
Abstract
Although sea snakes (Elapidae) are commonly encountered by fishermen, accurately authenticated envenomings by them are uncommon in clinical literature. We report an authenticated case of Shaw's short, or spine-bellied, sea snake (Hydrophis curtus) bite in a young fisherman from northern Sri Lanka. The patient had clinical and biochemical evidence of mild transient myotoxicity but no evidence of neuromuscular paralysis or significant renal injury. Consideration of the clinical manifestations suggests either a mild envenoming or a dry bite. The patient completely recovered without any antivenom therapy and was discharged on the fourth day. Prolonged observation may be beneficial to exclude complications of sea snake envenoming.
Introduction
Sea snakes are venomous elapids (subfamily: Hydrophiinae) found in the shallow coastal waters, estuaries, open ocean, and occasional inland lakes and rivers of tropical and subtropical regions of the Indian and Pacific oceans. 1 Although the venoms of some sea snakes are extensively studied, reported human cases of envenomings are relatively uncommon and have been reported from Malaysia, Sri Lanka, Thailand, and Australia, of which most are without species authentication.2–8 Most authenticated sea snake bites have been caused by the two beaked sea snakes, Hydrophis spiralis and Hydrophis zweifeli, in Southeast Asia and Australia, respectively. The most common cause of sea snake bites is the victim being bitten while attempting to remove a snake accidentally caught in the fishing net.2,4,5 Of the reported bites, only a small proportion of patients develop envenoming, 2 and the most common systemic effects of envenoming include myotoxicity of varying severity and its frequently associated manifestations, such as muscle weakness/paralysis and complications such as hyperkalemia and acute kidney injury.4,5,8 Australian sea snake antivenom (Sequirus Pty Ltd, Melbourne, Australia) raised against H. schistosus, which occurs in the Indian and Pacific oceans, is the only available antivenom for any sea snake envenoming due to its potential paraspecific neutralization. 9
Shaw's short sea snake (Hydrophis curtus) is a common sea snake in the Indian and Pacific oceans, inhabiting regional coastal habitats from the Indian subcontinent through Southeast Asia and Oceania. Although the venom of H. curtus and its neutralization by sea snake antivenom has been studied previously,9–11 clinical descriptions of authenticated envenomings are scarce. We report an authenticated case of a young man possibly developing mild myotoxicity following H. curtus envenoming in Sri Lanka.
Case Report
A 28-year-old male with no known significant past medical history was admitted to District General Hospital, Kilinochchi, a tertiary care center in Northern Sri Lanka, at 0230 h with a reported history of a sea snake bite that occurred 1 hour previously. The victim was a fisherman who had been removing fish from the fishing net on his docked boat on the shore; the snake was trapped in the net, and the patient reported being bitten in the foot. He had reported feeling pain at the bite site immediately after the bite and had applied a tourniquet proximal to the bite site with a rope, applied turmeric on the bite site, and presented to the hospital with the captured snake, which was later identified by a herpetologist (AS) as a juvenile specimen of Hydrophis curtus (Figure 1).

The juvenile H. curtus specimen (28.3 cm total length, sex undetermined) that caused the bite.
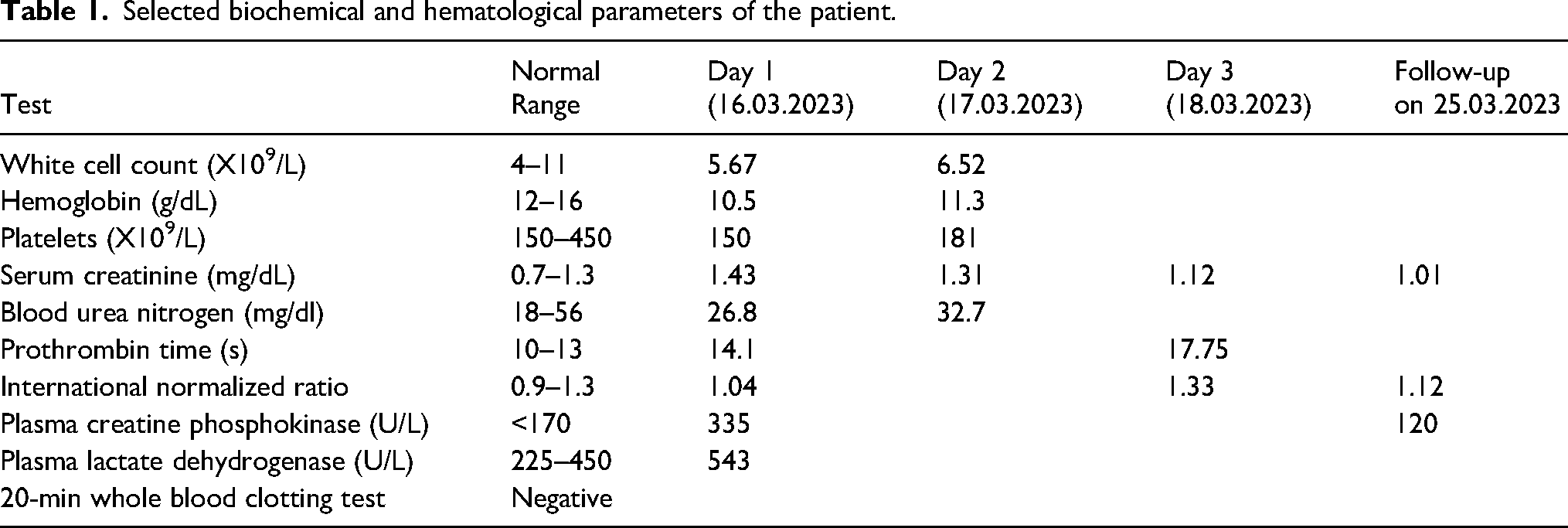
On admission, the patient was conscious and rational. There was a faintly visible bite mark on the fourth toe of the right foot. The fourth toe was mildly swollen and had mild pain at the bite site. The patient had no evidence of bleeding or features of neuromuscular paralysis, such as ptosis and ophthalmoplegia. Cardiac and respiratory examinations were unremarkable, with normal pulse rate (68 beats per minute), respiratory rate (16 breaths per minute), and blood pressure (128/84 mm Hg). The 20-min whole blood clotting test (WBCT20) on admission was negative, and the prothrombin time and international normalized ratio (INR) were normal on the first day (Table 1). An electrocardiogram (ECG) revealed sinus bradycardia. The patient was closely monitored for neurological symptoms and respiratory distress. The patient complained of generalized myalgia but did not pass dark-colored urine. The biochemical evaluation revealed mildly elevated plasma lactate dehydrogenase and creatine phosphokinase (CK) levels on the first day of envenoming, indicating mild myotoxicity. The patient did not receive any antivenom because of the unavailability of sea snake antivenom in Sri Lanka. His urine output was normal; however, his serum creatinine levels were elevated on the first day, which gradually became normal over the next couple of days. His low hemoglobin level and marginal platelet count on the first day had improved on the second day. Other biochemical and hematological parameters, as well as the complete urinalysis, were normal, apart from the marginally high prothrombin time and INR on the third day of the bite.
Selected biochemical and hematological parameters of the patient.
Hydration was maintained with intravenous normal saline and oral fluids at 2.5L and 2L per day, respectively. Pain management was achieved with 1 g of oral paracetamol, 3 times daily. The patient remained clinically stable with the resolution of myalgia and continued his routine activities. He was discharged on the fourth day of envenoming. Follow-up for review and repeated laboratory investigations occurred 1 week later. The serum creatinine, prothrombin time, INR, and CK levels were all within normal ranges. No adverse events were reported during the follow-up period.
Discussion
Although sea snakes are commonly encountered by fishermen, authenticated bites with accurate species identification are rarely reported in the literature. As highlighted in a recent case of a fatal sea snake envenoming, even when a snake specimen or a photograph is available for identification, it is of utmost importance to authenticate that it is the same specimen that has bitten the patient before its identity is authoritatively confirmed.12–14
H. curtus is a common species of sea snake in Sri Lanka, frequently collected from fishing nets of the northern, eastern, and southern coasts. 15 However, authenticated bites by this species are almost absent in the clinical literature. This report provides a documented example of a bite by a verified H. curtus that may have manifested only as mild myotoxicity and completely resolved spontaneously with no complications despite the unavailability of antivenom. Nonetheless, the possibility that the mild elevation of CK in our patient was a result of the tourniquet leading to local muscle damage or simply the exertion during fishing activities rather than a true venom effect, thus the possibility of this being a case of a dry bite, cannot be excluded.
The marginally low hemoglobin in our patient is unlikely to be related to the snakebite and is a common finding in our setting predominately due to iron deficiency anemia. The transient, marginally high INR and prothrombin time on the fifth day are unlikely to be related to the snakebite due to the timing, which is unlikely for a snakebite-triggered coagulopathy. In Sri Lanka, sea snake antivenom is not available, and the only snake antivenom available, the Indian polyvalent antivenom, is not indicated for sea snake envenomings. Therefore, the management of our patient was through supportive therapy. Since the circumstances of sea snake bites are mostly fishing activities, educating the fishermen on the safe removal of accidentally caught sea snakes would help minimize sea snake bites.
Footnotes
Author Contribution(s)
Consent
Written informed consent was obtained from the patient for publishing this case report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.