
Abstract
Introduction—
Performing cardiopulmonary resuscitation (CPR) in microgravity is challenging due to reciprocal motion between the patient and operator, requiring unique methods of stabilization for chest compressions. In this study, the Polaris Dawn mission crew evaluated optimal methods of CPR administration in the Dragon spacecraft during spaceflight as well as the impact of CPR tasks to the vehicle.
Methods—
CPR was simulated by compressing a CPR Adult Manikin Bellows Piston with Clicker against different surfaces of the vehicle. Crew members performed compressions at 3 different locations to select the optimal worksite. All 4 crew members then performed a 2-min round of compressions at the optimal worksite. Workload was measured using the Bedford workload and Borg rating of perceived exertion scales, where lower scores are desirable for both scales. Vehicle impacts were monitored with navigation and carbon dioxide sensors.
Results—
The outboard seat was selected as the optimal worksite. When performing a full 2 min of chest compressions at this location, average Bedford workload and Borg rating of perceived exertion scores among all 4 crew members were 4.75 and 16, respectively. All 4 crew members achieved the target-frequency range (mean, 1.8 Hz; range 1.7–1.9 Hz). Vehicle accelerations were observed in all axes, and cabin carbon dioxide increased to a peak level of >3.6 mm Hg, triggering a carbon dioxide caution limit.
Conclusions—
Outboard seat location provided the best ergonomics for administration of CPR on the Dragon spacecraft, although task performance had high difficulty ratings. CPR also was associated with elevated cabin carbon dioxide and vehicle accelerations, as measured by the navigation system.
Introduction
Cardiac arrest is a life-threatening emergency. Despite a low likelihood of cardiac arrest occurring in spaceflight, it carries high consequence as a potential threat to crew life and mission success. Some have postulated that the microgravity environment may be arrhythmogenic, with risk factors including cardiac atrophy, prolonged QT interval, elevated catecholamine levels, electrolyte disturbances, and oxidative stress, although a definitive link between microgravity and cardiac arrythmia has yet to be shown. 1 Other in-flight medical events also may present risk for cardiac arrest, including toxic exposures, hypoxia, electric shock, and trauma.
Primary prevention of in-flight cardiac arrest includes screening crew for cardiac history prior to spaceflight. Crews are also trained in basic life support response, including the administration of cardiopulmonary resuscitation (CPR) in the event that cardiac arrest does occur. However, performing CPR in a microgravity setting is challenging due to reciprocal motion between the patient and operator, requiring unique methods of stabilization for chest compressions. A number of CPR methods to secure both the patient and the operator in microgravity have been described previously.2–7
On the International Space Station (ISS), there are well-established methodologies for CPR administration. The most common method involves securing the patient with the Crew Medical Restraint System while the operator delivers chest compressions through the handstand technique with their feet on the ceiling. 2 However, due to differences in the internal volume and configuration of the SpaceX Dragon spacecraft, optimal techniques for administration of CPR in this vehicle have yet to be defined. In this study, the Polaris Dawn mission crew evaluated optimal methods of CPR administration in the Dragon spacecraft during spaceflight as well as the impact of CPR tasks on the vehicle.
Methods
During the Polaris Dawn mission, an in-flight demonstration of chest compressions was performed by the 4 investigator crew members using a CPR Prompt Adult Manikin Bellows Piston with Clicker (AED Superstore, Woodruff, WI), hereafter referred to as bellows (Figure 1). CPR was simulated by compressing against the bellows in various vehicle locations. Audible clicks from the bellows provided the operator with positive feedback on sufficient compression depth.

Cardiopulmonary Resuscitation Prompt Adult Manikin Bellows Piston with Clicker (AED Superstore, Woodruff, WI).
Subjects
The investigator crew members included 2 males and 2 females, with ages ranging from 30 to 50 y and height ranging from 165 to 188 cm. All 4 crew members underwent CPR training, with Basic Life Support provider certification achieved per the guidelines of the American Heart Association. All crew members also successfully completed preflight physical examinations. Two of the 4 crew members underwent additional focused medical officer training involving ∼40 h of hands-on hospital training.
Protocol
The first study aim was to evaluate different worksites within the cabin to identify the optimal site and patient/operator configuration for CPR administration. Three worksites and associated patient/operator configurations were tested by the investigators: 1) outboard seat, where the patient would be secured via seat restraints and the operator positioned upside down with buttocks and legs braced against ceiling and sidewall hand rail; 2) inboard seat, with the patient secured via restraints in the seat and the operator upside down with legs braced against ceiling and light ring with back braced against the control panel; and 3) inboard seat bottom, where the leg rests of the seat have been removed and the patient is positioned with their back pressed against the outer base of an inboard seat and the operator is positioned in front of them using stairs to brace and push against them (Figure 2). Thirty seconds of compressions into the bellows was performed by a crew member at each worksite.
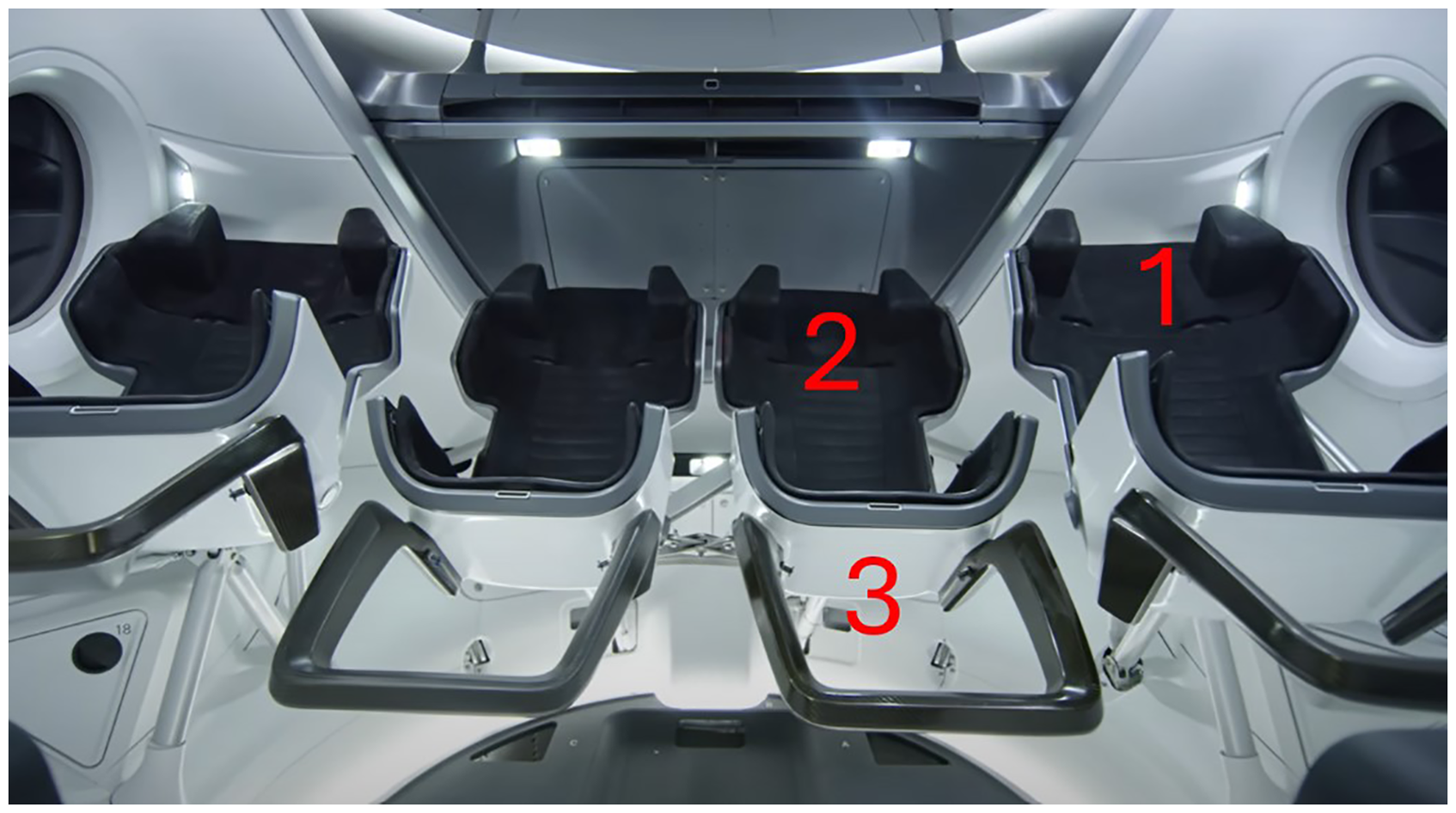
Internal structure of a four-seat Dragon spacecraft configuration with two inboard seats and two outboard seats.
Data collected for each worksite included: audio/video recording to enable postflight analysis of compression rate (as determined by bellows’ click rate) and compression effort. Compression effort was evaluated using 2 self-rated scales, the Bedford workload scale (a unidimensional rating scale from 1 to 10 designed to identify an operator's spare mental capacity while completing a task—with 1 indicating workload insignificant and 10 indicating tasks abandoned), and the Borg rating of perceived exertion (RPE, a quantitative measure of perceived exertion during physical activity, on a scale of 6–20, with 6 indicating no exertion and 20 indicating maximal exertion). The Borg RPE was developed with a lowest possible score of 6 so that scores could be easily converted to an estimated heart rate by multiplying each score by 10, where no exertion would represent an estimated resting heart rate of 60 beats/min. 8
After the preferred site was selected by the crew in the first task, the next aim was to determine the compression rate, compression effort, and vehicle impacts for a full round of CPR at the preferred worksite. Each of the 4 operators attempted 2 min of compressions at the preferred site. The same dataset was compiled for each of these 2-min compression sets: audio/video recording, Bedford workload, and Borg RPE. Vehicle impacts were assessed using navigation sensors to measure vehicle accelerations in all 3 axes as well as monitoring cabin carbon dioxide (CO2) concentration throughout the task with vehicle CO2 sensors. A 2-min duration was chosen for this final evaluation because current CPR recommendations are to switch operators delivering compressions every 2 min due to declining compression quality from fatigue. 9
Data Analysis
The audio/video files from the in-flight compressions using the bellows were analyzed postflight using MATLAB (MathWorks, Natick, MA). For each recording, the portion with rhythmic CPR was selected and first filtered for high frequencies that would correspond with the bellows clicking. A fast Fourier transform was then performed to determine the peak frequency of each compression set. The target frequency for chest compressions is 1.67 to 2 Hz (100–120 compressions/min). Audio/video files also were reviewed for commentary on the worksites and configurations.
Survey data from each operator and compression set were compiled to compare reported Bedford workload and Borg RPE. After the flight, key vehicle parameters including CO2 and vehicle accelerations measured in 3 axes were reviewed and assessed for their relation to the CPR tasks.
Results
Selection of Optimal Worksite
In the first task, an operator performed compressions for 30 s at each of the 3 worksites to determine the optimal worksite. The outboard seat received the lowest Bedford workload and Borg RPE ratings of all 3 locations. A second trial of compressions also was performed with a different operator at the outboard seat only. In this trial, the second operator assigned this location the lowest Bedford workload rating compared with all assessments performed by the operator in the first trials but also assigned this location with the highest Borg RPE rating compared with all assessments performed by the operator in the first trials (Table 1). A combination of workload scores and discussion among crew members was used to select the outboard seat location and configuration as the preferred location for chest compressions in this vehicle.
Bedford workload and Borg rating of perceived exertion (RPE) at each of the three worksites during the optimal worksite selection task.
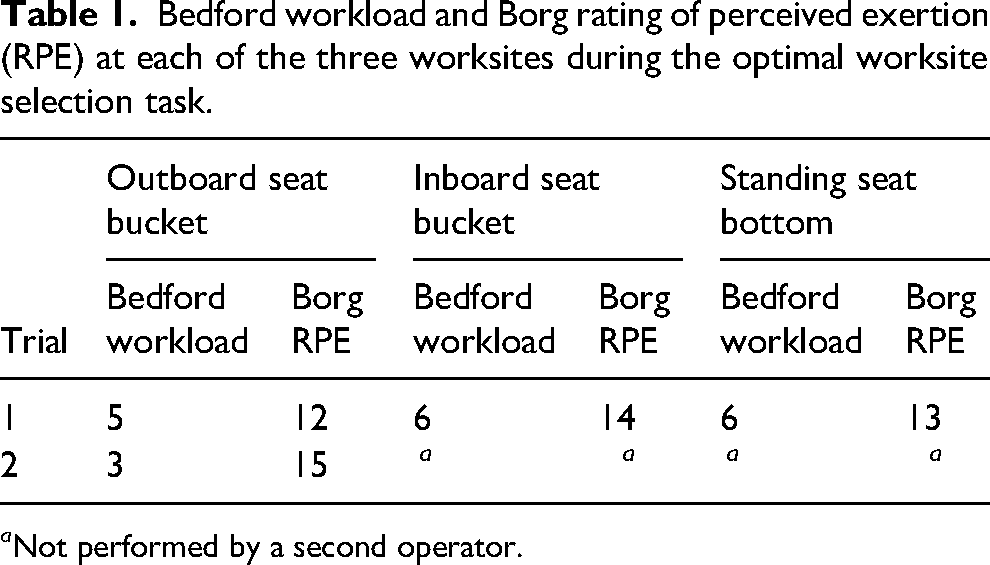
a Not performed by a second operator.
The outboard seat configuration (Figure 3) was deemed most functional for both securing a patient and obtaining leverage to perform CPR. The inboard seat location was noted to be obstructed by the displays, making it more complicated with a narrow amount of space that would be available between a patient's chest and the operator above them, limiting the ability to position the operator in an ideal compression configuration.

Outboard seat worksite and operator/patient configuration, the preferred method of cardiopulmonary resuscitation administration following evaluation of options.
Full Round of CPR at the Optimal Worksite
Each crew member then initiated 2 min of chest compressions at the preferred outboard seat location. Bedford workload and Borg RPE scores were recorded, where higher scores correspond with higher workload (Table 2, Figure 4). Three of the 4 operators rated the exertion at the very hard level (17 of 20), with the fourth operator rating it as somewhat hard (13 of 20). Two of the 4 operators rated higher workload in the little or very little spare capacity range (6 of 10 and 7 of 10, respectively), and 2 operators rated workload to have enough spare capacity for all desirable additional tasks (3 of 10). Of note, 1 of the operators who rated the exertion at the very hard level was unable to complete the full 2 min of compressions, reporting that they were unable to use their legs for force application and that the effort was highly draining on the arms. Compressions were halted after ∼45 s of the 2-min target period.
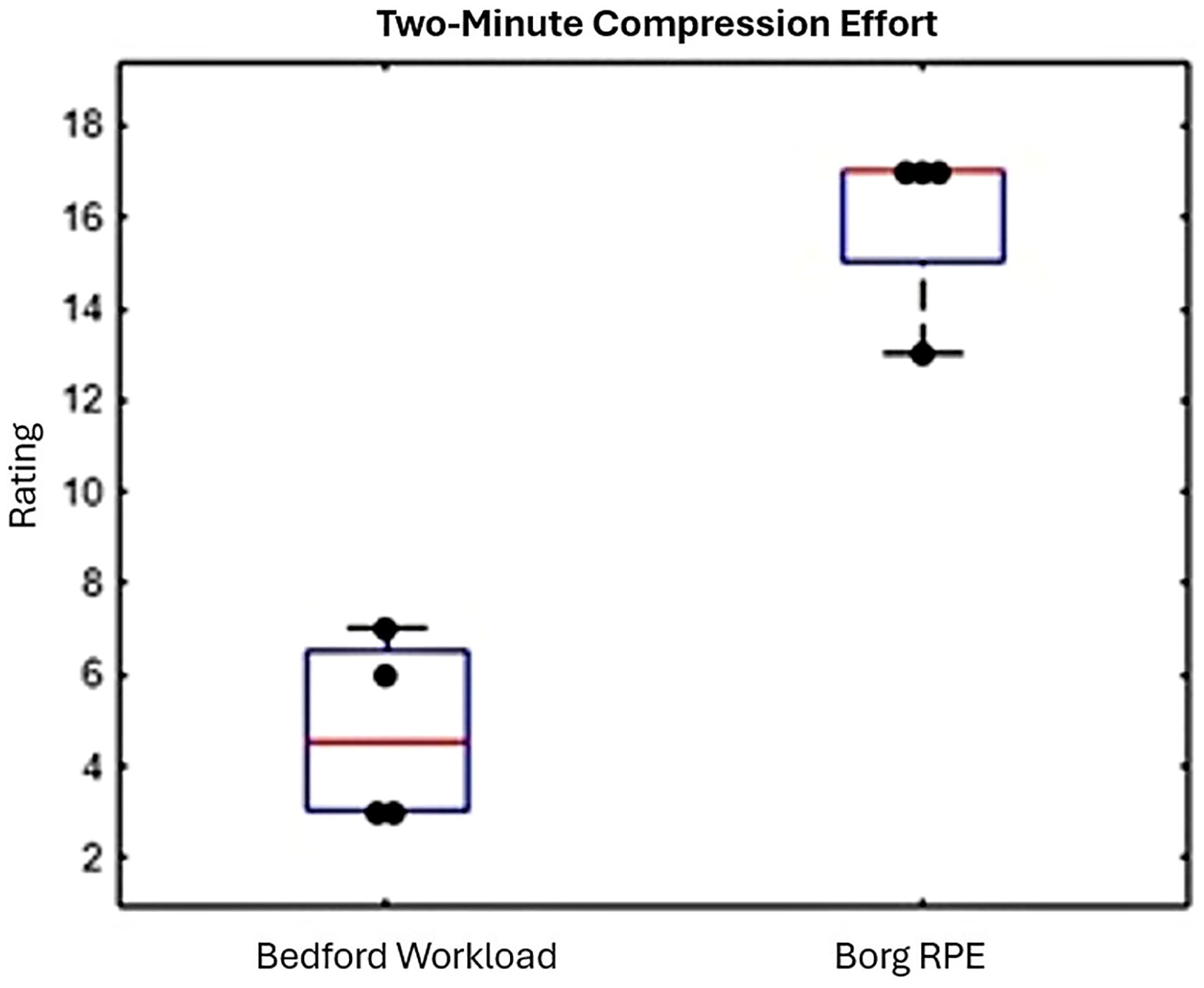
Bedford workload and Borg rating of perceived exertion during the 2-min compression test at the outboard seat worksite.
Two-minute compression effort and efficacy of the four operators.
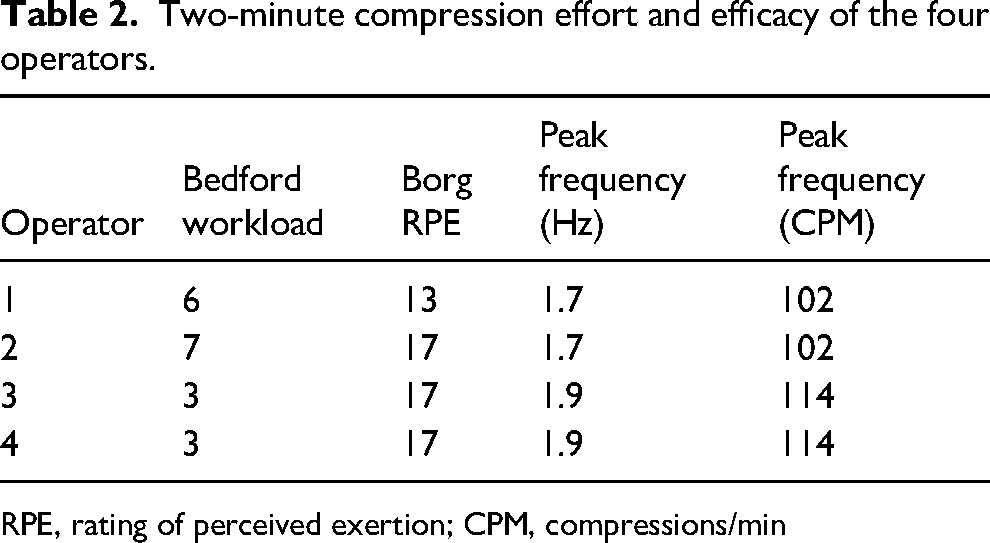
RPE, rating of perceived exertion; CPM, compressions/min
Postflight analysis of audio files to determine compression rate (Table 2, Figure 5) demonstrated that all 4 operators achieved the target frequency range, with chest compression frequencies ranging from 1.7 to 1.9 Hz (mean, 1.8 Hz). In addition to the exertion of the human operator, an impact on the Dragon spacecraft also was observed during chest compressions (Figure 6). Navigation sensors measured vehicle accelerations in all 3 axes; the z direction is displayed in Figure 6, for example. Additionally, an increase in cabin CO2 also was measured during CPR efforts. A vehicle CO2 caution limit was tripped during this study, reaching a peak level over 3.6 mm Hg.
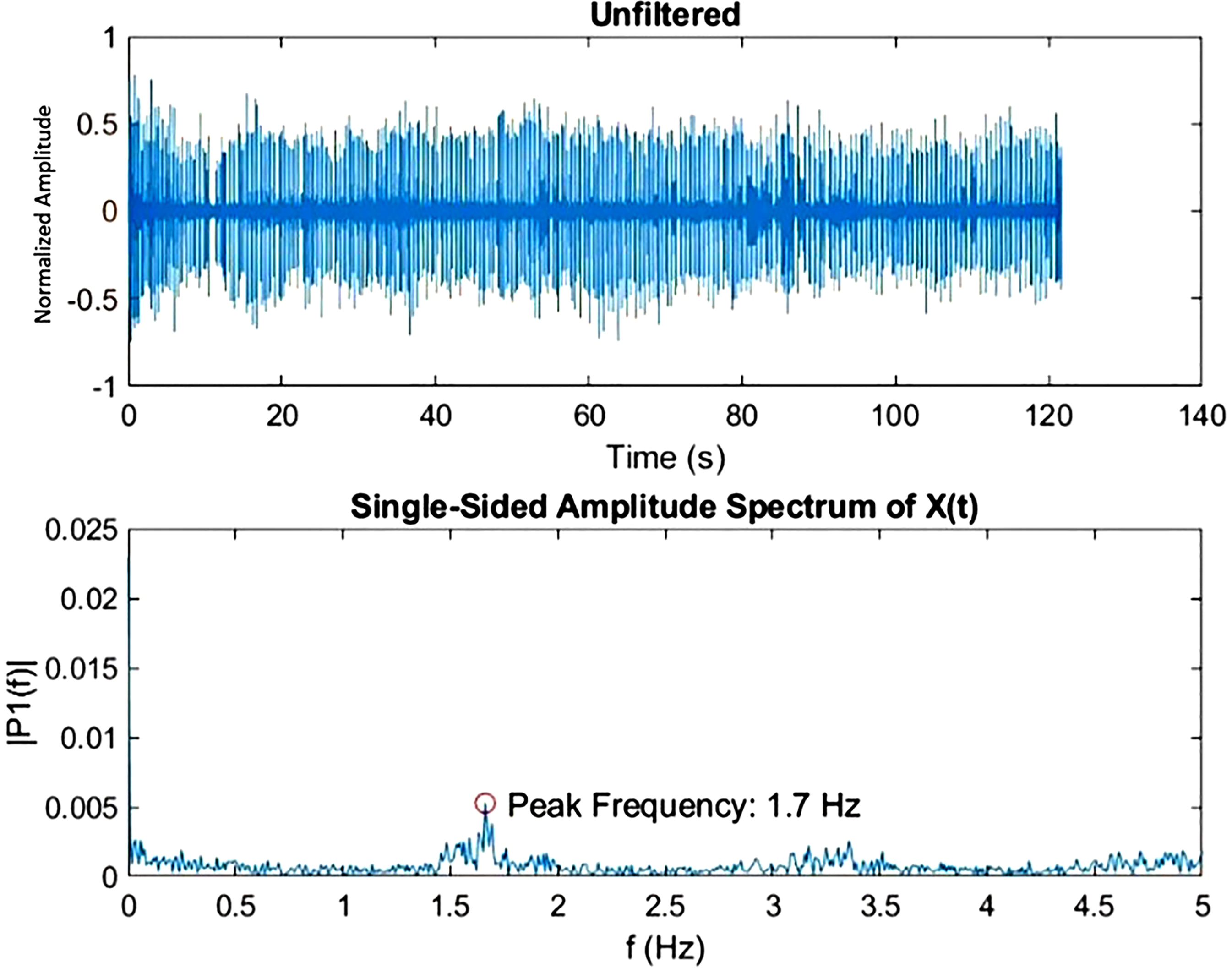
Example of peak cardiopulmonary resuscitation (CPR) frequency identified through fast Fourier transform of CPR audio/video files. The peak frequency of 1.7 Hz in this analysis corresponds with the target frequency of 1.67 to 2 Hz (100–120 compressions/min).
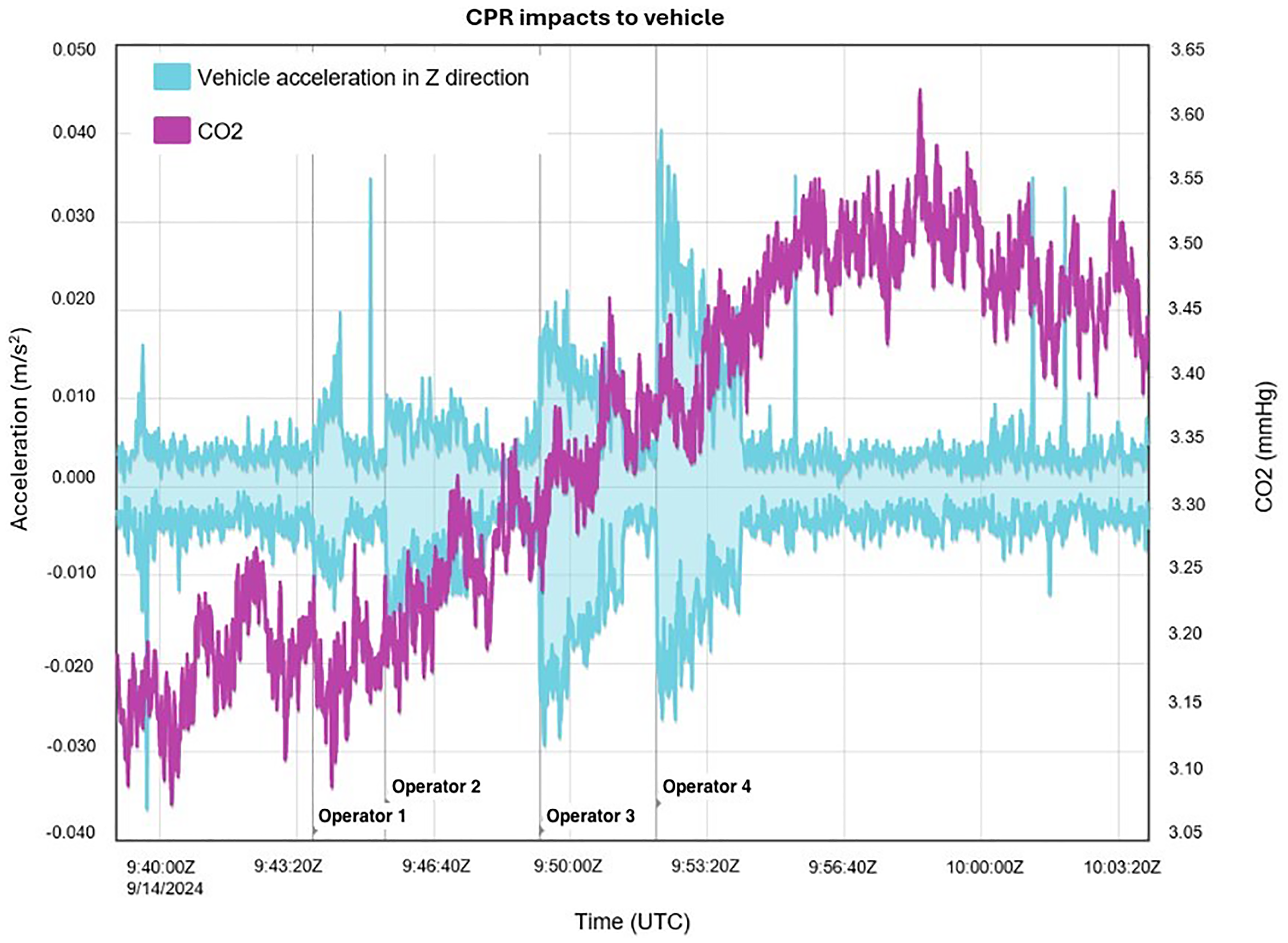
Cabin carbon dioxide and acceleration in the z direction during cardiopulmonary resuscitation at preferred outboard seat location.
Discussion
This study evaluated CPR administration during the Polaris Dawn mission to aid protocols in case of future need in Dragon missions as well as in spacecraft of similar size and shape. Although most studies of CPR in microgravity are limited to simulation studies, this is one of the few studies performed during spaceflight. We identified the optimal site of CPR to be the outboard seat position, with the patient restrained in the seat and the operator securing their posterior buttocks and feet against the ceiling. The outboard seat was evaluated first among the 3 sites and therefore not subject to learning bias through repeating the task at multiple sites. Although there are significant statistical limitations on site selection given limited trials across multiple crew members, crew members were in unanimous agreement about the decision.
In a microgravity setting, it is important to stabilize the patient to avoid reciprocal motion of the patient and operator. Our study was designed to restrain the patient to the vehicle seats, although other methods of restraint may be considered. On the ISS, stabilization is performed using the Crew Medical Restraint System. With this system, an operator could use a waist straddle, standard side straddle, or handstand technique. 10 In a prior underwater simulation, patients were stabilized on the operator's knees, and compressions were performed either with the hands (Schmitz-Hinkelbein method) or an elbow (Cologne method), where the Schmitz-Hinkelbein method showed superiority. 5 Other alternatives include having the operator encircle the patient's thorax with their legs, as is done in the Evetts-Russomano technique,3,11 locking the patient's arms under the operator's knees, 12 or tucking the operator's heels around the patient's legs. 4
Stabilization of the operator is also essential. In our study, this was done by bracing the operator's posterior buttocks and feet against the ceiling. On the ISS, this is typically done with the operator in a standing position with their feet on the ceiling, otherwise known as the handstand technique, which can be accomplished due to the larger internal volume of the station. The handstand technique has been reported previously to be the most effective method of chest compressions for microgravity,9,13–15 but such positioning is not feasible in the Dragon spacecraft with limited cabin size.
One notable finding in our study was that 1 operator was unable to complete a full 2 min of compressions due to fatigue. Specifically, they complained of significant fatigue in their arms. This is consistent with prior studies that have shown CPR delivery to be more difficult in hypogravity, reflected by an elevated heart rate and higher Borg RPE scores compared with terrestrial environments.16–19 Although terrestrial CPR depends on the weight of the operator's body over the subject, compressions in microgravity depend more on muscle contraction. 18 This usually requires flexion of the arms in microgravity to generate force, whereas terrestrial CPR may have the elbows in a locked position.4,17 Although the current American Heart Association guidelines recommend switching compressors every 2 min during terrestrial compressions, guidelines developed for microgravity may account for the enhanced fatigue and recommend a shorter interval for switching compressor roles. In addition to muscle strength, anthropometrics also could be a contributing factor to the arm fatigue observed in our study. When performing compressions, shorter astronauts had their arms more fully extended above their heads (comparable to a shoulder press), whereas taller astronauts had their arms more in front of their body (comparable to a push-up). This difference highlights how different body sizes may interact with the cabin structure and that body size may be an important factor in determining the optimal location of chest compressions. With difficult ergonomics in spaceflight, mechanical devices also may help deliver chest compressions. 10 Although mechanical compressions have been shown to deliver higher-quality compressions compared with manual compressions in parabolic flight,6,20 implementation of mechanical devices has been limited by mass and volume constraints. Some mechanical devices have been trialed previously during STS-40 space shuttle mission.19,21 Despite fatigue, all our astronauts were able to achieve the goal compression rate through their prior CPR training, although future implementation may be aided by the use of timing devices in microgravity. 22
We also analyzed impacts to the vehicle while CPR was being performed, showing elevated cabin CO2 levels. The elevated cabin CO2 could result in hypercarbia if prolonged CPR were performed, although with the short exposure in this study, no crew members complained of symptoms of hypercarbia such as headache. Importantly, CO2 levels continued to rise for several minutes after CPR was completed but soon returned to normal. These elevations were observed in the Dragon spacecraft, which has an internal volume of ∼9.3 m3 and is much smaller than other habitats such as the ISS, which has a habitable volume of ∼388 m3. Although microgravity can predispose to local elevations in CO2, larger habitats would be less likely to observe such significant elevations from this activity. The elevated metabolic rate in our study has important implications not only for performing medical procedures but also for potential exercise regimens in smaller spacecraft. Although our crew members were asymptomatic during this activity, the observed CO2 level of 3.6 mm Hg has the potential to cause symptoms with prolonged exposure. For example, the ISS previously had a CO2 limit of 5.3 mm Hg, which has been reduced over time due to findings of fatigue and full-headedness from 2.3 to 2.7 mm Hg, cognitive impact from 2.7 to 3.0 mm Hg, and headaches from 3.0 to 3.4 mm Hg.23,24 Investigators have found that the risk of headache doubles for every 1 mm Hg increase in CO2. 25
We also observed vehicle accelerations in all axes that were associated with CPR. These accelerations appeared most profound with the initiation of CPR and diminished over time. Importantly, this activity was of low magnitude and would not be expected to cause the vehicle to lose attitude control. Vibration from crew tasks has the potential to cause structural stress on the vehicle, which is one of the motives for a vibration-isolation system on the ISS exercise equipment. However, the accelerations observed during CPR tasks were of low magnitude and short duration such that a dedicated vibration-isolation system for CPR likely would not be required.
Limitations and Future Directions
This study has several strengths, being the first of its kind in the Dragon spacecraft and the first study to show the impact of CPR on a spacecraft vehicle and providing recommendations for updated microgravity CPR guidelines to account for enhanced fatigue. However, several limitations also should be acknowledged. Results are specific to the Dragon spacecraft and short-duration flight and may have limited generalization to other vehicle configurations. Additionally, musculoskeletal changes over long-duration flight may have implications for CPR administration not appreciated in this study of short-duration spaceflight. Several alternative patient/operator CPR configurations have been described previously and were not trialed in this study but may be areas of further investigation. Although crew members were in unanimous agreement about site selection of the outboard seat location, there are significant statistical limitations of the site selection given limited trials across multiple crew members in our small sample size. Although we tested the ideal positioning for delivering chest compressions, we did not evaluate the positioning of a second crew member near the airway while compressions were being performed or the ability of crew members to quickly alternate positions to switch compressor roles. Additionally, different body sizes were not incorporated into site selection. We had a range of operator body sizes in this study, but a broader range may be eligible for spaceflight. As such, our findings may have limited external validity as applies to future crews with anthropometric differences that may impact the optimal worksite, workload, and impacts to the vehicle. The time it takes to secure a patient into the outboard seat in an emergency situation also was not evaluated. Because rapid initiation of chest compressions is the most effective treatment for cardiac arrest, alternative methods, such as the Evetts-Russomano method (where the operator secures themselves to the patient by wrapping their legs around the patient's torso), may be considered to prevent delay in chest compressions. Alternatively, 2 different phases and methods of compressions may be employed, for example, starting with Evetts-Russomano compressions at the location of arrest until the patient can be transferred to the preferred location for compressions. 2 Given the significant fatigue observed in 1 crew member, it is unknown how long our preferred method of outboard seat CPR could be maintained and whether other alternative techniques may be better suited for their sustained efficacy over time. Also, because the bellows is an internal component of a larger manikin system, it clicks at a depth of 3 cm with a maximum compressible depth of about 5 cm. This is less than the recommended compression depth of 5 to 6 cm, but the bellows was advantageous for this study due to its low mass/volume and audible clicks. Finally, we did not perform a comparison of CO2 levels or vehicle accelerations at the other worksites trialed in this study to determine the differential vehicle impacts of the different locations.
Conclusions
Outboard seat location provided the best ergonomics for administration of CPR on the Dragon spacecraft in spaceflight. Although an optimal location of CPR was identified within the vehicle, the task had high difficulty ratings, as measured by the Bedford workload scale and Borg RPE. CPR also was associated with elevated cabin CO2 levels and vehicle accelerations, as measured by the navigation system.
Footnotes
Author Contribution(s)
Funding/Material Support
This work was supported by the Translational Research Institute for Space Health through NASA Cooperative Agreement NNX16AO69A.