
Abstract
Introduction
Crossbow injuries are rare but carry significant morbidity and mortality, and there is limited evidence in the medical literature to guide care. This paper reviews the case reports and case series of crossbow injuries and looks for trends regarding morbidity and mortality based on the type of arrow, anatomic location of injury, and intent of injury.
Methods
Multiple databases were searched for cases of crossbow injuries and data were abstracted into a spreadsheet. Statistics were done in SPSS.
Results
358 manuscripts were returned in the search. After deduplication and removal of nonclinical articles, 101 manuscripts remained. Seventy-one articles describing 90 incidents met the inclusion criteria. The mean age was 36.5 years. There were 10 female and 79 male victims. Fatality was 36% for injuries by field tip arrows and 71% for broadhead arrows, p = .024. Assaults were fatal in 84% of cases, suicides in 29%, and accidental injuries in 17%, p < .001. Mortality was similar for wounds to the head and neck (41%), chest (42%), abdomen (33%), extremities (50%), and multiple regions, p = .618.
Conclusions
Crossbows are potentially lethal weapons sold with fewer restrictions than firearms. Injuries caused by broadhead arrows are more likely to be fatal than injuries from field tip arrows. The anatomic location of injury does not correlate with fatality. More than half of crossbow injuries are due to attempted suicide, with a high case-fatality rate.
Introduction
Crossbow injuries are rarely encountered in clinical practice but may result from hunting incidents as well as assaults or attempted suicide. A prior review of 38 crossbow fatalities determined that the head and thorax are the most common sites of fatal injury and that homicides outnumber completed suicide and accidental injuries. 1 However, a more complete picture of the spectrum of injuries would include information on less severe injuries. In the United States, the National Electronic Injury Surveillance System estimates an average of 4216 injuries related to archery equipment annually from 2017–2021, with no fatalities reported during that period. 2
This study collates the multiple case reports and case series of fatal and nonfatal crossbow injuries, summarizes the epidemiology of injuries, and looks for trends in mortality based on the type of arrow, anatomic location of injury, and intent of injury. We then review the pathophysiology of crossbow injuries and discuss prehospital management.
Methods
A medical librarian completed searches in PubMed, Ovid MEDLINE, Scopus, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases. The PubMed search was a basic keyword search of the term crossbow. The Ovid MEDLINE, Scopus, and CINAHL searches were performed on October 18, 2021, with terms for crossbow, “cross bow,” recurve, arrow, compound, and archery, using adjacency searching and combined with injury, wound, and trauma variations. A total of 357 abstracts were found. EndNote was used to identify duplicates in the searches, and 85 duplicates were removed during this initial screening.
The remaining manuscripts were then compared against the inclusion criteria and screened for eligibility. Inclusion criteria were injuries resulting from a missile fired by a crossbow with available outcome data. Manuscripts that did not meet the criteria, such as injuries from the crossbow mechanism and injuries from other types of bows, were excluded. Demographic data, type of arrow, anatomic site injured, presence of drugs or alcohol, and intent were abstracted if included. The data were then organized and sorted by gender, country, age, anatomic injury, reported drugs/alcohol, intent, and outcome (fatality vs nonfatal injury). The search was updated on February 10, 2022, with one additional manuscript found that met the inclusion criteria. In addition, we added a published case seen from our institution that was not found using the previous search strategy (Figure 1).
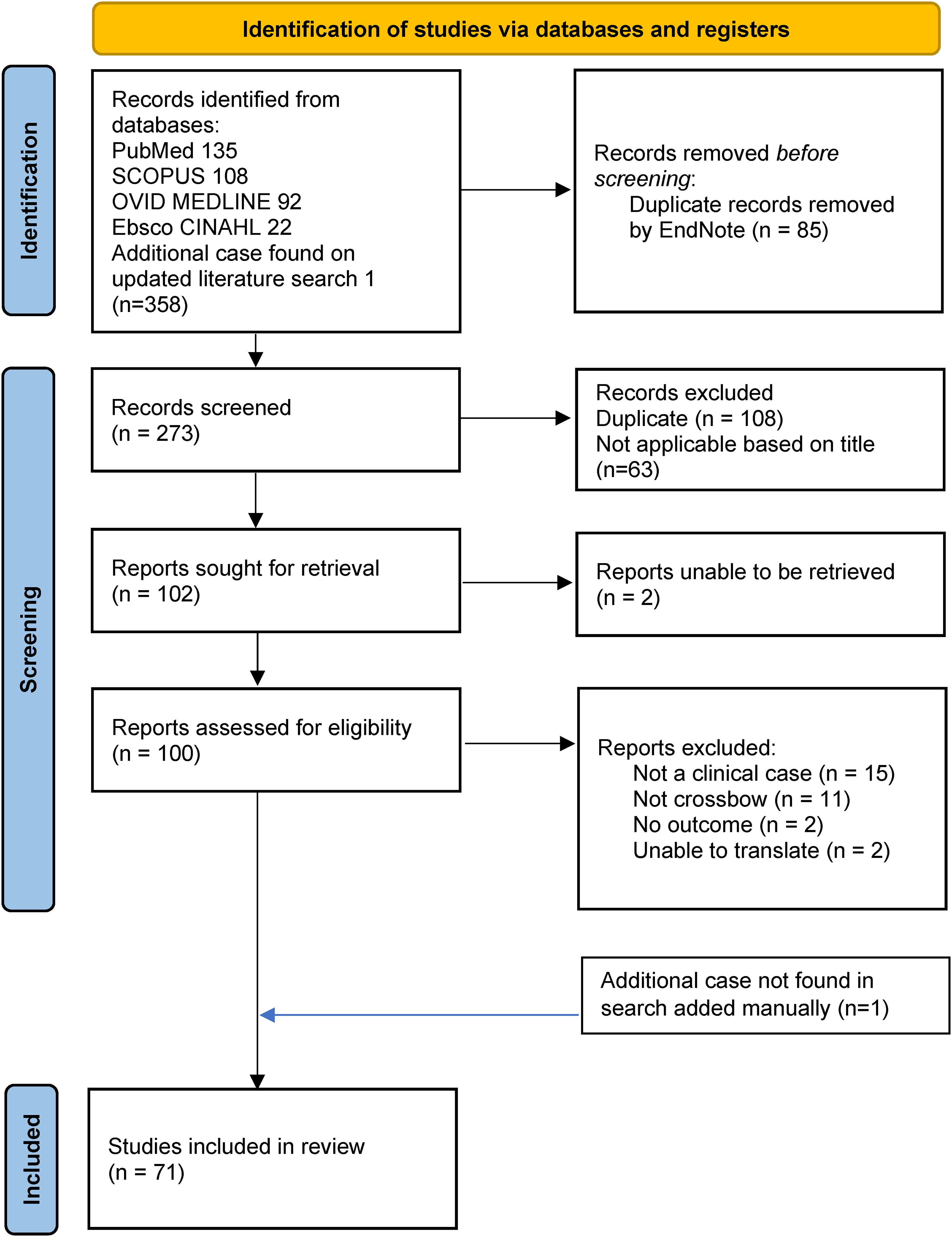
PRISMA 2020 flow diagram for new systematic reviews that included searches of databases and registers only. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. DOI: 10.1136/bmj.n71
Statistical analysis was completed using IBM SPSS, version 28. Chi-squared tests were used to assess significant predictors of fatality and effect size. A standard adjusted binary logistic regression was used to model the binary variable of fatality based on predictor variables. Predictor variables were the type of arrow and intent of injury.
Results
A total of 358 manuscripts were returned in the search. After deduplication and removal of nonclinical articles based on the title, 101 manuscripts remained. Seventy-one articles describing 90 cases met the inclusion criteria of wounds caused by arrows fired from a crossbow with information on patient outcomes. Cases came from a total of 18 countries; the first case was published in 1973, and cases continued into 2022 (Table 1).
The studies included from the search and the data extracted from each.
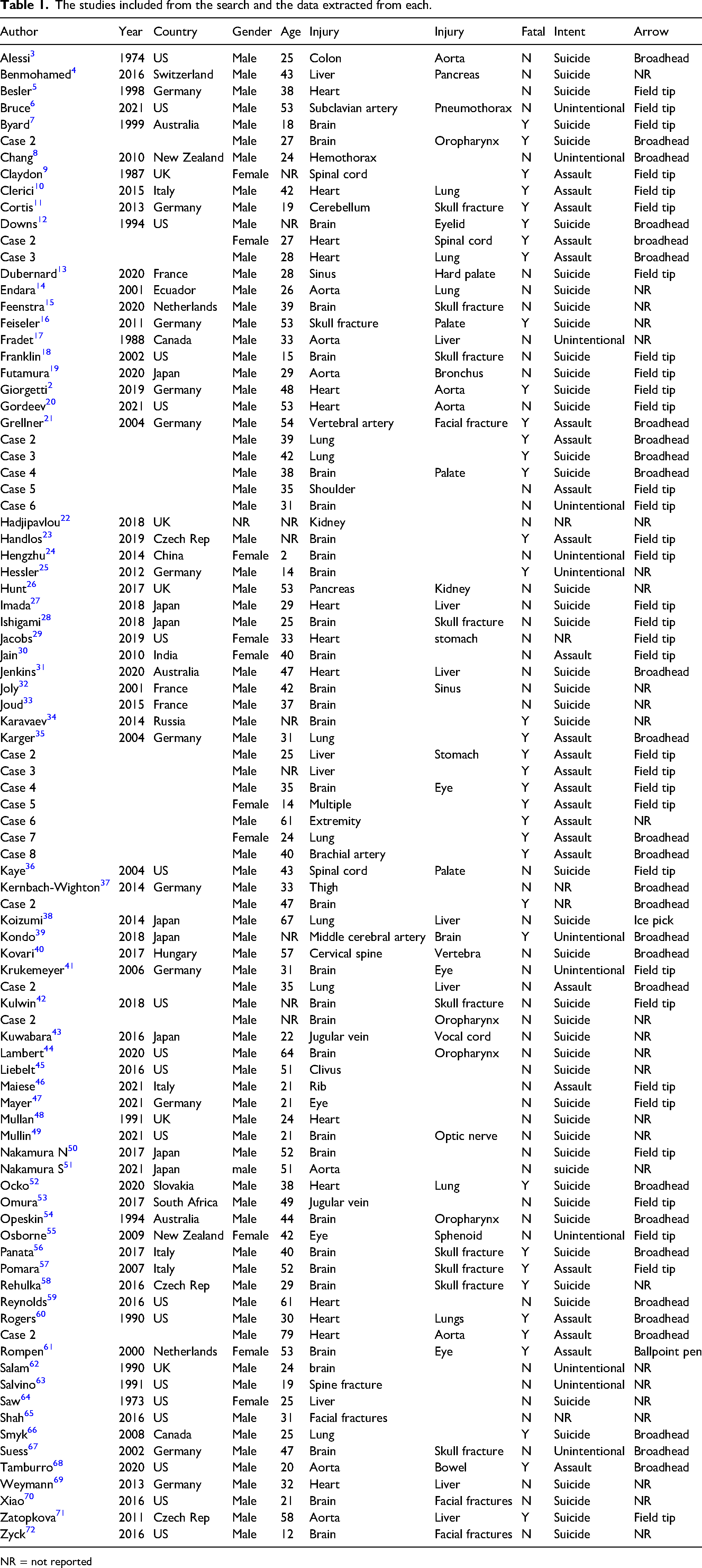
NR = not reported
The mean (SD) age was 36.5 (14.5) years. There were 10 female (11%) and 79 male (89%) victims with gender not reported for 1 (1.1%) case. Field tip arrows accounted for 37% of injuries, broadhead arrows for 31%, and the type of arrow was not described for 30% of cases. Most injuries occurred to the head and neck (53%), followed by the chest (31%), abdomen (8%) and extremities (4%). Multiple injuries were uncommon (2%). Injuries were due to attempted suicide in 48 cases (53%), assault in 25 cases (28%), and unintentional in 12 cases (13%), with no intent reported in 5 cases (6%). Two females and 1 male were victims of intimate partner violence. Crossbow injuries were fatal in 38/90 (42.2%) of cases (Table 2).
Demographics of patients and statistical breakdown of each injury in the cases reported in each included study.
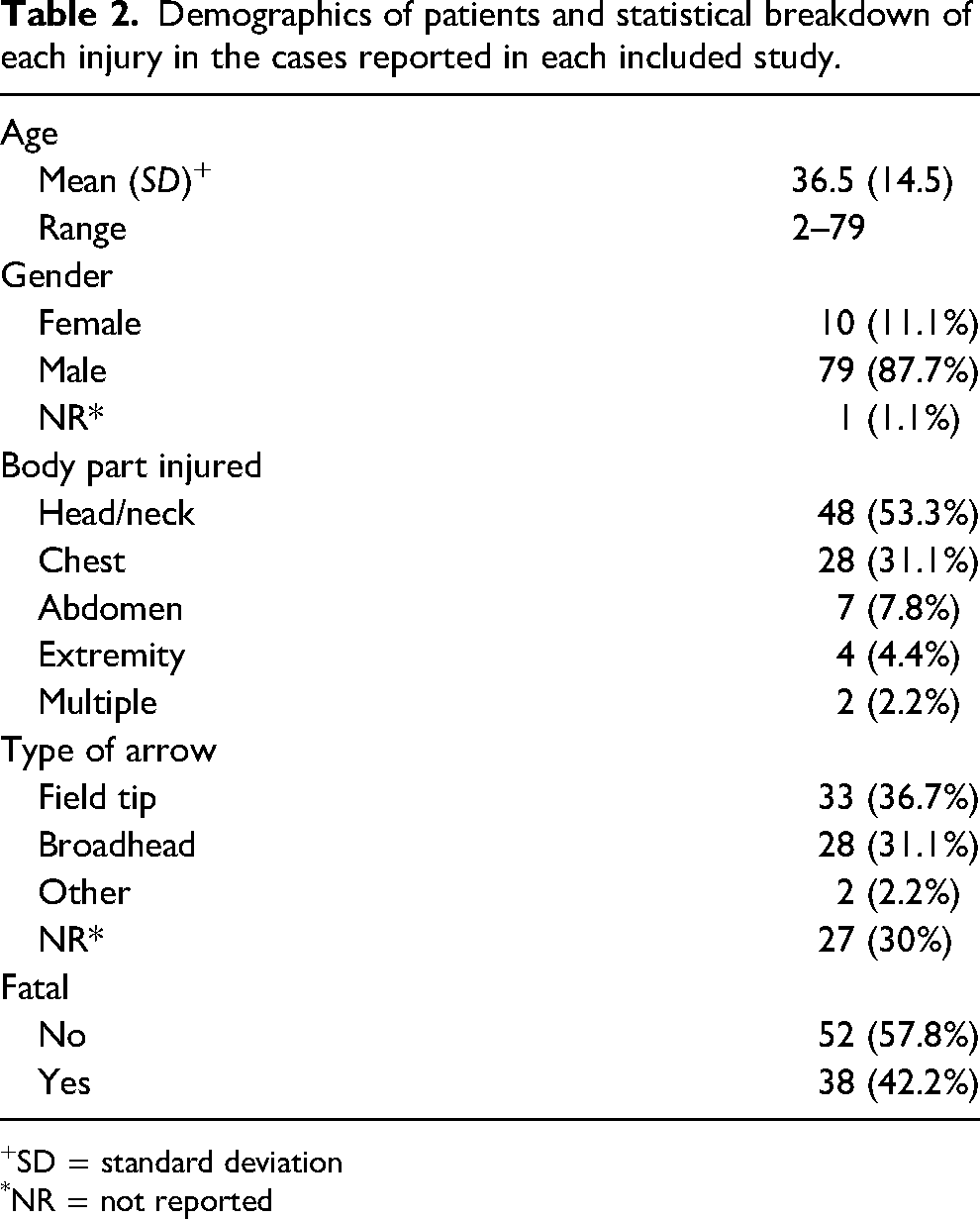
SD = standard deviation
*NR = not reported
The type of arrow and intent of injury were independent predictors of fatality. Injuries by field tip arrows were fatal in 12/33 cases (36.4%), broadhead arrows in 20/28 cases (71.4%), and other projectiles in 1/2 cases (50%), Χ2 (2) = 7.471, p = .024. The type of arrow was not reported in 27 cases (30%). Unintentional injuries were fatal in 2/12 cases (16.6%), assaults in 21/25 cases (84%), and suicides in 14/48 cases (29.2%), Χ2 (2) = 24.209, p < .001. The intent was not reported for 5 cases (5.6%). Mortality was similar for wounds to the head and neck (41.3%, n = 46), chest (42.3%, n = 29), abdomen (33%, n = 6), extremity (50%, n = 4), and multiple locations (100%, n = 2), Χ2 (4) = 3.021, p = .618.
Results of the logistic analysis indicated that the two-predictor model provided a statistically significant prediction of fatality, model Χ2, p < .001. The Nagelkerke pseudo Rsq indicated that the model accounted for approximately 48% of the total variance.
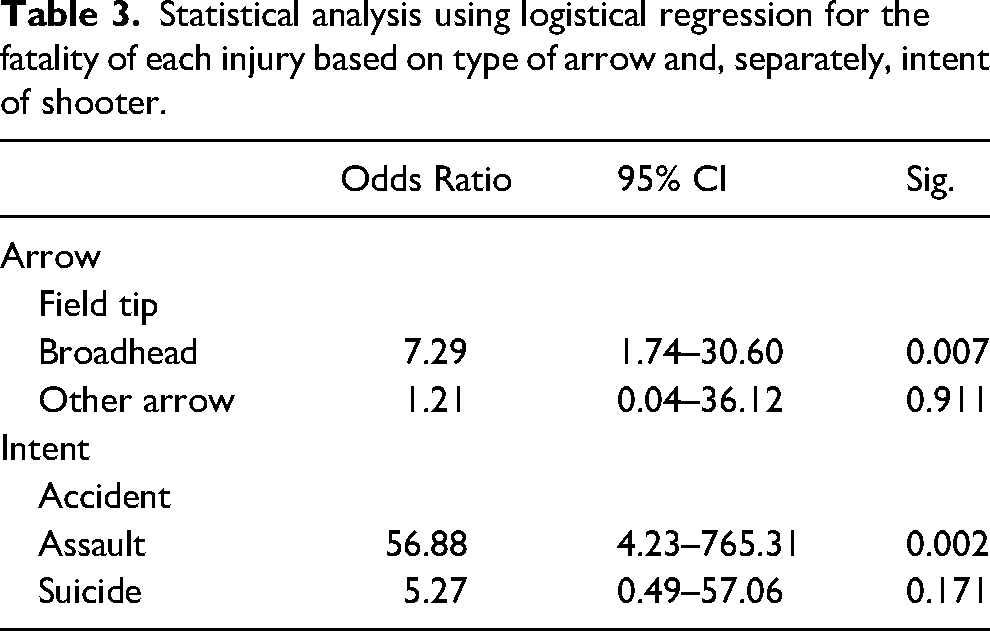
Table 3 presents the odds ratio, the 95% confidence intervals for odds ratios, and the statistical significance of each predictor. Both arrow type and intent were statistically significant predictors of fatality. The influence of arrow type was moderate; patients struck with a broadhead were approximately 7.3 times (95% CI 1.74, 30.6, p = .024) more likely to die from their injuries than those struck with a field tip, adjusting for intent of injury. Fatalities were approximately 57 times (CI 4.22, 765.31) more common in victims of assault compared to those with unintentional injuries, adjusting for the type of arrow. Risk of fatality was not different for patients attempting suicide compared to those with unintentional injuries (p = .17).
Statistical analysis using logistical regression for the fatality of each injury based on type of arrow and, separately, intent of shooter.
Discussion
The significantly higher proportion of males (87.7%) reported with crossbow injuries matches the pattern demonstrated in injuries from firearms. In the United States, males make up 86% of all firearm fatalities and 87% of all nonfatal firearm injuries. 73 Globally, this pattern is repeated, with firearm deaths for males exceeding deaths for females in all age ranges. 74 Most published reports of crossbow injuries came from Germany (25), the United States (22), and Japan (8). Adults in Germany may purchase crossbows without requirements for a license or background check. In the United States, no background checks are required to purchase crossbows, and minimum age and restrictions on the use of crossbows during hunting season may vary on a state-by-state basis. 75 In Japan, laws restricting crossbow ownership went into effect in March 2022. 76 National restrictions on access to firearms are associated with lower rates of firearm suicide and homicide, 74 but this has not been demonstrated for crossbows.
Characteristics of crossbow injuries are complex and less studied than ballistics from firearms. The kinetic energy of the arrow is determined by the speed and weight of the arrow. The draw weight of the crossbow correlates to the maximum speed of the arrow. Other factors include the distance traveled by the arrow, trajectory, and type of arrow. Crossbows can generate an arrow speed of 47 meters per second, equivalent to 34 joules. 77 Broadhead, or flanged, arrows are specifically designed for hunting and cause significant tissue damage by shredding through skin, fascia, muscle, and vasculature on entry such that the resulting wound cannot easily be approximated and closed. Field points are used during practice shooting and are designed to cause minimal damage to targets. Both field tip and broadhead arrows (shown in Figure 2) are capable of deep penetration into tissue when fired from a crossbow (experimental penetration into the thorax of pig corpse 17 cm field tip; 29 cm broadhead) and may result in exit wounds. 77 Thin bones, such as facial or metacarpal bones, are readily penetrated, although this reduces penetration depth into soft tissue. Arrowheads tend to become lodged in thicker bones, such as the femur and humerus. 35 Broadhead tips appear to do more damage than field tips in studies of experimental wounds.77,78

Image of crossbow arrowheads showing the field tip (left) and the broadhead (right).
Injuries by broadhead arrow were more likely to be fatal in this review. The extra blades and cutting surface area on the broadheads result in gaping wound tracks, which could provide an explanation for the higher fatality rate due to increased amounts of tissue damage. Wound tracks from field points are narrower with minimal tissue tearing, and tissue elasticity may close the track, reducing hemorrhage. Several of the case reports discuss the importance of leaving the arrow in situ and mention that the shaft serves to tamponade bleeding.6,14,17,19,20,27,43,53,77 This is likely more effective for field tips.
Persons assaulted using a crossbow are more likely to sustain fatal injuries. In several cases, multiple arrows or other means were used to kill the victim after initial injury by crossbow. Suicide attempts by crossbow were fatal 29% of the time. This case-fatality ratio (CFR) is much higher than that for attempts using cutting (0.7%) and poisoning (1.9%), similar to the CFR for attempts by jumping (27.9%), and much lower than the CFR for attempts by hanging (52.7%) and by firearm (89.6%). 79
Field Management
Prehospital management will begin with the primary survey, which should be conducted following the standard trauma ABCDE format includes evaluating patency of the airway (key if the arrow is located in the neck), breathing (penetrating thoracic trauma can lead to pneumothorax), circulation (broadhead arrows often cause major hemorrhage and this must be stabilized), deformity/disability, and exposure/environment (in the backcountry setting, performing regional exposure to assess all sites of injury while minimizing heat loss). As exsanguination is the most common cause of preventable death in penetrating trauma, proper assessment and stabilization of active bleeding is crucial. This can usually be achieved via stabilization in situ of the arrow or, if the arrow is removed, packing the wound with gauze. Per American College of Surgeons triage guidelines, penetrating injuries to the head, neck, torso, and proximal extremities require urgent transport to the most comprehensive trauma center in the region once ABCDE has been addressed. 80 The decision to stabilize the arrow in situ or remove it is an important one due to the risk of significant hemorrhage and depends on several factors. Among these, anatomic wound location, patient transport method, and time to definitive care are most important. Generally, penetrating foreign bodies should be stabilized in situ until the patient can receive definitive care, as removal may precipitate hemorrhage from a wound that was tamponaded by the arrow shaft. If the location of the arrow threatens the patient's airway or impedes indicated CPR, removal should be considered. If the scene is in the backcountry, here defined as >2 h of transport time from the scene to definitive care, packaging and/or transport methods to move the patient to an evacuation point may require removal or clipping of the arrow shaft for adequate patient mobility. If removal is indicated, field tip arrows can be removed directly by backing it out through the entry site. While there are no set removal techniques, some general principles can be applied. If there is significant resistance when attempting removal, it is possible the arrow has lodged in dense tissue (bone, solid organ, etc), and removal is likely contraindicated due to hemorrhage risk. In this case, or in the case of a broadhead arrow, heavy-duty trauma shears or multitools may be used to cut arrow shafts. Carbon fiber arrows may be crushed with pliers to allow for easier clipping. Care must be taken to avoid jostling the portion of the arrow remaining in the patient. If available equipment is not adequate to cut the arrow shaft or causes movement of the portion of the arrow remaining inside the patient, responders will need to reconsider the risks and benefits of removal versus transportation with the arrow in situ. See Figure 3 for further management details.81–86
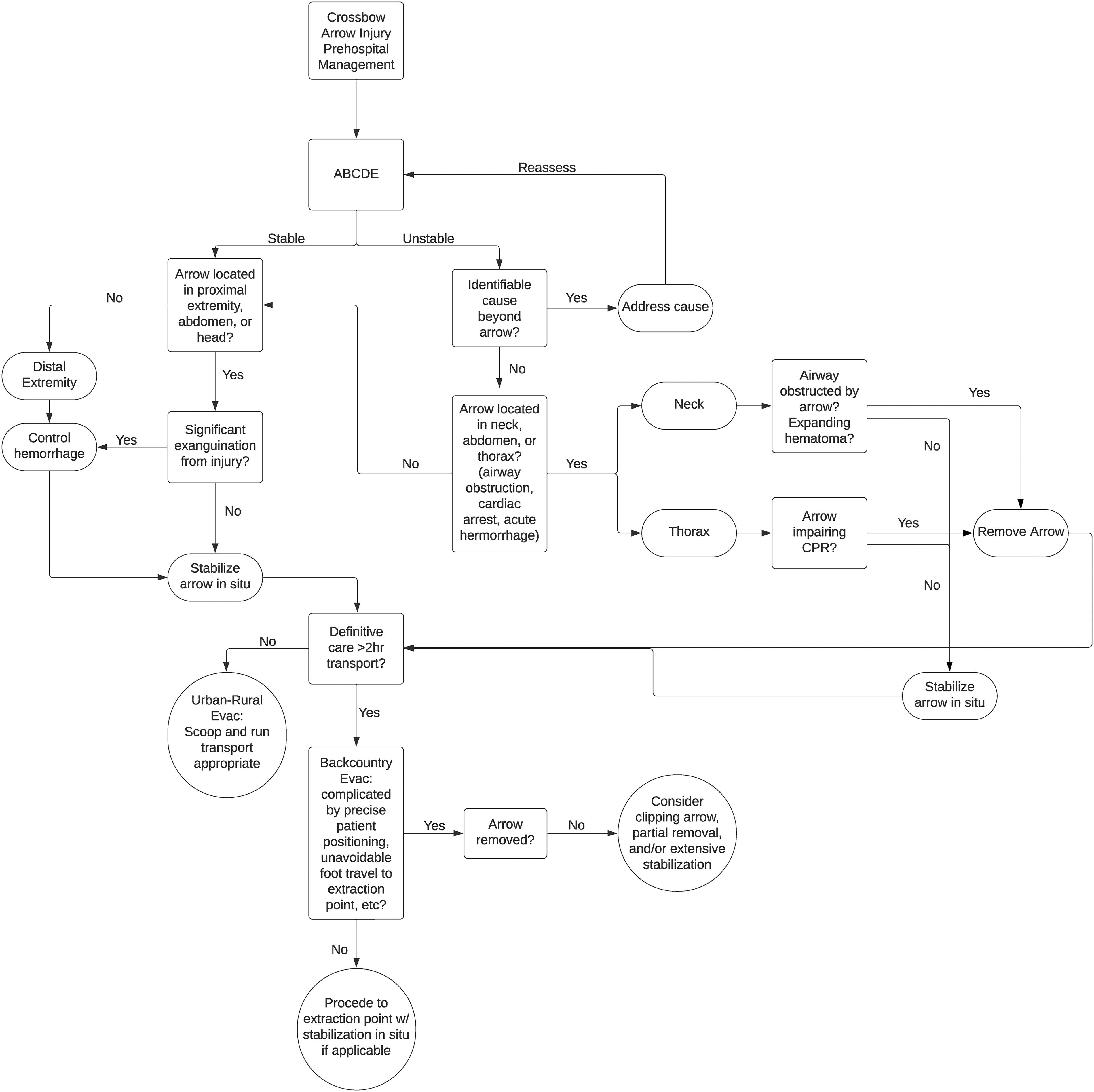
Prehospital management algorithm for penetrating crossbow injuries.
Limitations
This study is limited by the number of case reports and case series present in the literature and the search strategy, as evidenced by the failure to capture the case from our institution. The search strategy looked for the search terms in the titles and keywords of each paper. Our institution's paper did not have the terms in the title or keywords, yet it did directly discuss a case of crossbow injury. Other cases may have been missed for this reason as well. Patients with minor injuries may not have a case report published that provides information about the injury. Small numbers of published cases result in imprecise effect sizes with large confidence intervals. Also, the lack of uniformity among the case reports and case series limited the number that could be included in the statistical analysis. Further, the classification of arrow type was not known in 30% of the cases, leaving room for significant variance when comparing the mortality of field tips and broadhead injuries. Distance and time to definitive medical care may also impact outcomes.
Conclusions
Crossbows are potentially lethal weapons but are sold primarily as hunting equipment and have fewer restrictions on sales than firearms. Injuries from broadhead arrows are more likely to be fatal than those from field tips. The anatomic location of injury does not correlate with fatality. More than half of all crossbow injuries are attempted suicide and carry a high case-fatality rate. Management of crossbow injuries largely follows general principles of trauma care, and the arrows should be stabilized in situ unless the arrow threatens the airway, impedes CPR, or poses a significant risk for further injury during patient transport in backcountry settings, in which cases removal or clipping should be considered.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.