
Abstract
BACKGROUND: Mental health problems are estimated to affect one in six individuals in the European Union. Fifty percent of mental disorders start in adolescence, around the age of 14. The stigma associated with having a mental health problem is one of the main barriers to seeking help for psychiatric and psychological disorders among adolescents and young adults. Interventions to reduce social stigma could contribute to increased help-seeking behavior in this population.
Introduction
Mental health problems are estimated to affect one in six individuals in Europe. Despite the difficulty in obtaining accurate data, the total number of people affected by mental disorders in the European Union is estimated to be 84 million (OECD/EU, 2018), of which five million are reported to be affected by bipolar disorder and one and a half million by schizophrenia-related disorders. Most of these disorders start at an early age. Several authors point out that 50% of mental health problems start in adolescence around the age of 14 and 75% of them before the age of 24 (De Girolamo et al., 2012; McGorry et al., 2011), with neuropsychiatric conditions being the leading cause of disability among adolescents and young adults in high-income countries (Gore et al., 2011).
Once diagnosed with a mental disorder, the person has to cope with the symptoms and disabilities caused by the disorder and the consequences of the social stigma that these disorders still generate. Stigma affects individuals with a psychiatric diagnosis in various ways and may add to the mental health problem itself, especially among newly diagnosed adolescents and young adults. Stigma is a source of chronic stress for individuals experiencing it, contributing to the emergence of new health problems (Link & Phelan, 2006). Besides, due to both institutions and the community, stigma is a barrier to access health services for people with mental disorders (Henderson et al., 2013). Furthermore, society’s negative attributions and beliefs regarding mental disorders are also internalized by those experiencing them, especially at the onset of symptoms and at the time of diagnosis. This internalization generates self-stigma in individuals, whereby those who start to develop symptoms consistent with the presence of a mental health problem, generally adolescents and young adults, feel ashamed, experience a loss of self-confidence, and conceal their symptoms so as not to be labeled (Radmanović & Burgić, 2017). Thus, the stigma associated with having a mental health problem and the lack of information have become the main barriers for adolescents and young adults to seeking help for psychiatric and psychological problems, as they prefer to keep the problem a secret rather than seek therapy (Kaushik et al., 2016; Lynch et al., 2018).
Interventions to reduce social stigma in adolescents and young adults could help normalize mental health problems and contribute to increased help-seeking and information-seeking behavior (Wei et al., 2015). Three types of strategies have been described to address social stigma toward mental disorders (Corrigan, River, et al., 2001; Corrigan et al., 2012; Finkelstein et al., 2008): social protest, which seeks to challenge injustices toward people labeled with negative stereotypes, such as people with mental disorders; educational programs, which seek to convey accurate information about mental disorders to specific segments of the public; and direct contact programs involving individuals with mental disorders, which allow participants to challenge their negative attitudes by engaging in some form of direct contact with people with mental disorders. Several systematic reviews comparing the effectiveness of these stigma-reducing strategies have concluded that direct contact with individuals experiencing mental disorders themselves is the most effective method of reducing stigma in adults (Griffiths et al., 2014; Gronholm et al., 2017). However, to the best of our knowledge, scarce studies have explored its effectiveness among adolescents and young adults (Pinto-Foltz & Logsdon, 2009).
Therefore, this study aimed to assess the effectiveness of a direct contact intervention in the classroom involving individuals who have experienced a mental disorder themselves to reduce vocational students’ stigmatizing attitudes.
Method
Design and Setting
A quasi-experimental study was conducted using a pretest–posttest design with a within-subject control involving a sample of students from three different Vocational and Technical Schools in the city of Valencia, Spain, where students can access vocational studies from the age of 16, without upper limit. The exclusion criteria were having any degree of physical or intellectual disability that limited a proper understanding of and participation in the activity, not fulfilling the pretest or posttest, and completing less than 90% of the items of any questionnaire.
The sample size was calculated for a hypothesis test with a 90% confidence level, 80% statistical power, and considering a variance of the questionnaire of 2.5 (Corrigan et al., 2003), resulting in a sample size of 124 subjects. The participants were selected consecutively; no random sampling was applied. Data collection took place over two academic years until the required sample size was reached (from May 2019 to March 2020).
Instruments
Two questionnaires were used to measure stigma-related variables: the Community Attitudes toward Mental Illness (CAMI) and the Spanish Mental Illness Stigma Attribution Questionnaire (AQ-27-E). These questionnaires are public domain tools. In one of the cases, we were requested to register in a webpage before using the instrument (for the CAMI) and we followed this instruction. To use the Attribution Questionnaire (AQ-27), authors are only requested to cite the original study by Corrigan et al. (2003). The validation studies have been properly cited and referenced in the manuscript.
The AQ-27-E questionnaire was developed by Corrigan et al. (2003). The questionnaire was adapted to the Spanish language with good internal reliability (Cronbach’s α = .86) and psychometric properties for assessing stigma in the general population (Muñoz et al., 2015). Stigmatizing attitudes are measured with the AQ-27-E questionnaire after reading a short text describing a person with schizophrenia. Subsequently, participants must indicate their agreement level with a series of statements on a Likert-type scale ranging from 1 to 9, with 1 being the lowest and 9 being the highest agreement level. The 27 items are grouped into nine independent dimensions: responsibility, anger, dangerousness, pity, fear, help, coercion, segregation, and avoidance. The final score for each dimension results from adding up the scores for all the items. Higher scores indicate more negative attitudes or emotions in each dimension, except for the avoidance and help scales.
The CAMI questionnaire is commonly used to assess social stigma. It was adapted to the Spanish language for adolescent populations by Ochoa et al. (2016), with good internal reliability (Cronbach’s α = .86 in the first assessment and .91 in the second), and has been used to measure stigma in adolescents (Vila-Badia et al., 2016). The CAMI assesses stigmatizing attitudes of the population toward people with a mental disorder based on four dimensions: authoritarianism, benevolence, social restrictiveness, and community mental health ideology. Authoritarianism refers to the perception that individuals with a mental disorder are inferior and need supervision and guidance. Benevolence assesses the ability to have sympathetic and caring attitudes toward individuals with mental disorders and views against coercive measures. Social restrictiveness refers to the perception that individuals with a mental disorder are dangerous and need to be controlled. Community mental health ideology assesses the degree of agreement with the idea that individuals with mental disorders should be integrated into the community. Each dimension contains 10 items with a 5-point Likert-type scale ranging from 1 (strongly agree) to 5 (strongly disagree). The score for each dimension results from the sum of all item scores. Higher scores indicate more negative attitudes on the dimensions of authoritarianism and social restrictiveness, whereas on the dimensions of benevolence and community mental health ideology, higher scores indicate less stigmatizing attitudes and greater acceptance of people with mental disorders.
The level of contact or familiarity with mental disorders was measured using the Level of Contact Report questionnaire (Corrigan, Green, et al., 2001), explicitly translated for this study. The questionnaire consists of 12 daily life situations with different levels of contact with people with mental disorders, each item adapted from different traditional scales to measure stigma. The participants are invited to tick all the situations they have experienced in their life and the result is the item with a higher level assigned. The lowest level is 1 (“I have never observed a person that I was aware had a mental illness”). Other intermediate items are “I have watched a movie about mental illness” or “I have worked with a person with mental illness,” and 12 is considered the highest level (“I have a mental illness”). This questionnaire was included to categorize the participants according to their familiarity with mental disorders because it could influence their stigmatizing attitudes (Corrigan, Green, et al., 2001).
Procedure
As a first step, and after obtaining authorization from the principals, a researcher visited the schools and provided potential participants with information about the intervention, clarifying that the activity was not part of any subject in their studies and voluntary, with no impact in the participants’ grades. Students who agreed to participate were provided with the same information in writing and the informed consent form to sign. The students below 18 years of age who were willing to participate received the information in writing, and their parents or guardians had to sign a specific consent form.
After the informed consents were collected, the pretest assessments were administered. One week after the questionnaire completion, the intervention took place in each School. Every intervention involved one person with lived experience and one first-degree relative (children/siblings) of an individual with a mental disorder. There was no kinship between the two participants to favor greater freedom to voice their experiences. The intervention lasted approximately 90 min. During the first 60 min, persons with lived experience shared their firsthand experiences with a mental disorder following a general script to include the evolution from the onset of symptoms, how they coped with the diagnosis, the side effects of medication, its impact on their social and work relationships, and what their recovery has been like since they were first diagnosed. A discussion of 30 min followed in which all questions raised by the students were answered. Posttest measures were collected 10 days after the intervention.
Ethical Considerations
The study was conducted in compliance with the Declaration of Helsinki. Ethical approval was granted by the University of Alicante Research Ethics Committee (Reference No. UA-2017-11-13).
The questionnaires used in the study, the AQ-27 and the CAMI, are public domain tools. The only requirement to use the AQ-27 in research is to cite the original validation study by Corrigan et al. (2003). To use the CAMI, those working in a university or health setting can freely use the scale after registering in the webpage https://camiscale.com. The authors met both requirements.
Statistical Analysis
The Kolmogorov–Smirnov test was used to test the normality assumption. As our sample had a non-normal distribution, nonparametric statistics were used. The Mann–Whitney–Wilcoxon test was used to compare the median scores for the nine subscales in the AQ-27-E and CAMI questionnaires before and after the intervention. The Mann–Whitney–Wilcoxon test and the Kruskal–Wallis test were used to compare the influence of the independent variables with the scores obtained. The statistical significance threshold for all tests was set at 0.05. The effect size was calculated using Rosenthal’s r (Tomczak & Tomczak, 2014). SPSS Statistics version 25 (IBM Corp, Armonk, NY, USA) was used for data processing.
Results
A total of 166 students volunteered to participate in the study, divided into six groups of 25 to 30 students. The final sample consisted of the 128 subjects who had completed at least 90% of each of the pretest and posttest questionnaires, with a response rate of 77%. As shown in Table 1, the mean age of the participants was 18.5 (SD = 1.59) years and 43% (n = 56) had an acquaintance or family member with a mental disorder, the most common being schizophrenia and eating disorders, both at 14.1 % (n = 18). Regarding familiarity with mental disorders, 29% reported having a relative diagnosed with a psychiatric condition and 4% lived with a person with a mental disorder. After the interventions of the persons with lived experience, the students were invited to ask any questions they had. The most frequent questions were the following: “What did you think when you received a psychiatric diagnosis?” “What has helped you more to recover from your mental disorder?” and “How could I help a friend if he or she started experiencing psychiatric symptoms?”
Sociodemographic Description of the Sample and Frequencies of the Level Contact Report Questionnaire.
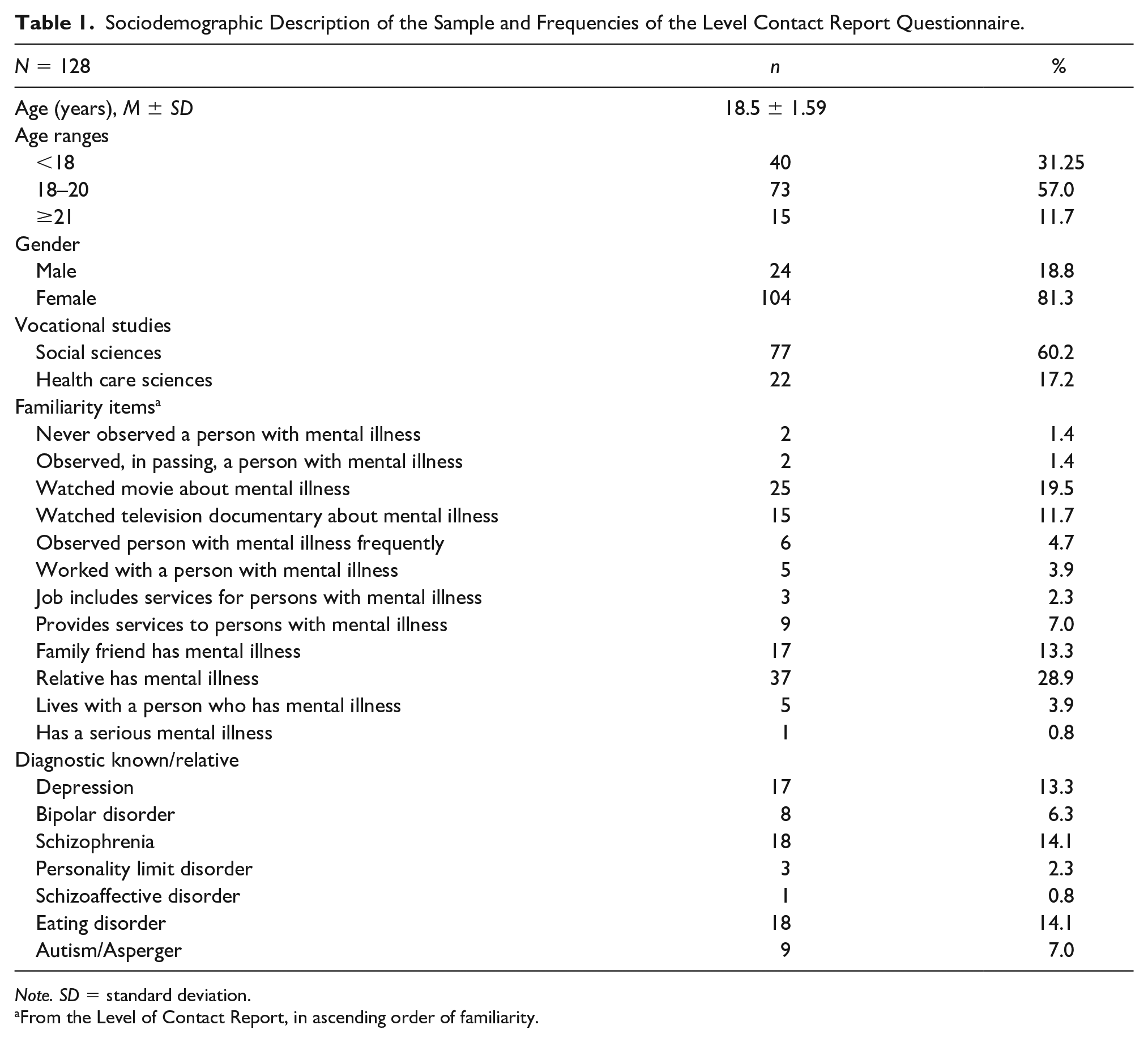
Note. SD = standard deviation.
From the Level of Contact Report, in ascending order of familiarity.
Preintervention Scores
Table 2 shows the relationship between baseline scores for the AQ-27-E and CAMI questionnaires and the variables gender, age, and familiarity with mental disorders. Statistically significant differences were identified in the dimensions of help, coercion, authoritarianism, and social restrictiveness between genders being higher for women, and in the dimensions avoidance, authoritarianism, benevolence, social restrictiveness, and community mental health ideology between age ranges. As shown in Table 2, the medians were higher for females and the lower and middle age ranges.
Influence of Independent Variables on Score Obtained Pre Intervention in AQ-27-E and CAMI Questionnaires.
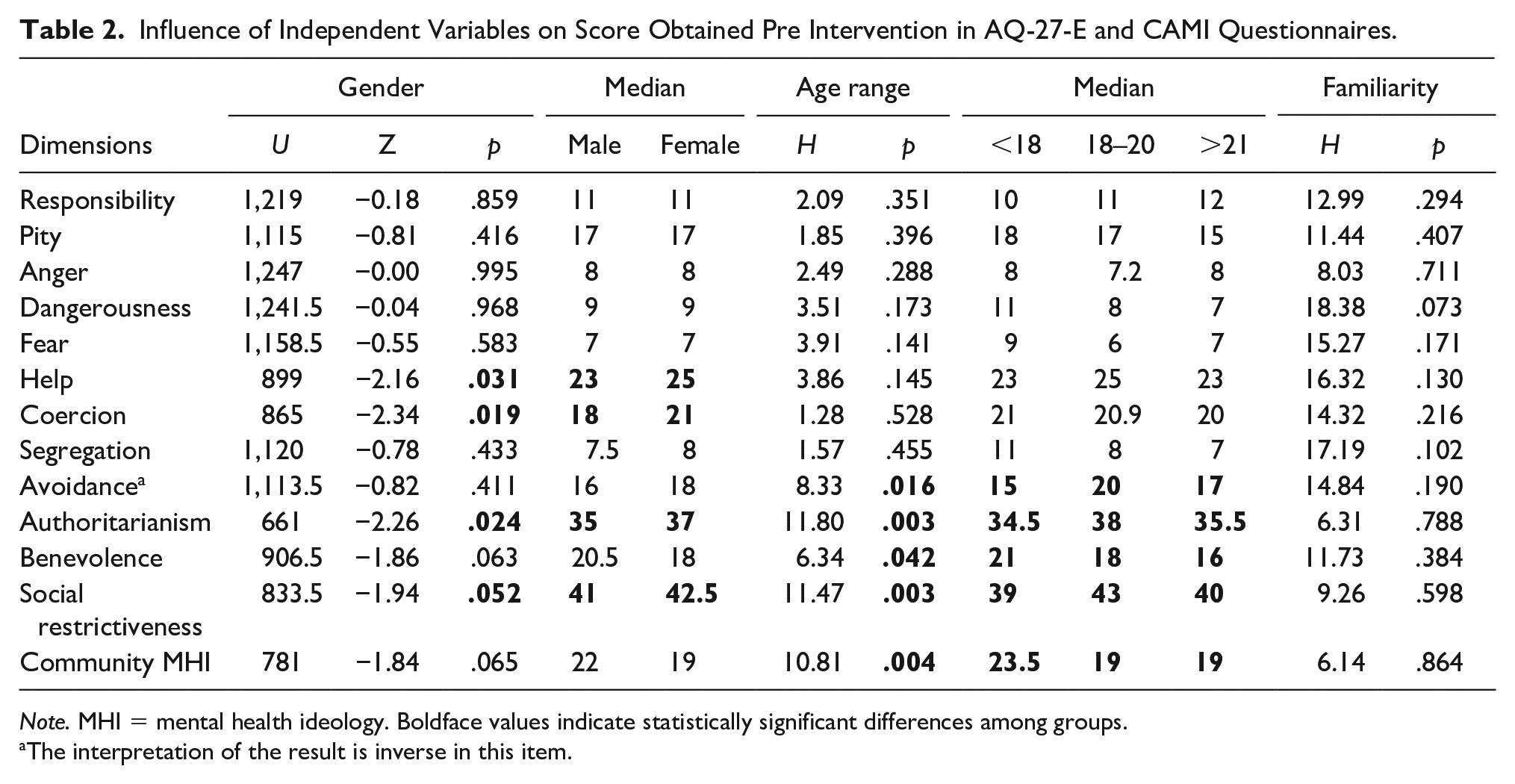
Note. MHI = mental health ideology. Boldface values indicate statistically significant differences among groups.
The interpretation of the result is inverse in this item.
Postintervention Scores
Differences between pre-and postintervention scores were statistically significant (p < .05) in 11 of the 13 variables measured with the AQ-27-E and CAMI questionnaires. Table 3 shows that the effect size was large for the variables anger, dangerousness, fear, coercion, segregation, avoidance, and benevolence as per the criteria suggested by Fritz et al. (2012).
Paired Samples Mann–Whitney–Wilcoxon Comparing Medians of Attribution Questionnaire Factors AQ-27-E and CAMI, Before and After the Use of the Intervention.
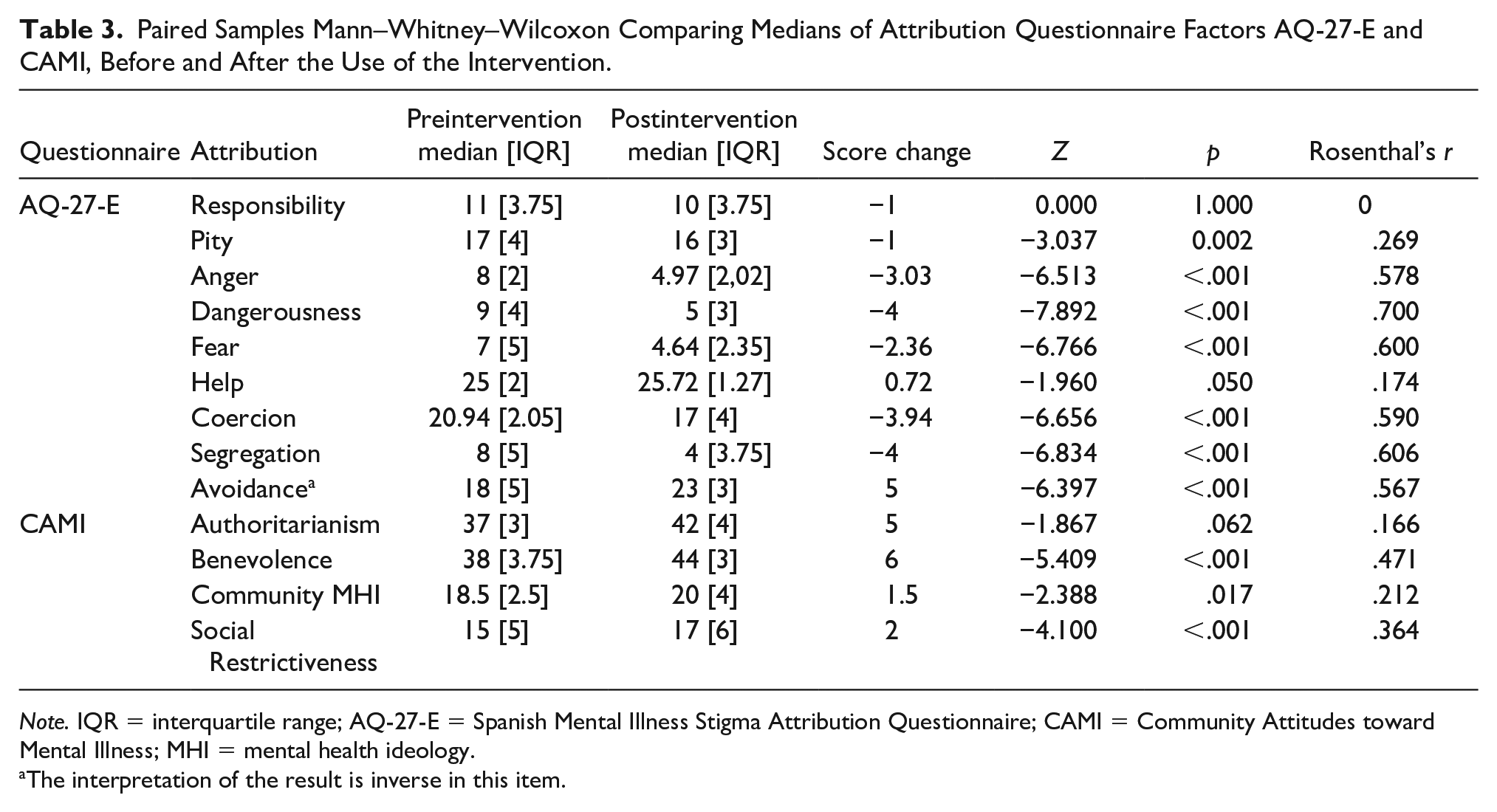
Note. IQR = interquartile range; AQ-27-E = Spanish Mental Illness Stigma Attribution Questionnaire; CAMI = Community Attitudes toward Mental Illness; MHI = mental health ideology.
The interpretation of the result is inverse in this item.
A description of the median score changes and the median scores comparisons before and after the intervention, considering age groups, is provided in Table 4. The Mann–Whitney–Wilcoxon test determined that most dimensions showed statistically significant modifications in the 18 to 20 years old age group, whereas less statistically significant score changes were found for students above 21 years of age. The Mann–Whitney–Wilcoxon test and the Kruskal–Wallis test results are shown in Table 5, illustrating the effectiveness of the intervention depending on the age group and gender for each dimension of the AQ-27-E and the CAMI. Statistically significant changes were found for the responsibility and the avoidance dimensions for age group.
Paired Samples Mann–Whitney–Wilcoxon Comparing Medians of Attribution Questionnaire Factors AQ-27-E and CAMI, Before and After the Intervention for Range Ages.
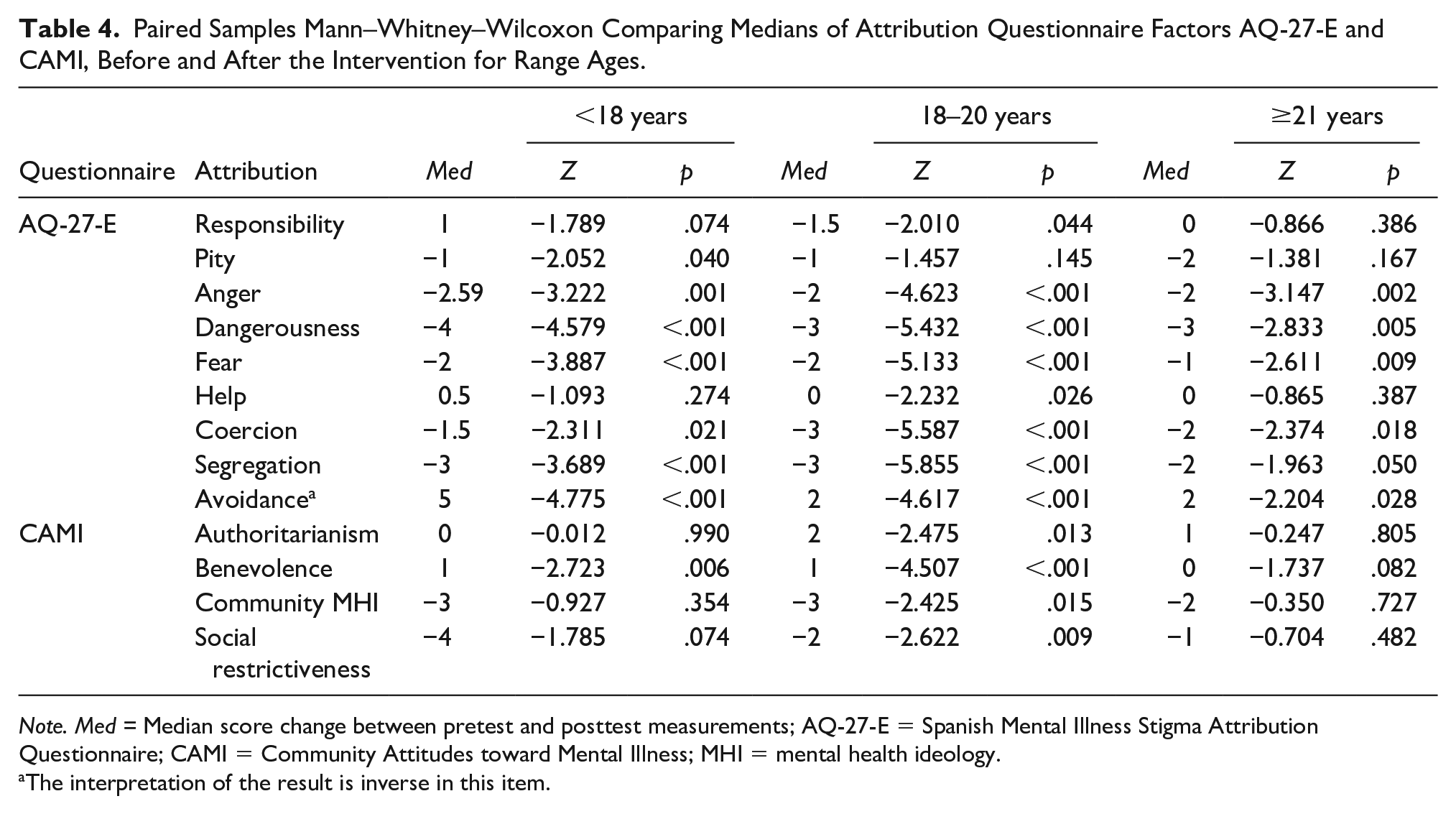
Note. Med = Median score change between pretest and posttest measurements; AQ-27-E = Spanish Mental Illness Stigma Attribution Questionnaire; CAMI = Community Attitudes toward Mental Illness; MHI = mental health ideology.
The interpretation of the result is inverse in this item.
Effectiveness of the Intervention as a Function of Age Group and Gender.
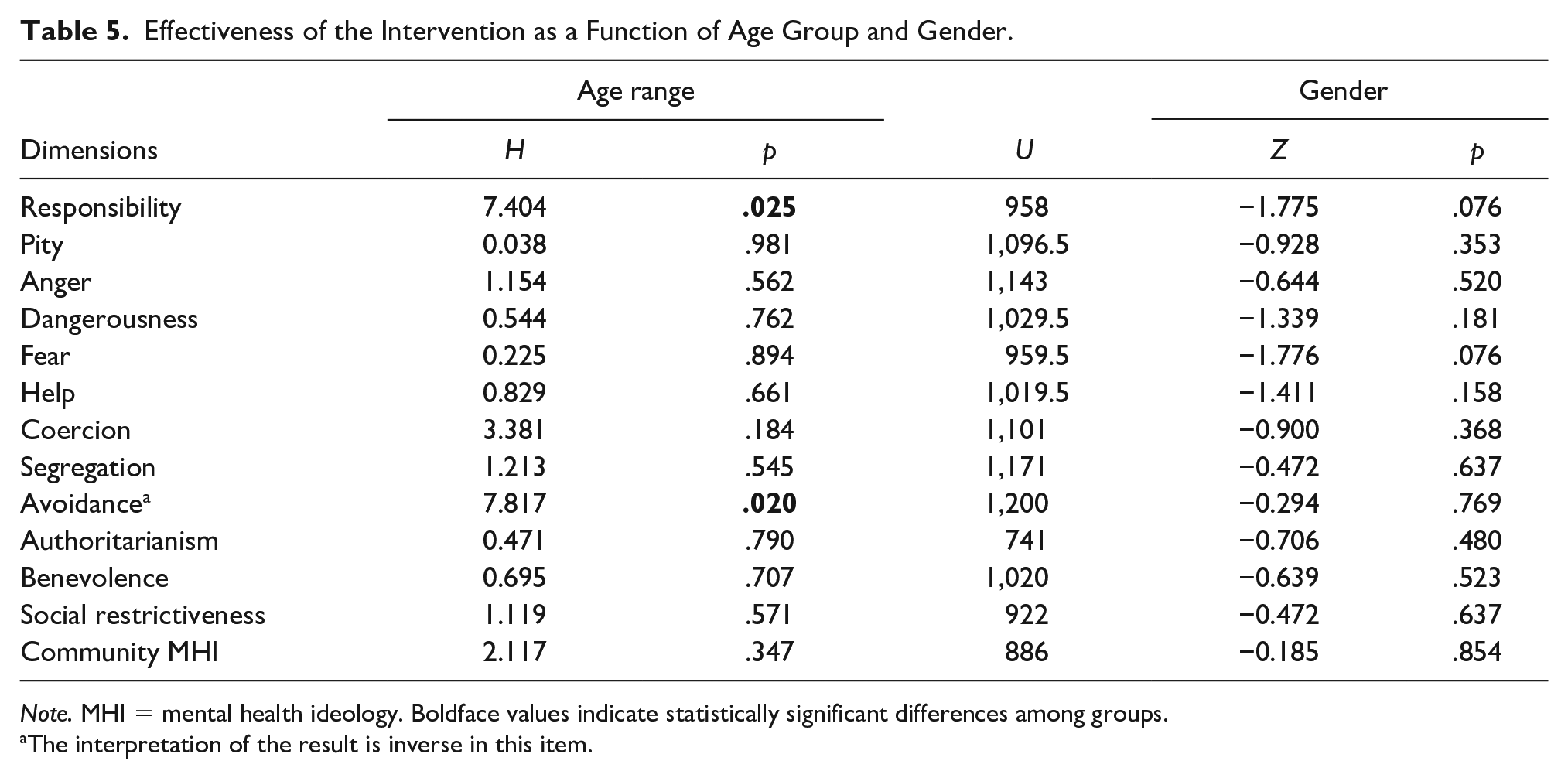
Note. MHI = mental health ideology. Boldface values indicate statistically significant differences among groups.
The interpretation of the result is inverse in this item.
Discussion
The objective of this study was to ascertain whether a direct contact intervention in the classroom involving persons with lived experience reduces vocational students’ stigma toward people with mental disorders. Our results indicate that statistically significant changes occurred in eight of the nine dimensions measured with the AQ-27-E questionnaire (pity, anger, dangerousness, fear, help, coercion, segregation, and avoidance) and in three of the four dimensions measured with the CAMI questionnaire (benevolence, social restrictiveness, and community mental health ideology).
These results are similar to those of another study conducted in a sociocultural context similar to ours that estimated the effectiveness of an indirect contact intervention for adolescents aged 14 to 18 years using the CAMI questionnaire. The intervention improved scores, especially in the authoritarianism dimension, and showed differences in effectiveness according to participants’ gender and familiarity with mental disorders (Vila-Badia et al., 2016). Another study that evaluated the effectiveness of an indirect contact intervention for young people aged 18 to 24 studying an introductory psychology course also reported an improvement in their desire for social distance and decreased negative emotions (Brown et al., 2010). The results obtained are also in line with another study that assessed the effectiveness of a direct contact intervention, developed with nursing students in the same cultural context, in which the authors obtained comparable results, reducing the scores in the same dimensions of the instruments used (Martínez-Martínez et al., 2019).
Our study results suggest that the intervention that we implemented effectively decreased stigma in vocational students, regardless of their gender and previous experiences with mental disorders, and significantly contributed to decreasing their perceived fear and dangerousness of individuals with mental disorders. This effectiveness may be explained by the fact that our intervention included the essential components of an anti-stigma program, as indicated by Corrigan et al. (2013). Including these components makes it possible for students to make direct contact with people with a mental disorder on an equal footing, through the narration of their personal story of self-improvement, in a space where vocational students can empathize with them and learn about their ability to overcome the problems they have encountered as a result of being diagnosed with a psychiatric condition. In addition, after their narration, a peer-to-peer dialogue was established in which all the questions raised by the students are answered, helping to debunk myths about people with mental disorders.
It should be borne in mind that age is a crucial factor in the effectiveness of a direct contact intervention. When analyzing the results by age range, we found that vocational students in the 18 to 20 age range improved their scores for more dimensions than vocational students in the lower and higher age ranges, possibly because the target population of direct contact interventions should be students in this age range. This finding can be explained by the fact that, on one hand, a minimum degree of maturity is necessary to be able to assimilate the new information provided, which in many cases will be inconsistent with what has been learned so far. Without that minimum degree of maturity, it is difficult to internalize that information to achieve a positive attitude change. It may even have a negative effect, raising further questions and concerns (Chisholm et al., 2016). On the other hand, the literature indicates that stigmatizing attitudes are more pronounced at older ages, even if one is more aware of mental disorders (Kaushik et al., 2016), which would explain why this intervention is less effective at ages above 18 to 20 years.
Given that the level of maturity of adolescents can differ significantly even at similar ages (Chisholm et al., 2016), to avoid undesired effects, it would be advisable that direct contact activities with minors be combined with educational interventions (discussions, role-play) that contribute to modifying misconceptions among younger students. Their beliefs are not as ingrained as in adults, which allows them to be addressed through educational interventions (Corrigan et al., 2012). Such is the case with the Mental Illness Education program in the Australian Capital Territory (MIE-ACT), which improved adolescents’ stigmatizing attitudes aged 14 to 18 through an intervention carried out entirely by persons with lived experience. In this intervention, individuals with a mental disorder took the teacher’s place and carried out the educational activities themselves (Rickwood et al., 2004).
It is also important to remark that, in contrast to other studies in which interventions were particularly effective for women (Koller & Stuart, 2016; Vila-Badia et al., 2016) and adolescents who had acquaintances or family members with mental disorders (Vila-Badia et al., 2016), we found no between-gender differences in the effectiveness of our intervention in our target population. First of all, it should be noted that our sample was 81% female and, as stated by Christov-Moore et al. (2014), it is well known that the women’s level of affective empathy is usually higher than that of men. In addition, the degree of familiarity with mental illness is not in itself a contributing factor to positive attitudes and emotions toward people with mental disorders, as it depends on the quality of that previous contact (Gaddis et al., 2018).
Implications for Clinical Practice and Research
Improving stigmatizing attitudes might reduce self-stigma among adolescents and young adults with mental health problems and contribute to their seeking professional help (Henderson et al., 2013). In the case of the intervention’s target students, who are being trained in professions related to care and support for people with different needs, the intervention could also improve the way they care for people with mental disorders.
Further research is needed to ascertain whether direct contact interventions may have an unintended effect on participants due to adolescents’ immaturity, leading to increased stigma toward people with mental disorders. It would also be advisable to continue to observe whether intervention effectiveness and student career paths are related. Longitudinal studies in the medium and long term are also necessary to assess whether results are sustained over time.
Strengths and Limitations
This study has some strengths. The intervention presented was not educational but awareness raising, offered by an association external to the schools to provide truthful information to improve vocational students’ stigmatizing attitudes toward mental disorders. The measurements were made using two different instruments and the analyses were segmented considering the participants’ age and gender. This study has several limitations, as well. First, the lack of a control group limits the generalizability of the results obtained. Second, despite the use of scripts to increase the validity of the study, it is often difficult to have complete control over the content of the intervention, which is continuously changing according to the feedback from the group.
Conclusion
Vocational students’ attitudes and emotions toward people with mental disorders can be improved through a direct contact intervention in the classroom involving persons with lived experience. The age range for optimal results with this type of intervention appears to be 18 to 20 years. Caution should be exercised when delivering interventions based solely on contact with persons with lived experience of mental disorders to minors, as minors may not have acquired the necessary degree of maturity to be able to internalize the new information provided, which may not match their previous knowledge and experiences, leading to undesirable effects. The combination of direct contact with educational activities seems to be the most suitable approach to improving the impact of an intervention (Corrigan et al., 2012).
Footnotes
Acknowledgements
We want to thank the generous collaboration of ASIEM users, family members, and technicians without whose involvement this study would not have been possible, and also Instituto PAX for including interventions by experts by experience in their students’ training. We also want to thank all of the teachers who allowed us to develop this project in their classrooms as well as the students who voluntarily completed the questionnaires, specially to Maria Jose García Martínez.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.