
Abstract
Snakebite is a significant public health issue in which venom-induced consumption coagulopathy is a common and serious complication that results from the activation of the coagulation pathway by snake toxins. We report a male patient, 56 y old, who was thought to have been bitten by a snake on his left foot. He was transported to a nearby hospital where he received analgesics and 3 snake polyvalent antivenom vials, and then he was transported to our hospital after 12 h. He presented with 2 small puncture wounds, pain, blistering, and edema of the left foot. On the 2nd day, the patient developed gingival bleeding and hematuria. Laboratory investigations upon admission revealed prothrombin time (PT) of more than 3 min, prothrombin concentration (PC) of less than 2.5%, and an international normalized ratio (INR) of 23.43. Further investigation of urine showed more than 100 RBCs. Despite receiving 16 packs of plasma and 40 snake polyvalent antivenom vials manufactured by VACSERA over 3 days, hemoglobin concentration and platelet count decreased with the appearance of jaundice, lactate dehydrogenase was 520, and reticulocytes were 3.5%. PT was more than 300 s, and INR was still over range. Plasmapheresis and corticosteroids were provided, which improved the patient’s general condition, PT, PC, and INR, and the patient was discharged after 6 days of hospital stay. This case report indicated that plasmapheresis and corticosteroids were clinically efficient approaches in the management of snake envenomation unresponsive to antivenom.
Introduction
Snakebite is a significant public health issue in many tropical and subtropical countries. About 5.4 million snakebites occur each year, resulting in 1.8 to 2.7 million cases of envenomation. There are between 81,410 and 137,880 deaths and around 3 times as many amputations and other permanent disabilities each year. 1
In Egypt, each year, venomous animals result in about 200 fatalities and around 10,000 envenomations. 2 However, because many victims choose to forgo medical attention and instead turn to traditional healers, these figures may actually be understated. 3
There are numerous snake species that are common in Egypt present in the Nile River Valley and Western Dessert where Alwahat district present, 3 including those belonging to the Elapidae family (Naja haje [Nh], Naja pallida, Naja Nubiae, and Walterinnesia aegyptia [Wa]), 4 Viperidae (Cerastes cerastes, Cerastes vipera, Pseudocerastes persicus fieldi, Echis pyramidum, Echis coloratus, Echis carinatus),5,6 Typhlopidae (Ramphotyphlops braminus), Boidae (Eryx jaculus), and Colubridae (Psammophis sibilans). 7 Cerastes cerastes, Echis carinatus, and Echis pyramidum are the most common snake species present in Alwahat. 3
Venomous snakes mainly have hemotoxic and/or neurotoxic venom. Their cytotoxic effect can lead to local tissue necrosis. 8 Coagulopathy is a common and serious manifestation of severe Viperidae snake envenoming. Venom-induced consumption coagulopathy (VICC) results from the activation of the coagulation pathway by snake toxins. It causes elevated D-dimer, low fibrinogen, and prolonged prothrombin time—all of which are features of disseminated intravascular coagulation (DIC). 8 VICC's high D-dimer, delayed prothrombin time, and reduced fibrinogen have led to comparisons to disseminated intravascular coagulation (DIC) quite frequently. However, VICC lacks other crucial DIC characteristics, such as end-organ failure and signs of systemic microthrombi. 9 Hemolysis can occur due to the action of phospholipase A2 enzyme (PLA2) (in snake venom) on the red cell membrane. Intravascular hemolysis and rhabdomyolysis enhance renal ischemia and can lead to acute kidney injury (AKI). 10
The polyvalent antivenom used in managing snakebite envenomation is usually effective when used at the appropriate dosage. However, there is still conflicting advice about the appropriate dosing, frequency of administration, and duration of therapy. The neutralizing power of antivenoms varies according to the type of antivenom. Even when the venom is neutralized by antivenom, there may be a delay before the recovery of the coagulopathy state. 11
In Egypt, only the polyvalent type of antivenom is produced by Vacsera. It is a sterile product produced from the purified plasma of healthy horses that have been immunized against the most dangerous snakes in Egypt, as well as a vial containing lyophilized powder and a 10 mL diluent vial (water for injection). 5 The polyvalent product can neutralize many Egyptian snake venoms—for example, Cerastes cerastes, Cerastes vipera, Pseudocerastes persicus, Vipera ammodytes, Macrovipera palestinae, Macrovipera lebetina, Echis carinatus, Echis coloratus, Naja haje, Naja nigricolles, and Naja oxiana. According to the manufacturers’ recommendations (Vacsera), the initial recommended dose is 5–10 vials by slow intravenous infusion after dilution with normal saline at a rate of 5–10 mL/kg body weight over 1 h. A further dose of 5 vials of antiserum is administered if signs and toxicity symptoms persist, until symptoms are improved. 12 Generally, the total dose required is needed to neutralize venom and cease symptoms. 5
Although the roles of antivenom therapy and supportive care are critical for successful treatment of venomous snakebites, some patients can be intolerant to snake antivenom, as it carries risks of life-threatening anaphylactoid reactions; therefore, plasmapheresis and steroids are very helpful. The role of plasmapheresis in the management of envenomation has been successfully explored in snakebite victims, especially those who were complicated with coagulopathies. 13 In addition to eliminating the venom circulating in the blood, redistribution will pull the extravascular toxin out, and then it can be cleared via plasmapheresis. 14 The role of corticosteroids in the management of snake venom–induced hemolysis is not widely explored. Therefore, we report a case of a severe snakebite envenomation in which plasma exchange and corticosteroid were used successfully as a means of therapy.
Case Report
A male patient, 56 y old, with no past medical history, was bitten on his left foot while he was working in the field in the Alwahat district; he did not see what exactly had bitten him. He was transported to the central hospital in his residency area, where he received traditional management in the form of washing the site of the bite, analgesics, and 3 vials of snake antivenom; then he was transported to an Egyptian national poisoning center in Kasr alainy teaching hospitals, Cairo University, about 12 h after the snakebite. The patient came with pain, swelling, and edema of the left foot. There were two small puncture wounds with blisters (Figure 1) on the swelling corresponding to the fang marks. On the second day of admission, the patient noticed gingival bleeding and hematuria with edema extended to the knee, as well as cellulitis and ecchymosis over the whole left lateral lower limb (Figure 2). At the time of admission, the blood pressure of the patient was 120/70 mm Hg, and the pulse was 70 beats/min. Laboratory investigations revealed a red blood cell count (RBC) at 6.7 million, hemoglobin concentration at 13.9 mg/dL, platelet count 232 thousand, prothrombin time (PT) more than 3 min, partial thromboplastin time (PTT) more than 3 min, prothrombin concentration (PC) less than 2.5% and international normalized ratio (INR) 23.43, creatinine 1.5 mg/dL, urea 32 mg/dL, Na 132 nm/L, and k 18.1 nm/L. Further investigation of urine analysis showed more than 100 RBCs. Vascular surgery consultation revealed cellulitis and no evidence of compression syndrome. The patient received 16 packs of plasma and 40 polyvalent snake antivenom vials over 3 days (according to the Egyptian Ministry of Health and Population protocol, which provides the polyvalent antivenom); antiedematous and anti-inflammatory local treatment as well was started upon admission. Despite that, no improvement was observed, and there was a further reduction in hemoglobin concentration—platelet and RBC counts reached 4.7 mg/dL, 50 thousand, and 2.23 million, respectively, and the patient became jaundiced. His total bilirubin was 3.2, direct bilirubin 1.24, indirect bilirubin 1.96, lactate dehydrogenase (LDH)was 520, and reticulocyte count was 3.5%, despite no schistocytes or spherocytes were detected in the blood film. Coombs test was done, revealing a negative result. PT reached more than 300 s, and INR was still over range. Plasmapheresis was chosen and took place at the hemodialysis unit after the hematology consultation. After this session of plasmapheresis, the patient’s local tissue reaction regarding the lower-limb swelling started to improve. His general condition, PT, PC, and INR improved as well, while his hemoglobin concentration was 7.1. The patient then received 1 gram of methylprednisolone IV for 3 successive days, and his hemoglobin concentration increased to 9.7; the patient was discharged after 6 days of hospital stay. The patient’s clinical and laboratory findings throughout his hospital stay are summarized in Table 1

Blister on the small puncture site of the snake venom.

Edema extended to the knee; cellulitis and ecchymosis spread over the whole left lateral lower limb.
The patient clinical and laboratory findings throughout his hospital stay.
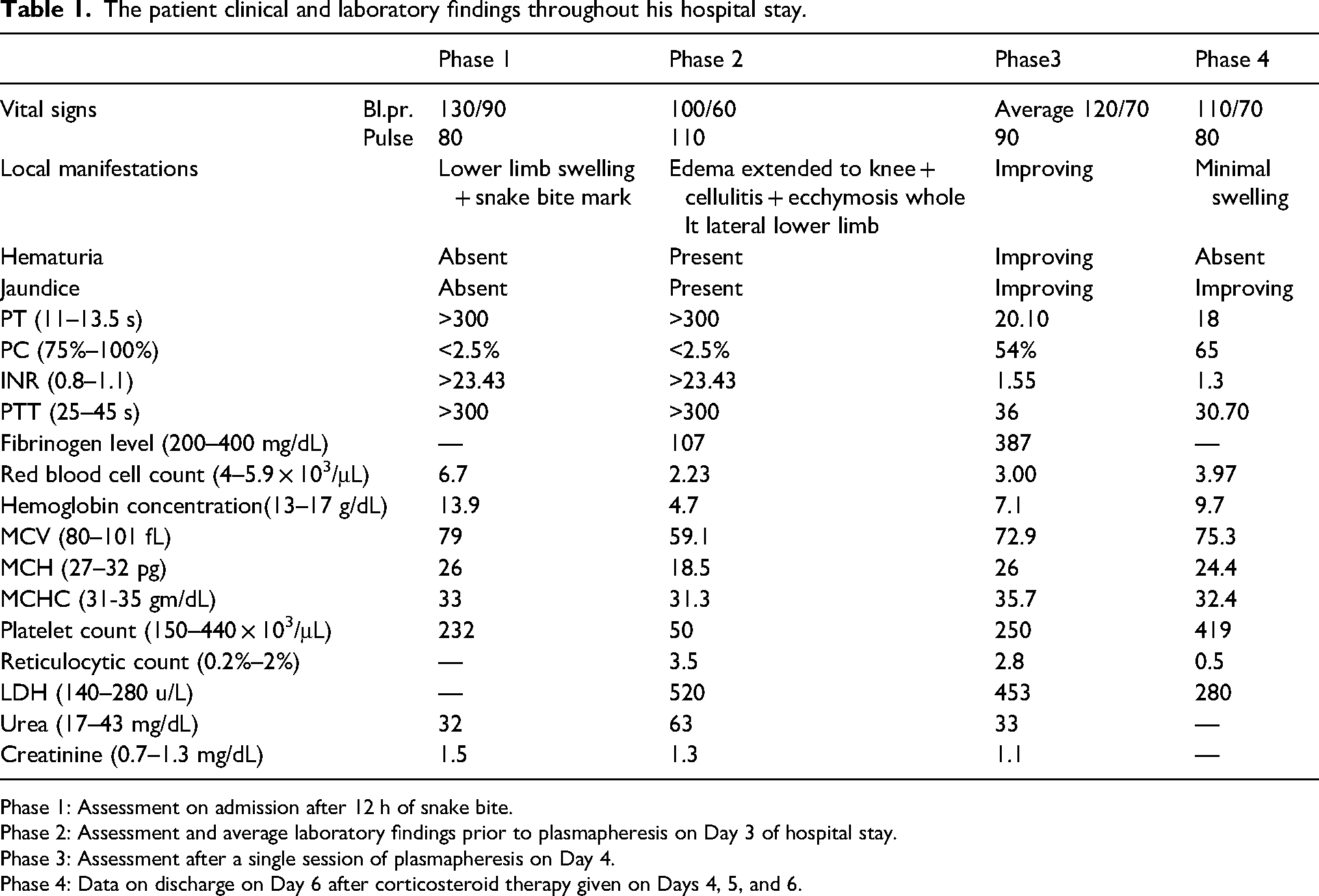
Phase 1: Assessment on admission after 12 h of snake bite.
Phase 2: Assessment and average laboratory findings prior to plasmapheresis on Day 3 of hospital stay.
Phase 3: Assessment after a single session of plasmapheresis on Day 4.
Phase 4: Data on discharge on Day 6 after corticosteroid therapy given on Days 4, 5, and 6.
Discussion
Snakebites in Egypt are common in areas of the Nile River Valley and Western desert, including the regions of South Valley and El-Wahat El-Bahariya. 3 It is a frequent and usually fatal occupational and environmental risk, especially in rural regions of developing nations. 8
Despite our patient not seeing exactly what has bitten him, the systemic signs in the form of venom-induced consumption coagulopathy (VICC) within 12 h of the bite, in addition to the local manifestations (pain, swelling, and blister formation at the location of the bite), suggested that it was a snake bite. The patient's increased PT and INR necessitated the delivery of antivenom on an urgent basis. Hence, the whole blood clotting test (WBCT) was not performed in this instance. He suffered hemolysis after that, which showed up in his lab and clinical tests. Our patient's INR levels were beyond the range, indicating that the VICC was severe, according to the commonly used criteria of VICC, which is INR > 1.5. 15
VICC develops because procoagulant toxins in snake venom activate a coagulation cascade, causing a severe coagulation factor deficit that ultimately results in bleeding. 8 Because of increased D-dimer levels, a prolonged prothrombin time (PT), and low or undetectable fibrinogen levels, VICC is associated with disseminated intravascular coagulopathy (DIC). VICC is distinct from DIC due to its quick start and remission of disarranged coagulopathy, which typically lasts for 48 h, absence of systemic microthrombi, and end-organ damage. 9
Bleeding can occur at the bite site or on the mucosal surfaces of different organs, and it is one of the main consequences. This is explained by the hypothesis that the presence of specific proteinases, such as hemorrhagins and hemolysins, which act on the arterial wall and cause endothelial damage in addition to coagulopathy, results in bleeding. 16
This case report was partially similar (apart from the acute kidney injury that did not happen in our case) to that reported by Mohan and colleagues, 14 who noticed a case of Russell's viper bite on the left index finger, and after giving 20 vials of anti–snake venom (ASV), that case developed hemolysis with elevated LDH, thrombocytopenia, and acute renal injury on day 3; microangiopathic hemolytic anemia (MAHA) was suggested, and after exclusion of other organ damage, the patient's platelet count, coagulation parameters, and LDH were improved after receiving 3 cycles of therapeutic plasma exchange. Our Egyptian case received a total of 40 polyvalent snake antivenom vials over 3 days (5 vials every 6 h according to the bleeding profile of the patient) 12 (conferring to the Egyptian Ministry of Health and Population protocol, which provides the polyvalent antivenom), even though no refinement developed until improvement in his blood picture and coagulation profile rapidly occurred after one TPE with FFP, and fresh blood administration followed by steroid intake for 3 days.
Intravascular hemolysis is a rare, life-threatening manifestation of snakebite envenomation, seen mainly after bites by exotic venomous snakes. Liapis and colleagues 10 reported a case of massive intravascular hemolysis due to Vipera ammodytes envenomation with characteristic spherocytic hemolytic anemia associated with hemoglobinuria and acute renal failure. Unlike our case, four vials of polyvalent antivenom (Imunoloski zavod-Zagreb European viper venom antiserum) were rapidly effective in reversing spherocytic hemolytic anemia.
Unresponsiveness to antivenom was also reported in an Indian patient with prolonged venom-induced consumption coagulopathy, lasting for 7 days and owing to Echis carinatus sochureki envenoming. The patient did not respond to 30 vials of Indian polyvalent antivenom in Jodhpur, India. The patient had features of local and hemotoxic envenoming in the form of prolonged prothrombin time and activated partial thromboplastin time. At the same time, platelet count and hemoglobin concentration were normal, with no signs of hemolysis. The patient received supportive care with no transfusions needed. Coagulation parameters were finally normalized completely by day 10. 17
The use of steroids in snakebites is debated; while some say they have no specific role, their administration does provide some help to the patient. 18 However, it was indicated that with many snakebite cases, intravenous hydrocortisone was administered to the more serious bites, as they found that it accelerated recuperation. In addition, antivenom contains a fair amount of horse serum, and if big doses are used, serum sickness results and steroids may be needed. 18
Corticosteroid is the first line of management in autoimmune hemolytic anemia and its type Coombs negative hemolytic anemia.19,20 Our patient developed hemolysis evident clinically by jaundice and laboratory by further decrease in hemoglobin level, increased reticulocytic count, bilirubin, and LDH, with negative Coombs test. Despite a modest increase in hemoglobin level after the single plasmapheresis session, the hemoglobin level and other lab parameters of hemolysis improved substantially after methylprednisolone administration.
To our knowledge, methylprednisolone has not been widely used for hemolysis induced by snake envenomation, especially when hemolysis responds to antivenom. However, it was used in a case report of spherocytic hemolytic anemia due to envenomation by a long-nosed viper (Vipera ammodytes), together with antihistaminic (as a part of early allergic reaction management to the antivenom), followed by the anti–snake venom administration and no clinical or laboratory evidence of continued hemolysis postinfusion; spherocytes decreased markedly from the peripheral blood. 10
Conclusions
We report a patient with prolonged venom-induced consumption coagulopathy and hemolysis owing to snakebite envenoming who did not respond to the Egyptian polyvalent antivenom but did respond to plasma exchange and steroid use.
Footnotes
Acknowledgments
We appreciate the patient's thorough explanation of his symptoms and desire to participate in developing the clinical report.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the patient.