
Abstract
Introduction
Facilities in austere environments may consider emergency care beyond their scope. Often patients with high-acuity conditions have no other choice than to present to these facilities. The disconnect between the intent of health systems planners and the reality faced by providers manifests as facilities unable to manage such cases.
The Indian Health Service, with a range of stakeholders, developed an emergency care delivery assessment tool for facilities in austere environments, designed to identify deficiencies in facility readiness for emergency care delivery across four areas:
1. Procedural 2. Human resources 3. Non-pharmacologic material resources 4. Pharmacologic material resources
Methods
The tool's underlying architecture is a resource matrix similar to hospital-based tools, using the “Facility” component of the WHO Emergency Care Systems Framework as the Y-axis and undifferentiated presentations taught by the WHO basic emergency care course, advanced trauma life support, and advanced life support in obstetrics as the X-axis. The tool was piloted at a remote frontier clinic.
Results
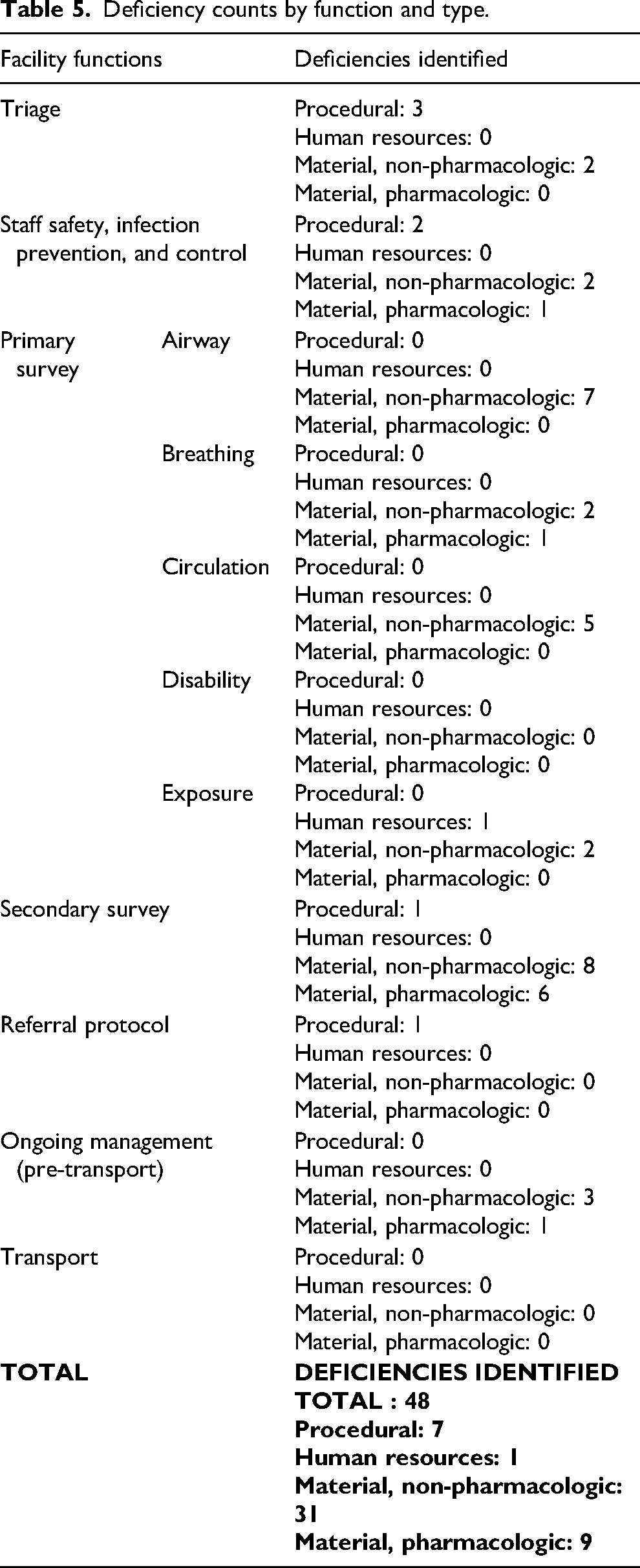
We found 48 deficiencies: 7 procedural, 1 human resources, 31 non-pharmacologic materials, and 9 pharmacologic materials. We aggregated deficiencies by facility function to assess the capacity to perform each. We also aggregated deficiencies by clinical presentation to identify targets for educational interventions.
Conclusion
We successfully created a novel emergency care capacity assessment tool for use in austere environments using materials with broad international consensus. The successful pilot found deficiencies across all 4 areas. This tool may be useful in many other remote domestic facilities and rural health posts in low- and middle-income countries.
Keywords
Introduction
Background
The Indian Health Service's (IHS) mission is to “raise the physical, mental, social and spiritual health of American Indians and Alaska Natives to the highest level.” IHS derives its mandate from article I, section 8, of the constitution, which was used to establish an intergovernmental relationship between the United States and Tribes. Included in this relationship is the provision of health services through the Snyder Act, which formally created IHS in 1921. 1 Many American Indians live in extremely remote and resource-poor settings. It has been estimated that in some regions, 60% of AI/AN households lack access to the internet, and 40% lack access to running water. 2 Healthcare must be delivered to these beneficiaries despite the significant challenges imposed by their geographic isolation. This is accomplished via a network of facilities, including health stations, clinics, health centers, critical access hospitals, and hospitals.
Many of these healthcare facilities located in austere environments consider “emergency care” beyond their scope of service. However, due to the isolated geographic location of these facilities, patients with high-acuity illnesses or injuries often initially present to these sites for care absent other alternatives. Facilities must stabilize and transfer such patients to higher levels of care as quickly and efficiently as possible, and they must also have the ability to provide the initial medical management of critically ill or injured patients. The disconnect between the intent of health systems planners and the reality faced by providers in austere environments manifests as facilities lacking the appropriate human and material resources needed to manage such cases.
These front-line rural facilities are essential points of emergency care delivery, though they are infrequently designed for this purpose. Facilities in extreme, remote environments that provide emergency care out of necessity frequently lack essential diagnostic capabilities. This hinders the establishment of definitive diagnoses and requires facilities to be prepared to stabilize and transport undifferentiated acute illness and injury. Assessing facilities’ capacity to do so effectively is a challenging task. Existing tools to assess emergency care capacity, such as the World Health Organization's Hospital Emergency Unit Assessment Tool (HEAT) and Columbia University's sidHARTe Emergency Services Resource Assessment Tool (ESRAT) were developed for use in the hospital setting and have limited applicability in remote health posts in austere environments.3,4,5 Therefore, a new context-relevant tool is needed for this special population.
Objective
We sought to develop an emergency care delivery assessment tool specifically for use in remote health facilities in austere environments. The development of this tool was a collaborative effort that included a range of key stakeholders, including the following:
Providers who practice in these settings Indian Health Service regional (area office) and subregional (service unit) leadership who support the facilities (eg, procure resources, support and hire the workforce, and write new policies) Wilderness and emergency medicine experts from the American College of Emergency Physicians Wilderness Medicine Section and the Wilderness Medical Society Procedural (eg, protocols such as triage, outside referral, and isolation). Human resources (both the presence and training levels/certifications of physicians, nurses, etc). Non-pharmacologic material resources. Pharmacologic material resources.
The tool was designed to identify gaps in four main areas:
The tool's output was a structured report of findings including a checklist for follow-up on action items and deliverables that were given to leadership for action.
Methods
This project was granted quality improvement exemption by the Phoenix Area Indian Health Service Institutional Review Board (IRB).
The assessment tool's underlying architecture is a resource matrix similar to the Hospital Assessment Tool (HEAT), which was developed by WHO to assess hospital readiness to care for the acutely ill patient. 3 The Emergency Services Resource Assessment Toolkit (ESRAT) is a similar hospital-based emergency care assessment to evaluate a facility's capacity to care for undifferentiated acute illness.4,5 Utilizing this architecture required the development of two axes that form a matrix. The Y-axis is composed of the essential functions of the facility in delivering emergency care. The X-axis serves as the clinical benchmarks against which the clinic's capacity is measured.
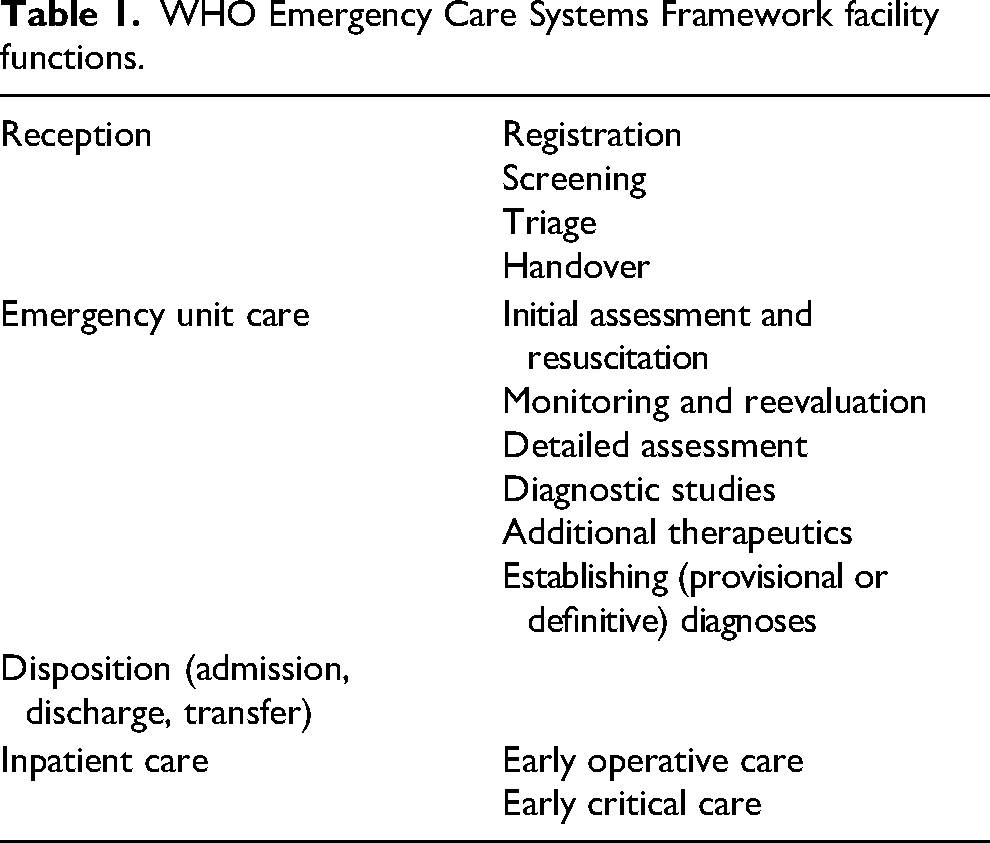
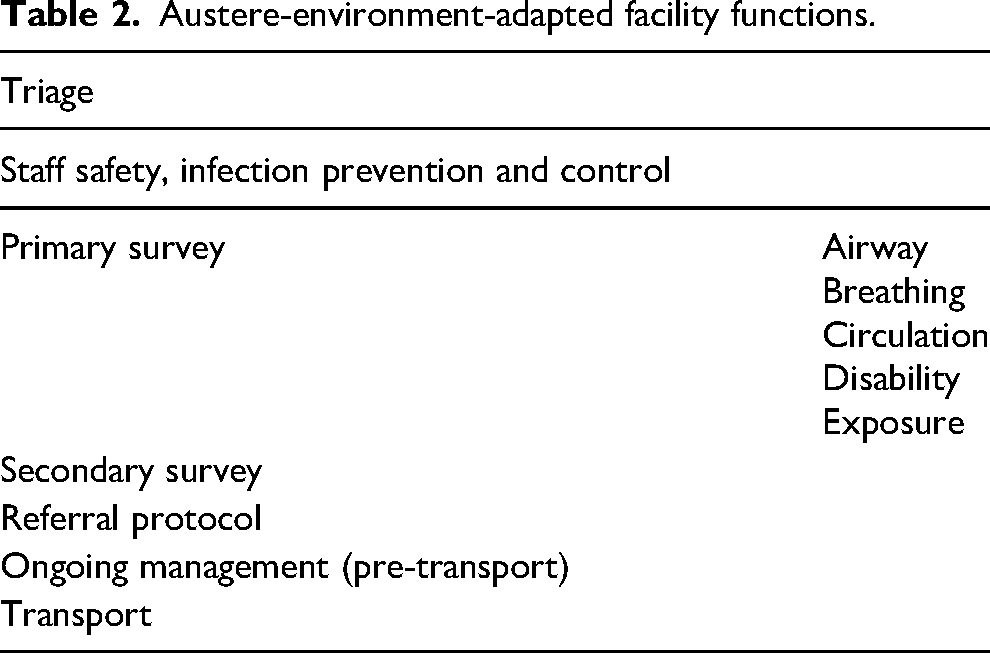
The first task in development was to define the essential functions of these remote clinics. We began with the “Facility” component of the WHO Emergency Care Systems Framework and adapted it to only include those services that have applicability in this context. Table 1 shows the WHO Emergency Care Systems Framework that served as the starting point for our Y-axis development. Table 2 shows the finalized set of essential functions for emergency care delivery in our remote facilities.
WHO Emergency Care Systems Framework facility functions.
Austere-environment-adapted facility functions.
The tool must then assess a facility's capacity to perform each of these functions. The X-axis outlines unique clinical scenarios that such a facility must be prepared to encounter. Most acutely ill and injured patients presenting to these facilities will remain undifferentiated throughout their encounters, and thus evaluating performance in addressing specific diagnoses would not reflect the reality faced by providers in these settings. We therefore opted to measure performance in managing largely non-disease-specific conditions (ie, undifferentiated presentations) that are utilized by emergency care courses. We ensured that the concepts from the following relevant courses were covered in the development of this tool:
World Health Organization (WHO) basic emergency care course (BEC)
6
Advanced trauma life support (ATLS)
7
Advanced cardiac life support (ACLS)
8
Advanced life support in obstetrics (ALSO)
9
Pediatric advanced cardiac life support (PALS)
10
BEC, ATLS, and ACLS courses teach the approach to undifferentiated acutely ill or injured patients, positing that any emergency condition must ultimately pass through a phase of altered mental status, difficulty in breathing, shock, or trauma prior to death.6,7,8 Therefore, if providers in remote clinics are prepared from a procedural, human resources, and material (pharmacologic and non-pharmacologic) resource standpoint, then they will be able to respond to these undifferentiated conditions and maximize the patient's chances of surviving until transport to definitive care. ALSO was added to address obstetric emergencies that may be encountered in these settings.
9
PALS was considered for resuscitation of pediatric patients.
10
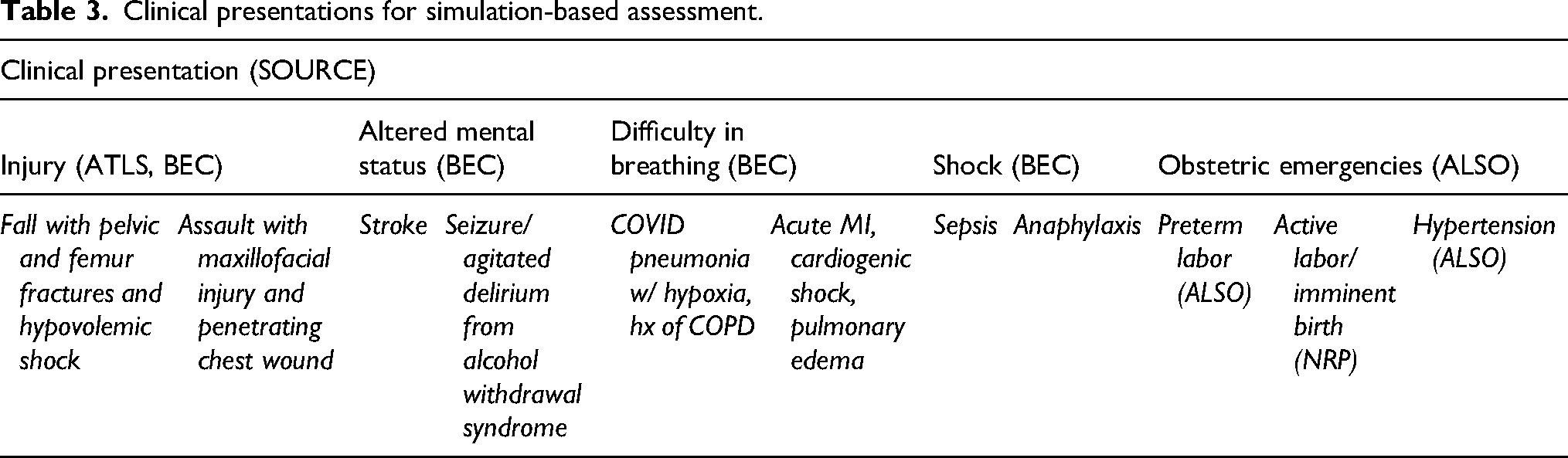
After placing the concepts taught by these courses as first-level categories and the undifferentiated conditions as second-level categories on this axis, we added a third level of “megacode” case equivalents. These are cases that, similar to an advanced cardiac life support megacode, were designed to incorporate multiple disease processes and physiologic responses into one clinical scenario for our assessment function. 8 Each undifferentiated condition (altered mental status, difficulty in breathing, shock, trauma) has between 1–2 megacode-style cases created to cover all of its content, and the obstetrics section is comprised of 3 cases. These cases were derived through author group expert opinion and were modified throughout the development phase within this cohort to best cover the content delivered by each corresponding undifferentiated condition. Brief descriptions of this axis are shown in Table 3.
Clinical presentations for simulation-based assessment.
These two axes were then combined to create the assessment tool matrix (see Appendix 1 for a large format table). The assessment was administered in case-based simulation format, as described in the upcoming Measurements section. Each cell represents the intersection of a facility function and a megacode-style case, answering questions such as: “To what extent can this facility perform the Airway component of the primary survey (and response) in patients with difficulty in breathing from an acute myocardial infarction with subsequent cardiogenic shock and pulmonary edema?” “To what extent can this facility perform staff safety, infection prevention, and control in patients with agitated delirium that ultimately evolves into seizure?”
The assessment was administered via a series of case-based simulations in which staff were gathered in the high-acuity room and each case was run as if the patient was on the gurney. Staff were asked to physically go through every procedure, find and place every material resource on the bed, demonstrate their ability to use each, and verify that its location was not restrictive. The assessment team created a structured data collection tool that was a series of “assessment sheets,” one for each clinical scenario, and had a row for each facility function, a column describing the details of the case, and the findings or physiologic response as it progressed. It also contained checkboxes that could be used to note the presence or absence of items associated with each function, and for notes to be taken on whether or not it was relocated, reorganized, or restocked due to expiry. Table 4 is an example of a completed assessment sheet.
Example sim case: Injury.
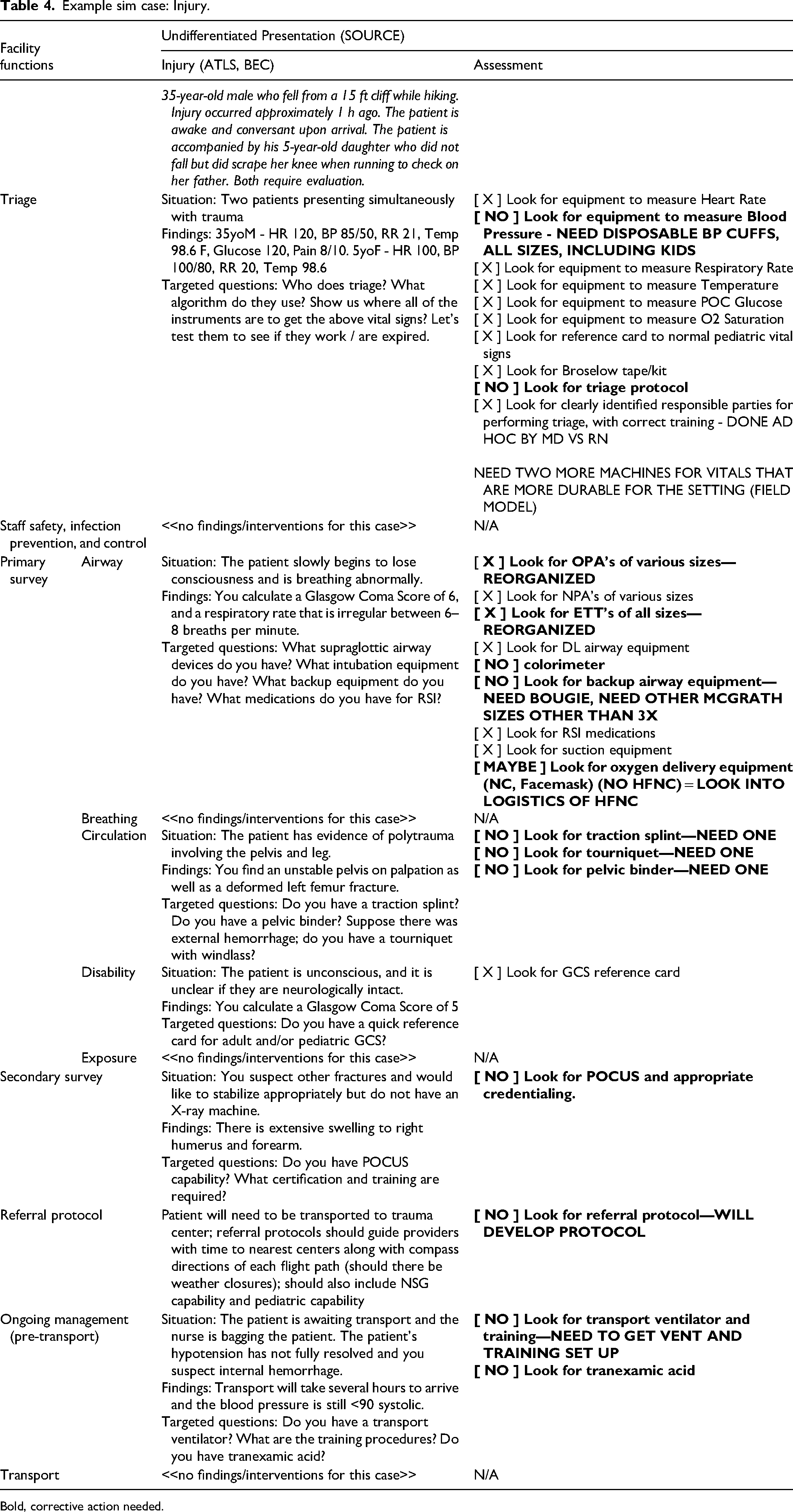
Bold, corrective action needed.
The scenarios were completed, and data from these assessment sheets were then used to create a report. The report was split into four areas of gap identification:
Procedural (eg, protocols such as triage, outside referral, and isolation). Human resources (both the presence and training levels/certifications of physicians, nurses, etc). Non-pharmacologic material resources. Pharmacologic material resources.
The report first described the findings in each area at a high level, followed by a spreadsheet that listed every deficiency, the rationale behind its need, space for assigning a responsible staff member, space for assigning a target date, and checkboxes to denote completion. This report was sent to facility leadership, who would periodically send it back to regional leadership to review each deficiency until all had been addressed.
Results
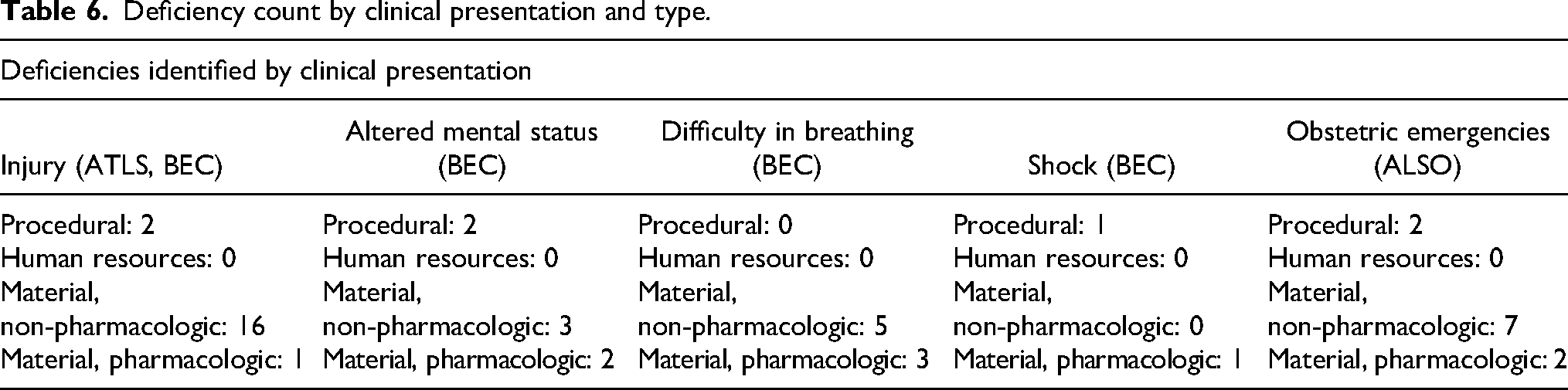
We found 48 total deficiencies as a result of our assessment. There were 7 procedural deficiencies, 1 human resources deficiency, 31 non-pharmacologic material deficiencies, and 9 pharmacologic material deficiencies. First, we aggregated deficiencies by facility function to gain a better understanding of our capacity to perform each. Table 5 shows this aggregation. We also aggregated deficiencies by clinical presentation to identify targets for educational interventions with the rationale that even if the deficiencies were chiefly material resources, providers had heretofore been unable to practice their use in this setting and thus might benefit from additional clinical training for these presentations after the items necessary to manage them were procured. Table 6 shows this aggregation.
Deficiency counts by function and type.
Deficiency count by clinical presentation and type.
Discussion
We have successfully created a novel emergency care capacity assessment tool for use in remote, resource-limited settings. Facilities in these settings were often not designed with input from specialists in emergency care, because they may not have intended to deliver emergency care in their scope of service. However, patients present to these facilities for healthcare regardless of their level of acuity owing to their geographic isolation and lack of alternate facility options, and thus it is of critical importance that these facilities be prepared to perform the initial management of undifferentiated acutely ill and injured patients.
Our assessment tool was developed using well-established resources with broad international consensus from the World Health Organization and included the Emergency Care Systems Framework and the basic emergency care course. It also used similarly highly recognized training courses in advanced trauma life support and advanced life support in obstetrics. Our tool, therefore, benefits from the high-quality work done by these organizations and minimizes the creation of de novo, unvalidated content.
The pilot assessment found 48 deficiencies, with gaps noted across all categories we intended to assess. All of these deficiencies have since been addressed, and the clinic's capacity to deliver emergency care has been substantially increased. Specific instances in which procedures, personnel, or material resources were put into place as a result of this assessment include stabbings, dog bites, burns, fractures, and preterm delivery. Providers in our pilot clinic have reached out multiple times to update us on how a specific item procured through this assessment has directly prevented morbidity or mortality. Furthermore, the process of administering the assessment has also sparked a culture of improvement at the site. Both physicians and nurses have since performed significant reorganization of existing resources to facilitate swift care delivery and have asked for additional items recognized after the restructuring of their architecture of thought on how emergency care should be delivered. The assessment has also served as a teaching function.
Limitations
The findings from our pilot assessment are facility-specific and may not be applicable to other facilities. As such, we have not described any specific findings in detail, and we leave only the raw counts to demonstrate the utility of the assessment. The purpose of this study is to describe the development of a new assessment tool, describe its pilot implementation, and demonstrate via the results that it was successful in identifying gaps.
Another limitation is that while the tool is intended for use in highly specific settings (ie, those facilities that are geographically isolated where patients have no other options for healthcare and that were designed to serve as clinics, health posts, etc), it was only tested in one of these potential settings. Further work could include testing this tool in additional clinical settings to assess is application.
Finally, another limitation is in the materials used to identify the potential gaps. While well-known and validated concepts were used, we found that not every possible scenario could be tested to identify possible deficits. While this author group developed the tool to account for as many scenarios or medical emergencies as possible, there may be factors that were unable to be assessed thus would remain unrecognized as a deficit. Furthermore, the recommendations found by using a tool like this may not be feasible for implementation in a rural or austere patient care center due to barriers including cost, physical space, or even weight.
Conclusions
This assessment tool has potential to be useful in a variety of health facilities ranging from other remote Indian Health Service facilities in the United States to rural health posts in low- and middle-income countries. We hope that by publishing our development and implementation process, systems planners will be able to identify facilities within their purview that may benefit from this tool and similar assessments. If validated in additional clinic environments, there is a potential to improve clinic readiness for acutely ill patients.
Supplemental Material
sj-pdf-1-wem-10.1177_10806032241278982 - Supplemental material for Creation of an Emergency Care Capacity Assessment Tool for Facilities in Austere Environments
Supplemental material, sj-pdf-1-wem-10.1177_10806032241278982 for Creation of an Emergency Care Capacity Assessment Tool for Facilities in Austere Environments by Vijay Christopher Kannan, Geoff Comp and Stephanie Lareau in Wilderness & Environmental Medicine
Footnotes
Author Contribution(s)
VK led the study conceptualization and design, data acquisition, data analysis, and drafting and critical revision of the manuscript.
GC and SL assisted with study conceptualization and design and critical revision of the manuscript.
Data Sharing
The assessment tool, as well as the deidentified dataset for this investigation, are available upon request from the date of article publication by contacting Vijay Kannan, MD, MPH, at vijay.kannan@ihs.gov.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was funded directly by the Indian Health Service as an internal quality improvement effort.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.