Blood-bellied coral snake (Calliophis haematoetron) is a recently discovered forest-dwelling species of elapid hitherto known from 3 specimens found from central Sri Lanka. Herein we describe the first authenticated case of blood-bellied coral snakebite. The victim, an 11-mo-old infant who received the bite while handling the snake at her home, had mild transient swelling at the bite site. The patient had no clinical or laboratory evidence of systemic envenoming. We highlight the importance of clinicians being aware of the occurrence of this potentially medically important elapid snake in anthropogenic habitats.
Sri Lanka records one of the highest snakebite incidence rates in the world, with an estimated 398 bites per 10,0000 population annually.1 There are >100 snake species in Sri Lanka. In terms of the number of bites and envenomings, the most medically important are Russell’s viper (Daboia russelii), Indian krait (Bungarus caeruleus), Common cobra (Naja naja), saw-scaled viper (Echis carinatus) and Merrem’s hump-nosed pit-viper (Hypnale hypnale).2 However, bites by some potentially medically important snakes in Sri Lanka have yet to be formally documented.
Asian coral snakes (genus Calliophis) belong to the family Elapidae, which includes many snakes of high medical importance such as kraits, cobras, sea snakes, and several Australian species such as brown snakes (Pseudonaja sp.) and the tiger snake (Notechis scutatus). Two species of coral snakes are currently recorded from Sri Lanka. The widely distributed slender coral snake (Calliophis melenarus [Show, 1802]) is found in the lowlands of Sri Lanka, India, and Bangladesh.3 The recently described blood-bellied coral snake (Calliophis haematoetron [Smith, Manamendra-Arachchi and Somaweera, 2008]) is currently known from 3 specimens from central Sri Lanka and considered endemic in Sri Lanka.4 So far, bites by C haematoetron have not been reported. Thus, its medical importance was unknown. Here we present the first authenticated case of an adult blood-bellied coral snakebite that caused only mild local envenoming.
Case report
An 11-mo-old female infant presented to the District General Hospital, Matale, of the central province of Sri Lanka with a snakebite that occurred 25 min before presentation. The mother had witnessed the infant holding a small snake with both hands, on the floor of the kitchen of their house (location: 07°57’N, 80°58’E; Yatawatta, Matale, central Sri Lanka). She had noticed a small drop of blood over the lateral side of the base of the index finger of the left hand and swelling and redness over the back of the same hand. The mother had washed the 2 bite sites and noticed redness and mild swelling around both sites. The swelling over the index finger had gradually subsided after about 10 min, and the infant was fine otherwise, according to the mother. The photographs of the dead snake specimen brought with the patient were immediately sent to a herpetologist (AS) who identified the specimen as an adult blood-bellied coral snake (Calliophis haematoetron) (Figure 1).
Blood-bellied coral snake (Calliophis haematoetron) specimen (total length, 30.0 cm; snout–vent length, 27.2 cm) that had bitten the patient. (A) Fresh specimen (before preservation) showing bright red over the subcostal scales and blue and black speckled appearance over the subcaudal scales. (B) Preserved specimen. (C) Dorsum of the head (head length: 0.8 cm).
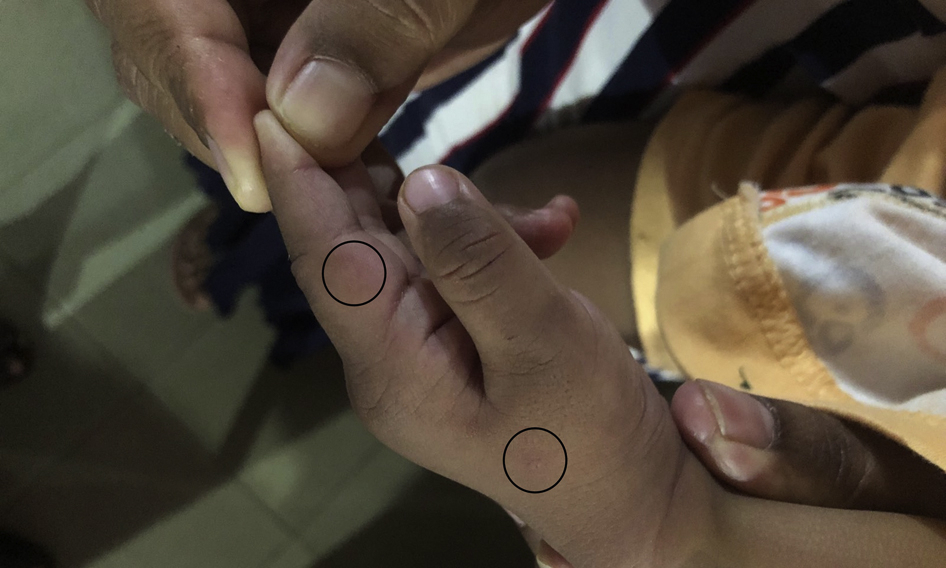
On admission, the infant was alert, was active, and had no signs of neuromuscular paralysis such as ptosis, ophthalmoplegia, or respiratory distress. Her heart rate was 120 beats·min-1, blood pressure was 100/60 mm Hg, and respiratory rate was 32 breaths·min-1. Mild swelling and redness were noted around a possible bite site over the dorsum of the hand near the metacarpophalangeal joint of the thumb (Figure 2); however, no local reaction was observed around the site on the index finger, where the mother had observed a blood drop. On admission, the patient’s 20-min whole clotting test was negative; her prothrombin time, international normalized ratio, and activated partial thromboplastin time were 12.8, 0.98, and 32.5 s, respectively. Her respective white cell count, red cell count, and platelet count were 10.38×103·mL-1, 4.87×106·mL-1, and 341×103·mL-1. The differential white cell count showed lymphocytes at 65% and neutrophils at 26%. Her serum creatinine levels, liver enzyme levels, serum Na+ and K+ levels, and electrocardiogram were normal. The patient was closely monitored for the next 6 h, but no signs of envenoming were observed. The 20-min whole clotting test done on the following morning was normal. The patient was kept under observation and was discharged on day 3. The patient was normal and healthy when followed up 2 wk after discharge.
The 2 sites of bites (encircled) over the infant’s left hand.
Discussion
Herein we describe an authenticated bite by an adult blood-bellied coral snake that resulted in no clinically detectable systemic envenoming. A literature search found no published reports of authenticated bites by this snake; hence, this could be the first authenticated case of a bite by this snake. The infant had 2 bite sites, of which 1 had bleeding and transient mild local swelling. The presence of numbness and pain at the bite site cannot be excluded because the infant was unable to explain her symptoms. The absence of any clinically detectable neurotoxicity, normal white cell counts, normal coagulation, and renal and liver profiles suggests the absence of systemic envenoming in the victim.
Although bites by Asian coral snakes (genus: Calliophis) are comparatively rare, they are proteroglyphous and possess venom glands similar to other medically important Asiatic elapid groups such as kraits (genus: Bungarus) and cobras (genus: Naja).5,6 The venom glands of both species of coral snakes inhabiting Sri Lanka are confined to the head, in contrast to some of their Southeast Asian congeners such as C bivirgata and C intestinalis, which have venom glands that extend beyond the head, along the body.5,6 The composition of the venom of C melenarus and C haematoetron has yet to be studied. However, based on the venom proteomes of C bivirgata flaviceps and C intestinalis, it could be assumed that the venom of C melenarus and C haematoetron are likely to contain phospholipases A2, snake venom metalloproteinases, and 3-finger toxin groups such as alpha neurotoxins and cardiotoxins.5,7-9 The reported bites by C melenarus in Sri Lanka and India resulted in pain and swelling at the bite site and regional lymphadenopathy.10,11 Features of systemic envenoming such as paralysis have not been reported in C melenarus bites.
Based on recorded specimens, both the C melenarus and C haematoetron appear to be relatively small snakes compared to their Southeast Asian congeners. The 3 specimens from which C haematoetron is known were measured as 15.2 to 41.4 cm,4 which suggests that the present specimen is an adult snake. Because of the smaller body size, proportionately smaller mouth, and shorter fangs, piercing of thicker-skinned areas of adult humans such as the lower limbs would be difficult for an adult C haematoetron. Even if piercing of the skin were achieved during the bite, the dose of venom injected may not be sufficient to cause systemic envenoming, as in this case.
C haematoetron has previously been reported as exclusively a forest-dwelling species. Of the 3 known specimens of C haematoetron, the 2 paratypes collected in 1944 originated from a tropical moist semi-evergreen forest (currently no forest cover); the holotype was collected in 1997 from Wasgomuwa National Park, where tropical dry (mixed) evergreen forest exists.4 In contrast, the present report suggests the existence of C haematoetron in anthropogenic habitats, suggesting a wider range of habitat. The snake is somewhat difficult to locate when moving among the leaf litter. When disturbed, it displays bright red coloration over the ventral scales and blue coloration over the subcaudal scales, probably as a warning behavior.4 In this case, it could be assumed that the snake crept into the kitchen of the house, and the infant was attracted to the snake due to its coloration, which led to the infant picking up the snake and the subsequent bite.
Conclusions
This infant, who was bitten by an adult blood-bellied coral snake while handling the snake, had mild transient swelling at the bite site, without clinical or laboratory evidence of systemic envenoming. Clinicians must be aware of the possible occurrence of this potentially medically important elapid snake in anthropogenic habitats.
Footnotes
Acknowledgements
Author Contributions: Managing the patient and collection of data (SJ, NR, AM, KP); identification of the snake and drafting the manuscript (AS). All authors approved the final version of the manuscript.
Financial/Material Support: None.
Disclosures: None.
References
1.
EdiriweeraD.S.KasturiratneA.PathmeswaranA.GunawardenaN.K.WijayawickramaB.A.JayamanneS.F.et al.Mapping the risk of snakebite in Sri Lanka - A national survey with geospatial analysis. PLoS Negl Trop Dis2016; 10(7)e0004813.
2.
KasturiratneA.PathmeswaranA.FonsekaM.M.D.LallooD.G.BrookerS.de SilvaH.J.Estimates of disease burden due to land-snakebite in Sri Lankan hospitals. Southeast Asian J Trop Med Public Health2005; 36(3), 733–740.
3.
SeetharamarajuM.GandlaC.K.SrinivasuluC.Notes on the rare slender coral snake Calliophis melanurus (Shaw, 1802) (Serpentes: Elapidae: Calliophinae) from Telangana state, India. Sauria2019; 41(2), 50–54.
4.
SmithE.N.Manamendra-ArachchiK.SomaweeraR.A new species of coralsnake of the genus Calliophis (Squamata: Elapidae) from the central province of Sri Lanka. Zootaxa2008; 1847(1), 19–33.
5.
SlowinskiJ.B.BoundyJ.LawsonR.The phylogenetic relationships of Asian coral snakes (Elapidae: Calliophis and Maticora) based on morphological and molecular characters. Herpetologica2001; 57(2), 233–245.
6.
ZaherH.MurphyR.W.ArredondoJ.C.GraboskiR.Machado-FilhoP.R.MahlowK.et al.Large-scale molecular phylogeny, morphology, divergence-time estimation, and the fossil record of advanced caenophidian snakes (Squamata: Serpentes). PLoS One2019; 14(5)e0216148.
7.
TanC.H.FungS.Y.YapM.K.K.LeongP.K.LiewJ.L.TanN.H.Unveiling the elusive and exotic: venomics of the Malayan blue coral snake (Calliophis bivirgata flaviceps). J Proteomics2016; 132, 1–12.
8.
YangD.C.DeuisJ.R.DashevskyD.DobsonJ.JacksonT.N.W.BrustA.et al.The snake with the scorpion’s sting: novel three-finger toxin sodium channel activators from the venom of the long-glanded blue coral snake (Calliophis bivirgatus). Toxins (Basel)2016; 8(10), 303.
9.
TanK.Y.LiewJ.L.TanN.H.QuahE.S.H.IsmailA.K.TanC.H.Unlocking the secrets of banded coral snake (Calliophis intestinalis, Malaysia): a venom with proteome novelty, low toxicity and distinct antigenicity. J Proteomics2019; 192, 246–257.
10.
de SilvaA.Calliopis melanurus singheleus bite – first record. Proc Kandy Soc Med1990; 12, 16–18.
11.
MirzaZ.PalS.Notes on the effects of a bite from Calliophis melanarus Shaw 1802 (Serpents: elapidae: Calliophinae). Reptil Rap2010; 9, 7–8.