
Abstract
Airway devices may be scarce in limited resource situations, such as prehospital settings or austere environments. Tube tip in pharynx (TTIP) ventilation is a simple, one-handed technique that may prove valuable for ensuring airway control in a life-threatening situation. The technique only requires a standard cuffed endotracheal tube and a self-inflating bag. This case report illustrates a scenario where both bag-valve-mask (BVM) ventilation and intubation failed, and the TTIP technique was utilized successfully several times during the case management. This case report illustrates that TTIP may be a useful technique, especially in limited resource settings. It is easy to learn, takes seconds to perform, and has minimal equipment requirements. The case report is reported according to the CARE guidelines. Informed consent from the patient is obtained.
Introduction
Airway access is imperative; however, airway management equipment may be scarce in limited resource situations, such as the prehospital setting or austere environments. This case report illustrates that the tube tip in pharynx (TTIP) technique may contribute to resolving a life-threatening situation with the use of readily available equipment. It is a simple, single-handed technique1,2 intended to obtain airway patency if bag-valve-mask (BVM) ventilation, supraglottic airway device ventilation, or endotracheal intubation fails.
The technique requires only a standard cuffed endotracheal tube and a self-inflating bag. The tube is inserted through the mouth or nose, without the use of a laryngoscope, with the tip in the pharynx. The cuff is then inflated to push the base of the tongue away from the surrounding tissue (Figure 1). One hand is used to enclose the patient's mouth and nose to create a tight seal (Figure 2), which is crucial to prevent air leakage. Additionally, the grip includes a chin lift, performed with the same operating hand, which contributes to an open airway.
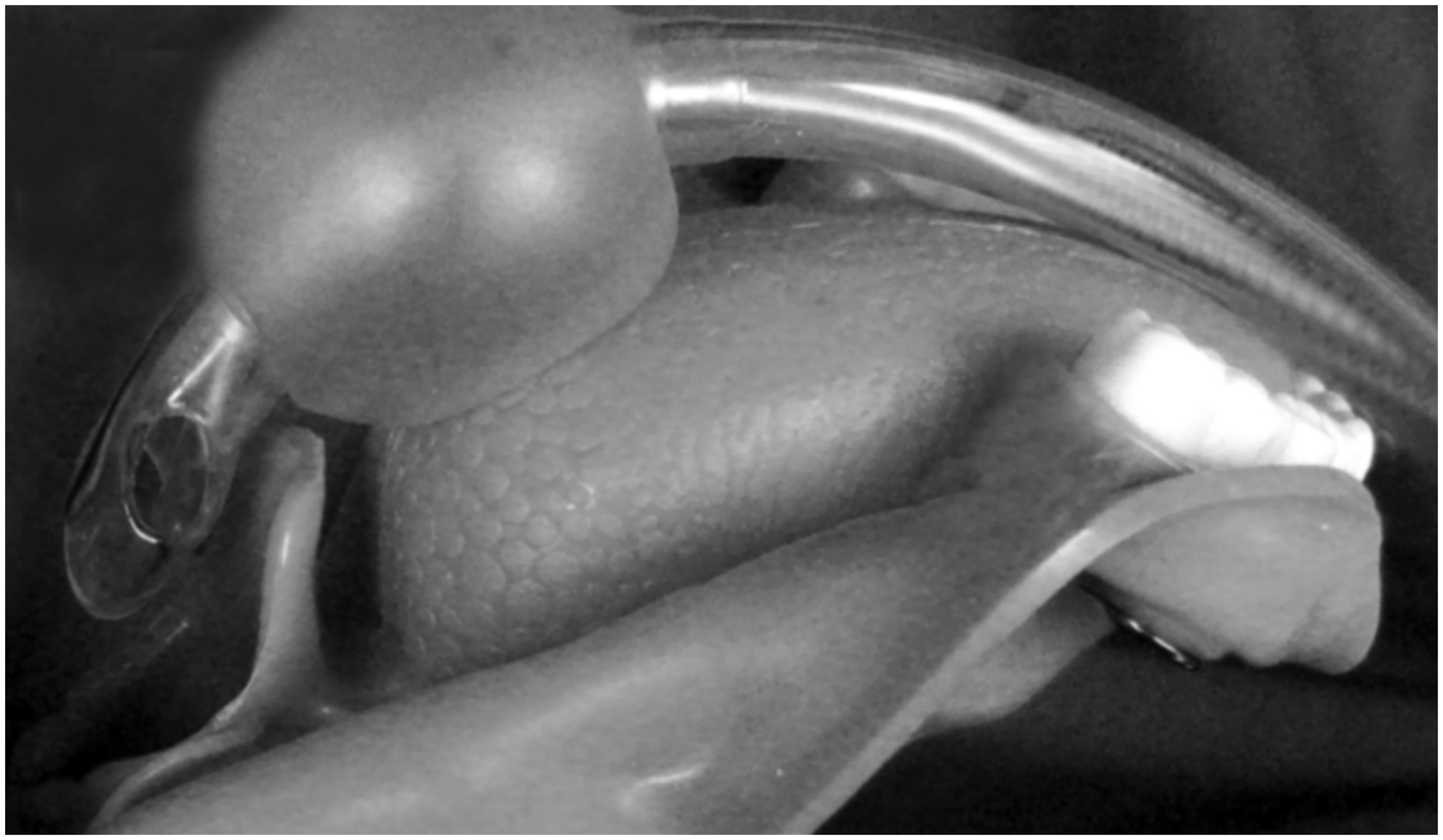
Relation of the tube tip, cuff, epiglottis, and the base of the tongue in tube tip in pharynx ventilation. 1 (With permission from Acta Anaesthesiologica Scandinavica and John Wiley and Sons).

An illustration of how the tube tip in pharynx technique is performed, with one hand enclosing the patient's mouth and nose to create a seal. 1 (With permission from Acta Anaesthesiologica Scandinavica and John Wiley and Sons).
The case report is produced according to the CARE guidelines, 3 and informed written consent from the patient was obtained for publication.
Case Report
The case was experienced by a Danish nurse anesthetist (author ABS). At the time, she had 4 years of experience as a nurse anesthetist and worked for a humanitarian organization at a 70-bed trauma hospital in Nigeria, which received approximately 30 patients per day. The patient was a Nigerian male in his mid-forties with an estimated body mass index (BMI) of 40 and an unknown medical history. He had suffered a gunshot wound to the abdomen and needed an urgent laparotomy. The patient was hemodynamically stable at hospital admission. Both computer tomography (CT) scan and ultrasound were unavailable, and an exploratory laparotomy was necessary to remove the bullet.
Airway access was regarded as potentially difficult due to high BMI, large abdomen, and a short neck. However, commonly accessible or advanced airway access equipment such as “rapid airway management position” pillows, 4 supraglottic airway devices, video laryngoscope, or equipment for awake intubation was not available. Available airway equipment included oropharyngeal airways, Macintosh blades sizes 3 and 4, a rigid stylet, and endotracheal tubes ranging in size from 6.0 mm to 8.0 mm. Additionally, a basic fingertip pulse oximeter was available, but there was no capnometer for monitoring end-tidal CO2. Even basic equipment, such as pillows, was scarce in this situation. The team had only one small pillow, which was used to tilt the patient's head slightly backward. No additional equipment to improve positioning was available. Oxygen supply was provided via an oxygen concentrator, with a maximum output of 5 L/min with 100% oxygen. Preoxygenation prior to the induction of anesthesia was conducted with a self-inflating resuscitation bag placed over the patient's mouth and nose without squeezing the bag.
General anesthesia was induced with thiopental at a dosage of approximately 5–7 mg/kg and succinylcholine at a dosage of approximately 1–1.2 mg/kg. The first intubation attempt was performed approximately 1 minute after administration of succinylcholine, after observing apnea and muscular twitching. With direct laryngoscopy, the epiglottis was seen, but it was not possible to visualize the vocal cords (Cormack-Lehane grade 3), and the first intubation attempt was aborted. BVM ventilation was tried but failed, despite efforts to reposition the patient's head and the use of an oropharyngeal airway size 4 (10 cm). This resulted in oxygen desaturation. When the induction agents wore off, the patient began to cough but remained unable to cooperate or maintain an open airway, with further desaturation. The lowest saturation level is not registered. With four years of experience, the nurse anesthetist (ABS) was not accustomed to managing difficult airway situations, did not have experience with emergent cricothyrotomy, and had limited resources available and therefore decided to try the TTIP technique. Ventilation and oxygenation improved, and the patient calmed down and cooperated as he became semi-awake. When the TTIP was removed, the patient desaturated again and the tube was reinserted in the pharynx. Oxygen saturation was restored to normal levels. To sedate the patient prior to intubation, halothane was administered via BVM ventilation using the self-inflating bag while the patient was spontaneously breathing. However, as the patient became sedated, desaturation recurred. The TTIP technique was used for the third time, again restoring oxygen saturation. Two additional attempts to intubate without additional muscle relaxant failed. Between the attempts, the TTIP technique was used to restore normal oxygenation.
Ultimately, airway management was resolved by a surgical tracheostomy performed by the surgeon while the patient was ventilated with the TTIP technique. Figure 3 describes the line of events in airway management.
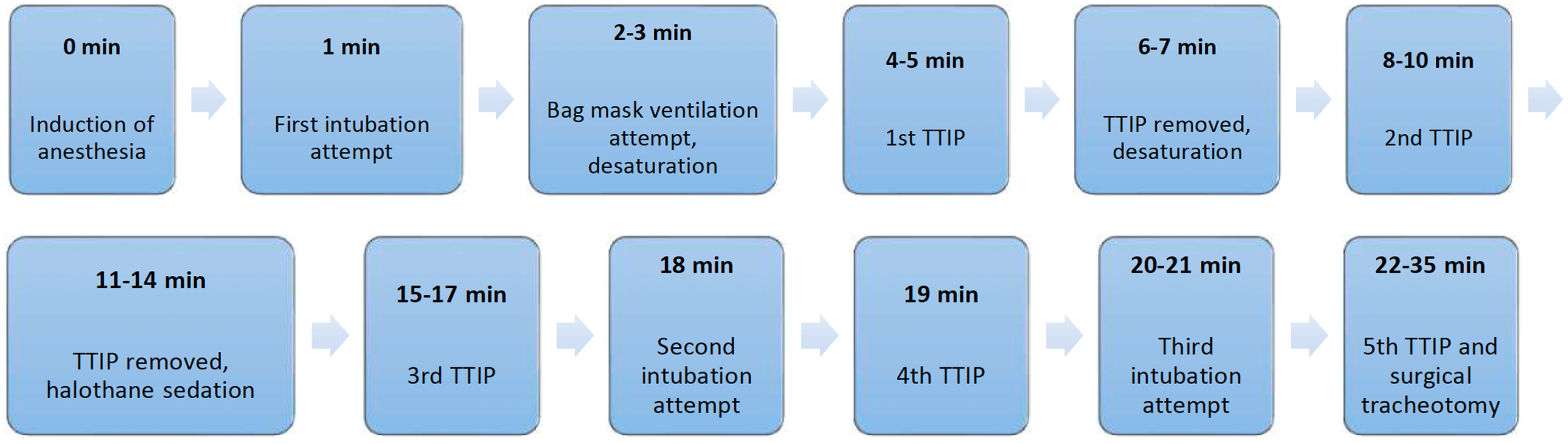
A timeline describing the line of events in airway management. TTIP, tube tip in pharynx.
An explorative laparotomy was performed, where a perforated colon was discovered and repaired. The patient recovered without sequelae.
Discussion
Guidelines for managing difficult airways are established,5,6 and the use of a cuffed endotracheal tube in the pharynx for ventilation1,6,7 and to aid intubation8,9 is previously described. It has also been shown to be effective in obese patients 1 and as a conduit for fiberoptic intubation. 2 Despite its efficacy, the technique is not widely reported or taught in anesthesiology, emergency medicine, or prehospital care. This case report demonstrates the successful application of TTIP ventilation in clinical practice, highlighting its potential usefulness in low-resource settings due to the requirement of only a standard endotracheal tube and a self-inflating bag. Consequently, we believe the TTIP technique could be taught as a rescue option in airway management, especially for healthcare providers working in prehospital or low-resource settings.
This case report has limitations. Firstly, the depth of anesthesia could have influenced the ease of BVM ventilation. Despite reports that all medications were given in recommended doses, it is difficult to guarantee that an adequate depth of anesthesia was achieved. However, problems due to inadequate depth of anesthesia may have been mitigated by the administration of the rapid-acting neuromuscular-blocking medication succinylcholine. In this case, ventilation conditions did not improve. Secondly, alternative readjustment measures between the intubation attempts could have been tried. However, this was not feasible due to the lack of available resources, even including basic items like pillows. Finally, this is a case report, managed by a nurse anesthetist with limited clinical experience and may not be transferrable to other specialties or clinical settings.
The TTIP technique carries potential complications, including barotrauma or gastric insufflation leading to subsequent aspiration. 10 However, these risks are inherent to most positive-pressure ventilation techniques and can be mitigated by exercising cautious ventilation. While trauma to surrounding tissue might potentially occur when the cuff is inflated in the pharynx, we posit that cuff inflation is less likely to cause mucosal trauma compared to multiple intubation attempts. Furthermore, there is a lack of scientific literature that addresses the optimal depth of tube insertion in the pharynx or the appropriate cuff volume. Based on our experience, a practical approach is to insert the tube to a depth corresponding to the distance from the patient's mouth to the angle of the mandible and to inflate the cuff with approximately 20 milliliters of air. However, this specific approach has not been scientifically validated and requires further investigation.
In conclusion, the TTIP technique is a simple, one-handed approach that can contribute to the management of difficult airway situations. It is easy to learn, takes seconds to perform, and requires only readily available equipment. Therefore, it may be a useful skill in both pre- and in-hospital settings and especially in low-resource and austere environments. Consequently, we advocate for the inclusion of the TTIP technique as a valuable addition to airway management.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.