
Abstract
Introduction
The Mars Interventional Tool Box (MITBO) technique, a simplified drainage procedure using point-of-care ultrasound, provides a versatile solution for use in resource-limited environments, such as space missions and remote terrestrial regions. This study aims to evaluate the safety and feasibility of the MITBO technique in a clinical setting.
Methods
We conducted a retrospective analysis of 111 patients who underwent ultrasound-guided abdominal drainage using the MITBO technique between August 2022 and February 2023. The study included patients with abdominal collections (eg, intra-abdominal abscesses, gallbladder infections) as well as retroperitoneal procedures such as nephrostomies. Fluoroscopic or CT-guided cases were excluded. Feasibility was determined by the successful placement of drains under ultrasound guidance alone. Safety was assessed by documenting complications.
Results
The overall technical success rate was 97%, with 3 cases of failure: 1 due to patient non-cooperation and 2 because of non-visualization of the collections. The complication rate was 4.5% (n = 5), all of which were minor. No major complications, such as hemorrhage or infection, were observed. Nephrostomies, accounting for 4% of the procedures, were performed exclusively by senior radiologists with 100% success.
Conclusion
The MITBO technique demonstrated high success rates and a low complication profile, consistent with previous reports on standard drainage techniques. The standardized procedure is a promising alternative in environments where advanced imaging is unavailable. However, the limited sample size, especially for complex cases, and the exclusive performance of nephrostomies by experienced operators suggest the need for further studies to generalize these findings.
Keywords
Introduction
Interventional radiology (IR) has transformed modern medicine, providing minimally invasive alternatives to traditional surgical procedures. Since the introduction of the Seldinger technique in the 1950s, 1 IR has continued to evolve, offering precision and reduced recovery times for a variety of conditions. However, as medical science advances, there is a growing need to adapt IR techniques for use in more extreme and resource-limited environments, such as space missions and remote terrestrial regions. 2
In recent years, space exploration has become a focal point for innovation in medicine. With planned missions to the Moon, Mars, and beyond, ensuring the health and safety of astronauts during long-duration spaceflights is a top priority. 3 The unique challenges of space, including microgravity and limited medical resources, require the development of versatile, lightweight, and easy-to-use medical tools.
The Mars Interventional Tool Box (MITBO) was developed to address these challenges. MITBO is a simplified drainage technique that can be performed using point-of-care ultrasound devices and minimal equipment. 4 This method is designed to be versatile, capable of addressing a range of conditions such as intra-abdominal collections and gallbladder infections, as well as retroperitoneal kidney obstructions, requiring percutaneous drainage. Moreover, its compact design makes it ideal for use in space missions, where every gram of payload is critical. The technique is structured into 3 standardized steps: (1) percutaneous puncture of the collection with a fine needle under ultrasound guidance, allowing confirmation of purulent content; (2) insertion of a flexible guidewire through the needle and removal of the needle; (3) progressive insertion of an introducer and placement of an 8.5 Fr drain over the guidewire.
Our goal with MITBO was not only to optimize and simplify classical drainage techniques that could be used in space but also to ensure that they could be easily adopted in resource-limited settings on Earth. In many developing countries, access to advanced medical imaging and specialized equipment is limited. By providing a cost-effective, portable, and easy-to-use alternative, MITBO has the potential to improve medical care in these regions.
This study aims to evaluate the safety and feasibility of the MITBO technique through a retrospective analysis of 111 patients treated at our institution. We seek to determine whether MITBO can be universally adopted in both terrestrial and extraterrestrial settings, offering a reliable solution for medical care in extreme environments.
Methods
Study Design and Population
This retrospective study was conducted at the University Hospital Center of Nîmes, France. The MITBO technique represents a simplification of a standard procedure of drainage and was introduced as part of a quality improvement process within routine care. All procedures were performed in accordance with institutional clinical criteria, and patients provided written informed consent for the drainage procedure. The study included all consecutive patients who underwent ultrasound-guided drainage using the MITBO technique between August 2022 and February 2023. The study protocol was approved by the local ethics committee (IRB number: 24.09.03).
Inclusion criteria were patients with fluid-filled targets identified via ultrasound: clearly visible on ultrasound, within 15 cm from the skin surface, and safe to approach with real-time ultrasound alone without bowel or vascular interposition. These targets could include intra-abdominal abscesses, gallbladder infections requiring percutaneous cholecystostomy, and liver abscesses, as well as retroperitoneal procedures such as nephrostomies. Patients for whom fluoroscopic or CT guidance was predetermined for drainage were excluded from the study. In the event of technical failure, conversion to CT-guided drainage was performed at the discretion of the operator. The decision-making process ensured that only cases with a high likelihood of success using ultrasound guidance alone were included.
A total of 111 patients were included in the study (Figure 1). Hemostasis management was ensured, with specific criteria including platelet count > 30 109/L, INR < 1.5. Only low-dose acetylsalicylic acid (75 mg/day) was tolerated. 5
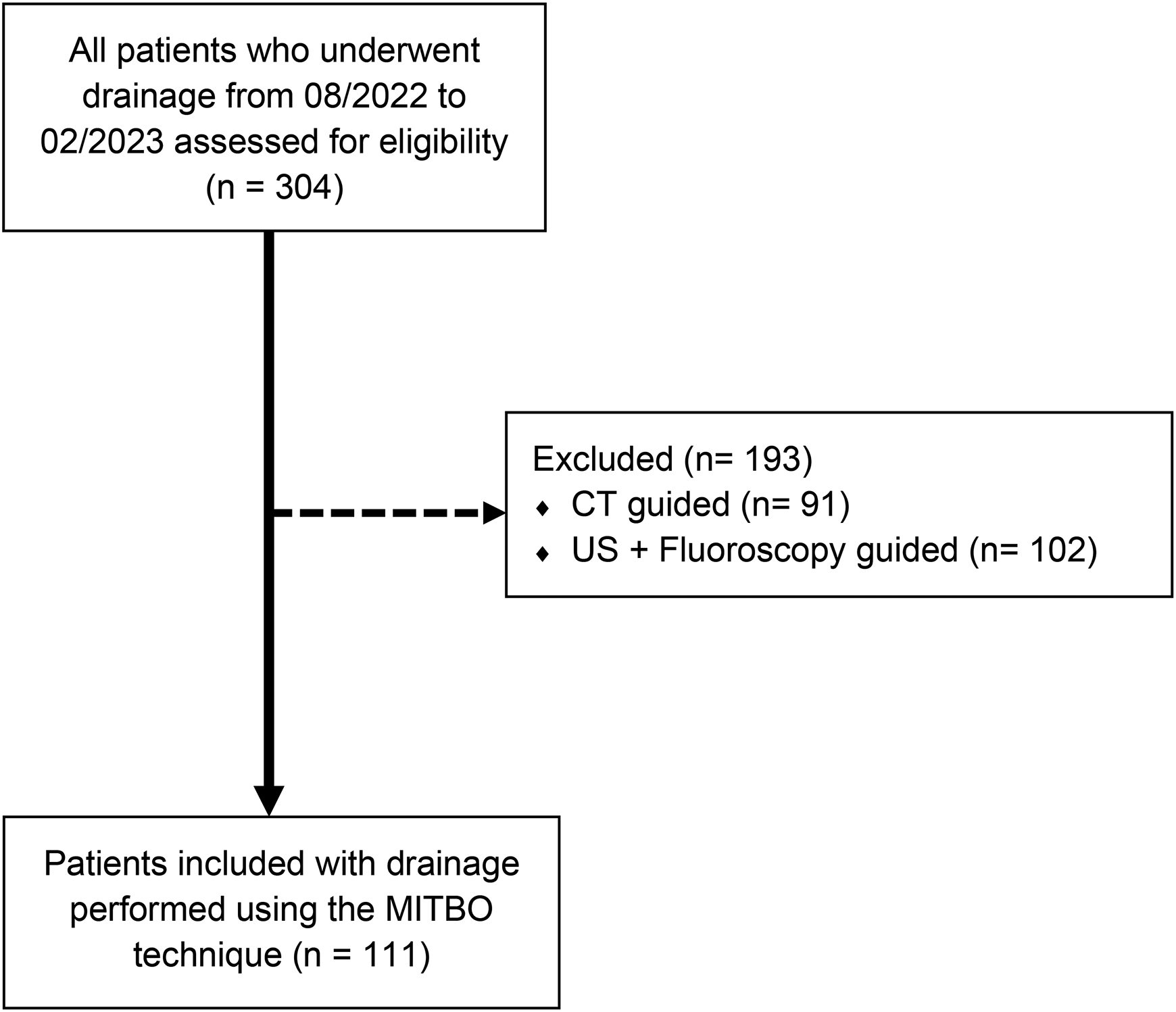
Consort flow diagram of the study.
Procedure
The MITBO technique was designed as a universal method for ultrasound-guided drainage with minimal equipment. The procedure was standardized and followed a step-by-step protocol to ensure consistency and reproducibility across operators with varying levels of experience. 4 The equipment included a point-of-care ultrasound machine (Viamo SV7 Canon Medical Systems Corporation, Otawara, Japan), local anesthesia, a One-Step coaxial needle (One-Step centesis catheters, Merit Medical Systems, Utah), an Amplatz guidewire (Amplatz Super Stiff guidewire, Boston Scientific, Massachusetts), and an 8,5 Fr drain (resolve drain, Merit Medical Systems, Utah).
The procedure began with ultrasound detection of the target collection. After sterilizing the area and administering local anesthesia, the One-Step coaxial needle was inserted into the collection under ultrasound guidance. Once the needle was in place, the guidewire was advanced, and the needle was removed. The drain was then prepared and inserted over the guidewire. The procedure concluded with the deployment of the drain, the attachment of a 3-way valve, and the fixation of the drain (Figure 2). No X-ray imaging was used for guidance.
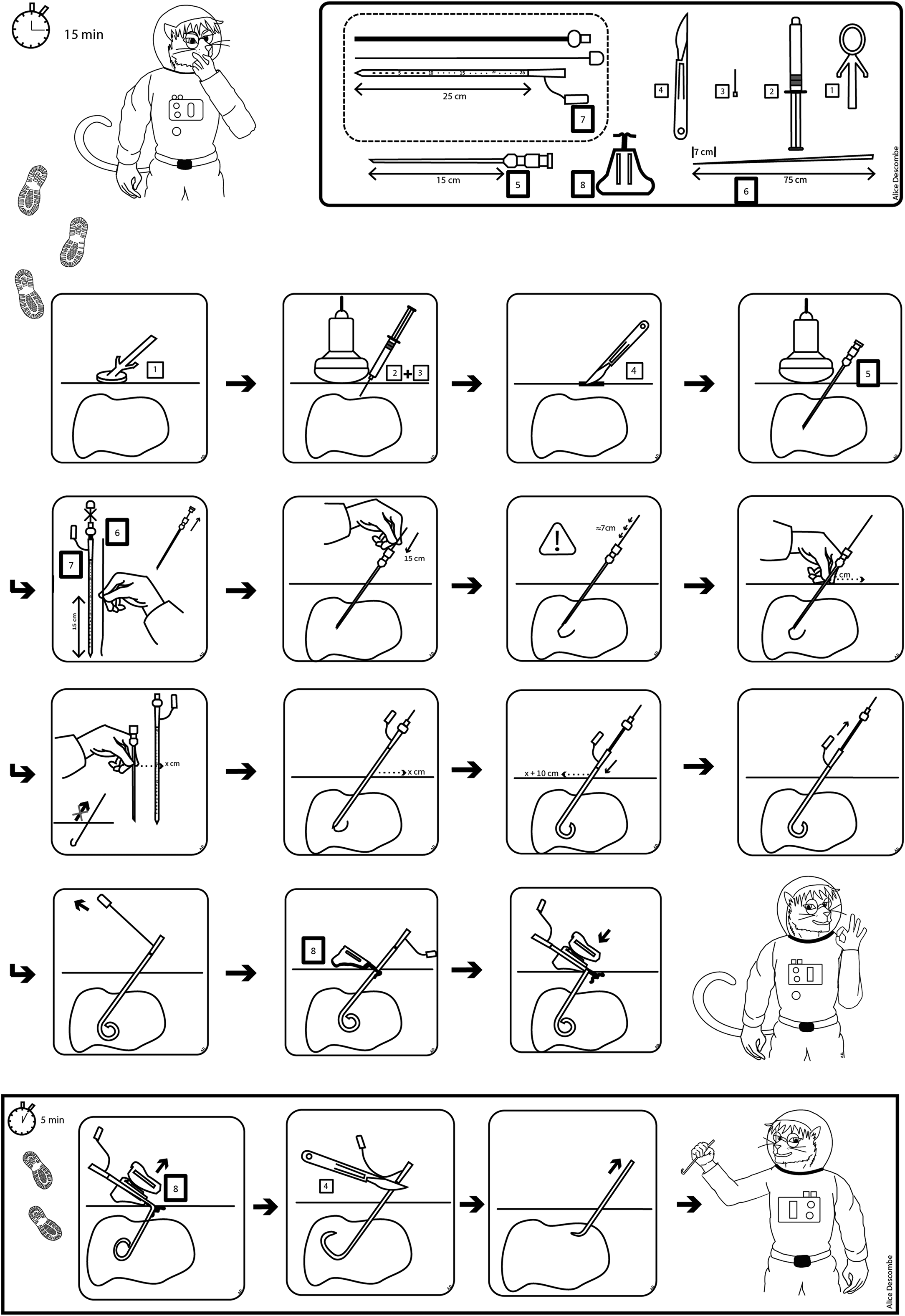
MITBO kit.
To ensure the effective implementation of the MITBO technique, we developed a comprehensive training program for junior radiologists, inspired by our previous work training analog astronauts for the Asclepios III mission. 4 This included (1) a theoretical session covering anatomy, indications, and complications; (2) an illustrated visual guide without text for universal comprehension (Figure 2); (3) a video tutorial demonstrating the technique (https://youtu.be/C7zZiw2f1eA); and (4) a hands-on practical session using a CAE Healthcare Blue Phantom (www.caebluephantom.com) simulating collections at various depths. Only after successfully completing this training under senior supervision were practitioners authorized to perform the procedure on patients.
Throughout the study, the technique was applied in various settings, including interventional radiology suites and bedside procedures in conventional hospital wards. This allowed us to assess the feasibility of the technique in different environments.
Feasibility Assessment
Feasibility was defined as the successful insertion of a drain into the target collection using ultrasound guidance alone, without the need for additional imaging. The technical success rate was recorded, along with the type of drainage performed (eg, intra-abdominal collections, gallbladder, liver abscesses, and retroperitoneal nephrostomy) and the operator's experience level:
-Junior: This group consisted of trainees with less than 4 years of experience in radiology and no prior experience in interventional radiology. -Intermediate: Trainees in this group had more than 4 years of radiology experience and had completed at least one 6-month rotation in interventional radiology. -Senior: This group included highly experienced trainees with over 6 years of radiology experience, including a minimum of 2 years in interventional radiology, as per the updated French radiology training curriculum.
6
To better understand the technique's adaptability, we compared the technical success rates of different operator levels and procedure types. This allowed us to determine whether the technique could be reliably performed by less experienced practitioners or in more complex cases.
Safety Assessment
Safety was evaluated by documenting any complications that occurred during or after the procedure. Complications of interest included significant bleeding (requiring more than manual compression), septic shock, embolic events, pneumothorax, and any other adverse events. These complications were classified according to the Society of Interventional Radiology (SIR) classification system. This standardized system allows for a consistent assessment of complications, ranging from minor events that require no or minimal therapy (classified as Grades A or B) to major complications that require significant intervention, result in prolonged hospitalization, or lead to permanent adverse sequelae or death (classified as Grades C to F). 7 We also recorded patient demographics, coagulation status, and follow-up data to identify potential risk factors for complications.
Follow-up was conducted by reviewing the electronic medical record and imaging within the hospital system. Clinical and imaging outcomes were monitored during the patient's hospital stay until hospital discharge. Additionally, medical records were rechecked at 6 months to identify any delayed complications or readmissions
Statistical Analysis
Quantitative variables are presented as mean, standard deviation (SD), minimum (min), and maximum (max) values and compared using either the Student's t-test or Mann-Whitney test, depending on their distribution. Qualitative variables are presented as frequencies and proportions, and comparisons are made using the Chi-squared test or Fisher's exact test if the validity conditions are not met. For comparisons involving more than 2 groups, the Kruskal-Wallis test was used. A result was considered significant if p < .05.
Results
Population Characteristics
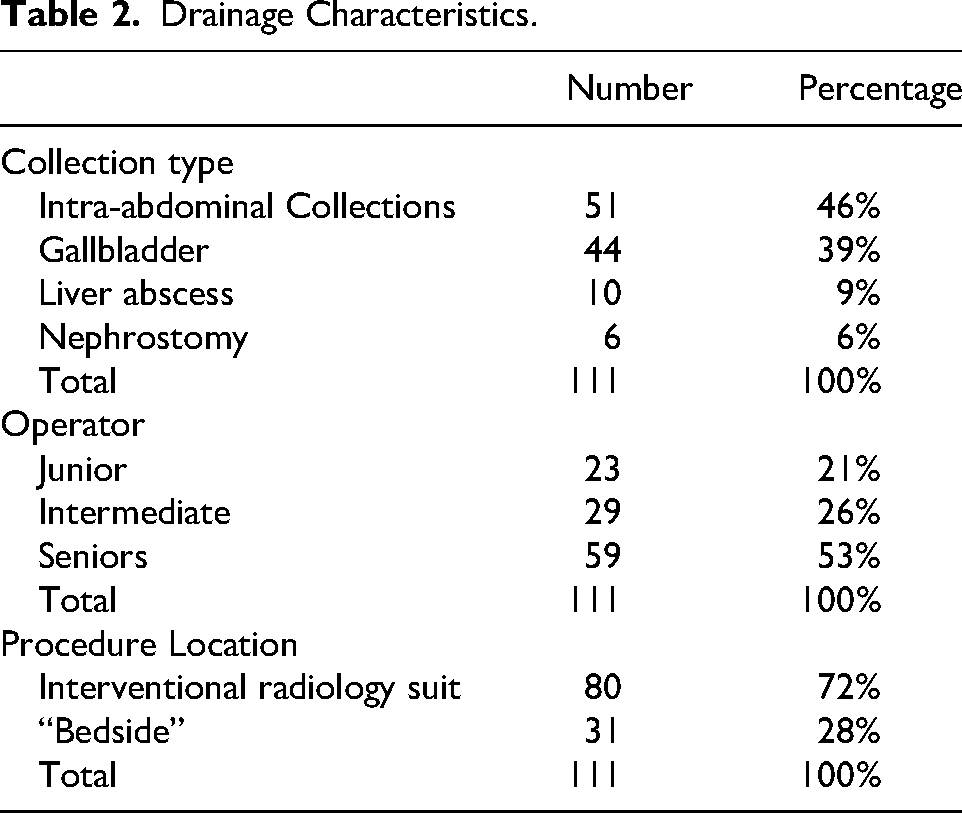
The study population included 111 patients with a mean age of 71 years and a mean BMI of 25.6 (Table 1). Twenty-two patients (19.8%) were on preventive aspirin at a dose of 75 mg, which was not discontinued. Three patients (2.7%) were on clopidogrel, which was discontinued 5 days prior to the procedure. Twenty-eight patients (25.2%) were on anticoagulants (enoxaparin, N = 12, 10.8%; apixaban, N = 9, 8.1%; warfarin, N = 5, 4.5%; other, N = 2, 1.8%), with discontinuation adapted according to the specific medication. The majority of patients presented with intra-abdominal collections (46%) and gallbladder drainage (39%). The distribution of operator experience levels was as follows: 21% of procedures were performed by junior radiologists, 26% by intermediate radiologists, and 53% by senior radiologists. Twenty-eight percent of the drainages were performed bedside, outside of a block environment (Table 2).
Patients’ Characteristics.
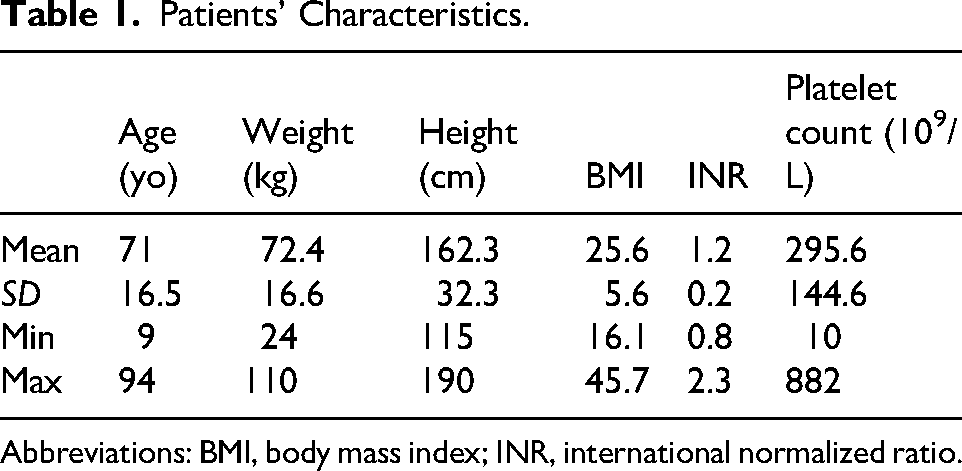
Abbreviations: BMI, body mass index; INR, international normalized ratio.
Drainage Characteristics.
Feasibility
The overall technical success rate was 97%, with 3 cases of failure: 1 for a gallbladder drainage performed bedside by a senior radiologist due to patient noncooperation (caused by patient agitation related to underlying cognitive impairment), and 2 abdominal collections in the interventional room, where the collections could not be visualized, requiring subsequent guidance by CT scan. These failures occurred in 1 case by a junior operator and 1 by a senior. The success rate did not significantly differ between operator experience levels (p = .65). Nephrostomy accounted for 4% (n = 6) of the total procedures, all of which were performed by senior radiologists with a 100% success rate.
Safety
A total of 5 complications (4.5%) were reported. The mean follow-up was 6 days (+/–7 days). Two drains were removed early due to poor tolerance (pain) in patients undergoing gallbladder drainage (minor complication, Grade B). Two patients required a drain change with the insertion of a larger drain, as the original drain was not productive (minor complication, Grade B). These were cases of abdominal collections with thick content. Additionally, 1 patient experienced a pneumothorax during a cholecystostomy, which did not require additional treatment and spontaneously resolved with the administration of level 1 analgesics (minor complication, Grade B). Of the 5 complications, 3 occurred with senior operators, 1 with a junior, and 1 with an intermediate, with no significant difference between groups (p = .62). No cases of infection, hemorrhage, or worsening of the condition were reported. The complications that did occur were managed effectively, and no long-term adverse effects were observed.
Discussion
Our study demonstrates that the MITBO technique is both safe and feasible for a wide range of drainage procedures. The high success rate and low complication rate suggest that this method is a viable alternative to traditional imaging-guided drainage techniques, particularly in settings where access to advanced medical imaging is limited. One of the key strengths of the MITBO technique is its adaptability. The fact that it can be performed by operators with varying levels of experience and in different environments makes it an attractive option for extreme environments, such as space missions and medically underserved regions. The standardized protocol and minimal equipment requirements further enhance its practicality.
There are 2 primary approaches to percutaneous drainage: direct puncture using a drain or the Seldinger technique, which involves an initial puncture with a fine needle followed by the insertion of a larger-caliber drain. We opted for the Seldinger technique in this study because it allows for the confirmation of purulent content with a fine-gauge needle before placing a larger drain. This approach is particularly advantageous in difficult punctures, as it offers greater control and safety during the procedure. 8 The use of the Seldinger technique resulted in a very low complication rate, under 5% and no major complications, which is lower than what has historically been reported in the literature. Prior studies have described complication rates ranging from 5% to 10%, including serious complications such as vascular injuries and mortality rates up to 5%.8,9,10 This low rate of complications can likely be attributed to the preselection of patients, most of whom had relatively accessible collections that could be easily visualized and drained under ultrasound guidance. Consequently, these cases may have been easier to manage and carried a lower risk of complications. Notably, our cohort did not include patients with more complex collections, such as those associated with digestive fistulas, which are known to carry a higher risk of complications. 9 Additionally, we did not encounter any hemorrhagic or septic complications, which are often described in drainage literature.10,11 This might be related to the minimally invasive nature of the approach used, further emphasizing the safety of the technique.
Percutaneous nephrostomy under 100% ultrasound guidance, without fluoroscopic assistance, has been described in the literature for pediatric populations, 12 but it's rarely performed in adults. This is largely due to the smaller body habitus of children, which makes them more amenable to ultrasound guidance. Our study demonstrates the feasibility of performing nephrostomies solely under ultrasound guidance in adults, offering a safe alternative to traditional methods. However, it is important to note that all of the nephrostomies in our study were performed by experienced operators, not by juniors. This highlights the need for a certain level of expertise to ensure the safety and success of the procedure. With the development of external guidance systems, such as computer-assisted stereoscopic ultrasound needle guidance, 13 it may be possible in the future to extend these techniques to less experienced operators, further expanding the accessibility and safety of ultrasound-guided nephrostomy in a broader range of clinical settings. These techniques could significantly alter current risk diagrams in aerospace medicine. At present, there are no viable options for managing complicated nephrolithiasis resistant to medical treatment during space missions. 3 The ability to perform percutaneous nephrostomy solely under ultrasound guidance could provide a critical solution to this problem, potentially reducing the risk of mission disruption or even crew life-threatening situations.
The literature is not conclusive regarding the optimal drain size for effective drainage, with recommendations ranging from 6 to 10 Fr.14,15 Studies have shown that increasing the drain size beyond 10 Fr does not necessarily result in better efficacy. For our study, we opted for an 8.5 Fr drain as a compromise, balancing sufficient drainage capacity with minimal invasiveness. This size proved effective for nearly all cases, with only 2 patients requiring an upgrade to a 10 Fr drain due to the initial drain being nonproductive. Additionally, by standardizing the use of the 8.5 Fr drain, we were able to limit the number of materials required, thus optimizing both weight and costs, key considerations in settings like space missions, where every gram counts.
While our study provides valuable insights into the safety and feasibility of the MITBO technique, several limitations must be acknowledged. One major limitation of our study is the potential for selection bias. All included patients underwent a preprocedural triage process in which only collections considered amenable to ultrasound-guided drainage were selected for the MITBO technique. This likely excludes more complex, deep, or poorly visualized collections for which CT or fluoroscopic guidance would be preferable. As a result, our findings primarily reflect outcomes in favorable anatomical scenarios and cannot be generalized to all drainage procedures. Furthermore, the sample size was relatively small, particularly for certain procedures like nephrostomy, limiting the generalizability of our findings. Additionally, the majority of the procedures were performed by senior operators, which may not reflect outcomes for less experienced practitioners. This raises questions about the broader applicability of the technique in settings where operator experience is limited. Another limitation is the age profile of our study population, which was older than the demographic typically expected in spaceflight or adventure tourism. However, this may provide useful insight into the upper age limit for the safe application of the technique. Finally, we did not conduct a long-term follow-up and thus cannot comment on late recurrence or complications beyond the immediate postprocedural period. Future prospective studies with predefined inclusion criteria and larger patient cohorts will be necessary to confirm the efficacy of the MITBO technique and validate its broader applicability. While our retrospective design allows for real-world observations, it does not permit strong conclusions about comparative effectiveness.
Although the procedures in this study were conducted by physicians—primarily interventional radiologists—the MITBO technique was developed with a high level of standardization to enable its transferability to other trained healthcare personnel in resource-limited settings. In the context of wilderness medicine or spaceflight, the technique could be performed by a physician or technician with appropriate training, potentially under real-time remote guidance using tele-ultrasound and the standardized visual guide.
Conclusion
The MITBO technique demonstrates a high success rate and low complication rate in our cohort of adult hospitalized patients, with most procedures performed by experienced radiologists and targeting collections deemed accessible by ultrasound. While promising, these results should be interpreted within the context of this selected population. With further validation, this method could play a crucial role in ensuring the safety and effectiveness of medical interventions in challenging environments.
Our study also highlights the potential for the MITBO technique to be adopted in a wide range of settings, from space missions to medically underserved regions on Earth. By reducing the complexity of medical procedures and minimizing the need for extensive medical equipment, MITBO could become a standard tool for medical care in extreme environments.
Footnotes
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.