
Abstract
Background
Maintaining activities of daily living (ADLs) in patients with cognitive impairment slows the progression from mild cognitive impairment (MCI) to major neurocognitive disorders. Among the various cognitive functions, executive function is closely related to ADLs. Therefore, utilising ADLs to train executive function may help stall cognitive impairment progression. With the advancements in digital technology, we can employ virtual reality (VR) to repetitively train patients using ADLs.
Objective
We present the design and concept of a VR-based ADL training programme tailored for patients with MCI.
Methods
Our programme targeted patients with MCI aged 60–79 years. We developed simulations of ADLs that are typically difficult to practise repetitively, such as shopping, using public transportation, and driving, in a virtual environment. The activities were designed to include both target tasks and unexpected events, with difficulty levels adjusted according to user performance.
Results
We designed and implemented VR-based supermarket, bus, and driving programmes. Each programme first presents the training objectives to the users. The users start the activity by pressing a button when they fully understand their goals and are ready to proceed. During these activities, unexpected events occur, such as characters asking questions in the supermarket or on the bus and abrupt stops during driving. The endpoint is delineated by the training objectives. The programme ends when the user reaches the designated endpoint in the VR environment.
Conclusion
We developed a VR-based cognitive training programme to maintain ADLs and slow cognitive decline in patients with MCI.
Introduction
Alzheimer's disease is a degenerative disorder characterised by progressive decline in cognitive function. 1 Mild cognitive impairment (MCI) precedes major neurocognitive disorder, and the preservation of activities of daily living (ADLs) is a key distinction between these stages. 2 Thus, if ADLs are preserved for a long time, MCI may not progress to major neurocognitive disorder.
Cognitive function is mental processes involved in the acquisition of knowledge, manipulation of information, and reasoning. 3 Cognitive functions included the domains of complex attention, executive function, learning and memory, language, perceptual-motor function, and social cognition. 4 Among them, executive function is a higher-order cognitive ability that enables humans to achieve goals, adapt to novel situations, and manage social interactions. 5 It comprises subdomains such as working memory, planning, reasoning, problem solving, and organising. 6 These abilities are essential for performing complex ADLs, including managing finances, preparing meals, and maintaining personal hygiene. 7 ADLs are complex activities that enable individuals to function independently in daily life and are closely related to various cognitive functions.8, 9 Improvements in executive function enhance capabilities, such as planning, problem-solving strategies, and attention shifts, leading to better performance in daily activities and greater independence and quality of life.10, 11 In this study, we conceptualised executive function according to the widely cited unity and diversity model of executive function. 12
ADLs serve as both a precise indicator of functional status in individuals with cognitive impairment and a means of providing cognitive intervention through physical and mental activities aimed at maintaining them.13,14 Although executive function declines continuously as neurocognitive disorders progress, 15 repeated training targeting executive function has been shown to help maintain cognitive function and potentially delay progression. 16 However, despite evidence that cognitive training programmes can improve specific cognitive functions, previous studies often demonstrate limited generalisability to real-life ADLs. 17 Traditional cognitive intervention programmes focus narrowly on specific cognitive functions. 18 Real-life activities, however, are inherently complex and require the integration of multiple cognitive domains. This mismatch between cognitive intervention and the demands of daily living reduces the ecological validity of such interventions. 17 ADL-focused training with a clear goal, such as grocery shopping or using public transportation, is more likely to engage multiple cognitive domains and be perceived as relevant.19, 20 Incorporating unpredictable elements encountered in real-life may further maintain the stimulation intensity and foster adaptive problem solving. 21 To implement this, it would be necessary to prepare scenarios tailored to each individual and have a trainer conduct the training on a one-to-one basis. 22 To address these issues, self-training options must be implemented using digital technology.
Mobile applications and virtual reality (VR) are potential digital therapeutics solutions. Mobile applications offer high accessibility and various forms of service or game-based training; however, they are limited by their two-dimensional displays, which may not effectively simulate real-life activities. 23 By contrast, VR can create environments that closely mimic real-life situations, potentially enhancing ecological validity. 24 Given these advantages, we sought to explore how VR-based interventions could be optimally designed to support cognitive function in individuals with MCI, particularly through tasks related to daily life. However, key design questions remain unanswered, including how to identify and translate relevant cognitive targets into practical VR scenarios and how to promote long-term, self-directed use among older adults. A critical determinant of intervention effectiveness is sustained engagement. User engagement in cognitive training can be strengthened through personalised task design, progressive difficulty, immediate and meaningful feedback, and ease of use. These factors are particularly important for older adults undertaking self-directed programmes. 25
Therefore, we aimed to explore the following research questions to guide the development of VR-based digital therapeutics intended to prevent cognitive decline in patients with MCI.
Research question 1: Which cognitive domains associated with ADLs are most frequently targeted in existing cognitive training interventions for patients with MCI?
Research question 2: How can the identified cognitive domains be translated into VR-based training scenarios that simulate meaningful ADLs?
Research question 3: What design features are necessary to enhance user engagement and promote sustained, self-directed use of VR-based cognitive intervention in older adults with MCI?
Materials and methods
Study design
This study aimed to design a VR-based cognitive training programme for patients with MCI, using a targeted literature review as the foundation for identifying relevant cognitive domains and effective intervention strategies.
Target population: older adults with MCI
Our digital therapeutics are aimed at older adults with MCI. The inclusion criteria were as follows: (a) Age 60–79 years; (b) patients with MCI met the diagnostic criteria for minor neurocognitive disorder as determined by the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition 26 ; (c) the absence of major neurocognitive disorder according to physician judgment; and (d) a Clinical Dementia Rating global score of 0.5 and a memory domain score of ≥ 0.5. 27 The exclusion criteria were as follows: (a) Severe illness with an anticipated fatal outcome within three months; (b) language barrier, (c) severe uncorrected visual or hearing impairment, (d) presence of severe neurological disease or disorder, and (e) inability to provide informed consent.
Targeted literature review
We conducted a targeted literature review using PubMed, focusing on studies that implemented VR-based cognitive interventions for patients with MCI that were published between 2001 and 2024. Search terms included ‘virtual reality’ and ‘mild cognitive impairment’. Inclusion criteria were studies published in peer-reviewed journals involving VR-based cognitive intervention in individuals with MCI. Exclusion criteria included non-VR-based interventions, unrelated cognitive domains, and studies not involving older adults. Among a total of 436 studies, 45 clinical trials were initially retrieved. After excluding studies that did not match the target condition or intervention type, we selected 26 clinical trials for further reference.
Design principles
We prioritised VR technology for ADL training in this study because of the need to simulate daily activities that require the dynamic integration of multiple cognitive processes.
General principles for VR-based ADL training
To design an effective VR-based ADL training programme, we employed the following strategies.
Ecological validity: The tasks should simulate real-world environments to promote generalisability and engagement. Simultaneous engagement of multiple cognitive domains: Real-life tasks involve multiple executive functions. Thus, the tasks should integrate rather than isolate cognitive components.28,
29
Repetition with variation: Repetitive training improves learning, but variation is necessary to prevent rote memorisation and encourage adaptive problem solving.
30
Incorporation of interference: To train inhibitory control, programmes should include embedded distractors.31,
32
Programme format for short-duration training: Each session should be brief and self-contained to support scalability and adherence in older adults.33,
34
Self-directed use: The programme should be designed for autonomous use, with minimal therapist supervision to enable regular and flexible training.
35
Engagement-driven design: Features such as goal relevance, contextual realism, adaptive difficulty, and timely feedback should be integrated to promote sustained user engagement.
Theoretical basis of executive functions
We designed a virtual environment to implement cognitive training for executive functions while patients perform daily activities to help those with MCI maintain their daily living abilities. Executive function is a cognitive domain that consists of three core components: Inhibitory control, working memory updating, and cognitive flexibility. 36 Inhibitory control refers to the ability to suppress automatic or dominant responses while selectively attending to relevant stimuli, thereby enabling the execution of the intended actions.37– 39 Classic paradigms such as the Stroop and Go/No-Go tasks illustrate this component by requiring participants to inhibit a dominant, easier response in favour of a more effortful but correct one.40, 41 Working memory updating involves the active monitoring and manipulation of information held in short-term memory, allowing new stimuli to be integrated and outdated or irrelevant content to be removed. 42 This process plays a key role in decision-making and reasoning by maintaining task-relevant information in an accessible and flexible state. 36 Representative paradigms include the n-back and letter memory tasks, which require participants to update their short-term memory content in response to incoming information.43, 44 Cognitive flexibility refers to the ability to shift mental sets in response to changing circumstances.45, 46 This capacity supports adaptive behaviour in dynamic real-world contexts, allowing for the rapid reconfiguration of goals, response strategies, and attentional focus. 47 Cognitive flexibility is typically associated with verbal fluency, category fluency, and set-shifting tasks, such as the Wisconsin Card Sorting Test, where participants must infer new sorting principles after prior rules become invalid.48, 49 Using these three core components, higher-level executive functions, including reasoning, problem solving, and planning, are performed.12, 36 However, there is no universally accepted definition of executive function. Some researchers conceptualise it as a unitary capacity,50, 51 whereas others emphasise a fragmented set of relatively independent subdomains.52– 54 A widely supported contemporary view is the unity-diversity framework, which posits that these subcomponents are partially separable yet correlated processes that jointly support complex goal-directed behaviour.12, 55 Accordingly, each scenario was designed to engage a primary subcomponent while allowing dynamic integration to foster higher-order executive functioning.
Operationalisation and intervention development
Operationalisation of executive functions in VR task design
To translate this theoretical framework into implementable cognitive tasks, each VR scenario was designed to embed executive demands into daily living activities. The operationalisation focused on three primary components.
Inhibitory control: Tasks were designed to require the suppression of irrelevant information. Interference elements, attention-dividing stimuli, and conditions that require refocusing on task goals were incorporated to elicit inhibitory responses. Working memory updating: Tasks were constructed to require the continuous monitoring, retention, and revision of short-term information. This includes maintaining a set of items, tracking sequential events, and updating internal representations as task conditions change. Cognitive flexibility: Dynamic task conditions were applied to induce shifts in strategy. Scenarios include elements that require users to adapt to new rules, reorient to updated goals, or revise plans in response to changes in the environment.
These operational definitions ensure consistency across scenarios and establish a structured link between executive function theory and task design logic.
Scenario design and cognitive targets
Based on the findings of our targeted literature review, we identified three VR programmes that simulate daily tasks: Grocery shopping, public transportation use, and driving. A psychologist and three clinicians collaboratively developed the initial intervention concepts by mapping cognitive domains to realistic ADL-based scenarios. Through iterative discussions with technical experts, we differentiated intervention methods that would be more effective using the VR format from those better suited to other conventional digital applications. The final selection reflected tasks optimised for VR-based cognitive engagement.
Supermarket scenario
The supermarket task was designed to simultaneously engage inhibitory control, working memory updating, and cognitive flexibility. Participants performing this task must maintain and revise goal-relevant information, manage distractors, and modify search strategies based on item locations. These cognitive demands reflect the executive requirements of effective shopping in real life and align with the targeted executive function principles.
Bus scenario
The bus scenario was designed to target working memory updating and sequential reasoning. 56 Participants must encode route information, track sequential progression, and adjust decisions under varying levels of distraction and uncertainty. This scenario captures the executive demands inherent in public transportation use, including route selection and destination tracking.
Driving scenario
The driving scenario was designed to engage higher-order executive functions, such as planning, reasoning, and decision-making, emerging from the coordinated operation of inhibitory control, working memory updating, and cognitive flexibility 57 to adapt to unexpected events. In this task, participants must integrate visual cues, update route information, and adjust strategies in response to route changes or hazards. These demands reflect the coordinated executive processes required for daily driving.
Behavioural indicators captured in VR
The VR system automatically records detailed behavioural metrics that serve as measurable proxies for executive functioning. Each indicator corresponds directly to the operationalised components of inhibitory control, working memory updating, and cognitive flexibility. The executive function targets of each VR scenario and their corresponding behavioural indicators are presented in Supplemental Table 1.
Inhibitory control indicators: Reaction time and accuracy during distractor events are used to assess the efficiency of inhibitory responses, while commission errors following interference provide an index of failures to suppress inappropriate actions.58,
59
Difficulties in inhibitory control are reflected by failure to resume task goals after an interruption, indicating challenges in re-establishing goal-directed behaviour.
60
In addition, participants’ responses to sudden obstacles in the driving scenario capture real-time inhibitory control under unexpected conditions. Working memory updating indicators: Accuracy of item recall and list completion in the supermarket scenario is used to evaluate the ability to maintain and update goal-relevant information. Route-tracking errors and mismatches between the expected and actual bus stops indicate deficits in sequential updating.
61
Updating efficiency is further assessed through corrective actions, repeated checking behaviours, and adjustments following mismatches. The integration of spatial–temporal information during driving provides an additional indicator of dynamic monitoring and the revision of internal representations.
62
Cognitive flexibility indicators: Cognitive flexibility is assessed through the frequency of strategy shifts during item searches, reflecting the capacity to adapt to changing task demands. Adaptation to route information changes in the bus scenario capture flexible reorientation of goals and strategies.
63
Flexibility during driving is evaluated by examining the number and type of corrective manoeuvres made in response to unexpected environmental changes, and the effectiveness of re-planning during detours serves as a direct indicator of flexible problem solving.
57
Task efficiency and global performance metrics: Overall task efficiency is evaluated using total task completion time, path deviation and trajectory efficiency, and the frequency of hesitation periods or pauses, which serve as behavioural markers of uncertainty, cognitive overload, or decision-making difficulty.
64
Error-recovery patterns are analysed to assess compensatory strategies and adaptive control, and performance variability across progressive difficulty levels is used to reflect the capacity to respond to increasing executive demands.
These behavioural indicators provide objective, fine-grained measures of cognitive functioning in complex daily-living contexts and will support the future empirical evaluation of training effects as well as the development of automated difficulty-adjustment algorithms.65, 66
Development of the application and implementation
We developed VR cognitive intervention programmes that simulate ADLs and are tailored for patients with MCI. The programmes were designed to train executive functions in realistic, immersive environments. In parallel, we developed an interface for healthcare providers to issue prescriptions and adjust intervention levels as well as a dashboard for tracking patient activities. The application development followed a structured, iterative process involving interdisciplinary collaboration. The initial scenarios were drafted by a psychologist and three clinicians and discussed during an offline meeting with VR development technicians. The technicians created the first prototypes based on these inputs. This was followed by two rounds of online feedback sessions per programme. In each round, the interdisciplinary team evaluated the prototypes and suggested improvements in cognitive relevance, difficulty adjustment, and interaction design. A third and final round of online meetings was held to confirm the final version of each programme. This iterative process ensured the clinical relevance, technical feasibility, and cognitive integrity of the final application.
Planned neuropsychological evaluation for subsequent validation
Although the present study focused on the design and development of the VR-based executive function training programme, a subsequent usability and efficacy study is planned to evaluate the cognitive effects of the intervention using standardised neuropsychological measures. The primary battery will be the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease Neuropsychological Assessment Battery (CERAD-K), which provides validated assessments of global cognition and domain-specific functions relevant to MCI. 67 The battery includes measures of verbal fluency, the Boston Naming Test; the Word List Memory, Recall, and Recognition tests; the Constructional Praxis, the Constructional Praxis Recall; and the Trail Making Test (Parts A and B), which collectively enable cognitive flexibility, memory, language, and visuospatial function to be profiled. To specifically validate the executive function components targeted by the VR tasks, the CERAD-K battery will be supplemented with established executive measures, including the Stroop Colour-Word Test and the Digit Span Test forward and backward. These instruments assess inhibitory control, selective attention, and working memory capacity, thereby enabling convergence between traditional neuropsychological performance and VR-derived behavioural indicators. The evaluation plan will examine correlations between CERAD-K executive indices and VR metrics such as reaction-time variability, error profiles, strategy-shift frequency, and updating efficiency. This approach will provide construct validity for the VR-derived indicators and support future clinical application of the intervention. These assessments are not part of the current design study but will be incorporated in a subsequent validation trial.
Acceptability assessment and stakeholder feedback procedures
To evaluate the preliminary acceptability and usability of the VR programme, we conducted brief semi-structured interviews with a group of stakeholders, including three clinicians familiar with digital cognitive interventions. Participants interacted with prototype versions of the supermarket, bus, and driving scenarios, after which a short interview lasting about 10 min was conducted on the same day.
The interview guide focused on experiential feedback and the questions covered the following topics:
overall satisfaction with the VR programme; willingness to continue using the programme in the future; perceived ability to maintain concentration during use; feasibility of using the programme for more than 10 min per day; perceived realism and similarity to daily-life experiences; ease of use and clarity of the interactions; aspects of the programme that were the most enjoyable; and aspects that were the most inconvenient or difficult.
All interviews were audio-recorded and summarised in field notes. A rapid content analysis approach was used, in which two researchers independently reviewed the notes, identified recurring themes, and categorised feedback into usability, cognitive load, ecological validity, motion comfort, and hardware accessibility. Discrepancies were resolved through discussion. These findings will inform iterative refinements to the programme, including adjustments to scenario structure, difficulty calibration, and controller interaction methods, as well as locomotion techniques for reducing motion sickness.
Ethics approval and consent to participate
This study involved stakeholder feedback interviews with clinicians and did not involve patients. The protocol describing the development and design process of a VR cognitive training programme was reviewed by the Kangdong Sacred Heart Hospital Institutional Review Board, which granted an exemption from ethics approval and informed consent requirements. (KANGDONG 2025-07-009)
Results
To provide a structured overview of our process, we present the results in three stages: (1) Findings from a targeted literature review, (2) the conceptual design of the intervention informed by these findings, and (3) the technical development and implementation of the VR programmes.
Targeted literature review
MCI and executive function
MCI is often accompanied by deficits in executive function, playing a critical role in managing daily activities and adapting to novel situations. Conventional training methods typically focus on specific subdomains such as working memory or problem solving. In contrast, VR provides an immersive experience that closely simulates real-life situations, enabling comprehensive training of executive function as a whole. 68 Numerous studies have reported that VR training improves executive function in patients with MCI.10,11, 68 –79 However, evidence for these effects remains unclear. Some studies have reported only modest or domain-specific gains, 80 suggesting that although VR shows potential, its effectiveness in generalised executive improvement remains inconclusive. In executive function training, the optimal level of stimulation is one that is slightly above the participant's current ability, providing a challenge that is achievable yet sufficiently demanding to stimulate cognitive adaptation. 81 As tasks become familiar and the patients adapt, the difficulty should be progressively increased beyond the current level to ensure continuous improvement. This principle aligns with the concept of progressive difficulty, which is recognised as a key factor for sustaining user engagement in cognitive interventions, particularly among older adults engaging in self-directed programmes. 25 Tasks that are too difficult can be overwhelming and lead to disengagement, whereas overly simple tasks may quickly result in a loss of interest. 82 Thus, adjusting task difficulty dynamically to match and slightly exceed each patient's evolving threshold is essential for the effective simulation of ADLs and maintaining long-term participation.
Optimal training time for VR in cognitive training
Previous studies on cognitive training using VR involved 20–100 min of stimulation per session, conducted 1–3 times per week over a period of 6–12 weeks. These sessions showed significant group-by-time interaction, indicating that the participants exhibited improvements over time with the training.70, 72 However, in certain cases, the improvements were modest and not sustained at follow-up. Furthermore, considerable variability in intervention duration and frequency across trials introduces uncertainty regarding the optimal training dose.
VR technologies, while promising, have notable technical constraints and usability challenges. While immersive and effective for simulating real-life cognitive tasks, VR equipment requires a controlled setup and special devices that can limit accessibility. Additionally, prolonged exposure to VR can cause motion sickness, headaches, and disorientation, with research suggesting that these symptoms often appear after approximately 20 min of continuous use. Consequently, the practical application of VR in cognitive training should generally be limited to shorter sessions of approximately 20 min to maintain comfort and minimise side effects (https://securecdn.oculus.com/sr/oculusquest-warning-english). Based on these findings, the present programme was deliberately designed to incorporate brief but repeatable sessions that maximised usability and safety while supporting sustained engagement. This approach directly addresses uncertainties regarding training duration, as well as concerns about potential side effects and user fatigue reported in earlier research.
Previously developed mobile applications and VR programmes
To date, mobile applications developed for cognitive training include one designed for post-stroke patients, 83 a programme for individuals with early-stage Alzheimer's disease, 84 and a programme targeting older adults with subjective cognitive decline. 85 VR programmes for individuals with MCI have been developed and studied in countries such as Italy, Hong Kong, the United States, China, South Korea, and Belgium, with reported outcomes indicating improvements in both global cognitive and executive functions. 86 However, these applications and VR programmes exhibit significant methodological limitations. Specifically, they were characterised by small sample sizes,68,71,72,74,76,77, 83 short intervention periods,68,69,72,73, 76 and the absence of long-term follow-up.70,77,78, 84 –86 In addition, there was substantial heterogeneity in VR protocols, ranging from the use of commercial gaming platforms such as Kinect 73 to task-specific simulations such as virtual shopping 68 and mixed reality systems. 72 This variability complicates comparisons across trials and is highlighted as a limitation of this meta-analysis. 86 While most studies have reported improvements, some have noted modest or short-lived effects, suggesting that generalisation to daily life remains uncertain. These mixed outcomes underscore the methodological limitations of previous VR-based interventions and highlight the need for more rigorous and standardised research designs to improve both interpretability and generalisability.
Intervention design
Among the various ADLs, such as setting the table for meals, organising items during cleaning, visiting a grocery store, selecting items at multiple stores, using kiosks, navigating without a GPS, using public transportation, and making phone calls with memorised numbers, we selected grocery shopping, public transportation, and driving as suitable activities for VR implementation after evaluating their alignment with the design criteria. We designed the following three VR cognitive intervention programmes.
VR supermarket
In the design of this programme, users are presented with a shopping list. They must then place the items from the list in a cart and reach the checkout to complete the task. The list includes 3–8 items, depending on the difficulty level, and the quantity for each item (1–9) is randomly chosen. After the first item has been added to the cart, an unexpected situation occurs: a question is presented to the user. The user must answer the question and continue shopping. Item categories are displayed on the ceiling, and users are required to check the category of each item before adding it to the cart, and adding an extra layer of information processing. Each item immediately disappears when added to the cart. Therefore, if users do not remember how many items they have collected, they may not be able to determine the total. The task terminates automatically when all items have been collected and checked, or after ten minutes. To ensure that users do not become too familiar with the programme settings through repeated use, the information about categories, item types, and quantities is designed to exceed ten times the required amount. The components of the VR Supermarket programme and their respective target cognitive domains are presented in Table 1.
Components of the virtual reality (VR) supermarket programme

VR bus
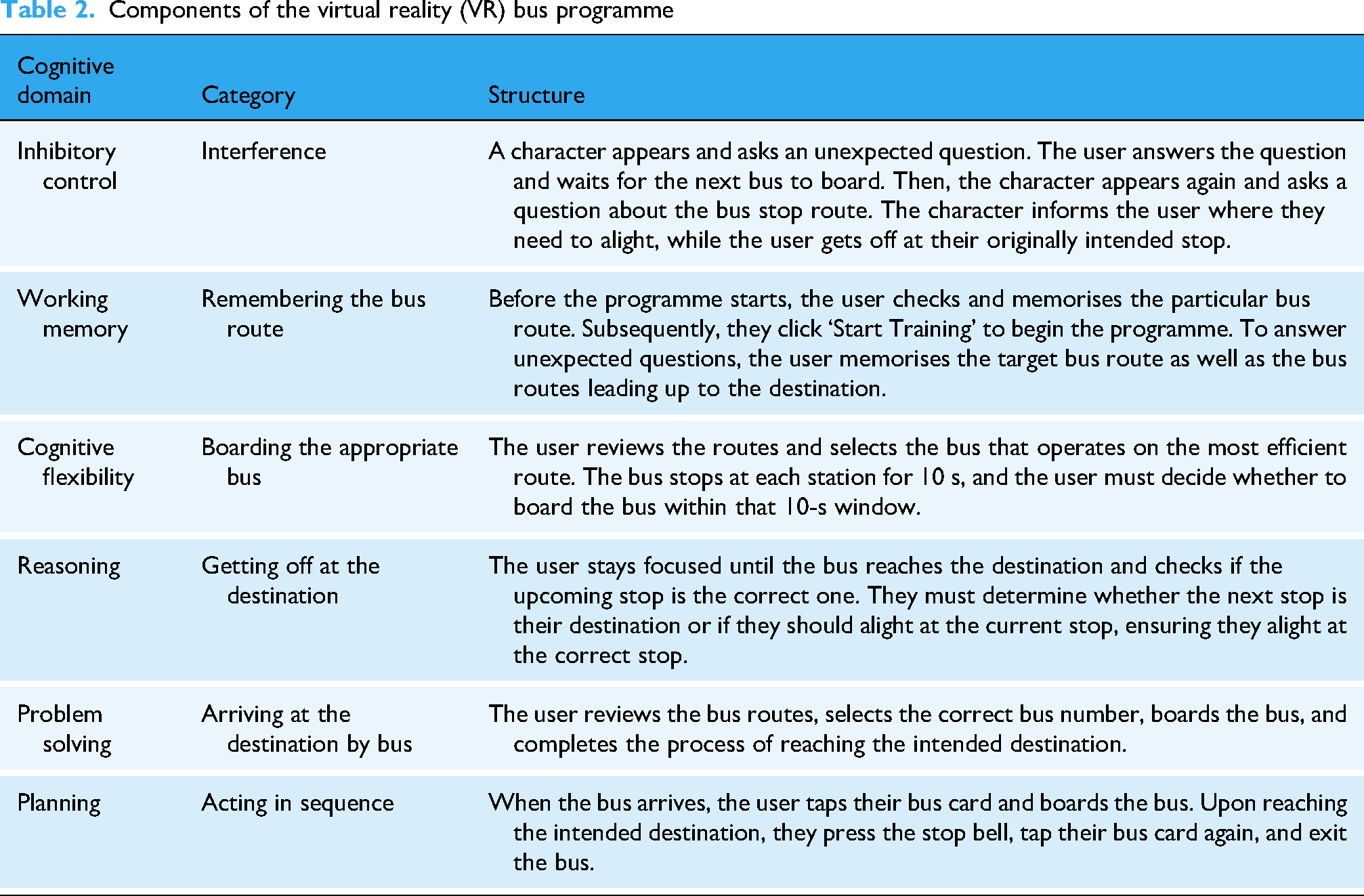
The VR Bus programme presents users with their current locations and destinations. Users must examine the route map to select an appropriate bus from their current location to the destination and board the bus. While on the bus, users should follow the information provided on the digital display of the bus and as announcements to determine when to leave. Users are required to scan their bus cards when boarding and alighting, simulating the tasks they would perform on a real bus ride.
Three unexpected questions are posed during the task. To answer these questions, users should remember the bus stops they have passed on their route to the destination, which ranges from three to seven stops depending on the difficulty. Approximately 400 real bus stop names in Seoul, excluding those with details that are difficult to display, were stored in the database. At the start of each task, the programme randomly selected these names to generate the training content. This approach helps prevent users from relying on previously memorised bus stop information and encourages learning through the programme rather than the use of pre-existing knowledge. The components of the VR Bus programme and their respective target cognitive domains are presented in Table 2.
Components of the virtual reality (VR) bus programme
VR driving
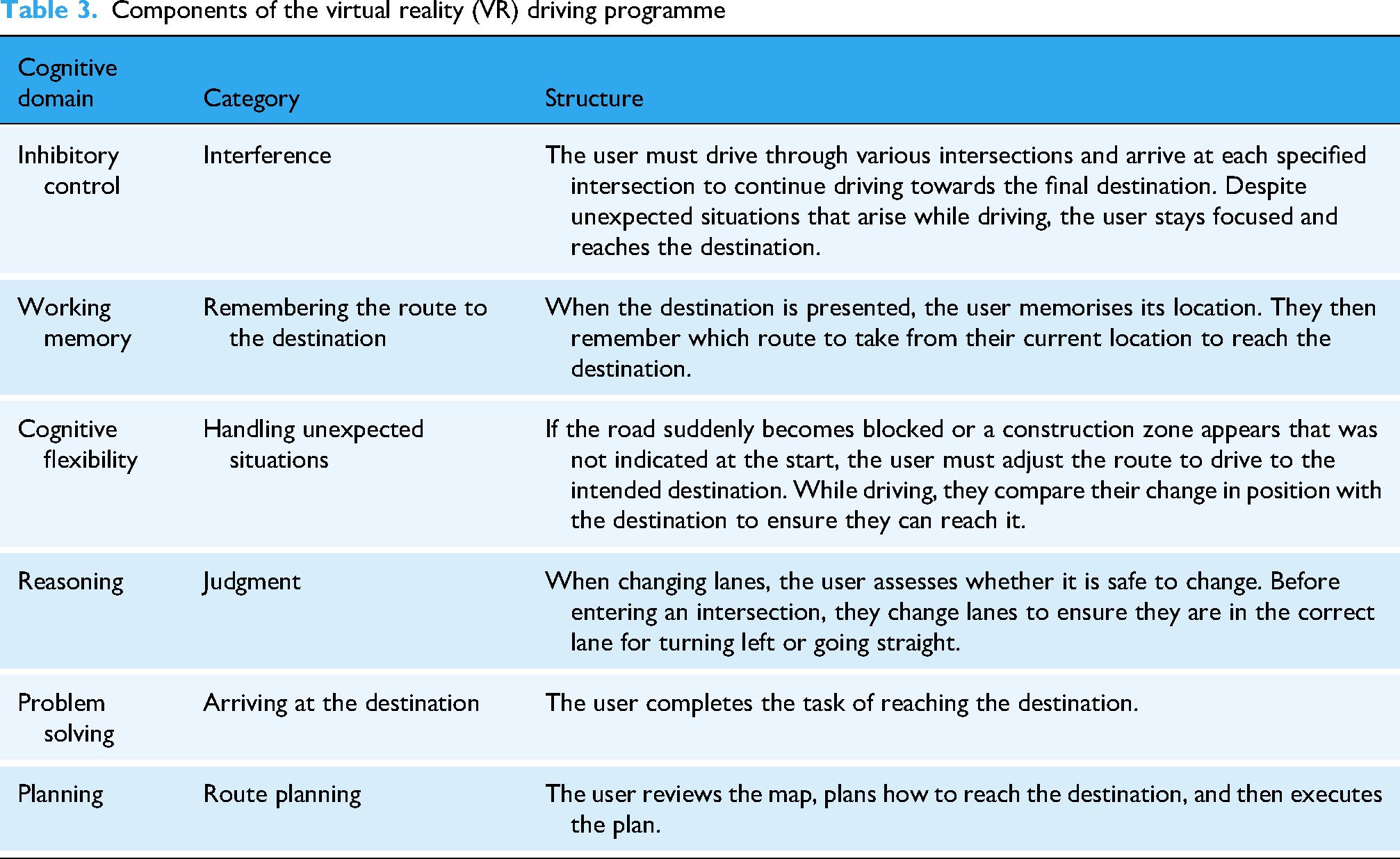
This programme is designed such that the current location and destination are shown on the map, and users are provided with the intersections that they must pass through to drive to the destination. A three-lane road is displayed, and at each intersection, users must determine the direction based on the lane: Left turn – first lane, straight – second lane, and right turn – third lane.
If the user turns the steering wheel towards the desired lane for three seconds, a lane change occurs automatically. At this time, users must check the rearview mirror to ensure that no cars have entered the lane and so they can change lanes without collision. The programme was designed to continuously insert memory information related to the attention tasks that must be performed when driving an actual vehicle.
In addition, random situations, such as collisions with randomly generated vehicles, traffic violations, entry into areas restricted because of construction, and collisions with preceding vehicles suddenly braking, are included in this programme. Users must make judgments about accidents and return to the starting point to repeat the tasks. Intersection names are randomly presented to prevent users from performing programmes based on pre-existing knowledge. The components of the VR Driving programme and their respective target cognitive domains are presented in Table 3.
Components of the virtual reality (VR) driving programme
Development of VR cognitive intervention programmes
VR supermarket
According to the design of the programme, when the training begins, a shopping list is presented to the user detailing the items to be purchased and the quantity of each item. The items and quantities provided vary according to the difficulty level. After reviewing the shopping list thoroughly, the user can start the training by pressing the ‘Start Training’ button at their desired time. The start screen of the VR Supermarket programme is presented in Figure 1.

Start screen of the virtual reality (VR) Supermarket programme.
After the training begins, unexpected questions are presented by a character in a manner that simulates an event. The character appears during the shopping process and induces an interference effect by asking questions that are unrelated to the shopping items. The scene in which interference factors appear in the VR Supermarket programme is presented in Figure 2.

Scene in which interference factors appear in the virtual reality (VR) Supermarket programme.
When the trainee has completed the training, the medical staff obtains the trainee's performance data, which includes the accuracy and total performance time as well as the time-stamped movement path data. By analysis of these data, they can identify the difficulties that users experience and derive areas for improvement. The user management screen of the VR Supermarket programme is presented in Figure 3.

User management screen of the virtual reality (VR) Supermarket programme.
VR bus
As per the programme's design, when the training begins, the user is provided with information about their current location and destination. The start screen of the VR Bus programme is presented in Figure 4.

Start screen of the virtual reality (VR) Bus programme.
When the user presses the ‘Start Training’ button, the information about the current location and destination disappears, and a bus-stop environment is presented. The user must observe the route map, remember the correct bus information required to reach the destination from their current location, and accurately decide whether to board each incoming bus. The route map viewing screen in the VR Bus programme is presented in Figure 5.

Route map viewing screen in the virtual reality (VR) Bus programme.
If a user decides to board a bus, they must check the bus numbers sequentially and board the appropriate bus. During this process, they perform the common action of using a transportation card, which is typically used on Korean buses. The electronic display at the front of the bus shows information about the current and next stops, allowing users to repeatedly compare this information with what they memorised. During the bus ride, unexpected questions are added as events. These questions are about specific stops other than the destination. This encourages the user to memorise multiple stop names and the next stop as they progress towards their destination. The scene in which interference factors appear in the VR Bus programme is presented in Figure 6.

Scene in which the interference factors appear in the virtual reality (VR) Bus programme.
VR driving
In the VR driving training programme, when a session begins, information regarding the current location and destination is presented on a map. Location details are provided visually on the map, whereas the names of the intersections that the user needs to pass through are displayed in text at the bottom. Users must memorise the map and intersection names sufficiently. When they feel ready to proceed, they can press a confirmation button to start the programme. The start screen of the VR Driving programme is presented in Figure 7.

Start screen of the virtual reality (VR) Driving programme.
When the user presses the confirmation button, the screen transitions to the interior of the car, functioning similarly to a driving simulation. The programme is designed to allow users to navigate towards a target destination by interacting with various situations and road signs on a three-lane road. When the user reaches the desired location, the programme ends. The driving screen in the VR Driving programme is presented in Figure 8.

Driving screen in the virtual reality (VR) driving programme.
When the programme ends, the medical staff can obtain the user's performance data, including the route the user travelled and the time taken to pass each point. This detailed information enables a comprehensive analysis of user performance during the simulation. The user management screen of the VR Driving programme is presented in Figure 9.

User management screen of the virtual reality (VR) Driving programme.
Acceptability based on stakeholder feedback
The supermarket programme was perceived as the most realistic and engaging, with an appropriate level of difficulty. Some participants reported dizziness during smooth locomotion, which was subsequently addressed by adopting teleportation locomotion. In addition, while the Oculus system typically requires applying two hand-held controllers, stakeholders suggested that operating the programme with a single controller was cognitively less demanding and more accessible to older adults, thereby enhancing its overall usability. The bus programme was regarded as less engaging, because the waiting period until arrival was considered tedious, and the associated memory load was occasionally excessive. The driving programme was described as enjoyable and realistic but required additional hardware such as pedals and a steering wheel, raising concerns about accessibility. Moreover, a higher level of difficulty was perceived as potentially discouraging, with an increased risk of discontinuation. Overall, stakeholders ranked the scenarios in order of preference: supermarkets, driving, and buses.
Discussion
Each task was developed to ensure that successful performance necessarily involved specific executive processes, allowing users to practise inhibitory control, working memory updating, and cognitive flexibility in realistic situations. In the supermarket scenario, remembering shopping items requires the maintenance and continuous updating of goal-relevant information as users check off purchased items and plan subsequent actions, whereas ignoring irrelevant stimuli such as non-target products demands inhibitory control. Furthermore, navigating aisles and locating specific products among multiple similar options involve cognitive flexibility, because users must switch search strategies and adapt to changing task conditions. 87 The supermarket task parallels the dual-task paradigms involving selective attention and cognitive switching. 45 Supermarket tasks provide supplementary cognitive benefits in addition to these executive components. Shopping is a familiar and essential activity in daily life, and its complex visual and semantic environments offer opportunities for training memory strategies. 68 By presenting each target item with both a picture and word label, the programme engages both verbal and visual memory, facilitating dual encoding and enhancing recall efficiency. 88 The gradual increase in the number and type of items following the standard item-number format used in memory training further supports the activation of memory habits and encourages users to develop effective mnemonic strategies for managing multiple pieces of information.89, 90 In the bus scenario, bus routes consist of a long chain of connected stops that must be remembered and updated in real time in an A-B-C linkage, exemplifying meta-information processing. 91 By simulating real-time route information, boarding, and alighting, the programme required participants to continuously update their internal representations of spatial and temporal information. 92 This dynamic updating process parallels the mechanisms underlying n-back or letter memory tasks but is implemented within a realistic transportation context. 93 Using the bus is a cognitively demanding daily activity that engages higher-order processes, such as monitoring, anticipation, and adaptive updating. This demand fosters executive flexibility, which is essential for real-world navigation. 94 The driving scenario requires real-time processing of complex visual information, including route confirmation, lane changes, and response to traffic signs or obstacles under time constraints.95, 96 The task introduces interference, such as unexpected detours or roadblocks, to elicit adaptive control and error regulation. Driving thus represents a highly dynamic real-world activity in which multiple executive components must operate in a coordinated manner, requiring immediate judgment and rapid information integration.
Our programme includes interference from non-player characters asking questions in the supermarket and bus environments because, in real life, distractions can reduce focus when shopping or taking the bus. These ecological distractions were intended not only to enhance realism but also to manipulate selective attention demands. By requiring users to regulate competing information streams, this design element supports the development of executive function training. 97 In the driving environment, while there were no non-player characters asking questions, interference existed in the form of rearview mirror checks, sudden obstacles on the road, or detours due to road construction. These various forms of interference help maximise executive function training.
In addition to cognitive training, feedback based on cognitive assessments is important for executive function training. If a programme is very easy or difficult for the user, it will fail to provide proper stimulation. Therefore, programmes should be slightly challenging but achievable and motivate users to engage in cognitive training. 98 Offline cognitive training methods have limitations in that they cannot immediately adjust levels based on user reactions. However, digital devices allow for real-time data collection, such as user reactions during performance. This enables a more precise level adjustment. Although applications rely on button-click logs for user response data, VR can capture more detailed information, such as the user's path and the information acquisition process. By tracking eye movements and user movements in VR, activity patterns can be analysed repeatedly, allowing for more concrete data on task performance. 99 Maintaining long-term engagement is essential for ensuring the effectiveness of cognitive interventions. 25 To enhance user engagement, we prioritised the implementation of a level system and integrated real-time feedback in all three programmes. These mechanisms are designed to maintain optimal challenge and reinforce a sense of competence, thereby supporting sustained participation over time. A major challenge in cognitive training is limited transfer of task-specific gains to untrained daily activities. 100 This lack of generalisation likely reflects not only contextual differences but also the interaction between the motivational and cognitive components of engagement. 101 Motivation influences persistence and willingness to exert effort, whereas the cognitive component is closely related to executive control. 102 When motivational drive is high but executive aspects are not sufficiently activated, participants may exert effort inefficiently. Conversely, when cognitive control is strong but intrinsic motivation is low, they may disengage early. From a neurocognitive perspective, this interaction aligns with models of motivational–executive coupling where dopaminergic reward sensitivity modulates prefrontal control, thereby influencing persistence and transfer efficiency. 103 Therefore, effective transfer requires the co-activation of both systems through adaptive challenge that sustains interest while promoting strategic regulation. 104 Our programme was designed with this principle in mind, progressive difficulty and personalised feedback were used to maintain optimal challenge and reinforce a sense of competence, 105 while task dynamics require continuous monitoring and adjustment, thereby engaging executive control mechanisms. 106 The integration of motivational and cognitive engagement was designed to consolidate learned strategies and enhance real-world transfer.
Previous VR-based cognitive training studies have exhibited several key limitations that motivated the design of the present programme design. First, several previous interventions targeted a single or narrow cognitive domain and employed fixed repetitive task structures. 107 This approach limits the ability to understand the multidimensional nature of executive functioning. Therefore, our programme was designed to integrate multiple executive subcomponents within an ecologically valid and dynamically changing ADL contexts. Second, early studies frequently suffered from methodological limitations, such as short intervention durations, small sample sizes, and limited personalisation, which likely restricted the generalisation of training effects to daily life. 86 In contrast, our system incorporates adaptive difficulty, contextually meaningful tasks, and iterative stakeholder feedback to promote sustained engagement and enhance ecological validity. Third, most of the existing VR-based cognitive training literature conceptualises cognitive enhancement as a technical rather than a theoretical challenge, often prioritising task realism or user engagement over mechanistic validity. 108 However, the cognitive processes in immersive VR environments may fundamentally differ from those in traditional laboratory settings. 109 Therefore, cognitive training should not merely replicate conventional paradigms in virtual space but be redefined to reflect the unique characteristics of VR. Recognising these limitations, our programme was explicitly grounded in the unity-diversity framework of executive functions12, 36 linking theoretical models of cognitive control with adaptive and ecologically valid task designs to enhance interpretability and real-world transfer. Within this design framework, we distinguished between core cognitive principles and adaptable implementation elements. The core cognitive principles include mechanisms, such as inhibition, working memory updating, and cognitive flexibility, which serve as consistent theoretical targets across all scenarios. The adaptable elements involved modifiable design features, including task difficulty, feedback timing, and interaction methods, which could be adjusted according to user feedback, technical feasibility, or clinical context. This structure maintains theoretical coherence while enabling iterative refinement and personalisation. Furthermore, progressive difficulty was implemented to engage executive monitoring and cognitive flexibility by requiring users to adapt to changing task demands, whereas feedback mechanisms enhanced metacognitive regulation and self-directed learning. These design strategies were not only technical optimisations but also theoretically grounded applications of executive function principles, aiming to bridge laboratory-based paradigms and real-world cognition.110, 111
In addition to the cognitive considerations, stakeholder feedback provided insights into the acceptability of the three scenarios. The supermarket programme was regarded as realistic and engaged, with appropriate difficulty. However, some participants reported dizziness during smooth locomotion. Therefore, teleportation locomotion was adopted for our programme. Because the target population consisted of older adults, it was difficult for them to walk around during the task because of safety concerns, and they were required to remain seated. Nevertheless, the visual scene continues to move, which increases the likelihood of dizziness depending on the locomotion method. Previous studies have reported that teleportation locomotion reduces dizziness, 112 therefore, we adopted teleportation locomotion in the present programme. However, this method may reduce ecological validity, which warrants further investigation. The stakeholder also indicated that using two controllers simultaneously was less suitable for older adults, particularly for those with cognitive decline. Barriers to controller use may have led participants to abandon the programme altogether. 113 Therefore, simplifying the controller operations and enabling single-hand operations may provide a more accessible approach for developing VR cognitive training programmes. The bus programme was perceived as less engaging owing to the long waiting times for arrivals and excessive memory demands. After boarding the bus, the participants had limited activities available until the bus arrived at the destination, resulting in a sense of passivity and boredom. It has been reported that people begin to feel bored after approximately five minutes, 114 indicating that the waiting time inside the bus should be limited to less than this threshold. Alternatively, additional activities can be incorporated to make the bus more engaged during the waiting period. The driving programme was described as realistic and immersive, and the participants considered it enjoyable, similar to a game. However, concerns have been raised regarding accessibility owing to the need for additional hardware and the possibility of discontinuation because of its higher difficulty level. To increase ecological validity, actual steering wheels and pedals were used; however, operating these devices required cognitive resources, which in turn made it more difficult for participants to remember the route to the destination. Prior research has demonstrated that accessibility to hardware, such as interactive devices, can significantly affect user acceptability. 115 In addition, because the programme primarily provided novel visual stimulation combined with a sense of speed inherent to driving, the participants perceived the task as more difficult. 116 These findings indicate that acceptability depends not only on ecological validity, but also on engagement, memory load, and hardware accessibility.
This study has several limitations. First, although the design process was informed by a targeted literature review, this approach inherently limits comprehensiveness and transparency compared to a systematic review. Because the review selectively focused on executive function theories and VR-based cognitive training frameworks, relevant studies outside these domains may have been overlooked, introducing a potential selection bias. This partial presentation of the literature may also limit the generalisability of our conceptual model across cultural, technological, or clinical contexts. Future research should adopt a systematic or scoping review methodology to ensure more balanced, reproducible, and inclusive theoretical foundation. Second, while our VR system can capture rich performance data, such as movement paths, we did not implement automated, real-time level adjustments based on these data in the current version due to technical constraints. This feature will be considered in future prototype development to enhance adaptability and personalisation. Third, feasibility and acceptability were assessed through qualitative stakeholder feedback rather than validated instruments, and stakeholder diversity was limited. Therefore, future studies should include a broader range of participants and employ standardised usability and acceptability measures to provide more rigorous and generalisable evidence. Finally, as members of the development team were involved in the evaluation, potential bias cannot be entirely excluded. This risk may be mitigated by including independent stakeholder feedback during the design process. Future studies should address this issue by incorporating blinded or externally conducted assessments to ensure objectivity.
Conclusion
We developed and implemented a VR-based cognitive training programme tailored to maintain ADL in patients with MCI. The study aimed to improve cognitive function and maintain ADL in patients with MCI by implementing cognitive training targeting executive function in environments similar to real-life settings. By incorporating random variables, the training was designed to provide novel stimuli even during repetitive practice, preventing user boredom. Additionally, user interaction data was recorded to lay the groundwork for developing a level-based system tailored to individual user profiles. Future system development will aim to create an automated, level-based VR training programme for executive function in patients with MCI.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261415852 - Supplemental material for Design and implementation of virtual reality-based cognitive training programmes for patients with mild cognitive impairment: Development study
Supplemental material, sj-docx-1-dhj-10.1177_20552076261415852 for Design and implementation of virtual reality-based cognitive training programmes for patients with mild cognitive impairment: Development study by Hayeong Choi, JaeKyoung Shin, Ji H Kim, Hyojun Cho, Sang-Kyu Lee and Moo-Eob Ahn, Yeo J Kim in DIGITAL HEALTH
Footnotes
Author contributions
Conceptualisation, Hayeong Choi, JaeKyoung Shin and Yeo Jin Kim; Funding acquisition, Yeo Jin Kim; Methodology, Sang-Kyu Lee and Moo-Eob Ahn; Software, Hyojun Cho; Visualisation, Hayeong Choi and Ji Hye Kim; Writing – original draft, Yeo Jin Kim; Writing – review & editing, JaeKyoung Shin.
Funding
This research was supported by National Research Foundation of Korea (NRF) grant funded by the Korean Government [grant number NRF-2022R1A2C1011286; RS2022NR069669]. This research was also financially supported by the Ministry of Small and Medium-sized Enterprises(SMEs) and Startups(MSS), Korea, under the “Supporting Project for boosting a Local Innovation Leading Company(R&D), S3453280” supervised by the Korea Technology and Information Promotion Agency for SMEs(TIPA).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data generated during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.