
Abstract
Introduction
B-lines on lung ultrasound have been found in asymptomatic competitive breath-hold divers, but their significance and time to resolution are not well understood. We sought to investigate the relationship between B-lines, oxygen saturation, and respiratory symptoms after competitive dives to diagnose pulmonary injury.
Methods
We performed lung ultrasounds before (predive), immediately after (postdive), and within 1 h (follow-up) of a competitive dive. B-lines were counted in each intercostal space in the anterior, lateral, and posterior lung fields, and the highest number of B-lines within a space was recorded for each lung region. At follow-up, each diver's oxygen saturation and respiratory symptoms were recorded. Statistical analysis included the Kruskal–Wallis test, Spearman's correlation, and sensitivity and specificity calculations.
Results
Forty-four divers completed 143 individual dives of four different disciplines. The median number of B-lines was 0 (IQR inclusive=0) predive, 1 (IQR=3) postdive, and 0 (IQR=1) at follow-up. There was a significant difference in total B-lines between measurement times (p<0.001). Sensitivity and specificity of hypoxemia, clinically significant B-lines, and both measures in tandem in detecting respiratory symptomatology were 52% and 76%, 24% and 92%, and 24% and 95%, respectively.
Conclusions
B-lines are a common phenomenon in competitive breath-hold divers on surfacing and decrease within 1 h, suggesting a physiologic fluid shift. B-lines are negatively correlated with oxygen saturation, indicating that extravascular fluid impairs gas exchange in the lung. Neither hypoxemia nor clinically significant B-lines were found to be reliable indicators for respiratory symptomatology, suggesting that there may be multiple phenotypes of freediving-induced pulmonary syndrome.
Introduction
Breath-hold divers, often called freedivers, can reach significant depths on a single breath hold, far exceeding the recreational depth of scuba divers and in a much shorter time frame. With deeper dives, athletes report pulmonary symptoms believed to result from immersion pulmonary edema and/or barotrauma of descent. 1 This is colloquially referred to as a squeeze by many breath-hold divers, and a recent workshop suggested using the term freediving-induced pulmonary syndrome (FIPS) to encompass both barotrauma and immersion edema when the etiology is unknown. 1
Pulmonary edema can be diagnosed in the field with ultrasound evaluation for B-lines, pulse oximetry, and reported symptoms.2,3 In freediving, pulmonary ultrasound has been suggested as a potential diagnostic measure for identifying pulmonary edema or barotrauma of descent. 4 B-lines indicating extravascular pulmonary fluid have been found after asymptomatic competitive dives,2,4,5 but the number, distribution, and duration of these B-lines are not well understood in determining the presence or extent of lung injury. 2
A pneumothorax can be diagnosed via ultrasound 6 and could possibly occur in freedivers who “pack” before a dive, filling their lungs beyond the total lung volume. Such overinflation using glossopharyngeal insufflation 7 has been shown to cause pneumomediastinum,8,9 and pneumothorax has been reported as a consequence of freediving. 10 The increased pressure from this air can cause alveolar rupture either at the onset of the dive or toward the end, when air redistributed at depth expands on surfacing. Therefore, some divers decide to exhale several meters before surfacing.
Competition organizers such as the Association Internationale pour le Développement de l’Apnée (AIDA), headquartered in Geneva, Switzerland, provide diagnostic criteria for squeeze as the presence of hypoxemia (SpO2≤95%) in conjunction with hemoptysis and have proposed frequent reevaluation periods for divers with a squeeze and suggest that pulmonary ultrasound could be a useful tool for medical staff as an adjunct to lung auscultation and finger pulse oximetry, which could be unreliable in patients with peripheral vasoconstriction. 11 The ability to diagnose pulmonary injury in the competition arena is relevant to the allocation of limited medical supplies in remote locations where evacuation is difficult. Return-to-diving guidelines are currently based on expert opinion. 12
We hypothesized that most B-lines after freediving are a regular physiologic phenomena that occur after immersion and naturally resolve within an hour of exiting the water. We postulated that the presence of persistent clinically significant B-lines, defined as three or more within an intercostal space, 13 along with associated respiratory symptoms, would be diagnostic for squeeze.
Methods
This study was done in accordance with the Declaration of Helsinki and was approved by the University of California, San Diego institutional review board as study 807628.
This study was an observational pre–post study with convenience sampling. Freedivers competing in the Vertical Blue 2023, the Confederation Mondiale Des Activites Subaquatiques (CMAS) Freediving World Championships 2023, and Blue Element 2024 were invited to participate. Volunteer competitors were given the option to participate in data collection prior to their dive (and before any warm-up dives), immediately after their competition dive (within 1 min of receiving their card from the judge, which could take up to 30 s after the 15 s allotted to perform the competition surface protocol, prior to any medical evaluation or treatment), and/or within 1 h after their dive (follow-up). Precise timing from surfacing was not recorded because many athletes did not know the exact time that they surfaced and presented for measurement at varying intervals after their dives. All athletes were required to check out of the competition area within 1 h of their competition start time, which could be adjusted slightly (as deemed by the judges) according to the previous diver's performance and/or any delays. At Vertical Blue and Blue Element, competitors were recruited at the registration area, where they were required to check in and check out of the competition each day. At CMAS, competitors were recruited from a support vessel central to the marine competition area.
After signing a paper consent form, volunteer competitors were assigned a random number. Participants were instructed to keep the same number for subsequent days and data-collection instances. Then they were directed to the data-collection area and informed of the times in relation to their scheduled competitive dive that they could present for data collection.
Lung ultrasound using the Vscan Air CL (GE Healthcare, Chicago, IL) or EagleView Cprobe-CL (Wellbin Technology Co Ltd, Tuen Mun, Hong Kong) connected to an iPad 10.2 (Apple Inc, Cupertino, CA) was performed using the curvilinear probe (2–5 MHz) on a lung setting held perpendicular to the ribs to visualize multiple intercostal spaces. Participants were scanned in the anterior, lateral, and posterior lung fields on bilateral sides. A recording of the iPad screen was taken, with the verbal statement of the subject's number and each measured field as the ultrasound was performed. A separate researcher reviewed all the videos later and counted B-lines for each subject and each recorded field. B-lines were counted for each intercostal space within a lung field (maximum of three), and the intercostal space with the highest number of B-lines was recorded as the result of that lung field. Then the total number of B-lines from all six fields was tallied for a sum, with 18 B-lines being the highest possible value. If there were any areas with absent lung sliding, this was also noted.
Heart rate and oxygen saturation were measured by a pulse oximeter (MightySat Rx Fingertip Pulse Oximeter, Masimo Corp, Irvine, CA). This pulse oximeter shows dimmer values when first placed on the finger; then the numbers brighten once a full reading has been taken. The value recorded was that of the bright numbers that stayed on the screen for more than 1 s, as was the convention accepted by the medical team that took those same measurements during check-in and check-out. During the follow-up evaluation, participants also were asked to fill out a survey of their dive profile, whether or not they packed predive and exhaled before surfacing (to account for pneumothorax risk), and any respiratory symptoms they were experiencing at that time. Fluid intake was not surveyed. Age, gender, and years of experience were not collected because the focus of the data collection was on the characteristics of each individual dive.
Statistics
Statistics were calculated using Statistics Kingdom's online calculators. Due to the nonparametric nature of our data, a Kruskal–Wallis test was run to compare the median number of B-lines at each of the three different measurement points. A post hoc Dunn's test with Bonferroni correction was run to determine which measurement times were significantly different. Spearman's correlation was calculated to compare B-lines with oxygen saturation. A p value of <0.05 was considered significant.
Results
A total of 44 competitive freedivers volunteered for the study. They volunteered to have data collected before (predive), immediately after (postdive), and/or within 1 h (follow-up) for 143 individual dives, which varied in depth and discipline over multiple competition days. On each competition day, each individual diver performed only one competition dive. Dives of a different discipline and/or depth on a different day were considered a new dive for measurement. A total of 53 predive, 73 postdive, and 86 follow-up measurements were recorded for a total of 212 measurements. The median number of B-lines was 0 (IQR inclusive=0) predive, 1 (IQR=3) postdive, and 0 (IQR=1) at follow up. Nine divers (17%) had B-lines predive compared with 41 divers (56%) postdive and 28 divers (33%) at follow-up. Seventeen dives had all three measurements completed (Figure 1).
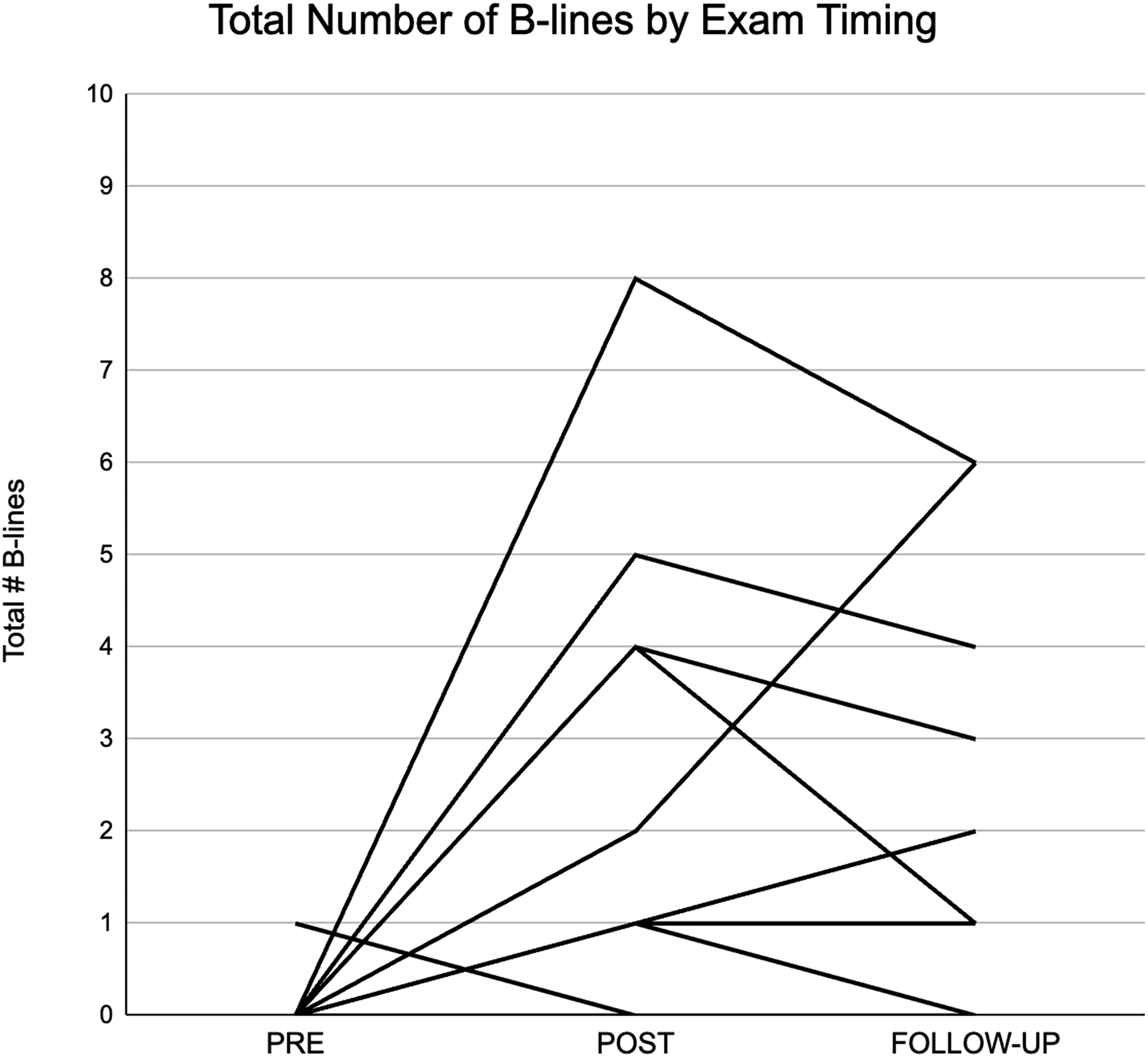
Change in total number of B-lines across dives measured at three time points.
Eighty-nine divers had filled out surveys during follow-up measurements. Twenty-six (29%) reported respiratory symptoms, five of which were noted to be symptoms present prior to the dive and thus excluded. Seventeen (19%) sought treatment with oxygen between the postdive and follow-up measurements (Table 1). Seven divers (41%) who sought treatment postdive still had symptoms at follow-up.
Comparison between divers who sought treatment after a dive

Divers competed in the following disciplines: free immersion (FIM), constant weight (CWT), constant weight bifins (CWTB), and constant weight no fins (CNF). Results by discipline are displayed in Table 2.
Comparison between dive disciplines
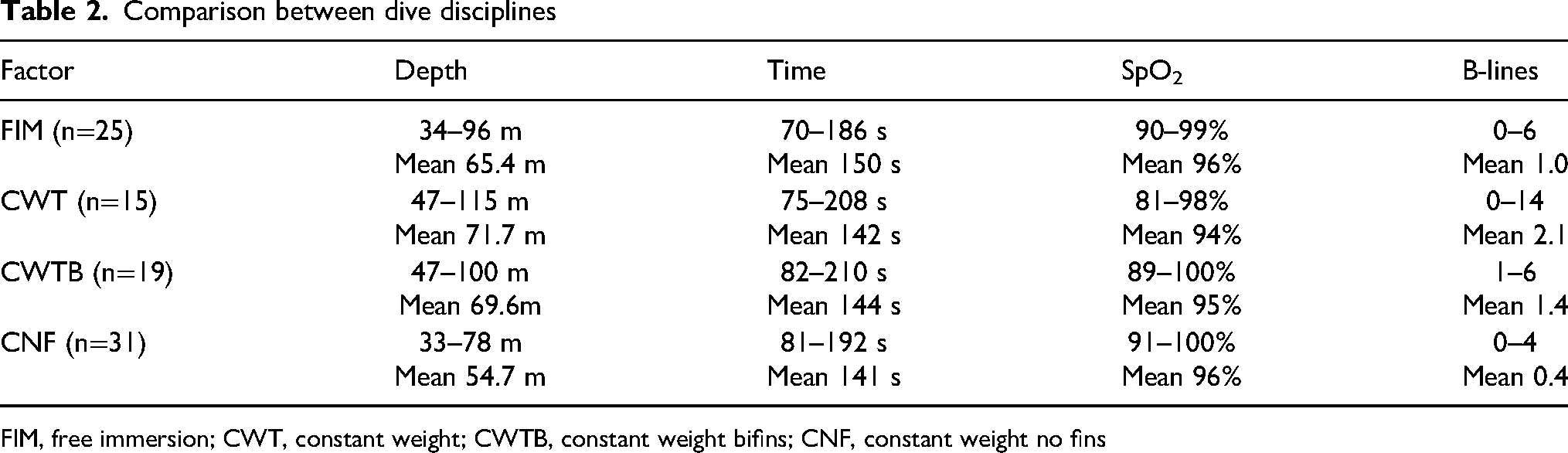
FIM, free immersion; CWT, constant weight; CWTB, constant weight bifins; CNF, constant weight no fins
Based on the high degree of variability between dives, with individual divers diving a wide range of depths and disciplines and participation in the study data collection being voluntary, we chose to examine B-line measurements as independent groups despite our data containing both paired and unpaired measurements because individual pairwise and unpaired tests would be limited by the small sample sizes that completed all three measurements (n=17). The Kruskal–Wallis test was selected based on the nonparametric nature of the B-lines data, and predive, postdive, and follow-up measurements were assessed as independent groups in order to include all data points, which include both independent and dependent measurements. The results of this test indicate a significant difference between the three measurement times (χ2(2)=25.37; p<0.001) with a mean rank score of 81.34 for predive, 128.99 for postdive, and 102.92 for follow-up. The post hoc Dunn's test using a Bonferroni corrected alpha of 0.017 indicated that the means between predive and postdive (p<0.001) and postdive and follow-up (p=0.002) were significantly different. The difference between predive and follow-up (p=0.020) did not reach significance. Figure 2 provides a visual representation of the change in B-line data across all time measurements.
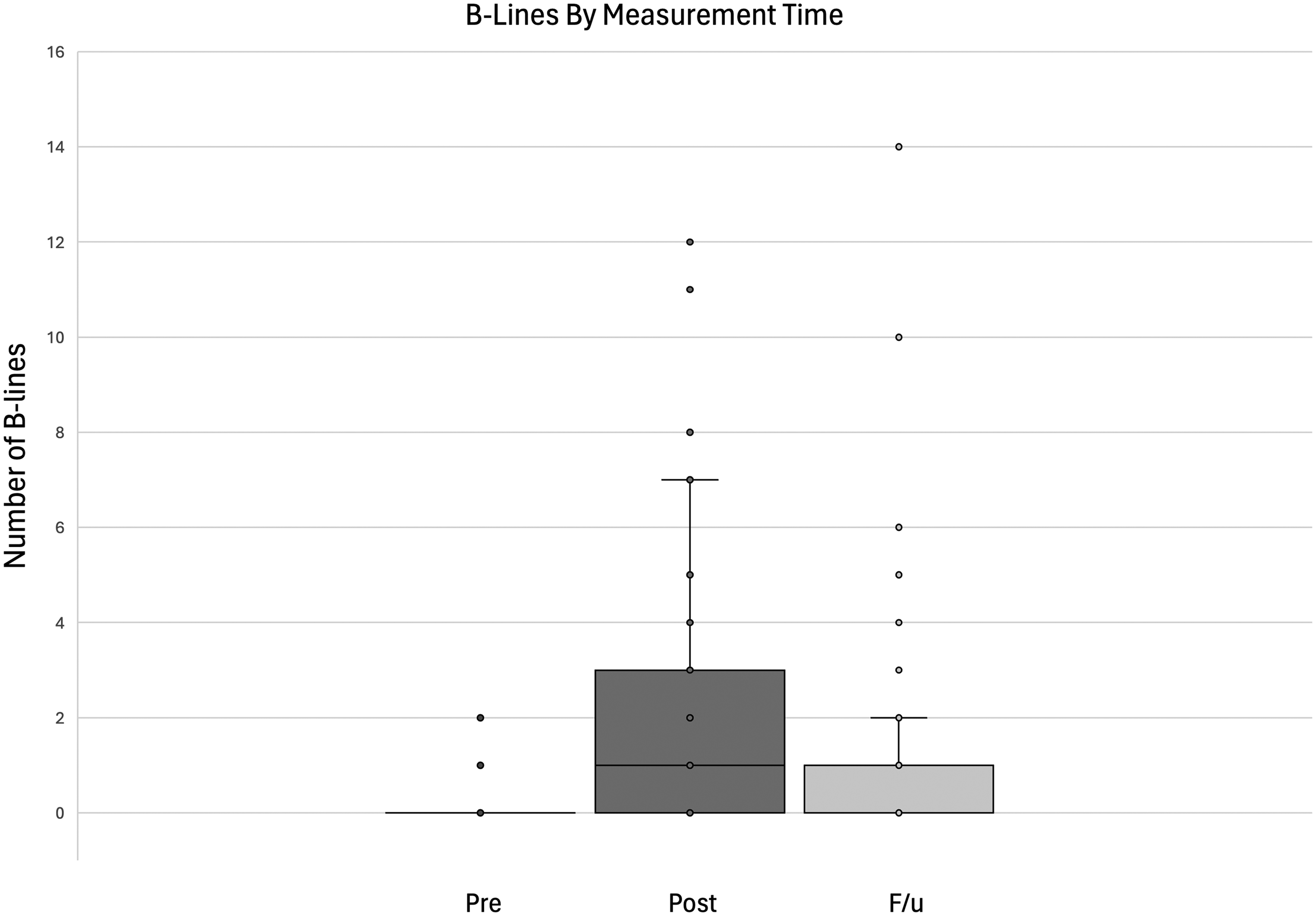
Box and whisker plot for total number of B-lines by time point.
A Spearman's correlation was run to determine the relationship between total B-lines at follow-up and oxygen saturation (SpO2) at follow-up. There was a medium negative monotonic correlation between total B-lines and SpO2 (r(84)=–0.323; p=0.002). A scatterplot depiction of these data is shown in Figure 3.
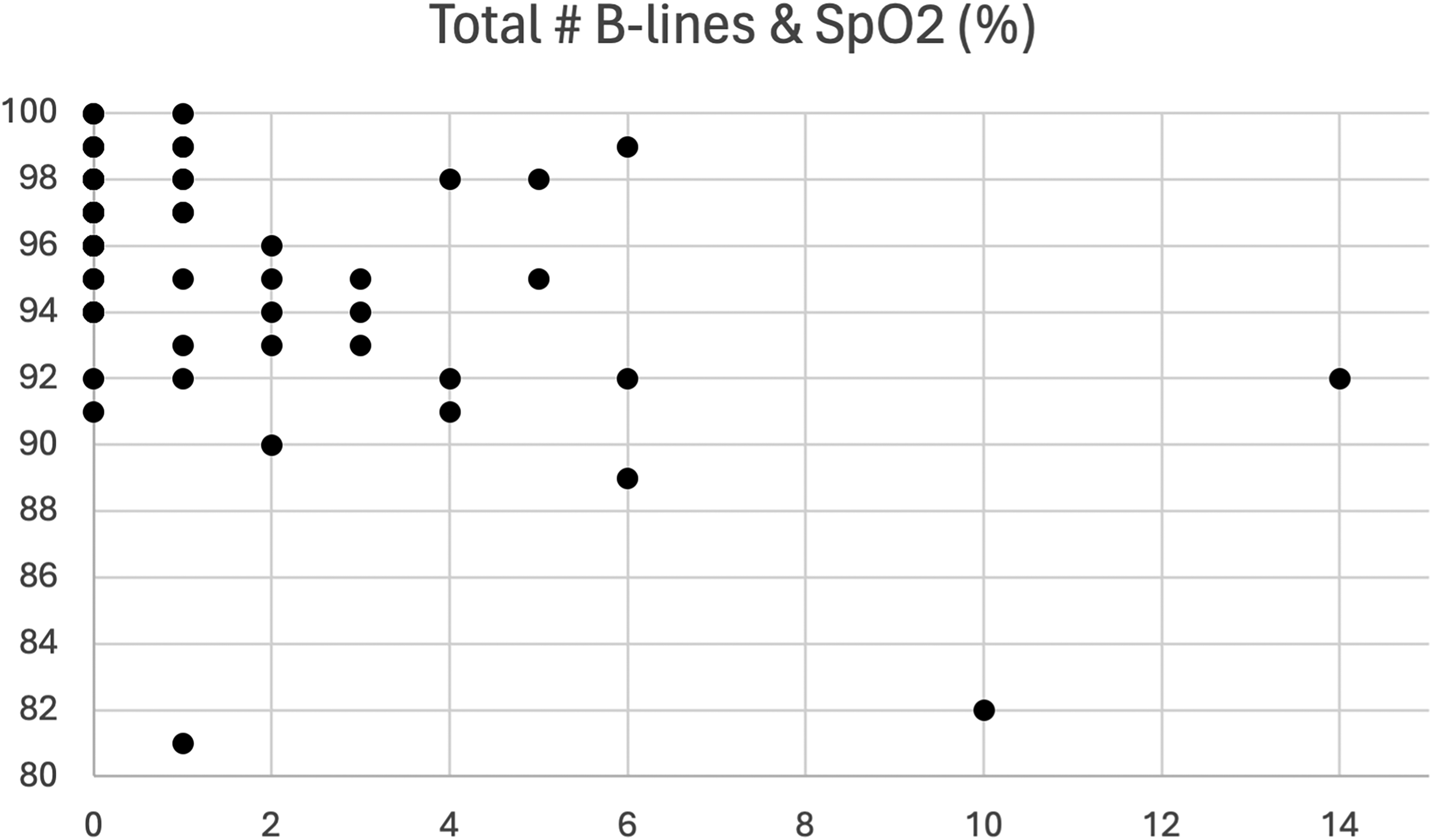
Scatterplot of B-lines and SpO2 measured at follow-up.
We evaluated the sensitivity and specificity of pulse oximetry as a screening exam for squeeze, as defined by the presence of self-reported symptoms on the questionnaire. Using a cutoff of SpO2≤95%, pulse oximetry alone was 52% sensitive and 76% specific for respiratory symptomatology. Clinically significant B-lines—defined as three or more B-lines within a single intercostal space—were 24% sensitive and 92% specific for symptomatology after a dive. When combined, the sensitivity and specificity of these diagnostic tests in tandem were 24% sensitive and 95% specific for detecting symptomatic divers.
Squeezes
Using the AIDA definition of a squeeze (ie, bloody sputum and SpO2≤95%), four squeeze incidents were documented in the study. Of those, two divers (50%) had no B-lines on lung ultrasound, whereas the other two divers (50%) had a large number of B-lines (ie, 10 and 14), with clinically significant B-lines seen in three or more lung fields. Other notable respiratory symptoms besides bloody sputum also were documented among many divers and are described in Figure 4.
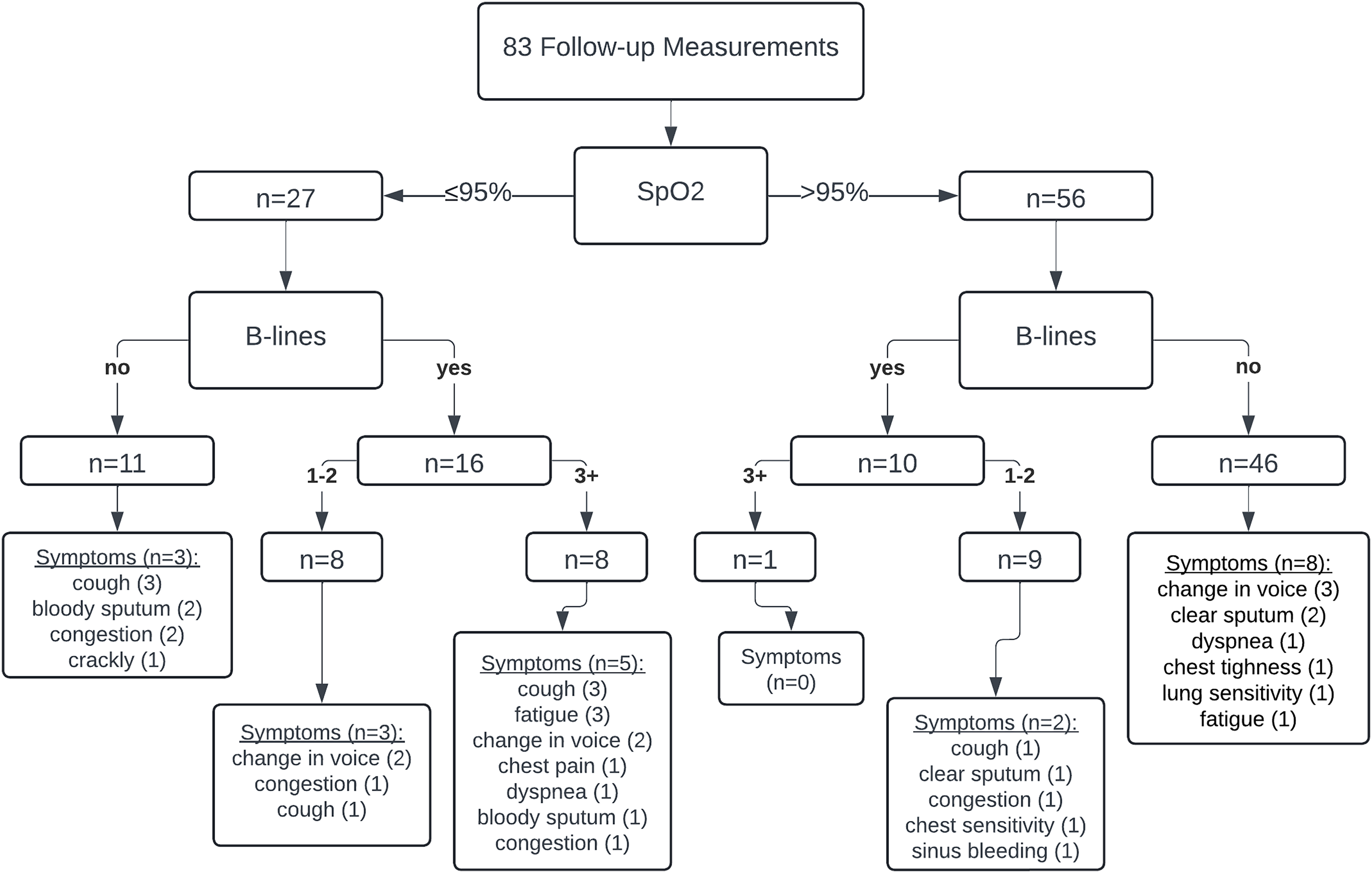
Follow-up measurements including pulse oximetry, lung ultrasound, and survey of symptoms.
Discussion
Our study found a significant increase with subsequent decrease in the number of B-lines measured across three time points in competitive freedivers. These findings support the theory that B-lines represent a natural fluid shift secondary to immersion and naturally resolve once out of the water. Findings from previous studies suggest that B-lines occur in 45% of subjects after freediving and have 100% resolution within 24 h. 3 Our measurements immediately postdive were similar to those from the Frassi study with B-lines 56% prevalent, dropping to 33% at 1-h follow-up.4 This trend suggests that B-lines may resolve faster than 24 h. Our study also found a higher incidence of respiratory symptoms at follow-up (29%) compared with the Frassi study (14%). 4
Our study found the lowest individual and mean oxygen saturations in divers who competed in the CWT and CWTB disciplines, in contrast to the Schagatay study that concluded FIM dives resulted in the most desaturation due to upper body work. 14 However, they measured SpO2 at 10 min, whereas we measured at the 1-h mark. It is possible that FIM causes more immediate desaturation, whereas our study showed that CWT/CWTB dives result in more persistent hypoxemia that may be indicative of a squeeze. The results of this study also confirmed findings from the Patrician study showing a correlation between increased B-lines and decreased oxygen saturation. 2
While the exact causes and pathophysiology of FIPS are still being explored at this time, 1 there is room for expansion of the definition beyond the AIDA requirement of bloody sputum and hypoxemia. 2 Our findings suggest that a wide array of respiratory symptoms can manifest independent of hypoxia or B-lines. In addition to edema, alveolar and/or tracheal hemorrhage, which can cause bloody sputum, are unlikely to be seen on ultrasound and are better imaged via laryngoscopy, bronchoscopy, 15 or computed tomography, 16 none of which are practical in a field setting. Edema limited to the upper airways, colloquially termed a tracheal squeeze,17,18 is unlikely to cause hypoxemia or result in B-lines, but it can result in upper airway symptoms of a change in voice or congestion. Varying findings from lung ultrasound, pulse oximetry, and a survey of respiratory symptoms can help diagnose different types of FIPS (Figure 5).
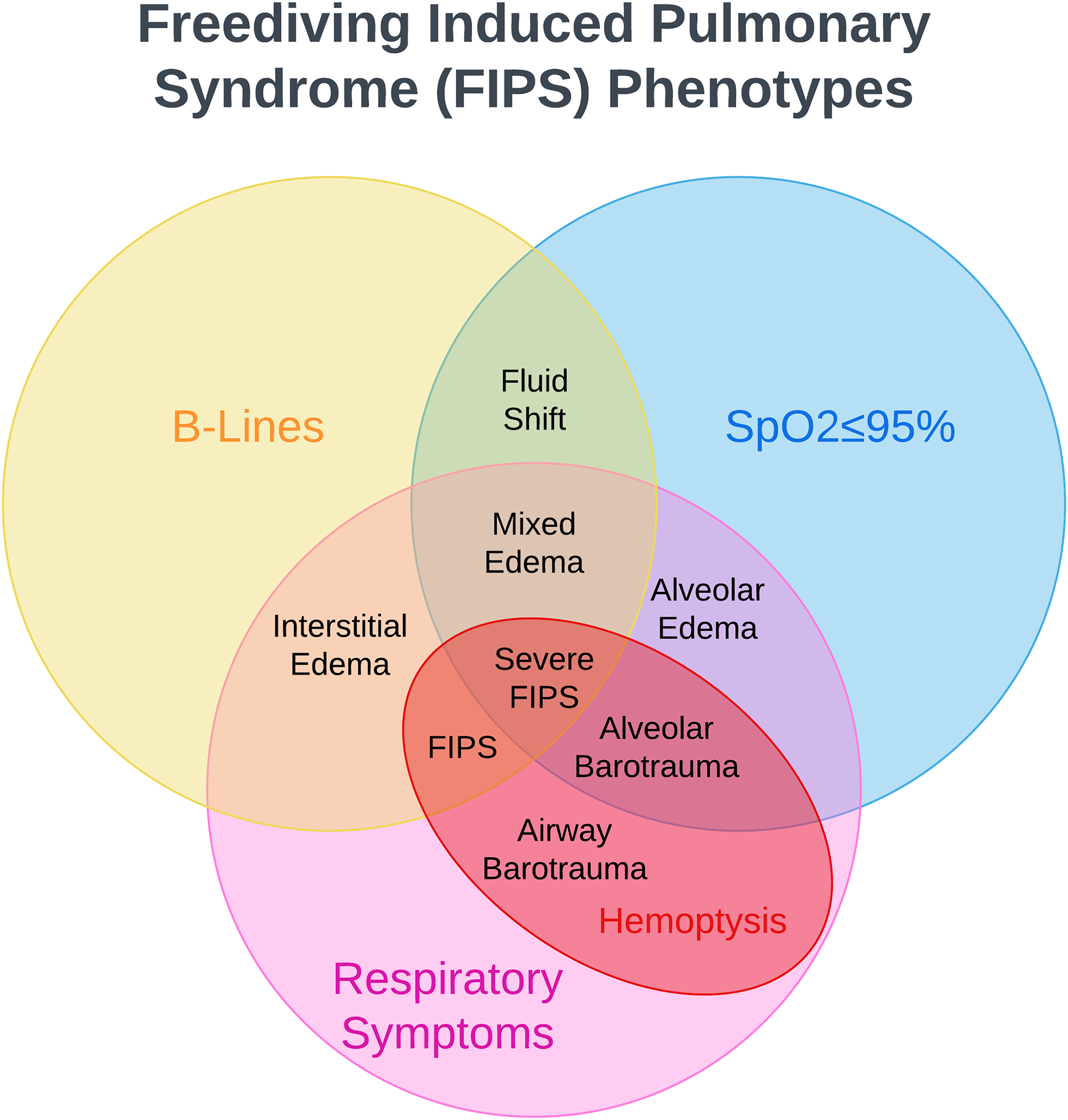
Different freediving-induced pulmonary syndrome (FIPS) phenotypes: alveolar edema, interstitial edema, mixed edema, alveolar barotrauma (lung squeeze), airway barotrauma (tracheal-bronchial squeeze), FIPS (edema and barotrauma), severe FIPS (edema and barotrauma with hypoxemia).
Our study found poor sensitivity of pulse oximetry and lung ultrasound for identification of respiratory symptoms among competitive freedivers. These results highlight the importance of continued investigation of diagnostic modalities as well as the role of clinical evaluation and contextualization for evaluating and diagnosing FIPS in the field.
Limitations
Due to limited research personnel and equipment, we were not able to measure oxygen saturation immediately after the dive, limiting our ability to track changes in pulse oximetry directly in tandem with B-lines. Additionally, because this was a convenience sample and participation was voluntary, we were unable to force divers to participate in measurement within an exact time frame given that many stayed in the water for varying amounts of time after their dives to support teammates or spectate other athletes, minimizing our ability to record the exact time between when each athlete completed their dive and had measurements taken. Therefore, we used a blanket time frame of 1 h because that is the upper limit of time the athletes had to check-out or leave the competition area.
Regarding the lower number of predive measurements, many divers did not want to have measurements taken predive because they did not want to disrupt their precompetition ritual(s). Although all measurements were blinded by random number assignment, some competitors may not have presented for data collection for fear that they may have findings consistent with a squeeze diagnosis, which, if made known to the judges, may have resulted in disqualification from the competition. Other reasons for loss to follow-up may include leaving early, being caught up with celebrations after a successful dive, or wanting to remain in or on the water longer. This variation in participation limited our ability to perform paired assessments of B-lines data across all time points and decreased the power of our sample size.
Future Avenues
In this study, we observed an increase in B-lines immediately following a dive, which appeared to mostly resolve by follow-up within a 1-h time-frame (Figure 2). In future studies, more accurately documenting the time from surfacing to the time of lung ultrasound and repeating ultrasound measurement at a later time point could help continue to track the decrease or persistence of B-lines and interpret their clinical significance.
Additionally, in future studies, it would be interesting to collect data and the type and duration of treatments competitive divers are receiving either from medical staff or self-administered and analyze the effect of varying treatments on the resolution of B-lines and improvement of symptoms.
Conclusions
Competitive breath-hold diving is associated with a spectrum of pulmonary injuries termed freediving-induced pulmonary syndrome (FIPS). The pathophysiology, diagnostic criteria, and treatment guidelines for FIPS are still being developed. The results of our study indicate that B-lines are a common finding immediately after competitive breath-hold diving and are significantly associated with decreased oxygen saturation. Most B-lines decrease within 1 h, indicating a physiologic fluid shift once out of the water. Tracking their complete resolution merits further investigation at future time points. Combining pulse oximetry, lung ultrasound, and screening for respiratory symptoms 1 h after surfacing can detect multiple types of FIPS.
Footnotes
Author Contribution(s)
Acknowledgments
We acknowledge William Trubridge and the Vertical Blue 2023 Safety Team for their support of our research. We also acknowledge Esteban Darhanpe and the CMAS 2023 Depth World Championships Safety Team for their support of our research. We also acknowledge Harry McCahill and the Blue Element 2024 Safety Team for their support of our research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Divers Alert Network (DAN), University of California, San Diego, the 2023 AUAS/DAN Diving Medicine Scholarship, and the 2023 DAN/Alfred Bove Research Grant for Cardiac Health in Scuba Diving.