
Abstract
Introduction
Rural emergency prehospital care in British Columbia is conducted primarily by the British Columbia Ambulance Services or ground search and rescue volunteers. Since 2014, the volunteer Air Rescue One (AR1) program has provided helicopter emergency winch rescue services to rural British Columbia. The aim of this research was to describe the activity of the AR1 program and to make recommendations to improve future operations.
Methods
Data were collected retrospectively from September 2014 to May 2021, and parameters of emergency callout statistics from the organization's standard operating guidelines, rescue reports, and interviews were summarized and reviewed.
Results
Of 152 missions within the study period, 105 were medically related rescues involving trauma or cardiac events. Snowmobiling, mountain biking, and hiking were the most common activities requiring rescue. The 38 medical callouts that were not completed by AR1 were reviewed for contributing factors. Response time varied due to the vast service area, but median time from request to takeoff was 55 min (interquartile range 47–69 min), and median on-scene time was 21 min (interquartile range 11–33 min).
Conclusions
AR1 provides advanced medical care into British Columbia's remote and difficult-to-access areas, minimizing delays in treatment and risk to patients and responders. Callout procedures should be streamlined enabling efficient AR1 activation. Collection of medical and flight information should be improved with standardized documentation, aiding in internal education and future research into the program's impact on emergency prehospital care. Future directions for improvement of care include the possibility of introducing portable ultrasound technology.
Introduction
Access to medical services in rural British Columbia (BC), Canada, has been a growing point of discussion in recent years. BC has a population of >5.3 million and is a popular travel destination, in large part due to its varied geography and outdoor recreation, attracting millions of tourists annually. With a land area of 944,735 km2, BC is home to world-famous ski resorts, mountain ranges, parks, lakes, and rivers. Popular activities include snow and water sports, hiking, and hunting. Of BC's residents, 14% are considered rural (population <1000), and another 12% live in small population centers (population 1000–1029,999) with sparse access to medical and paramedical services, including emergency medical response. 1
The BC Ambulance Service (BCAS) is tasked with providing emergency prehospital treatment and transportation to the public. However, rural responses are often limited by factors including long transport distances, adverse weather conditions, and unstaffed ambulance stations, leading to extended response times to emergency calls. Further, rural rescue services often have additional challenges accessing patients due to their location in complex or technical terrain. This gap in service availability is currently filled by search and rescue (SAR) volunteers who are dispatched to a scene by a requesting agency (ie, ambulance, police, fire) through the Emergency Coordination Centre under the jurisdiction of Emergency Management British Columbia. 2 BC's 78 SAR groups and their >3400 professional volunteers respond to >1900 annual incidents involving >2100 lost or injured persons. 3 Between 2014 and 2016, the Vernon Search and Rescue (VSAR) group, located in BC's Okanagan Valley, initiated a successful 2-y pilot project to explore the feasibility of operating a winch-equipped Bell 412 EP helicopter staffed by paramedic and physician volunteers to perform advanced rescues. 4 VSAR's Heli Winch team, formally called the Air Rescue One (AR1) program, was the first Class D volunteer SAR helicopter winch rescue program in Canada and was dispatched to >160 emergency calls between 2014 and 2022.
AR1 serves a significant land area covering dozens of rural and small population centers. Based out of the Central Okanagan Valley, AR1's 720-km operating range extends north toward Blue River, south to the US-Canada border, east to the BC-Alberta border, and west to Manning Park in the Cascade Mountains. The volunteer rescue team consists of primary care paramedics, advanced care paramedics, and physicians.
AR1 is equipped with advanced life support equipment and operates according to the scope of the advanced care paramedic on staff. Capabilities include rigid immobilization, traction splinting, sedation, intubation, pain management, needle decompression, intravenous and intraosseous access, rewarming, and advanced cardiac life support. Available advanced equipment includes the Lifepak 15 for monitoring, defibrillation and cardioversion, a video laryngoscope, and the LUCAS II automatic chest compression device. 4 The Bell 412 EP helicopter is a strategic choice, permitting greater hover capabilities on 1 engine and the capability to transport patients directly to H1 helipads at larger medical centers such as at Kelowna General Hospital, Penticton Regional Hospital, and Royal Inland Hospital in Kamloops.
Winch rescue is extremely flexible, especially when used in coordination with ground SAR assets, resulting in significantly reduced time taken to transport patients to definitive care. An air response also reduces risks that would otherwise be faced by ground SAR teams accessing dangerous terrain in potentially harsh environments. The AR1 medical team provides advanced-level medical care in addition to technical skills such as avalanche forecasting, rope and pick-off rescues, and swift-water rescues. All crew members are trained and certified in a roster of technical skills including ground SAR, swift-water rescue, avalanche rescue, rope rescue, emergency medical response, and helicopter winch rescue and emergency operations. AR1 crew members hold additional technical training in avalanche operations, advanced swift-water rescues, pediatric advanced life support, and advanced cardiac life support, and crew members include primary care paramedics, advanced care paramedics, rope rescue team leaders, and emergency physicians with experience in wilderness medicine. This unique competency in technical, medical, and austere training exceeds that of other resources in BC. The level of training and winch capabilities allow AR1 to perform rescues from complex and difficult-to-access terrain, stabilize and treat patients, and directly transport them to definitive care. AR1 will often overfly smaller clinics and hospitals and land directly at tertiary care centers (unstable patients) or adjacent airports (stable patients), decreasing the need for ground transfers after air rescue. While the typical difficult-to-access medical rescues take place in the remote and rural backcountry, AR1 is also dispatched to the urban environment in conditions where a winch extrication and transfer to ambulance or hospital helipad would be more efficient, quicker, and safer for the patient and responders than traditional Emergency Medical Services response. Some specific criteria that define the preferable dispatch of AR1 over other conventionally deployed resources include an imminent threat to the lives of the patient(s), patient has entered swift water, weather conditions likely to cause hypothermia, patient in potential avalanche terrain, SAR volunteers with advanced medical training being requested, request by BCAS or police to perform medical rescue, patients’ medical condition and/or situation requires expedient extraction, terrain or environmental hazards risky to responders, and ground transport time likely to cause a negative outcome for the patient and/or rescuers.
The aim of this study was to describe the helicopter rescue activity of a volunteer air rescue program in BC, to make recommendations to improve operations in the future, and to present a potential model for other locations where such a volunteer service could fill critical gaps in prehospital emergency response.
Methods
This study was approved by the Air Rescue One Heli Winch and Vernon Search and Rescue Society boards. A retrospective review of all AR1 missions between September 28, 2014, and May 16, 2021, was performed by reviewing data including date, location, and call type as well as by reviewing the standard operating procedures of the program. All data reviewed were anonymized, without access to patient identifiers, and therefore were exempt from institutional review board approval under National Institutes of Health Category 4. Due to the absence of affiliation with a Canadian institution or federal research funding, the Canadian Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2) institutional review requirements did not apply. Statistical analyses were carried out by categorizing tasks based on call type, showing the distribution of tasks for medical rescue, nonmedical rescue, search, recovery, flood, avalanche, or other need. The tasks identified as medical calls were further grouped to identify common medical injuries, such as general and multitrauma, cardiac, other, or unknown. Types of activity leading to injuries necessitating an AR1 rescue also were tabulated. The cumulative medical responses by month were reviewed and graphed, showing the number of callouts completed and not completed by AR1. Factors that led to a task not being completed by AR1 also were reviewed and graphed. Finally, response times were calculated by reviewing a subset of 17 medical rescue calls between November 8, 2014, and September 26, 2016, for which specific flight duration data were available, showing the mean, median, and interquartile range (IQR, min) of time to AR1 activation, AR1 request to take off, arrival to patient contact, and patient contact to patient and crew loaded. 5 AR1 capabilities, strengths and limitations, and future recommendations were highlighted based on this information.
Results
A retrospective review of 152 AR1 missions between September 28, 2014, and May 16, 2021, shows that 69% of calls (n=105) were medically related rescues, 13% (n=20) were nonmedical rescues, and 12% (n=18) were strictly searches for missing individuals (Figure 1).
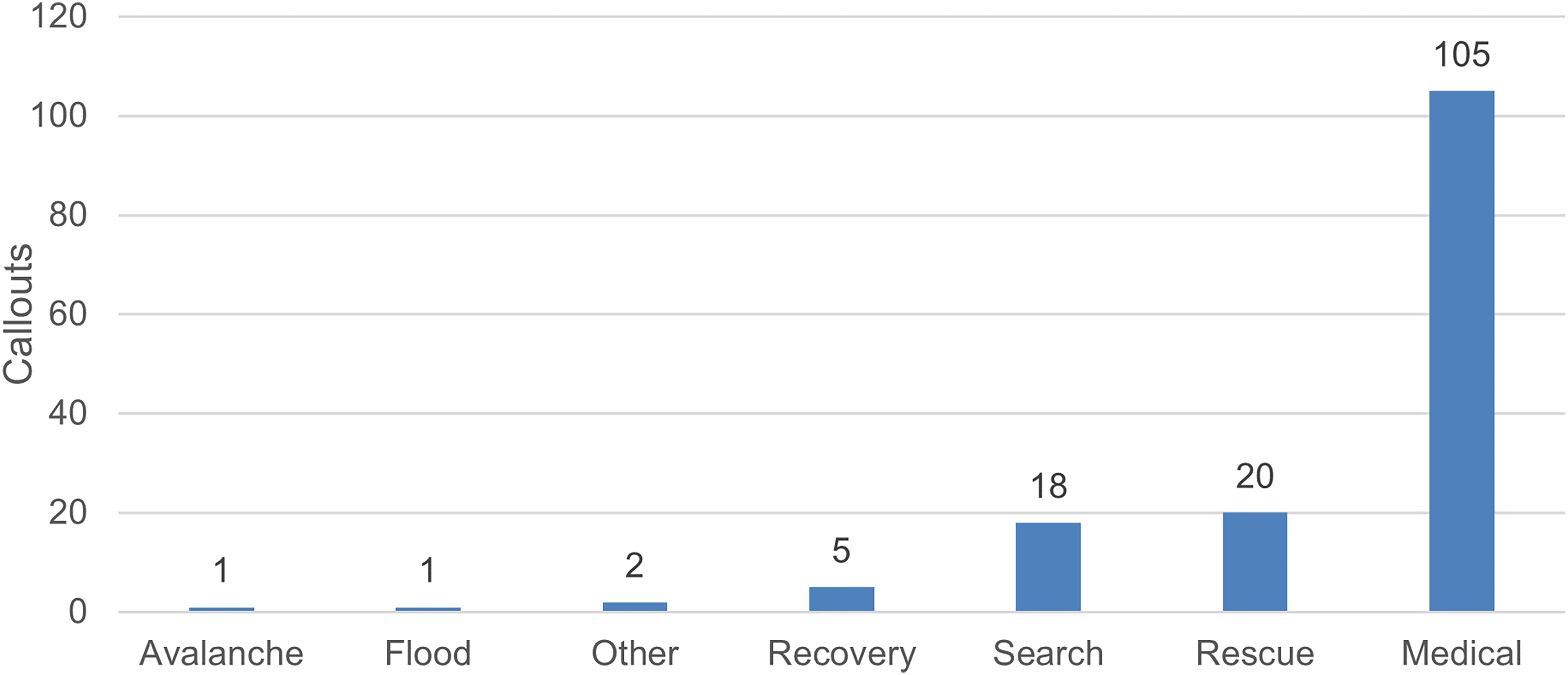
Total calls for which AR1 was requested, by type, between September 28, 2014, and May 16, 2021.
Medical rescue calls varied widely but generally can be grouped into the following subcategories (Figure 2):
Trauma (59%): Calls categorized as trauma included patients who experienced falls with resulting head, spinal cord, or limb injuries or were involved in a vehicular accident (eg, ATV rollover, snowmobile collision) and experienced polytrauma. Some illustrative examples include a hunter with a hip dislocation, a skier with a pelvic fracture, and a snowmobiler with a fractured femur. Cardiac (8%): Cardiac calls included cardiac arrests, myocardial infarctions, and patients with chest pain. Other (8%): Other medical calls included patients requiring medical attention due to heat exhaustion, sudden loss of consciousness, diabetic emergencies, seizures, syncope, shortness of breath, and anaphylactic reactions. Unknown (26%): The remainder of cases encompass calls where the type of injury or medical emergency was unknown. This is primarily due to noncontact with the patient by the AR1 crew either because the rescue was performed by a different responding agency (eg, GSAR) or the patient managed self-extrication.
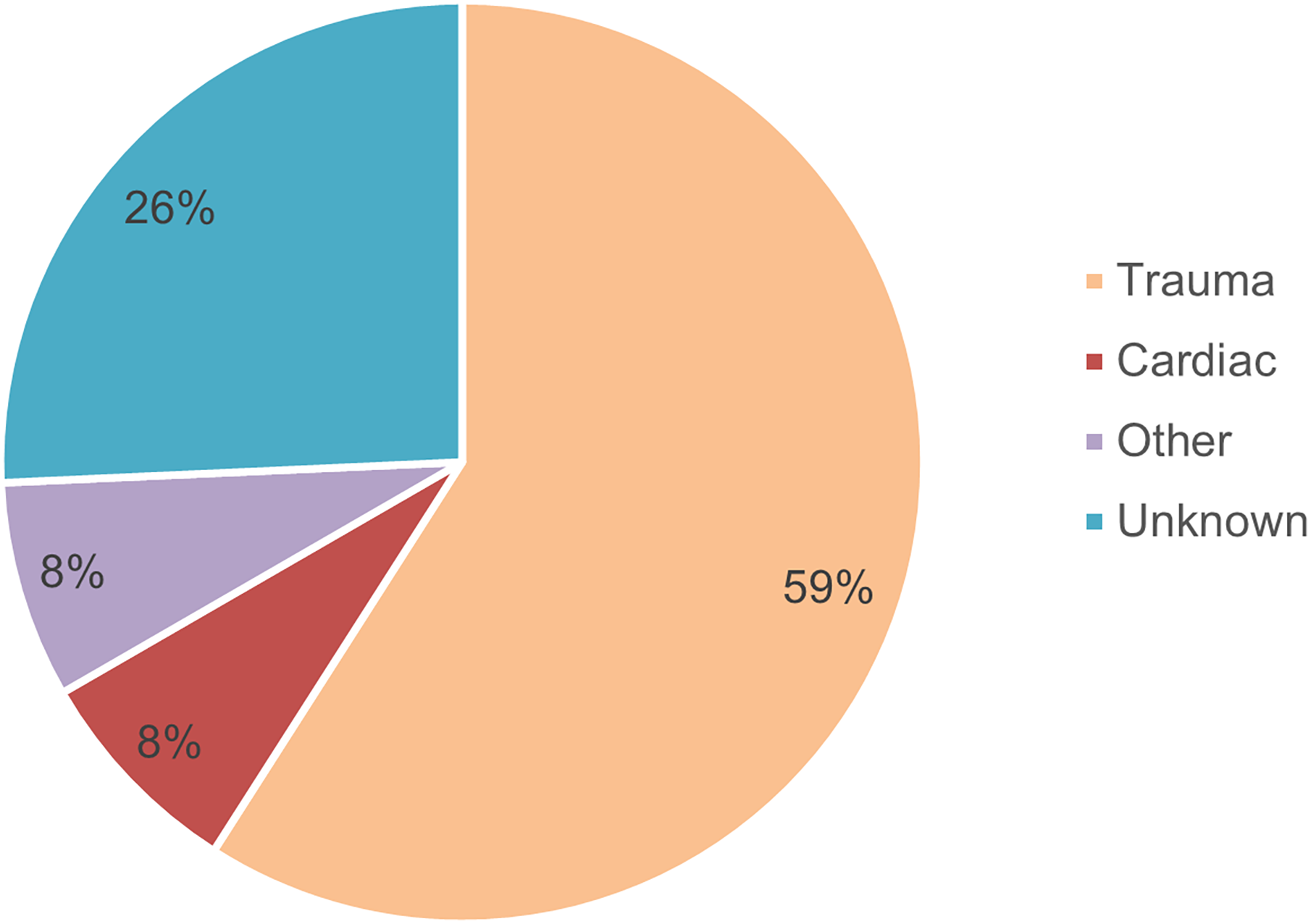
Medical calls by type of event.
Hikers, climbers, and mountain and dirt bikers comprised the most frequent patients during warmer seasons, whereas snowmobilers were the most common during winter months. Other activities included individuals in medical distress due to boating or equestrian accidents, avalanches, or other reasons not specified (Figure 3).
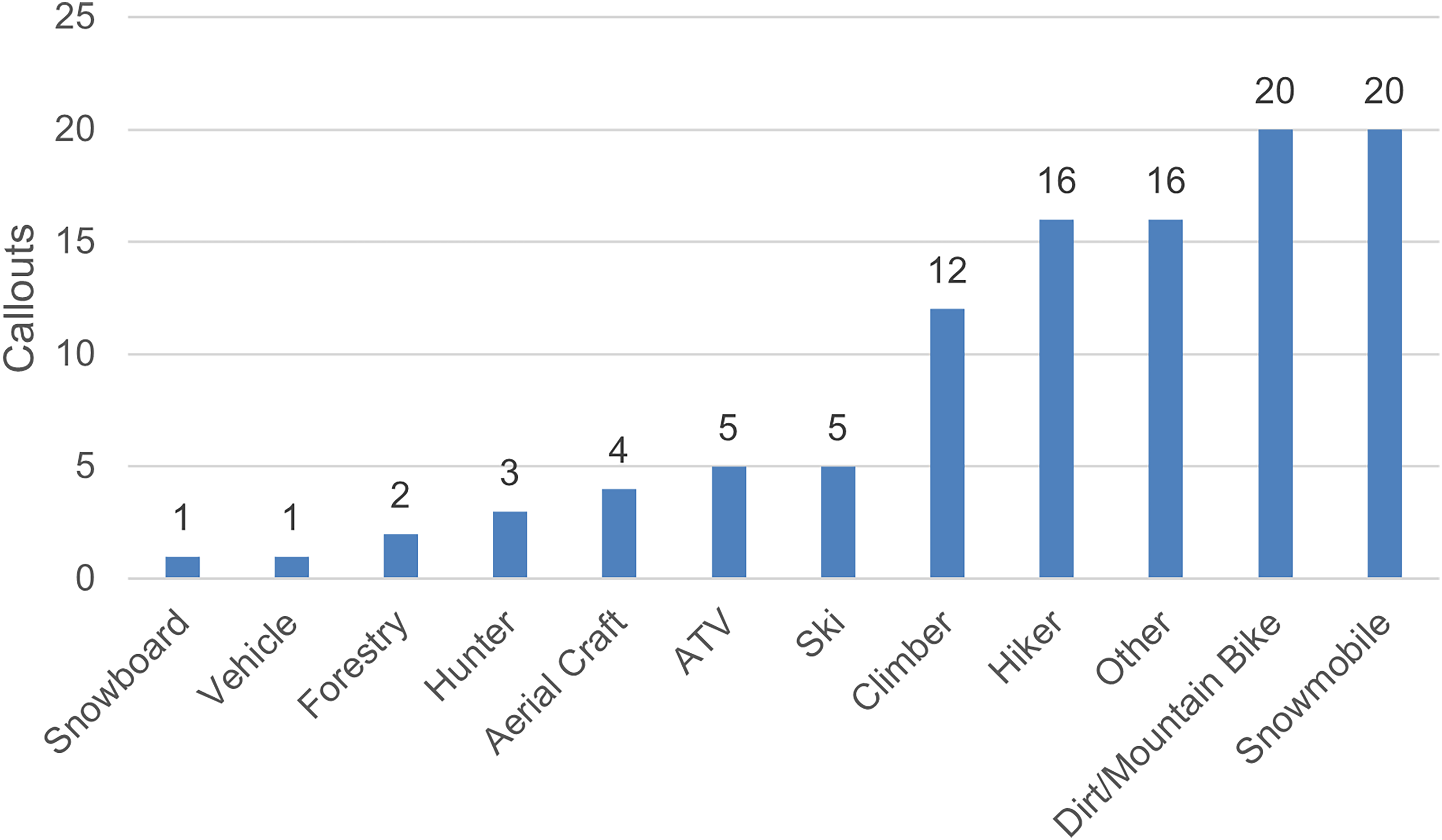
Mechanism of injury for medical rescues.
A review of the cumulative medical responses by month is provided in Figure 4, taking into account callouts with and without a response by AR1. Thirty-eight of 105 medical callouts were not completed by AR1, with contributing factors shown in Figure 5. While AR1 responds to medical rescues year round, the busiest seasons are winter and summer. The highest number of noncompleted callouts were during the winter and early spring seasons.
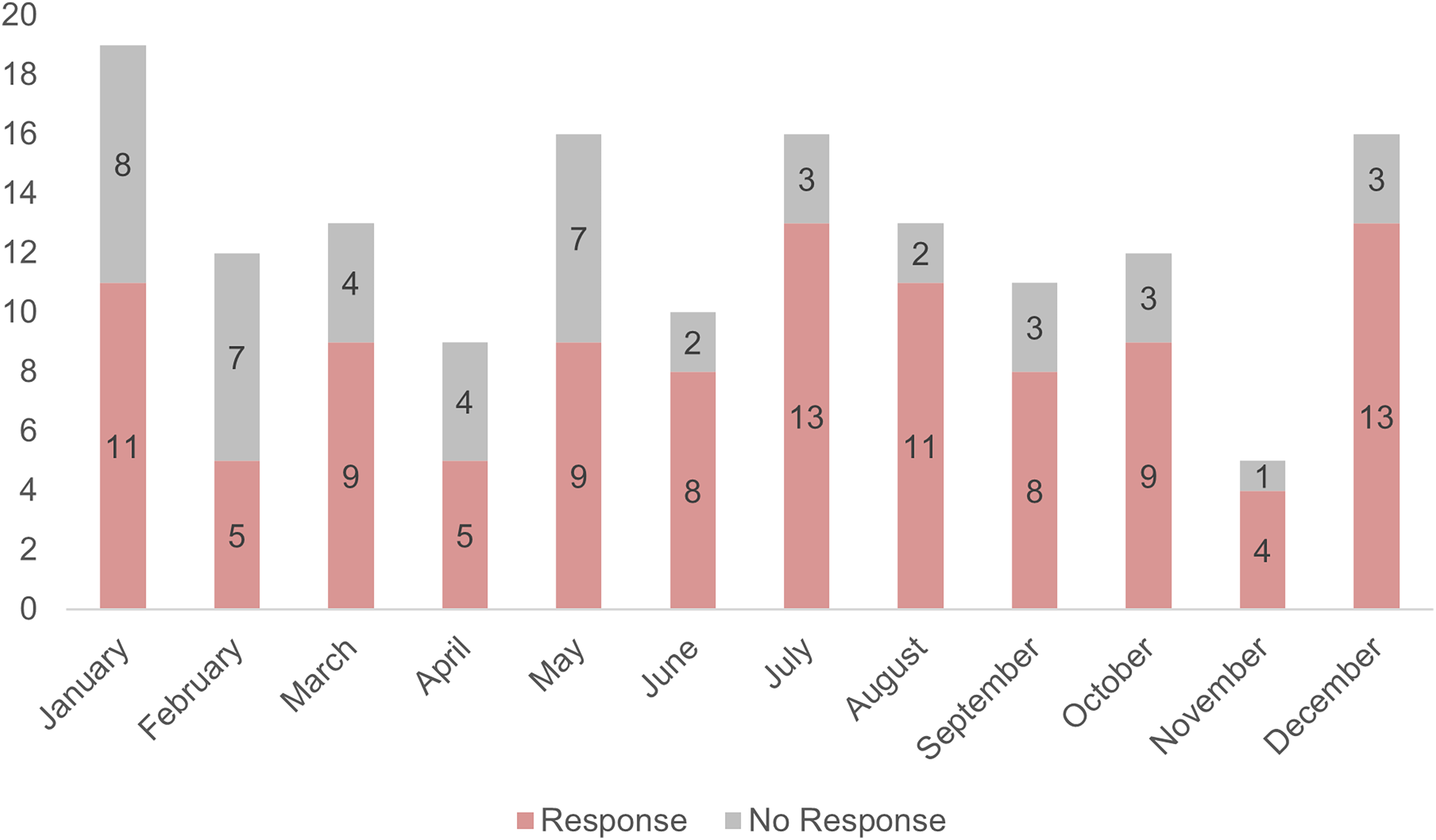
Cumulative AR1 medical calls by month showing number of calls completed and not completed.
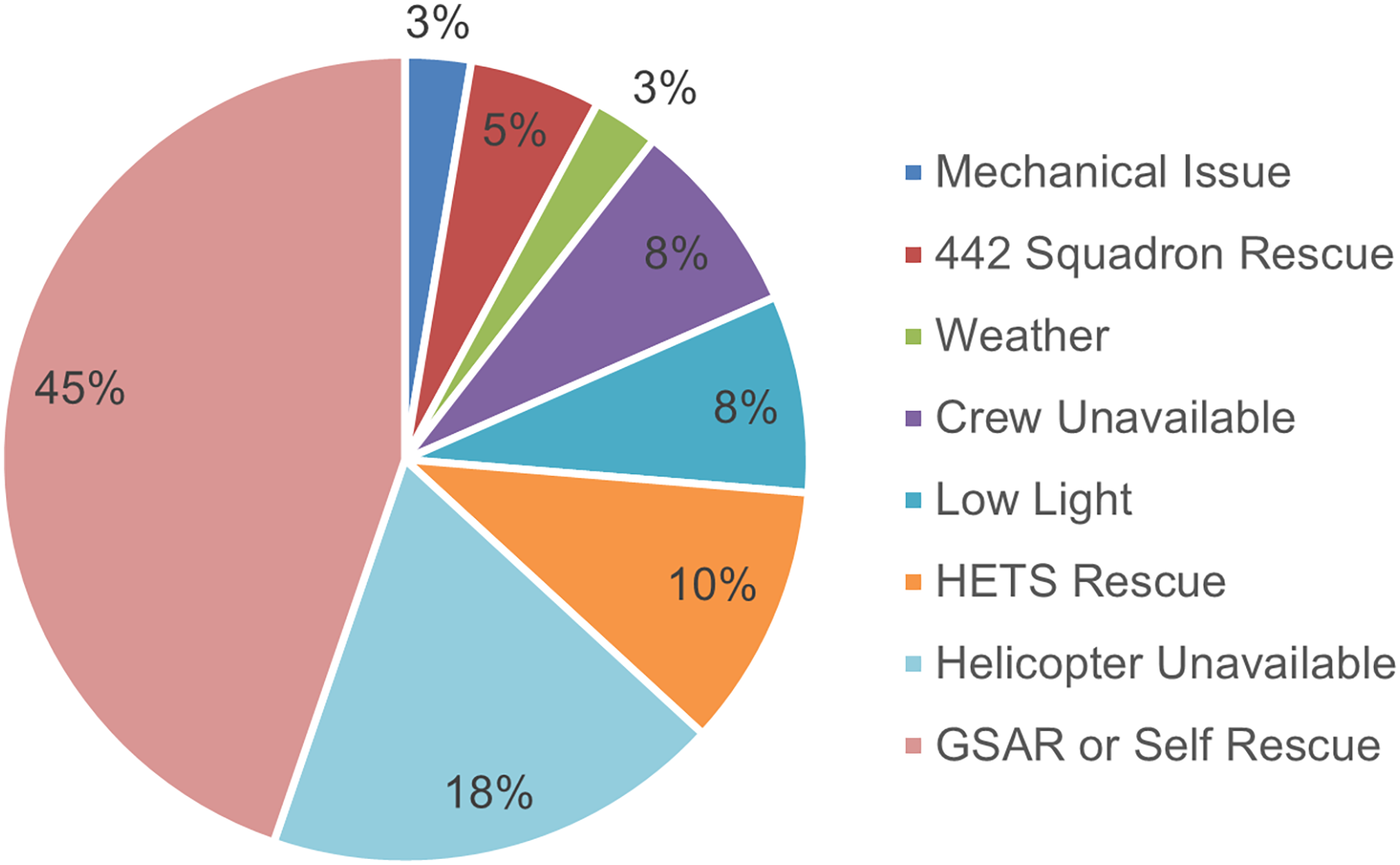
Factors that led to AR1 medical tasks not being completed.
Forty-five percent of medical rescues in the study period were called off due a rescue taking place by a ground SAR group or due to the subject managing self-rescue (Figure 5). It is important to note that AR1 was already activated and enroute in many of these callouts prior to being canceled. Eighteen percent of medical rescues were canceled due to the helicopter not being available on task activation. Other factors that led to a rescue not being completed by AR1 include inclement weather, mechanical issues, unavailable crew, and low light.
Analysis of callout statistics shows very short on-scene times, even when complicated access and patient stabilization and treatment were required (Table 1). A review of an illustrative sample of 17 medical rescue calls between November 8, 2014, and September 26, 2016, for which detailed flight data were available, shows a median of 15 (IQR 4–23) min for a ground SAR team to request AR1 and a median of 1 h (IQR 47–69 min) from helicopter request to takeoff. This time from request to takeoff includes the contractor pilot’s travel time to base and initial warming up of the helicopter. Once on scene, the arrival time to first patient contact was a median of 6 (IQR 2–10) min. On-scene time, or time from first patient contact to patient and crew loaded on the helicopter, was a median of 21 (IQR 11–33) min.
Callout statistics based on 17 medical rescue calls performed between November 8, 2014, and September 26, 2016.
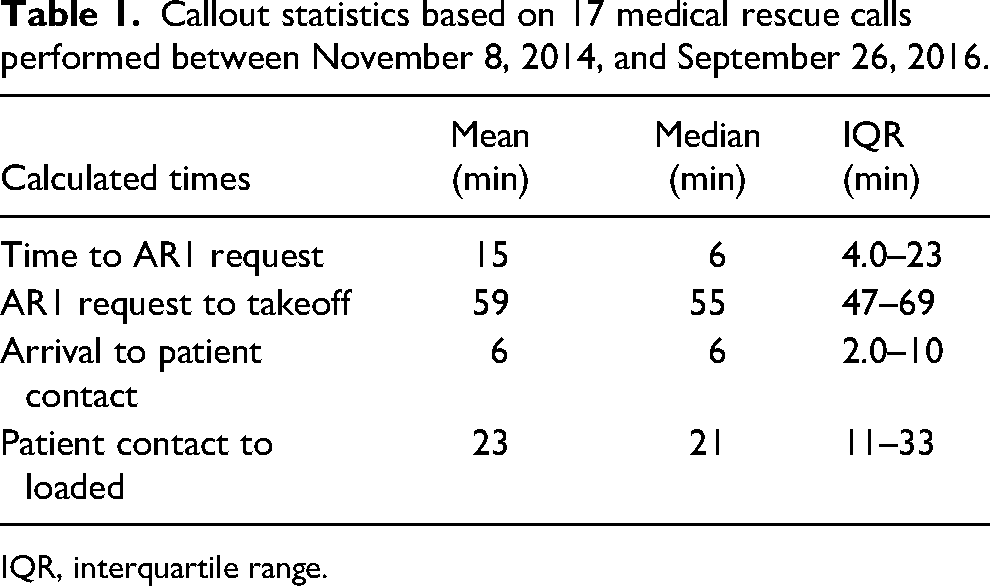
IQR, interquartile range.
Several illustrative examples of previous AR1 missions that demonstrate the organization's abilities in safely and efficiently accessing patients are summarized in the online Appendix. 5
Discussion
Rural SAR operations are inherently dangerous and complex operations. Even more so, helicopter winch rescue possesses its own sets of risks and limitations. Maintaining a high level of technical rescue proficiency, medical knowledge and experience, clear communications, and an organized workflow is paramount to mission success. While it is clear that this unique combination of skills provides an important resource in an environment as austere as BC, it therefore requires continuous quality improvement to ensure that it remains effective, efficient, and reproducible in other areas. In reviewing the data available from AR1 operations, 3 main areas were highlighted where improvements may benefit future development—diagnostics, tasking, and reporting.
Diagnostics
The standard AR1 air crew consists of 4 crew members—1 pilot, 2 rescue technicians, and 1 winch operator. While the Bell 412 helicopter is well suited for winch rescues, the interior configuration of the stretcher, medical equipment, and rescuers can complicate management of the patient. Additionally, noise and vibration generated by the helicopter make physical examinations difficult and may render vital signs or diagnostic measurements inaccurate. Auscultation, for example, can only be performed when the rescue technician is on the ground with the patient and requires the rescuer to remove personal protective equipment such as helmets. While the available diagnostic tools on the AR1 helicopters include standard advanced life support equipment such as cardiac monitor with defibrillator, 12-lead electrocardiogram, end-tidal carbon dioxide monitor, pulse oximetry, and adjuncts such as video laryngoscopy, the unique environment of the helicopter and the nature of austere prehospital medicine would most likely benefit significantly from the introduction of a diagnostic tool such as point-of-care ultrasound (POCUS).
There is a growing application of POCUS as a diagnostic tool for identifying life-threatening injuries in prehospital environments. In rural Canadian hospitals and clinics, primary and emergency physicians have seen increased access to POCUS from 60% in 2013 to >90% in 2019. 6 However, to date, neither BC SAR groups nor AR1 use portable POCUS devices in the field.
A recent study from the Medical College of Wisconsin Department of Emergency Medicine analyzed charts of 213 helicopter transports to determine possible use of various POCUS protocols in the field. The authors found that 51% of trauma patients would potentially benefit from an Extended Focused Assessment with Sonography in Trauma exam and that 65% of shock patients would potentially benefit from a Rapid Ultrasound in Shock exam. 7 These figures include patients who were direct scene transports with a presumed critical diagnosis necessitating emergency air transport to a tertiary care center as well as interfacility critical care transfers. Based on these data, one can infer that patients transported directly from the casualty scene would most benefit from POCUS. A 2018 German cohort study showed that prehospital ultrasound use resulted in a change in management in 50% of patients, 33% of which were transport-related changes. 8 For example, lung ultrasound in trauma to evaluate for pneumothorax prior to transfer could be critical because helicopter transport may lead to pneumothorax exacerbation with changes in air pressure. This is especially relevant for rural sites at higher elevations. With a diagnosed pneumothorax, the informed flight crew can be extra vigilant of vital signs and be prepared for chest decompression in the event that the patient becomes unstable. Additionally, polytrauma and hypothermia may mask other injuries, especially in patients suffering from blunt force trauma to the chest and abdomen. POCUS, with proper training and deployment, could improve patient outcomes by improving assessment capabilities and directing emergent treatments. POCUS also can guide management decisions regarding fluid resuscitation and shock, improve destination selection, improve prearrival preparation, and help determine resource utilization for receiving hospitals. Previous studies have evaluated and proven the success of effectively training rescue crews in POCUS in as short a time as 2 days using a combination of free open-access medical education, hands-on practice, and learning assessments. Integrating future POCUS training into the AR1 program would be feasible with minimal training-related financial and cognitive load. 9
Tasking
The current emergency management model within BC, under the jurisdiction of Emergency Management British Columbia, only allows AR1 to be tasked as an extension of a SAR group. Medical calls are primarily the responsibility of BCAS, which, in turn, calls on regional SAR groups to handle rescues in remote and difficult-to-access areas. AR1 then can be called on by a SAR search manager as a mutual-aid asset in cooperation with VSAR. This process can prolong activation time and ultimately time to patient contact. One of the disadvantages of this process is that many remote SAR groups may not have well-established relations with BCAS or AR1, resulting in lack of awareness of AR1's capabilities and activation procedures. Expanded education on AR1's capabilities to remote and rural communities, as well as establishing a clear memorandum of understanding with local and regional organizations, could significantly help in addressing this issue. As an alternative, operating procedures may be changed for AR1 to be dispatched directly by BCAS. Currently, only special road rescue units are dispatched directly by BCAS. 10 Adding AR1 as a special rescue unit dispatchable by BCAS would streamline operations and allow ground SAR teams and other responding agencies to use their resources more efficiently (Figure 6).
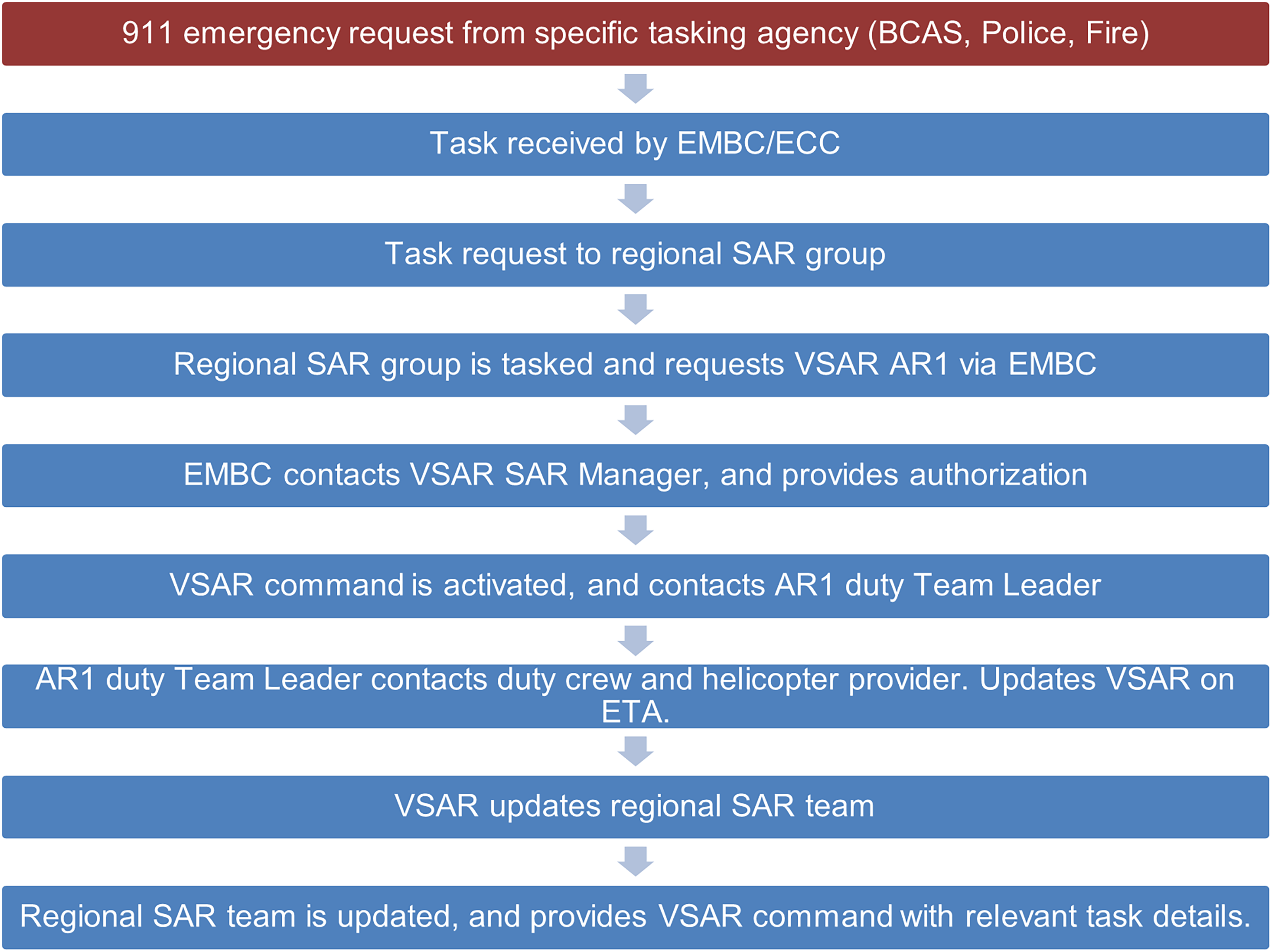
Tasking procedure demonstrating interagency involvement.
Additional considerations of factors that affect the ability of AR1 to complete calls include crew readiness, helicopter availability, and presence of night-capable operations. Continued emphasis should be on ensuring that these resources are available on a consistent basis and expanding night-vision equipment and training. Consistency in 24/7 response capability is critical in ensuring that an agency can be called on in a reliable manner and will increase aid requests.
Ultimately, AR1 is a mutual-aid asset that supports the regional SAR group. In many instances, a ground team may succeed in locating, accessing, stabilizing, and transporting a patient to an ambulance. However, unlike AR1, BC ground SAR teams rarely transport patients to a clinic or hospital and often lack the advanced medical capabilities useful in the austere environment.
While the AR1 helicopter is specially equipped with a winch and medical equipment, it is not solely dedicated to rescue response. As such, AR1 is limited by diversion of the helicopter by the contracting company for more profitable activities such as aerial firefighting and heliskiing. AR1 is currently working on securing a more reliably available helicopter that will also include night-vision capabilities. Medical conditions that may be considered minor or easily addressed in an urban setting are particularly challenging when compounded by isolation, dangerous terrain, and harsh environments. Therefore, streamlining activation procedures and minimizing response times are critical for the effectiveness and efficiency of such a resource.
Reporting
Analysis of existing limited AR1 callout data highlights the need for implementing a standardized reporting and documentation system within the program. The team has used several premade forms to provide a handoff report to BCAS, sometimes relying on verbal handoffs or retrospective documentation. Due to a lack of documentation, at least 26% of the calls lacked information on the type of injury and 15% on the mechanism of injury and could not be further classified in this study. Additionally, in most of the available medical cases, there was no record of medical interventions or care given during extraction and transport.
There is much value in optimization of data collection, which is useful for future research, evidence-based prevention strategies on a community level, and internal quality improvement. 11 Data collection should be performed in a standardized template and include the type of medical emergency, mechanism of injury, details of the injuries or illnesses, and specific interventions and treatments performed throughout the operation. For example, the National Advisory Committee for Aeronautics score is widely used to evaluate the severity of trauma and medical emergencies in the prehospital setting and could be implemented to optimize SAR operations in the future. 12
Specifics about medical and flight information, including mechanism of injury, geographic location, and terrain type, also can be vital for targeted fundraising efforts, effectively demonstrating AR1's unique capabilities and impact on BC communities. Such information also can be used for much-needed public awareness campaigns, both to improve awareness of the AR1 program and to provide communities with evidence-based injury-prevention strategies and wilderness safety education.
Limitations
Several limitations were encountered throughout this research, some of which form the basis of recommended improvements regarding reporting. This was a retrospective study using a database that was not designed for the purpose of this research, and data were limited by consistency and availability of records. Clinical information, such as type and mechanism of injury, was limited mainly due to missing, incomplete, or nonstandardized records, and long-term patient outcomes after transfer were not available, limiting the strength of the data. Additionally, while AR1's versatility is clear, there was no analysis to compare AR1's callout statistics and patient outcomes with alternative rescue options. This would establish the unique need for this particular type of rescue program as opposed to the standard GSAR groups. Finally, additional studies are needed to substantiate the discussion on impact to patient outcomes regarding the use of POCUS in helicopter emergency medical services.
Conclusions
The AR1 team is a critical and highly skilled asset to prehospital care in BC. This program has demonstrated its unique capabilities in providing access to advanced medical care in remote and difficult-to-access areas. Without its capabilities, similar patients are subjected to significant delays in care, and both patients and responders experience additional environmental risks. While AR1 has advanced life support capabilities, the addition of POCUS would be a relatively inexpensive tool that might significantly improve quality of care and resource utilization. Additionally, streamlining BC's SAR callout procedure is needed to ensure more direct and efficient access to mutual-aid entities such as AR1. Finally, collection of detailed medical and flight information should be improved with a standardized documentation system, which would facilitate internal education and quality improvement as well as future research into the program's breadth of impact on emergency prehospital care.
Supplemental Material
sj-docx-1-wem-10.1177_10806032241258425 - Supplemental material for A Qualitative Review of the Air Rescue One Rural Search and Rescue Program in British Columbia, Canada
Supplemental material, sj-docx-1-wem-10.1177_10806032241258425 for A Qualitative Review of the Air Rescue One Rural Search and Rescue Program in British Columbia, Canada by Raphael Nowak, Jeremy N Vandekerkhove and Deena D Wasserman in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
The authors acknowledge the support and contributions of the Vernon Search and Rescue Society and the Air Rescue One Heli Winch Society in the writing of this paper, including the valuable input from Drs. Jared Baylis and Nick Kuzak.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RN and JV are British Columbia SAR volunteers, and JV is the executive director of the Air Rescue One Heli Winch Society and a paramedic with the BC Ambulance Service.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.