
Abstract
Pig bite injuries are an infrequently described consequence of human–animal conflict. The domestic pig is thought to be a placid animal not given to unprovoked aggression. We report 2 separate cases of children managed at our institution who sustained abdominal injuries after attack by domestic pigs in rural Zimbabwe. Both incidents occurred at home in remote rural areas with long prehospital transport times. Initial resuscitative interventions were performed in both cases in the prehospital setting and at poorly resourced peripheral hospitals before referral. Prophylactic antibiotics were also given in both cases. Laparotomy was performed for both patients. Reduction of eviscerated bowel, exploratory laparotomy, and peritoneal lavage were performed with closure of the abdominal wounds. No surgical site infections were encountered, and patients were subsequently discharged after an uneventful convalescence. Prehospital care is the crucial phase of management of these injuries, which frequently take place in remote, rural settings and usually have a long time to definitive intervention. Expeditious laparotomy and exploration are indicated, as well as meticulous attention to techniques to avert infectious complications. Despite the generally placid temperament of the domestic pig, their bite can result in grave injuries, including abdominal evisceration necessitating prompt referral and emergency laparotomy.
Keywords
Introduction
These cases have been reported in accordance with the surgical case report guidelines criteria. 1 Pig-bite injuries are a relatively rare consequence of human–animal conflict. 2 Attacks by the domestic pig, Sus scrofa domesticus, are even more rare because of the characteristic placidity of these animals.3,4 Bites have been known to occur in the context of an occupational hazard in pig farmers, 5 as well as those who keep pigs as pets. 6 It was reported that pig-bite injuries constituted just 3% of occupational injuries on swine farms, 5 and only sparse case reports or small series exist. 6 Provoked attacks are more common than unprovoked ones and frequently occur during attempted capture, transport, or immobilization of the animal. 5 The ferocity of the attacks in the following cases is striking, and the severity of the injury is almost without precedent for the domestic pig. We have not been able to find previous cases of domestic pig bite leading to abdominal evisceration in the English literature. In contrast, attacks by the Eurasian wild pig are frequent and have been described for centuries. 7 This is a reflection of the well-documented aggressiveness of the wild pig and the presence of large tusks. One report compiled 11 previous cases of evisceration after wild pig attacks. 7
The Landrace pig is a well-known breed that originated in Denmark. 8 Prized for its fast growth and large litter size, it is a popular breed the world over. In rural Zimbabwe, a variety of breeds are kept by smallholder farmers, including the Landrace and Yorkshire breeds, as well as the indigenous Mukota breed. 9 Pigs owned by smallholder farmers comprise 80% of the estimated 202,234 total pig population of Zimbabwe. 10 Rural animal husbandry in Zimbabwe typically takes place in semi-arid farming areas with small herd sizes and makeshift enclosures. 9
Management of abdominal pig bites with evisceration includes mandatory laparotomy with careful exploration and meticulous attention to antisepsis. Prehospital maneuvers as well as resuscitation may improve outcome, particularly when a long interval between injury and surgery is anticipated. We report 2 cases of abdominal injuries inflicted by domestic pigs causing organ evisceration in children managed at an academic hospital in Zimbabwe. Written informed consent was obtained from both patient’s parents for publication of these case reports and accompanying images. Ethical approval for this publication has been exempted by our institution.
Presentation of Cases
Case 1
A 6-y-old boy was referred to our hospital after having been attacked by a domestic pig. He was at his family homestead in rural Zimbabwe when he was attacked during the day, apparently without warning or provocation. The pig charged toward him, biting him in the right lower abdomen and right anterior thigh before retreating. He immediately fell to the ground with bleeding of the bite area. The incident occurred outdoors where 3 pigs were kept in a fenced pen near the house. The child and his friends had opened the pen and approached the animal to feed it. This happened during the winter month of July.
The homestead was 79 km from the closest district hospital (Figure 1). He was transported from the homestead to the nearest district hospital first by an animal-drawn scotch cart and then by a public commuter omnibus in the company of his grandmother and siblings, none of whom had any medical or first aid training. He arrived approximately 3 h later. Fluid resuscitation was initiated with two 20 mL·kg-1 normal saline boluses for class 2 hypovolemic shock (anxiety, irritability, tachycardia [132 beats·min-1] and normal blood pressure [77/54 mm Hg]), and the bowel was covered with an occlusive dressing. Specialist surgical services are not available at district hospitals, and therefore a decision to transfer to our academic hospital was made. He was transferred from the district hospital to our academic, referral hospital by ambulance in the company of a registered general nurse. The time he spent at this district hospital in addition to travel time to our hospital was 8 h in total.
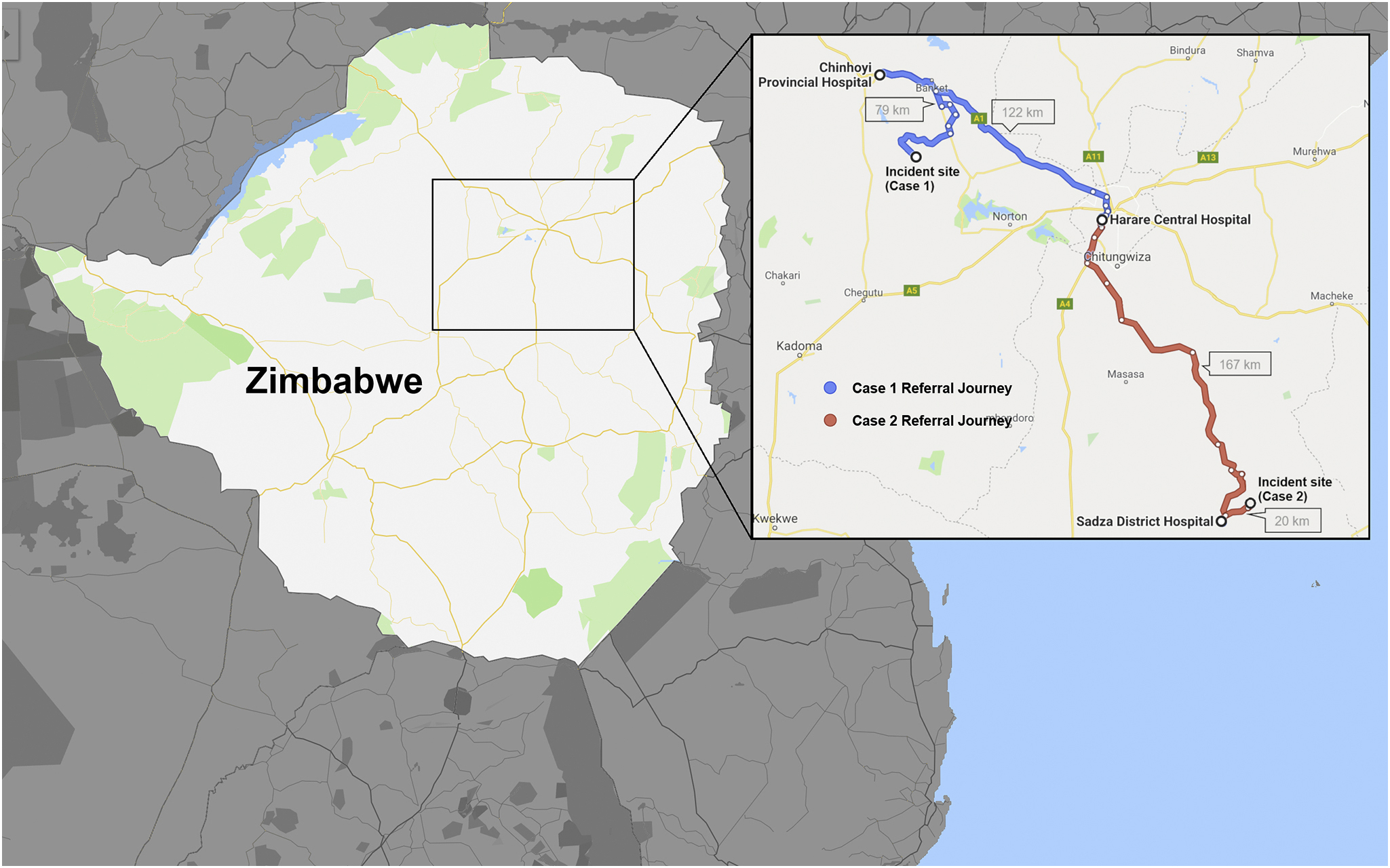
Map showing both patients’ referral journey. This image shows a map of Zimbabwe illustrating the distances the patients had to travel to reach definitive care at the academic hospital.
On arrival in the emergency department, his vital signs had improved with a pulse rate of 120 beats·min-1 and a respiratory rate of 30 breaths·min-1. He was afebrile (36.2°C) and normotensive for age (85/60 mm Hg). He was noted to be pale and significantly dehydrated. His abdomen was soft and not distended, with mild tenderness around the wound. He had evisceration of small bowel through a ragged wound (4 × 3 cm) in the lower right abdomen as well as an additional 3 × 1 cm small wound on the right anterior thigh (Figure 2A and B). The bowel looked viable with no perforations immediately visible. There were no defensive injuries noted elsewhere.
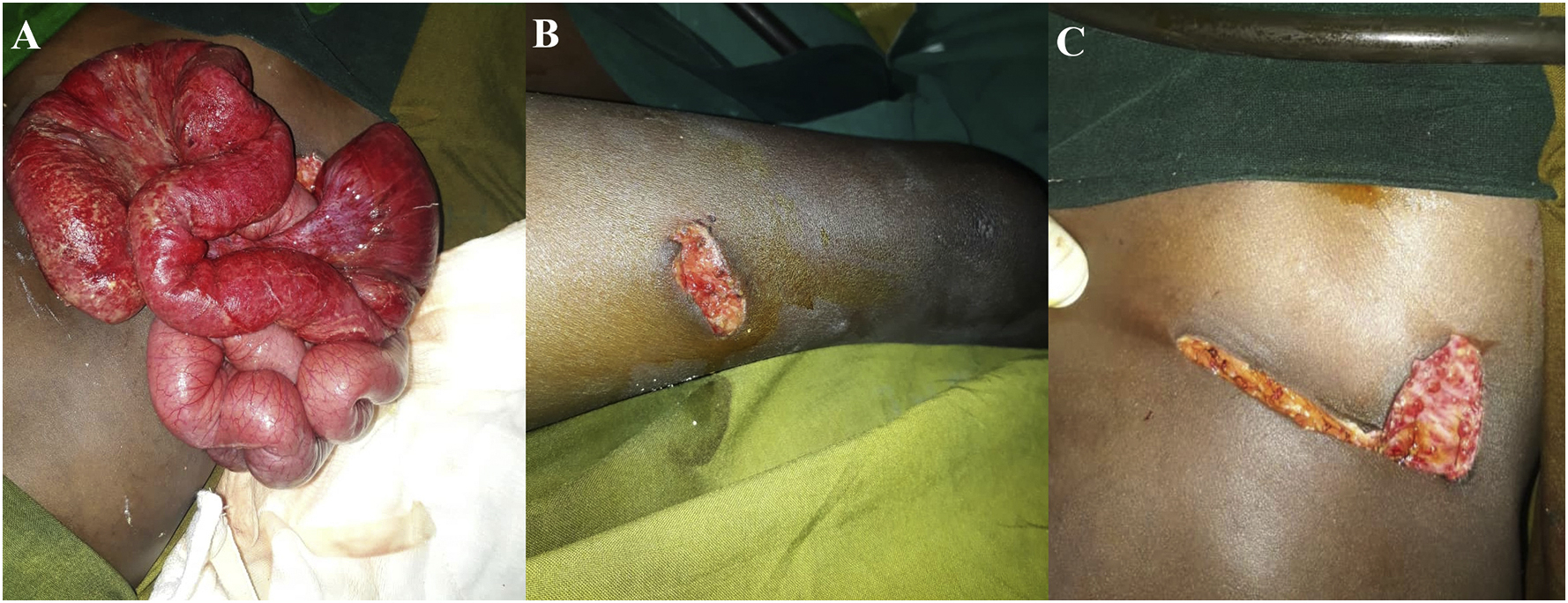
Intraoperative images of case 1. (A) Preoperative state with eviscerated small bowel. (B) Laceration on the right anterior thigh. (C) Postoperative appearance after sheath closure.
The urinary bladder was catheterized, and the patient received a 20 mL·kg-1 bolus of normal saline via 2 large bore peripheral intravenous catheters in the upper extremities. Good urine output response and improved peripheral pulses were noted, and fluids were maintained at 60 mL·h-1 of Ringer’s lactate. Oxygen was administered to improve perfusion to eviscerated bowel, and prophylactic intravenous antibiotics were given (ceftriaxone and metronidazole).
Serum biochemistry was normal and complete blood count was remarkable for a mild leukocytosis 4 –11 of 11,800/mm3 and a slightly low hemoglobin of 12.5 g·dL-1.
At laparotomy, the abdominal wound was extended medially to increase the wound aperture that had caused the bowel to become dusky in the 1 h after admission. A thorough examination of intra-abdominal viscera and retroperitoneum was performed. The bowel was inspected from the ligament of Treitz to the rectum, as were all solid organs and biliary tree. No hollow viscus perforation or solid organ injury was noted. After a wound swab, the abdominal wall wound was debrided and irrigated with saline, and the sheath was closed (Figure 2C).
Wound cultures taken from the wound swab at the time of surgery revealed profuse growth of Acinetobacter baumannii (anitratus). The isolate was sensitive to ciprofloxacin, amikacin, and piperacillin/tazobactam. The wound remained macroscopically clean, and the skin was closed 72 h later with good results. Antibiotics were given for 24 h.
Case 2
A 13-y-old boy was referred to our hospital from a peripheral district hospital after having sustained an injury from a pig bite. The incident occurred at his rural home in Zimbabwe while he was feeding the animal (Figure 1). The attack involved a close rush in the open from an adult domestic pig. The child was bitten once on the abdomen, after which he fell and was bitten again when on the ground before being rescued by onlookers.
He arrived at the nearest district hospital 1 h later via a hired private car accompanied by his father. He was noted to have eviscerated bowel. He was given a 20 mL·kg-1 normal saline bolus and empiric intravenous antibiotics (ceftriaxone and metronidazole), and the bowel was covered in saline soaked swabs. Thereafter, he was transferred via ambulance to our academic hospital accompanied by a registered general nurse. He arrived at our hospital 9.5 h after the incident.
On arrival he was febrile (38.2°C), tachycardic (115 beats·min-1) with a blood pressure of 107/62 mm Hg, and dehydrated. He had a scaphoid abdomen with no evidence of peritonitis. He had a 5 × 5 cm epigastric wound with viable eviscerated stomach and large bowel and ragged wound edges. There were 2 additional small wounds in the epigastrium and right hypochondrial region (Figure 3A and B).
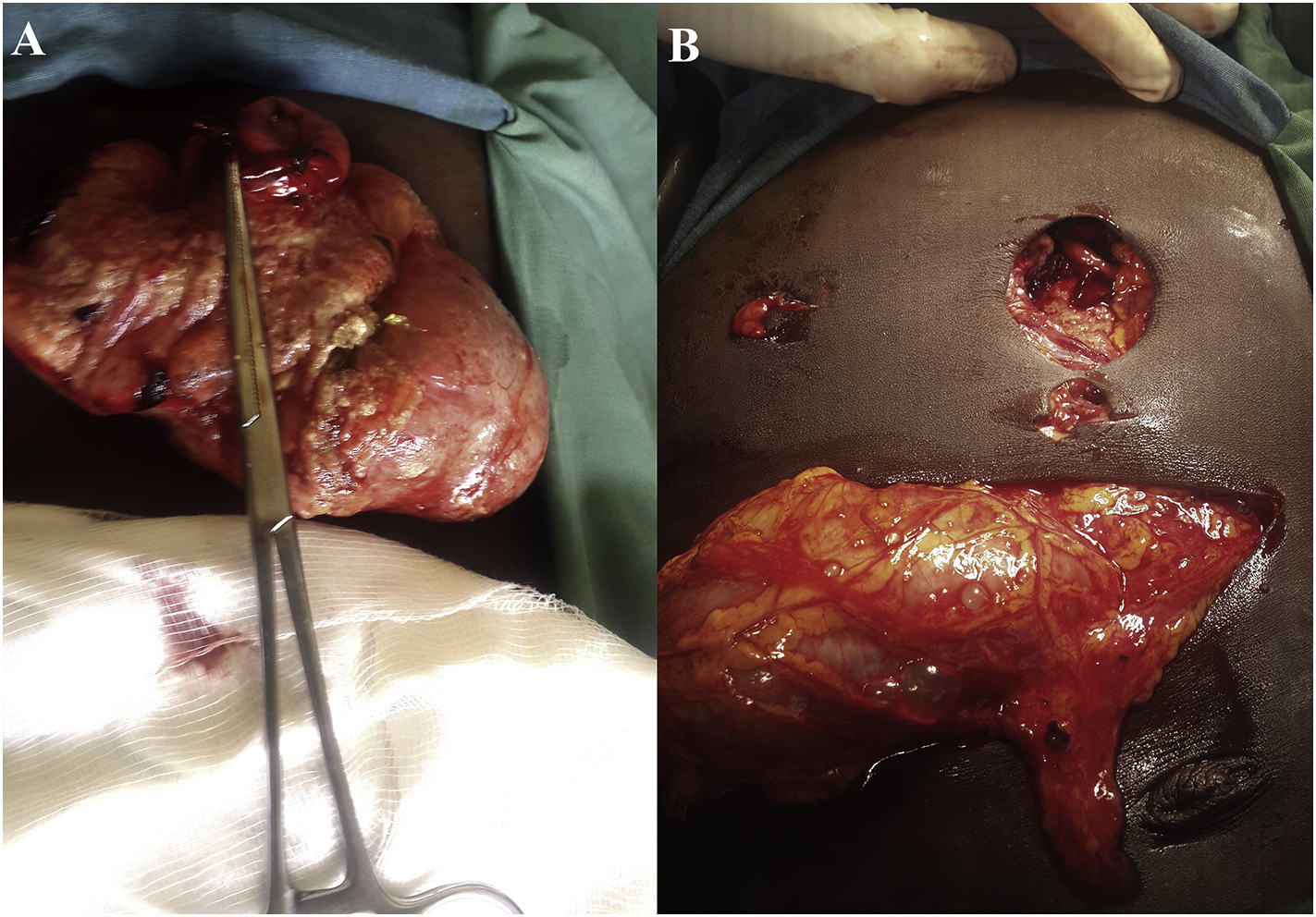
Intraoperative images of case 2. (A) Eviscerated stomach with an anterior perforation. (B) Abdominal wounds after reduction of viscera.
Routine blood investigations revealed normal serum electrolytes and hemoglobin of 11.6 g·dL-1. The coagulation profile was normal.
After fluid resuscitation with 90 mL·h-1 of Ringer’s lactate maintenance as well as oxygen and analgesia, he was taken for surgery. There was transverse colon and stomach protruding from the largest wound, with an anterior gastric perforation. This was freshened and closed primarily. A separate supraumbilical incision was made to facilitate reduction of the visceral herniation by intra-abdominal traction and full abdominal exploration. No additional intra-abdominal injuries were found. Saline peritoneal lavage was performed, and the wounds were debrided and closed in layers.
Postoperatively, the patient was admitted into the intensive care unit and electively ventilated for 7 h because of episodes of intraoperative hypotension requiring vasopressors. He made an uneventful recovery. Antibiotics were continued for 24 h.
Discussion
The incidence of pig-bite injuries has been estimated as 1.5 per 100,000 population in Brazil with a male to female ratio of victims of 6.7:1. 11 Children may be particularly vulnerable to animal bite injuries and tend to sustain more severe injuries. 12 –14 This could be attributed to the discrepancy between the size of the animal and child and the perceived threat of the victim by the pig. It was previously shown that young pigs considered a human who adopts a low squat position to be less threatening than a human who stands tall and erect. 15 This may have contributed to the behavior noted in our cases. Other human behaviors considered to be threatening include closely approaching the pig and attempting to interact with the pig. 16 Fear of humans in pigs is associated with negative contact between the two15,17 and may contribute to adverse behavior. 4
In a comprehensive compilation of wild pig injuries, it was 7 noted that the typical pattern in adults involved injury to the lower part of the body below the waist, whereas in our cases the injuries were exclusively above the waist, presumably reflecting the relative size of animal and victim. Bite wounds are typically ragged lacerations inflicted by sharp teeth. 2 The prominent lower canines of the wild pig are commonly implicated in lacerations inflicted by bite wounds, 2 whereas the canines of domestic pigs in commercial pork farms are typically clipped to reduce injury to piglets 2 and are anatomically smaller.18,19 These practices are neglected in rural smallholder systems and may augment the risk for serious injuries.
Bite wounds are characterized by penetrating trauma mixed with blunt trauma to tissues, which leaves relatively devitalized, ragged wound edges. 7 This in addition to contamination from the animal’s mouth, the environment, and enteric organisms as well as the long time between injury and presentation increases the theoretical risk for wound infection. Prophylactic antibiotics, saline lavage, debridement of wound edges, and staged wound closure may help avert this complication. The use of primary closure in the second case may justifiably be critiqued in view of the risks of infection, and we would recommend staged closure in all such cases. Fortunately, wound infection did not develop in this case.
Wound infection after pig bite is rare2,20 and the causal bacteria have included Pasteurella aerogenes, 21 Actinobacillus suis, 22 and various streptococcal species.6,23 Prophylactic antibiotics that have been found useful in preventing infections from these organisms include ampicillin, cephalosporins, and ciprofloxacin, 21 and this informed our choice. Metronidazole was also given to cover for the possibility of enteric anaerobes. Guidelines by the Eastern Association for the Surgery of Trauma for prophylactic antibiotic use in penetrating abdominal trauma emphasize that prophylactic antibiotics should have a broad coverage including aerobes and anaerobes. 24 The rationale for prophylactic antibiotics is to prevent abdominal surgical site infection, which occurs at a rate of 23% for contaminated abdominal wounds in our hospital. 25 The consensus in the literature seems to be that a single preoperative dose is sufficient for penetrating trauma not of animal origin in the absence of evisceration and bowel injury, whereas administration should be continued up to 24 h in the presence of hollow viscus injury. 24 ,26,27 We gave antibiotics for 24 h because of the evisceration and the presumed heavy contamination from the porcine mouth and environment as well as the prolonged pretreatment period. Administration for longer than this in penetrating abdominal trauma is not supported by the available evidence. 24 ,26,27 Routine wound swabs should be performed whenever there is a risk for wound infection in a contaminated wound, particularly when atypical organisms are anticipated whose sensitivity is unknown. This allows for early goal-directed therapy if infection occurs and is standard practice in our hospital.
Acinetobacter baumannii is a well-recognized cause of nosocomial infection that has gained recent prominence because multidrug resistant strains can cause nosocomial outbreaks with high mortality rates. 28 Acinetobacter spp can be found almost anywhere in the environment in different habitats such as soil, water, sewage, human, foods, and animals. 29 They have been isolated from birds and fish but not from pigs, as far as we are aware. 29 It seems more plausible in the first case to implicate a nosocomial contaminant source for the isolated pathogen rather than the oral flora of the pig. Previous authors have found that isolates from pig bites may be misidentified or remain unidentified because of the limitations of available commercial kits or conventional methods. 30
Both of our cases occurred in remote, rural areas where access to medical facilities was difficult and at least one transfer was required to reach definitive treatment. This emphasizes the importance of first aid and preliminary resuscitation in remote district hospitals to improve outcome. Prompt transfer is the priority; however, a number of prehospital maneuvers may be used before transfer to improve outcomes. Enlargement of a tight wound causing vascular compromise of the bowel has been suggested31,32; however, this procedure has not been evaluated in large studies, nor has this recommendation been incorporated into guidelines. 33 It has been used to prevent loss of large lengths of bowel that would cause catastrophic short bowel syndrome. 34 We suggest this maneuver should be used in patients with bowel evisceration when laparotomy is not anticipated in the next few hours and signs of bowel ischemia are noted, including dusky color and reduced contractility in addition to a tight entrance wound. It should be carried out under local anesthesia by someone with some experience in abdominal surgery 31 in a direction that facilitates the subsequent laparotomy. Potential risks of performing this procedure include the risk of inflicting more injury to the bowel or its mesentery and abdominal wall vessels. There may also be a risk of causing reperfusion injury to the bowel.
Attempts to reduce eviscerated abdominal contents into the abdomen in the prehospital setting without going to the operating room are generally discouraged because of the risk of reducing an occult perforation into the peritoneum or inflicting additional injury to the bowel. 32 The only conceivable situation in which manipulating the bowel before operating may be useful is the case in which an acute angle exists on the mesentery as a large loop of bowel hangs precipitously over the abdomen, causing vascular compromise. The bowel may be gently placed in a less dependent position on top of the abdomen, or the patient may lie on his or her side to minimize kinking of the mesenteric vessels. Isolated omental evisceration may be ligated and amputated with the ligated proximal portion reduced back into the abdomen when absolute indications for laparotomy are not present. 35 Covering the bowel with an occlusive dressing or nonadhesive plastic to avert fluid and heat loss and protect the exposed bowel from further injury is another maneuver that may also prove useful, particularly when the time to definitive care is long.31,36 Guidelines for penetrating abdominal trauma recommend laparotomy within 15 min. 37 This may not be feasible with the constraints imposed by the long distances traveled by patients.
Visceral evisceration is definitive evidence of peritoneal violation and continues to be an absolute indication for laparotomy. 33 Nonoperative management of stable patients with visceral evisceration has a high failure rate, as high as 20%. 38 In a prospective study of patients with penetrating abdominal injuries over 8 y of age, 78% were found to have intra-abdominal injuries requiring repair.37,39 Multiple additional studies have found high rates of intra-abdominal injury38,40 with intestinal evisceration, which justifies the need for mandatory laparotomy and exploration in these patients.
Conclusions
Despite the generally placid temperament of the domestic pig, its bite can inflict grave injuries, including abdominal evisceration necessitating prompt referral and emergent laparotomy. Prereferral resuscitation and other maneuvers may facilitate transport and improve outcome when incidents occur in remote areas far from definitive care.
Author Contributions
Case report design, subject research, consent, and writing (DSM); case report design, writing, research, and editing (PM, TZ); case report design and editing (TG, BAM, KM, CM, MM, YM).
Financial/Material Support
None.
Disclosures
None.