner with lived experiences caring for a family member with cognitive impairment. Feedback was sought through email and during meetings, where stakeholders could provide feedback about the content, style, and layout of resources. A comprehensive education plan (synchronous in-person and asynchronous video-based) was developed to accommodate the variability of homecare OT and PT schedules. The synchronous education session was also used as an opportunity to solicit feedback on the intervention handouts and inform any necessary refinements. OTs and PTs were compensated for their time for attending the education session, or for viewing the online videos. The education was complemented by a set of 4 handouts that clinicians could provide to clients and caregivers to share the importance of physical activity for people with cognitive impairment, provide tips for safely assisting with this exercise, and provide specific recommendations for low- and moderate-intensity exercises that could be customized for each client (Table 1).
Figure 1 highlights how the intervention targeted different barriers to knowledge and physical activity recommendations using a driver diagram. A driver diagram is a quality improvement tool that shows what change ideas or interventions the project team hypotheses will result in the achievement of the project’s aim. 24
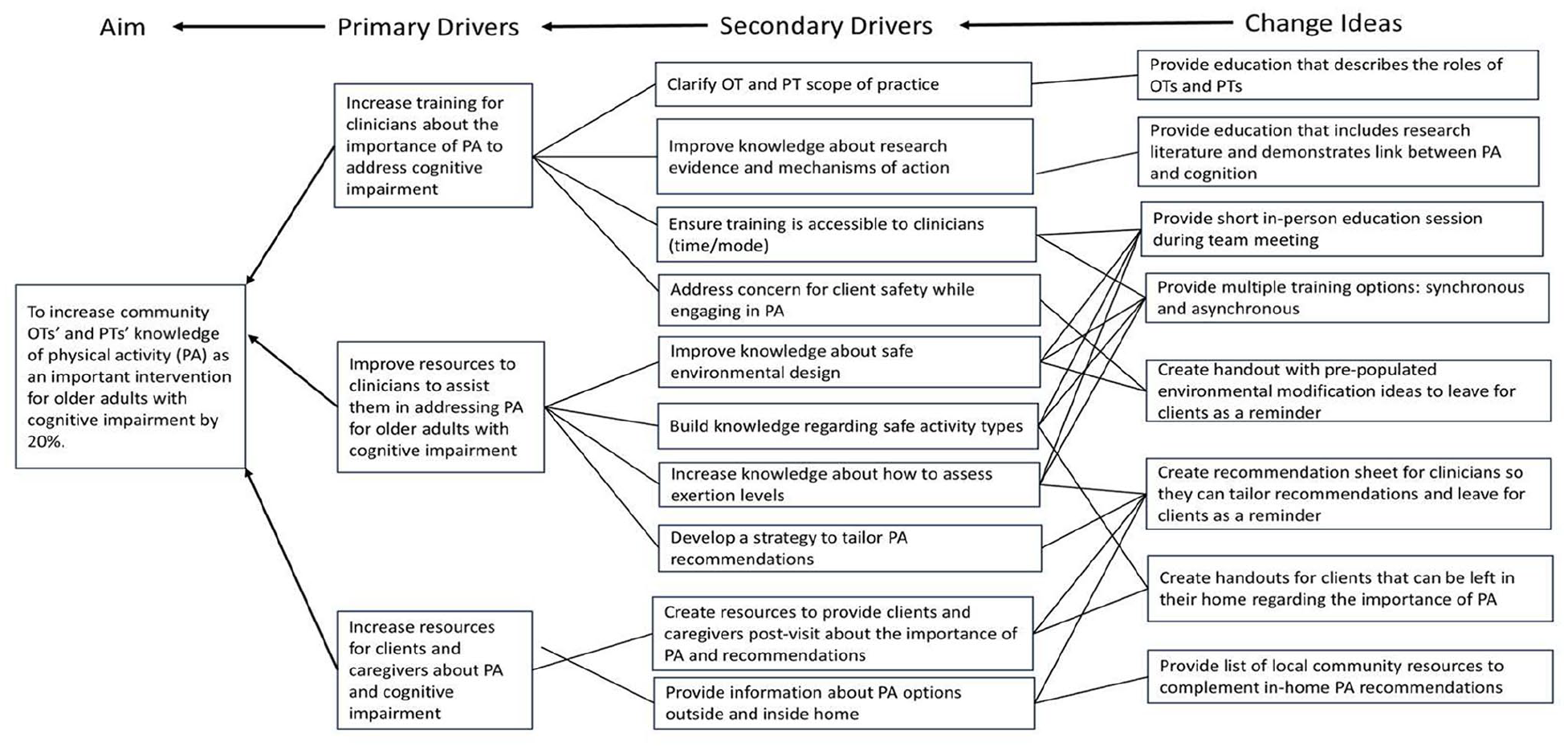
Driver diagram demonstrating link between project aim and change ideas.
Measures and Data Collection
Intervention implementation was tracked using 3 process measures: percent of OTs and PTs attending the in-person/synchronous training, number of hardcopy handout packages distributed to OTs and PTs, and number of times that the online resources were accessed.
Two main outcome measures were used related to knowledge and practice change. OTs’ and PTs’ knowledge of physical activity as it relates to cognitive impairment (MCI, dementia/neurocognitive disorder, and/or AD) was measured through average scores on the knowledge portion of a clinician survey distributed before the start of the intervention (i.e., before the education session) and after the intervention. Practice change was measured as the proportion of charts providing a physical activity recommendation for these clients, and the proportion of charts where education about physical activity in relation to cognitive impairment was documented. We also noted the types of physical activity recommendations that clinicians reported providing to clients. As a secondary practice change measure, the pre-post survey for clinicians also asked about the types of physical activity recommendations that they were making for clients with cognitive impairment.
Pre-post survey for clinicians
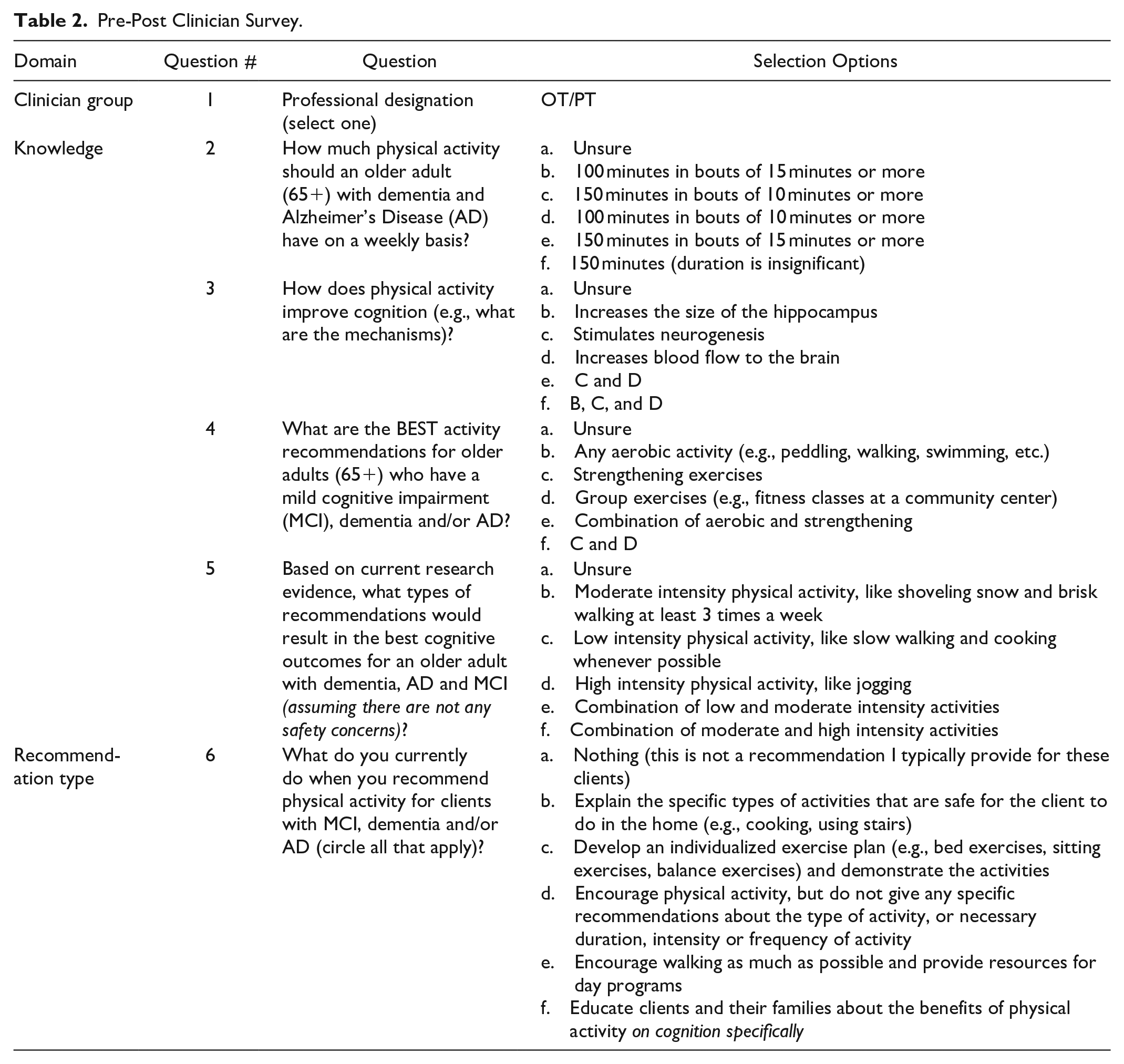
The survey was administered to OTs and PTs in the region selected for implementation of this quality improvement project. The survey was developed by the first author (BE) and reviewed by the fourth author (AR). These questions were developed based on clinical experience, availability of evidence, and the scope of practice for OTs and PTs in homecare (see Table 2).
Pre-Post Clinician Survey.
The survey evaluated:
(1) Change in knowledge based on 4 knowledge-based multiple-choice questions that asked about: (1) the recommended amount of physical activity per week for older adults with cognitive impairment; (2) the mechanisms by which physical activity improves cognition; (3) the best types of activity recommendations for older adults with cognitive impairment; and (4) the most appropriate types of activities to recommend.
(2) The types of physical activity recommendations that were being made for clients with cognitive impairment in multiple choice format. The options included: (1) Nothing (this is not a recommendation I typically provide for these clients); (2) Explain the specific types of activities that are safe for the client to do in the home (e.g., cooking, using stairs); (3) Develop an individualized exercise plan (e.g., bed exercises, sitting exercises, balance exercises) and demonstrate the activities; (4) Encourage physical activity, but do not give any specific recommendations about the type of activity, or necessary duration, intensity or frequency of activity; (5) Encourage walking as much as possible and provide resources for day programs; (6) Educate clients and their families about the benefits of physical activity on cognition specifically.
The pre-intervention survey was administered in hardcopy in December 2017 during a team meeting. The post-intervention survey was administered in February 2018. Both hardcopy and online versions of the post-intervention survey were available to optimize response rates. Clinicians who viewed the videos online were required to complete the post-intervention survey to receive compensation for their time. An individualized email to all OTs and PTs on the team was sent prior to the post-intervention survey deadline (February 28, 2018).
Pre-post chart audit
The pre-post intervention chart audit was conducted to evaluate practice change related to the proportion of charts where physical activity recommendations were being made and the nature of these recommendations. Physical clinical charts were pulled from the organization’s Record Management based on service type (OT and PT only), and discharge date.
The pre-intervention chart audit was conducted in February 2018 and included a random selection of OT and PT clients discharged between August 1 and October 1, 2017. The post-intervention chart audit was conducted in March 2018 and included a random sample of charts for OT and PT clients discharged between January 27 and February 14, 2018. To be included in the evaluation, charts had to meet 2 additional criteria: (1) clients were aged 65 years or older; (2) have a diagnosis of dementia, AD, or MCI on referral, or MCI documented on clinical assessment (i.e., based on clinical observation).
For charts that met the inclusion criteria, the primary author recorded the clinician recommendations/treatment plan (open-ended), whether physical activity recommendations were provided (yes/no), and whether physical activity education was provided in relation to cognition or brain health (yes/no).
Analysis
Descriptive statistics were used to capture counts and proportions. For knowledge change, we calculated the average score received on the knowledge survey before and after the education session stratified by profession (OT vs PT) and calculated the percent change. For practice change, we calculated the proportion of charts with a documented physical activity recommendation and education. Fisher’s exact test (p < .05) was used to test for significant differences between the number of documented pre- and post-intervention physical activity recommendations and education about physical activity in relation to cognitive impairment. An unpaired t-test (p < .05) was used to assess changes in knowledge scores pre- and post-intervention. All statistical tests were conducted in R. Practice change was also evaluated by synthesizing physical activity types as documented in the client’s chart.
Ethical Considerations
This was a quality improvement project and did not require review by a research ethics board, as confirmed by the ARECCI Screening Tool. 25
Results
In total, 57% of the team’s OTs and PTs attended the in-person training (20/35). At this time, 32 hardcopy handout packages were distributed. There were 6 copies of each handout included in 1 package. Clinicians were encouraged to take as many packages as they felt they needed according to their case load and distance from the office. By March 2018, the digital education folder had been viewed 61 times.
Pre-Post Survey of Clinicians
In total, 13 clinicians (6 OTs and 7 PTs) completed the hardcopy pre-intervention survey, and 17 clinicians (11 OTs and 6 PTs) completed the post-intervention survey. Due to the multi-model nature of the education plan (e.g., handouts, in-person and online videos), the project team was flexible with pre-post survey sampling. The pre-education survey was completed before individuals accessed any of the intervention components, and the post-education survey was completed after participants had an opportunity to engage with all education materials or aspects of it (e.g., online videos or in-person education). As such, it is possible that some participants only engaged in one data collection approach.
An increase in the average number of correct knowledge-based answers was observed post-intervention for both OTs and PTs, although the increase was not statistically significant (Table 3). After the intervention, PT knowledge increased from 0.86/4 (21.5%) to 2/4 (50%), p = .114, and OT knowledge increased from 1.5/4 (37.5%) to 1.73/4 (43.25%), p = .529.
Change in Knowledge—Average Correct Responses to the 4 Knowledge-Based Questions.

When asked about current practices related to recommending physical activity for older clients with cognitive impairment, OTs and PTs in the post-intervention survey reported providing more individualized physical activity recommendations with greater specificity (e.g., specific in-home activities, walking, adult day program) than in the pre-intervention survey; more also reported providing clients with education about the benefits of physical activity for managing cognitive impairment. Pre-post differences in these measures were non-significant.
Pre-Post Chart Audit
The pre-intervention chart audit included a review of 97 charts for clients discharged between August 1 and October 1, 2017, of which 24 charts met the inclusion criteria. The post-intervention chart audit included review of 114 charts for clients discharged between January 27 and February 14, 2018, of which 35 met the inclusion criteria. These charts did not necessarily belong to the clinicians included in the pre-post survey since the survey was anonymous.
The results of the chart audit are shown in Table 4. While there was not a statistically significant change in the proportion of charts with a documented physical activity recommendation, there was a significant change in the number PT charts indicating that physical activity education had been provided in relation to the client’s cognitive impairment (p = .046). No such increase was seen in the OT charts.
Physical Activity Recommendations Documented in Client Chart.
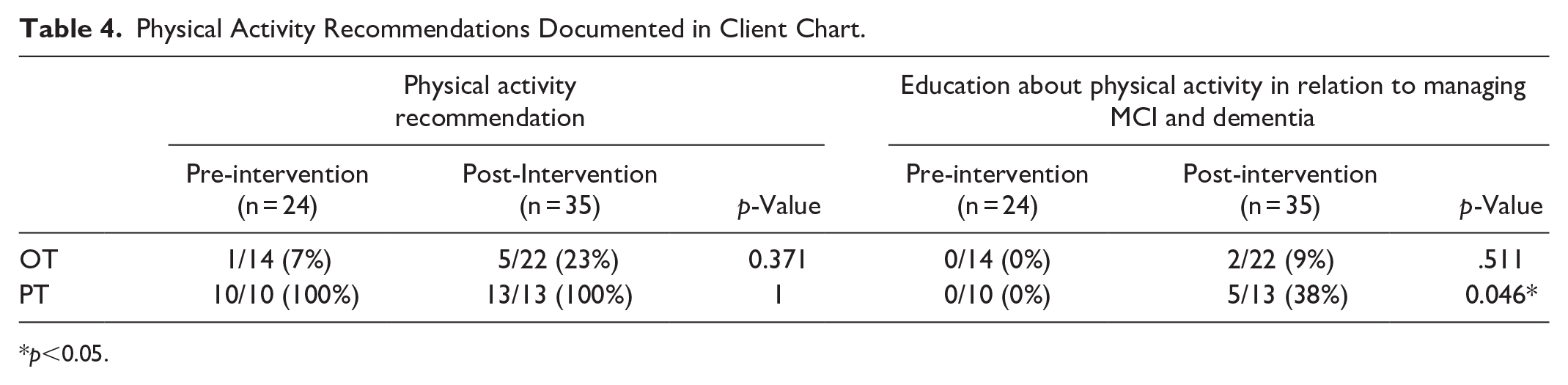
p<0.05.
A synthesis of the types of physical activities recommended by OTs and PTs in the client chart showed an expansion in the range of exercise types prescribed post-intervention. Pre-intervention, OT physical activity recommendations were limited to balance and posture exercises; post-intervention, more charts reflected a greater variety of physical activity recommendations, including day programs and reinforcement of the value of adhering to PT exercise programs. All PT charts both pre- and post-intervention included physical activity recommendations; pre-intervention, these focused on seated home exercise programs to improve upper body strength and range of motion activities; post-intervention, they also included walking, gait training, and community exercise/fitness programs.
Discussion
The results of this quality improvement project showed that the combination of education and access to handouts significantly increased the frequency of PTs’ patient education, as it pertains to the role of physical activity on cognitive health. OTs also provided more recommendations related to physical activity, including education about the benefits of physical activity on cognitive health. These educational tools may also help to improve OT and PT knowledge of the impact of physical activity on cognitive health, despite not reaching statistical significance. Furthermore, the range of physical activity recommendations provided by OTs and PTs was broadened post-intervention, and clinicians self-reported providing more individualized and specific recommendations for their clients.
While significant changes to PT practice was observed, similar improvements were not observed for OTs. This could be due in part to differing roles and role perceptions between these clinical specialties, however, there is an opportunity for clinicians in both roles to contribute to promoting physical activity for clients with cognitive impairment. While physical activity recommendations are more typically viewed as being the domain of PTs, increases in physical activity for clients with cognitive impairment would help to address the types of clinical outcomes (physical performance, cognition, occupational performance, mood, and short-term memory) that OTs typically target. Further work, ideally in collaboration with OTs, is required to understand how to adapt the education and clinical supports to promote a more substantial adoption of this practice change for OTs.
The multimodal intervention, which included clinician education, informational client handouts and access to recommendation forms, increased the range and specificity of OT and PT recommendations of physical activity for this client group. These findings align with recent research, which emphasizes the importance of education in empowering professionals to provide evidence-based recommendations to address physical activity for their clients.21,26 Evidence-based education, in combination with client-facing clinical support tools, supported OTs and PTs in tailoring their physical activity recommendations to clients based on activity level, comorbid conditions, lifestyle, and preferences. Ensuring continued access to educational materials, such as online videos, client handouts, and recommendation templates can help to encourage best practices and sustain change.27,28
To facilitate sustainability, which can be difficult following the introduction of a quality improvement intervention, 28 this project incorporated a sustainability plan informed by the National Health Service (NHS)’s sustainability model. 27 The strategies employed were: (1) providing clinicians with ongoing access to education—both through access to the online education videos and through offering periodic synchronous in-person education sessions; (2) providing ongoing access to the client education resources and physical activity recommendation templates; and (3) incorporating physical activity recommendations into OTs’ workflows when a new electronic documentation system was introduced after the completion of this quality improvement project. These strategies were designed to help standardize and sustain project improvements, and are based on similar strategies demonstrated to drive and reinforce behavioral change in healthcare setttings.28,29 The incorporation of end-user feedback in refining the resources (following the initial education session) also supports their relevance and likelihood of sustained use.27,29 Finally, to supplement the core intervention resources, an information video was created for clients and caregivers and shared on the organization’s external website to raise awareness about the benefits of physical activity for older adults living with cognitive impairment and to further engage clients and families to increase the potential for long-term change. 29
The range of sustainability strategies implemented was specific to the community-based care context in which the intervention was conducted, including geographically-dispersed clinicians visiting clients in their homes and relying on hardcopy documentation at the time of project implementation. However, with the digitization of documentation, it may be possible to implement more active ongoing monitoring systems, such as a quarterly reports or best practice dashboards (i.e., visual management system), as an additional facilitating strategy to sustain change.28,29 In other care contexts (e.g., such as acute care and clinic settings, where clinicians are working in the same building), strategies including team quality improvement huddles can also help to sustain change and manage any barriers that arise. 28
Limitations and Recommendations for Future Research
This relatively rapid quality improvement project was strictly time-bound as it was designed and implemented as part of a 6-month Quality Improvement Fellowship. It focused solely on clinician outcomes and did not include client or caregiver outcomes. Extensions of this project could include measuring a broader range of outcomes, including impacts on client/patient and family perceptions of, adherence to, the recommendations. This intervention was more impactful for PTs than OTs, thus further work is required to adapt the intervention to support increased OT engagement in providing physical activity recommendations to clients with cognitive impairment. As identified above, there are also opportunities to embed reminders and clinical supports within the clinical assessment and documentation process. Visual management systems and ongoing clinician feedback could be helpful for understanding new or emerging barriers to sustainability of this intervention. Future initiatives could expand and apply this intervention to other professional groups, different regions and/or different clinical contexts to understand the broader potential of this intervention. Future projects would also benefit from adopting an alternative, more robust quality improvement design that controls for organizational and/or environmental factors, such as individual or cluster randomized control trials. 30
Conclusion
With the prevalence of cognitive impairment rising amongst older Canadians, effective self-management, including physical activity, will help to mitigate the impact on the affected older adults and their caregivers. A multimodal intervention consisting of education, recommendation forms, and informational handouts led to improvements in PTs’ knowledge and range of cognition-specific physical activity recommendations. Smaller non-significant changes in OT practice highlight an opportunity to further tailor the intervention to increase its relevance and usefulness for this group. Further investment in adapting the educational and clinical resources can help to capitalize on the potential of community-based OTs and PTs as champions for promoting physical activity and its numerous clinical benefits for older adults with cognitive impairment.
Supplemental Material
sj-pdf-1-hhc-10.1177_10848223241247837 – Supplemental material for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project
Supplemental material, sj-pdf-1-hhc-10.1177_10848223241247837 for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project by Brydne Edwards, Emma Perera, Emily C. King, Sandra M. McKay and Arlinda Ruco in Home Health Care Management & Practice
Supplemental Material
sj-pdf-2-hhc-10.1177_10848223241247837 – Supplemental material for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project
Supplemental material, sj-pdf-2-hhc-10.1177_10848223241247837 for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project by Brydne Edwards, Emma Perera, Emily C. King, Sandra M. McKay and Arlinda Ruco in Home Health Care Management & Practice
Supplemental Material
sj-pdf-3-hhc-10.1177_10848223241247837 – Supplemental material for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project
Supplemental material, sj-pdf-3-hhc-10.1177_10848223241247837 for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project by Brydne Edwards, Emma Perera, Emily C. King, Sandra M. McKay and Arlinda Ruco in Home Health Care Management & Practice
Supplemental Material
sj-pdf-4-hhc-10.1177_10848223241247837 – Supplemental material for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project
Supplemental material, sj-pdf-4-hhc-10.1177_10848223241247837 for Enhancing Physical Activity Recommendations to Support Cognition in Homecare: A Quality Improvement Project by Brydne Edwards, Emma Perera, Emily C. King, Sandra M. McKay and Arlinda Ruco in Home Health Care Management & Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors were employed by the organization where the quality improvement initiative was conducted at the time of their primary contribution to this project.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.