
Abstract
Introduction
Young people are at risk of developing mental health disorders. Depression, anxiety, and behavioral problems are among the primary causes of illness and impairment among teenagers. Suicide is the fourth highest cause of mortality in those aged 15 to 29. This study aimed to assess the determinants of mental health among children in Ethiopia.
Methods
Online databases were searched from inception until March 2023. Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 was used in this review. Subgroup analysis, I2 test, funnel plot, and Egger’s test were performed. Pooled odds ratios (OR) were calculated.
Result
Fourteen studies were included in the meta-analysis. The pooled prevalence of mental illnesses among Ethiopian children was 24.68% (95% CI: 19.99%–32.38%). Having previous child abuse history (OR: 5.65; 95% CI: 4.32-7.39), poor socio-economic status (OR: 1.94; 95% CI: 1.24-3.04), urban residence (OR: 1.93; 95% CI:1.39-2.67), and being male (OR: 1.65; 95% CI: 1.15-2.38) were determinants of childhood mental illness in Ethiopia.
Conclusion
and Recommendations: Mental disorders are highly prevalent in children with a history of child abuse, and a strong legislative body must be established to prosecute child abusers. Interventions that focus on gender equality in education and the creation of a safe environment for poor urban children are suggested.
Introduction
A mental disorder or mental health condition is described as a disturbance in psychological, biological, or developmental processes that underpin mental and behavioral functioning (World Health Organiation, 1992, World Health Organiation, 2022; World Health Organiation). Disturbances are typically associated with difficulties or impairments in personal, familial, social, educational, occupational, and other critical aspects of functioning (World Health Organiation, 2022). Broadly, mental disorders include psychosocial disabilities and other mental states associated with considerable distress, functional impairment, and the risk of self-harm (World Health Organiation). Mental health problems pose a risk for other diseases and lead to both unintentional and purposeful damage (Organization(PAHO) & P.A.H).
Childhood and adolescence are critical stages of physical and mental development. The development of good mental health is critical for good overall health and wellbeing throughout life. Mental diseases in children are characterized by substantial changes in how they normally develop, act, or manage their emotions, resulting in dissatisfaction and difficulties in their daily lives. Many children have occasional concerns, worries, and violent behaviors that cause anxiety (Lebrun-Harris & et al., 2022).
Worldwide, mental health problems affect over 15% of young people aged 10–19 years, accounting for 13% of the global disease burden in this age group (World Health Organization, 2021). From 2016 to 2019, the rate of emergency department (ED) visits in the United States of America (USA) with a primary mental health diagnosis increased only among those aged 0–17 years, rising from 784.1 to 869.3 per 100,000. This declined marginally in 2019, but in 2018 it was 976.8 per 100,000 people, a 25% increase from 2016 (Office of the Surgeon G).
More than 20% of children aged 2–8 years in the United States (17.4%) have documented mental, behavioral, or developmental disabilities (Cree et al., 2018). Over 15% of teenagers aged 12–17 years had major depressive episodes, 37% had chronic feelings of despair or hopelessness, and nearly 20% seriously considered suicide (Bitsko et al., 2022).
Boys were more likely than girls to have mental, behavioral, or developmental impairments between the ages of 2 and 8 years. However, a review in the Middle East and USA revealed that depression in teens is a difficult challenge among adolescent girls because it is caused by both environmental and hereditary factors (Cree et al., 2018; Beirão et al., 2020). Furthermore, more than one-fifth (22%) of the children living in poverty had mental, behavioral, or developmental impairments. Age and socioeconomic status influence the likelihood of children receiving therapy for anxiety, depression, or behavioral issues (Ghandour et al., 2019).
Deaths due to suicide among black children and adolescents in the USA have increased considerably in recent years. Suicide deaths among black youths climbed from 2.6 per 100,000 in 2017 to 4.8 per 100,000 in 2018. Compared to their white counterparts, black males aged 5–11 years are more likely to commit suicide (Ring-the-Alarm-TASKFORCE-REPORT.pdf).
At least one in every seven children in sub-Saharan Africa suffers severe psychological distress. In Africa, millions of young people have been exposed to situations that most adults would find difficult to deal with, frequently dealing with psychological consequences without support (Anonymous).
In sub-Saharan Africa, depression was reported to be prevalent in 27% of the population aged 10–19 years, anxiety disorders in 30%, emotional and behavioral difficulties in 41%, and suicidal ideation in 12%. According to one study, the prevalence of post-traumatic stress disorder (PTSD) was 21% (Jörns-Presentati et al., 2021).
The prevalence of mental disorders in eastern Mediterranean children is estimated to range between 12 and 25% (World Health Organization, 2020). According to the World Health Organization, the age-standardized suicide rate in Ethiopia was 11.4% in 2016, with males having a higher rate (18.7) than females (4.7) (Meshesha & Johnson, 2020).
Attention-deficit/hyperactivity disorder (ADHD) (Lian et al., 2013), fears or anxieties (Sacco, 2022), and behavioral disorders (Tadesse, 1999a) are some of the most prevalent mental diseases in the Ambo region of Ethiopia, and can be diagnosed in children.
The Federal Ministry of Health (FMOH) identified more specific categories of mental health problems among children and adolescents on its website in 2019 as part of a mental health forum, namely ADHD (Greene et al., 2021), oppositional defiant disorders/conduct disorders (Isaksson et al., 2017), anxiety disorders (Lippman, 1976; Ayano, 2021), mood disorders (Ashenafi et al., 2001), elimination disorders (Adewuya et al., 2014), and autism spectrum disorders (Zeleke et al., 2021). The research also revealed a prevalence of "common mental health disorders” (depression, anxiety, and psychological discomfort) ranging from 21.56% to 27.9% (Barsisa et al., 2021).
Although various efforts have been made to address the negative effects of mental disorders and reduce the prevalence of mental illnesses, challenges remain. Emerging rifts, political instabilities, and financial crises are at the forefront of this trend. Although effective prevention and treatment options exist, most children with mental disorders do not receive treatment. Furthermore, many experience stigma, discrimination, and human rights violations (World Health Organiation, 2015).
Identifying factors that contribute to mental disorders can help reduce their prevalence and promote early action. This study aimed to estimate the pooled factors associated with mental disorders among Ethiopian children.
Methods
Exploration approach for primary studies
We searched ScienceDirect, PubMed, the Cochrane Library, and Google scholar for articles. The following keywords on the condition, context, and population were combined using Boolean words for searching: (Mental Disorder) OR (Psychiatric Illness) OR (Psychiatric Illnesses) OR (Psychiatric Diseases) OR (Psychiatric Disease)) OR (Mental Illness) OR (Illness, Mental) OR (Mental Illnesses) OR (Psychiatric Disorders)) OR (Psychiatric Disorder) OR (Behavior Disorders) OR (Diagnosis, Psychiatric)) OR (Psychiatric Diagnosis) OR (Mental Disorders, Severe) OR (Mental Disorder, Severe)) OR (Severe Mental Disorder) OR (Severe Mental Disorders) OR (Mental patients) OR (Mental Disorder[MeSH Terms]) OR (Psychiatric Illness[MeSH Terms]) OR (Psychiatric Illnesses[MeSH Terms]) OR (Psychiatric Diseases[MeSH Terms]) OR (Psychiatric Disease[MeSH Terms]) OR (Mental Illness[MeSH Terms]) OR (Illness, Mental[MeSH Terms]) OR (Mental Illnesses[MeSH Terms) OR (Psychiatric Disorders[MeSH Terms]) OR (Psychiatric Disorder[MeSH Terms) OR (Behavior Disorders[MeSH Terms]) OR (Diagnosis, Psychiatric[MeSH Terms) OR (Psychiatric Diagnosis[MeSH Terms]) OR (Mental Disorders, Severe[MeSH Terms) OR (Mental Disorder, Severe[MeSH Terms]) OR (Severe Mental Disorder[MeSH Terms) OR (Severe Mental Disorders[MeSH Terms]) AND (Ethiopia) OR (Federal republic of Ethiopia) OR (Ethiopia[MeSH Terms]) AND (Children) OR (Child[MeSH Terms) OR (children[MeSH Terms]) OR (Boys[MeSH Terms]) OR (Girls[MeSH Terms).
Eligibility criteria
Inclusion criteria
This systematic review and meta-analysis included both published and unpublished studies in English from the beginning of data inception until February 2023 that reported any type of mental illness in children in Ethiopia. Cross-sectional, case-control, retrospective, and prospective cohort studies have also been included. Only Ethiopian studies that reported any mental disease or at least one adjustment-related factor were considered.
Exclusion criteria
After submitting requests to the respective corresponding authors of the studies, articles that were not fully accessible were excluded. Reports and reviews were excluded from this study.
Outcome measurements
The primary outcome of this study was to assess prevalence, and the secondary outcome was to identify the factors linked to children’s mental health. We estimated the odds ratio (OR) from the primary studies using two-by-two tables for key variables.
Data extraction
The relevant data were extracted using a data extraction format created independently using Microsoft Excel. The data extraction format for the primary outcome included the first author, region (according to the Ethiopian political administration), study period, publication year, study design, sample size, response rate, and prevalence of mental disorders among children.
A data extraction format for the secondary outcome (related factors) was established for each item (age, domicile, parental income, marital status, parental educational status, child abuse history, living situation, and family size). To calculate the odds ratio (OR), we gathered the data for each factor in the form of two tables. Any disagreements between the researchers (KWM, SDH, and BM) during the extractions were resolved by consulting with MA, BM, and ET.
Operational definitions
Children
Young people under 18 years
ADHD
Continuing pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development (Sathiyasusuman, 2011)
Depression
Mood illness characterized by a persistent sense of sadness and loss of interest (Nyundo et al., 2020).
Emotional Behavioral Problem (EBP)
An emotional condition characterized by excesses, deficits, or disturbances in behavior (Tadesse et al., 2012).
Quality assessment
We used the Newcastle-Ottawa Scale to assess the quality of the included cross-sectional studies (Peterson et al., 2011). The tool consists of three main sections: 1) assessing the methodological quality of the studies, 2) evaluating the comparability of the studies, and 3) measuring the outcome and statistical analysis qualities of the original studies.
Statistical analysis
The data were extracted using Microsoft Excel™, and the data were exported from Microsoft Excel to Stata™ Version 14.0 (software) for management and further analysis. The data are presented using text, tables, graphs, and forest plots. We calculated the standard error of the prevalence for each original article.
The heterogeneity between the prevalence of the previous studies was checked using the I2 test together with p-values. Owing to the presence of significant heterogeneity between previous studies (I2 = 96.5%, p < .001), a random-effects meta-regression analysis model was used to estimate the pooled prevalence of children’s mental illnesses in Ethiopia. Moreover, the univariate meta-regression model considered the publication year and sample size of the studies to identify possible sources of heterogeneity. However, these differences were not statistically significant. Potential publication bias was assessed using Egger’s correlation and Begg’s regression intercept tests at 5% significance level. The results of these tests revealed significant publication bias (p > .001 in Egger’s test). To minimize the heterogeneity of the original studies, a subgroup analysis was performed based on the publication year and study setup. Sensitivity analysis and meta-trim-and-fill analysis were performed to determine the impact of a single study on the overall meta-analysis estimate and to remove extremely small studies from one side of the funnel plot. The relationship between mental illness and its associated factors was determined using pooled odds ratios (OR with 95% confidence intervals (CI) for each factor.
Ethics approval
Not applicable.
Results
Exploration of original articles
A total of 1,267 studies were obtained from PubMed, Cochrane, Science Direct, and Google Scholar. Owing to duplication, 240 articles were removed from the list of articles retrieved. Of the remaining 1,027 articles, 600 were excluded after reviewing the titles. Next, 220 articles were excluded because they had multiple outcome variables. After reviewing the remaining 207 abstracts, 194 were eliminated, of which 16 were eliminated due to differences in outcome variables. One new article conducted in January 2023 were added. Finally, 14 articles were retained (Alenko et al., 2020; Aliye et al., 2023; Ashenafi et al., 2000; Fekadu et al., 2006; Gebeyehu et al., 2019; Girma et al., 2021; Jebena et al., 2016; Lola & Belete, 2019; Mulatu, 1995; Mulu et al., 2022; Nyundo et al., 2020; Shiferaw et al., 2018; Tadesse et al., 1999b, 2012) for final qualitative analysis, as shown in the PRISMA flowchart (Figure 1). PRISMA flow chart of studies on mental illness among children in Ethiopia.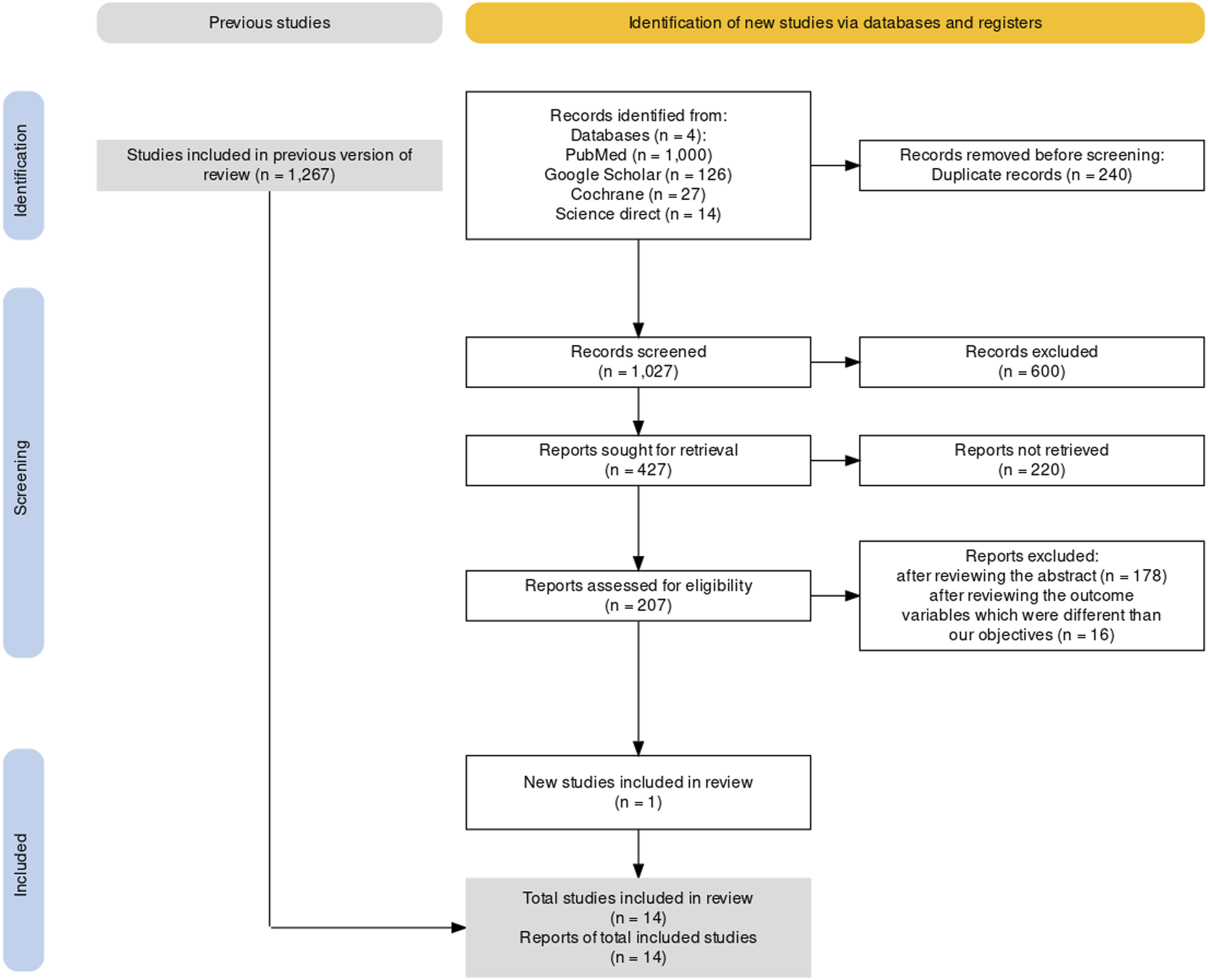
Characteristics of original studies
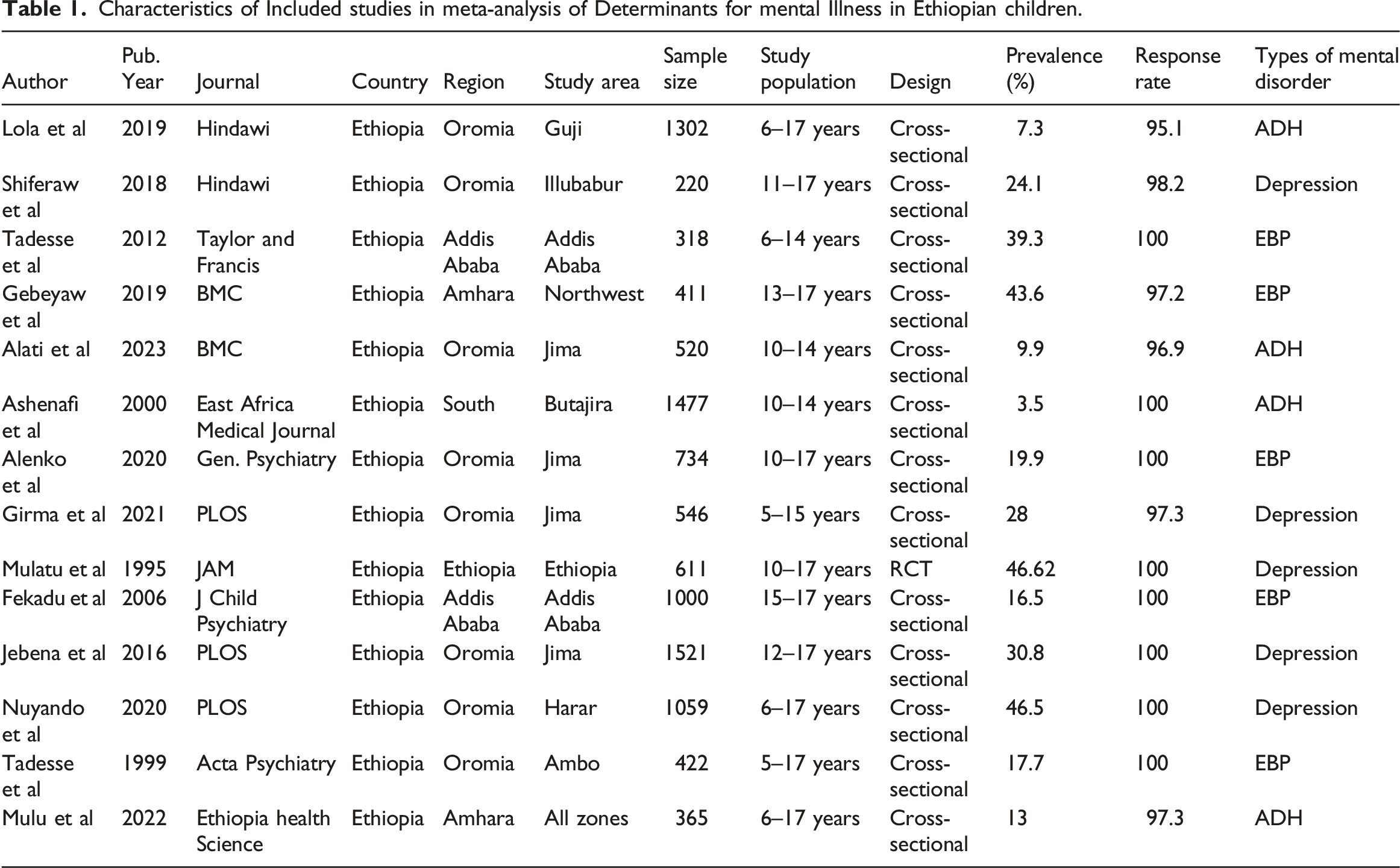
Characteristics of Included studies in meta-analysis of Determinants for mental Illness in Ethiopian children.
Data management and analysis
Attention Deficit Hyperactivity (ADH) among children in Ethiopia
There was evidence of heterogeneity (I2 = 94.4%, p ≤ .001) in the included studies. Therefore, we used a random-effects meta-analysis to estimate the pooled prevalence of ADH in Ethiopian children. The pooled prevalence of ADH in Ethiopian children was 8.16% (95% CI:4.51-11.82) (Figure 2(a)). Pooled prevalence of ADH, EBP, depression, and any mental illness among children in Ethiopia.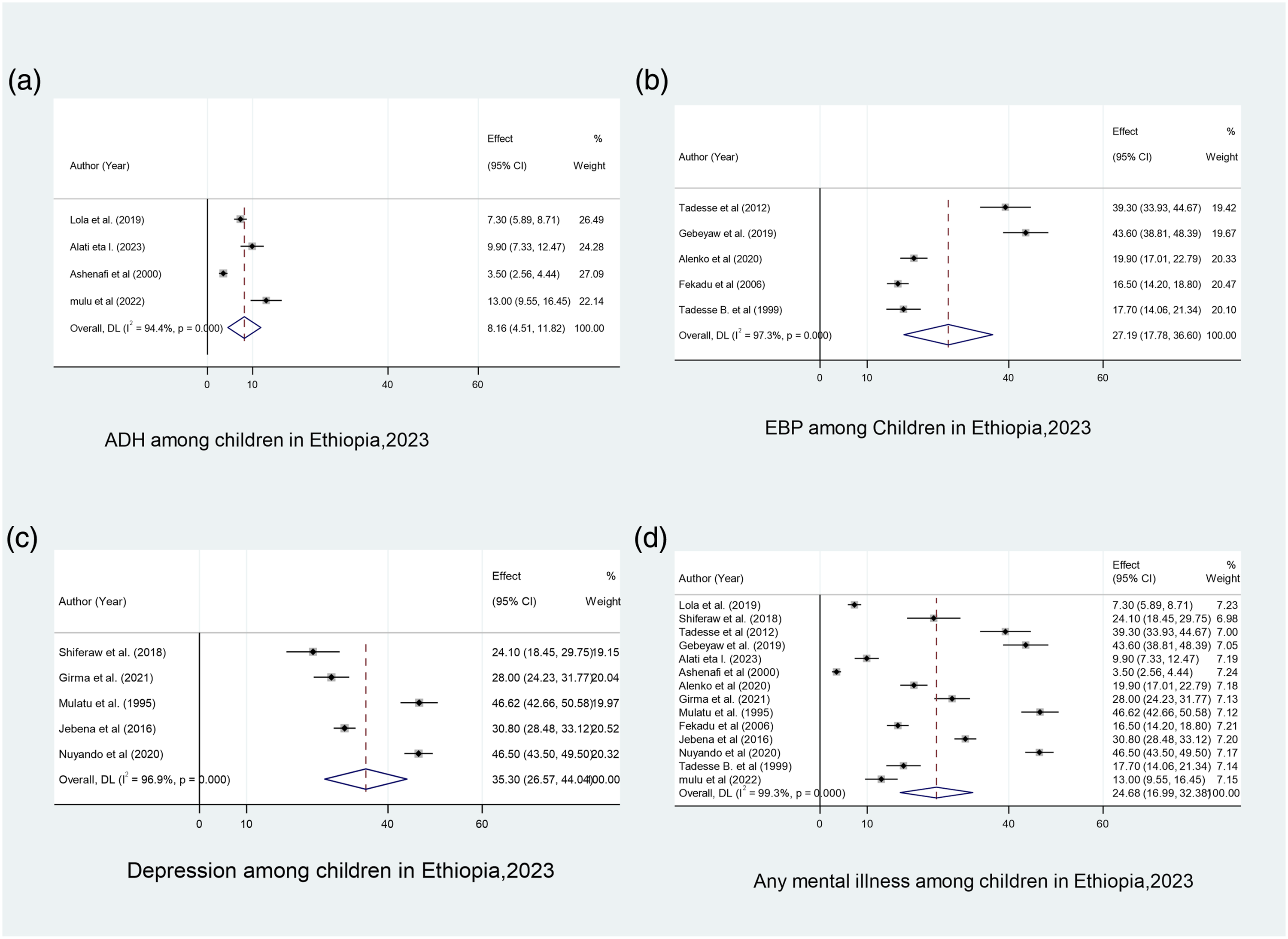
Emotional and behavioral problems (EBP) among children in Ethiopia
Heterogeneity was observed (I2 = 97.3%, p < .001) in the included studies. Therefore, we used a random-effects meta-analysis model to estimate the pooled prevalence of EBP in Ethiopian children. As a result, the pooled prevalence of EBP in Ethiopian children was 27.1% (95% CI:17.78-36.60) (Figure 2(b)).
Depression among children in Ethiopia
Heterogeneity was observed (I2 = 96.9%, p < .001) in the included studies. Therefore, we used a random-effects meta-analysis model to estimate the pooled prevalence of depression among Ethiopian children. The pooled prevalence of depression among Ethiopian children was 35.30% (95% CI:26.56-44.04) (Figure 2(c)).
Any mental illness among children in Ethiopia
There was evidence of heterogeneity (I2 = 99.3%, p ≤ .001) in the included studies. Therefore, we used a random-effects meta-analysis model to estimate the pooled prevalence of mental illnesses among Ethiopian children. The pooled prevalence of mental illness in Ethiopian children was 24.68% (95% CI:19.99-32.38) (Figure 2(d)).
Factors Related to Heterogenicity in studies of any mental Illness Among Ethiopian children (Univariate Meta Regression Model).

Funnel plots and Egger tests were used to assess publication bias. Visual inspection revealed slight asymmetry, indicating publication bias (Figure 3), while the p-value of Egger’s tests was .001, which suggests publication bias. Funnel plot tests for publication bias of studies of any mental illness among Ethiopian children.
Meta trim and fill analysis
Trim-and-fill analysis were used to remove extremely small studies from one side of the funnel plot (Figure 4). Meta trim and fill analysis of studies of any mental illness among Ethiopian children.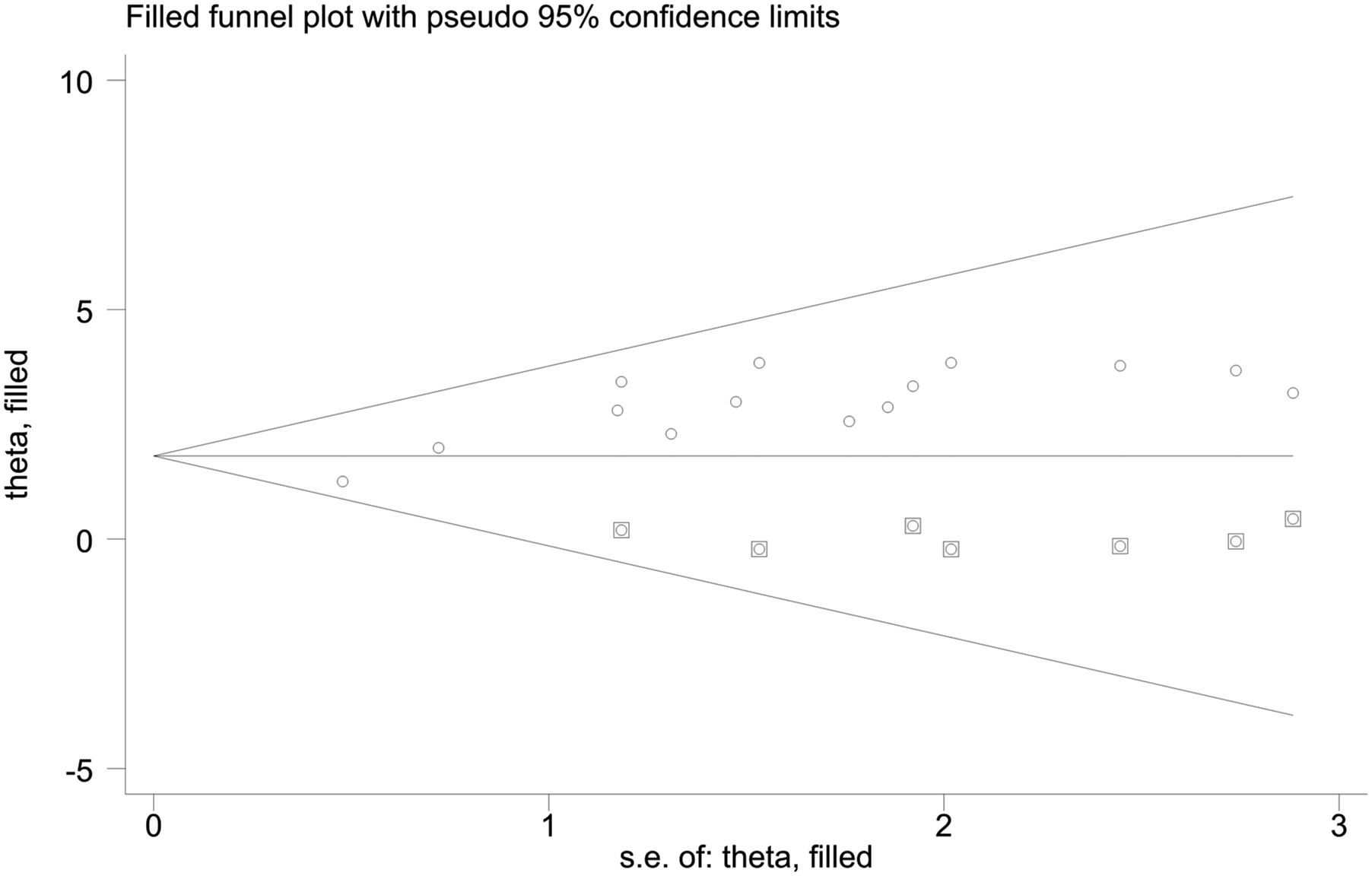
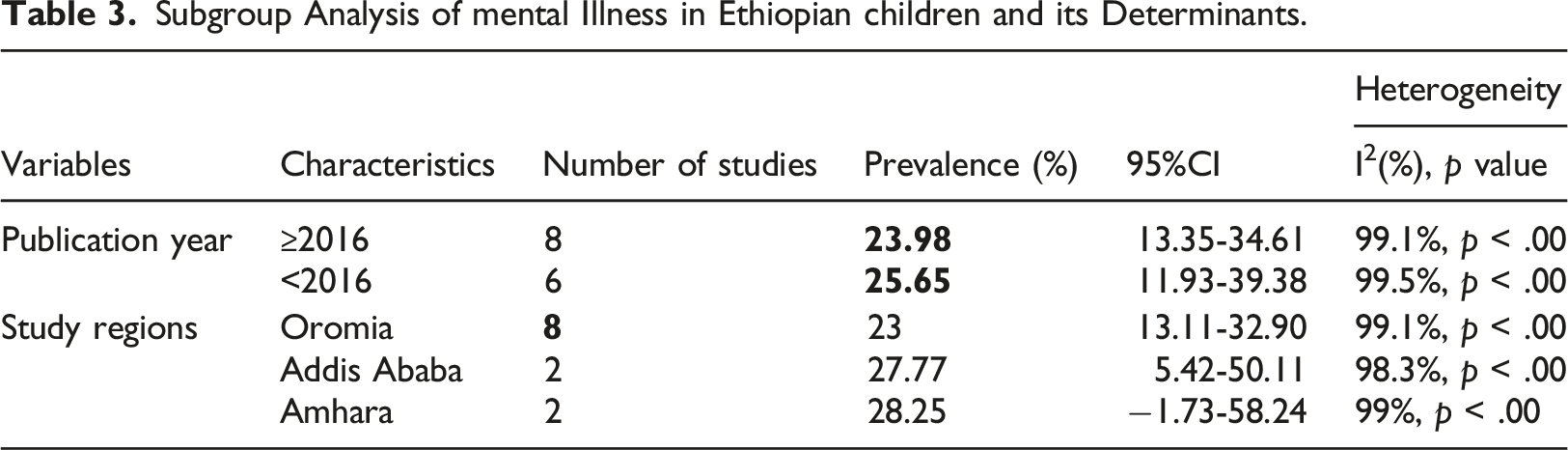
Subgroup analysis
Subgroup Analysis of mental Illness in Ethiopian children and its Determinants.
Sensitivity analysis
Sensitivity analysis was used to show how a single study affected the overall meta-analysis. Thus, sensitivity analysis revealed that our findings were strong and did not rely on a single study (Figure 5). Sensitivity analysis of studies of any mental illness among Ethiopian children.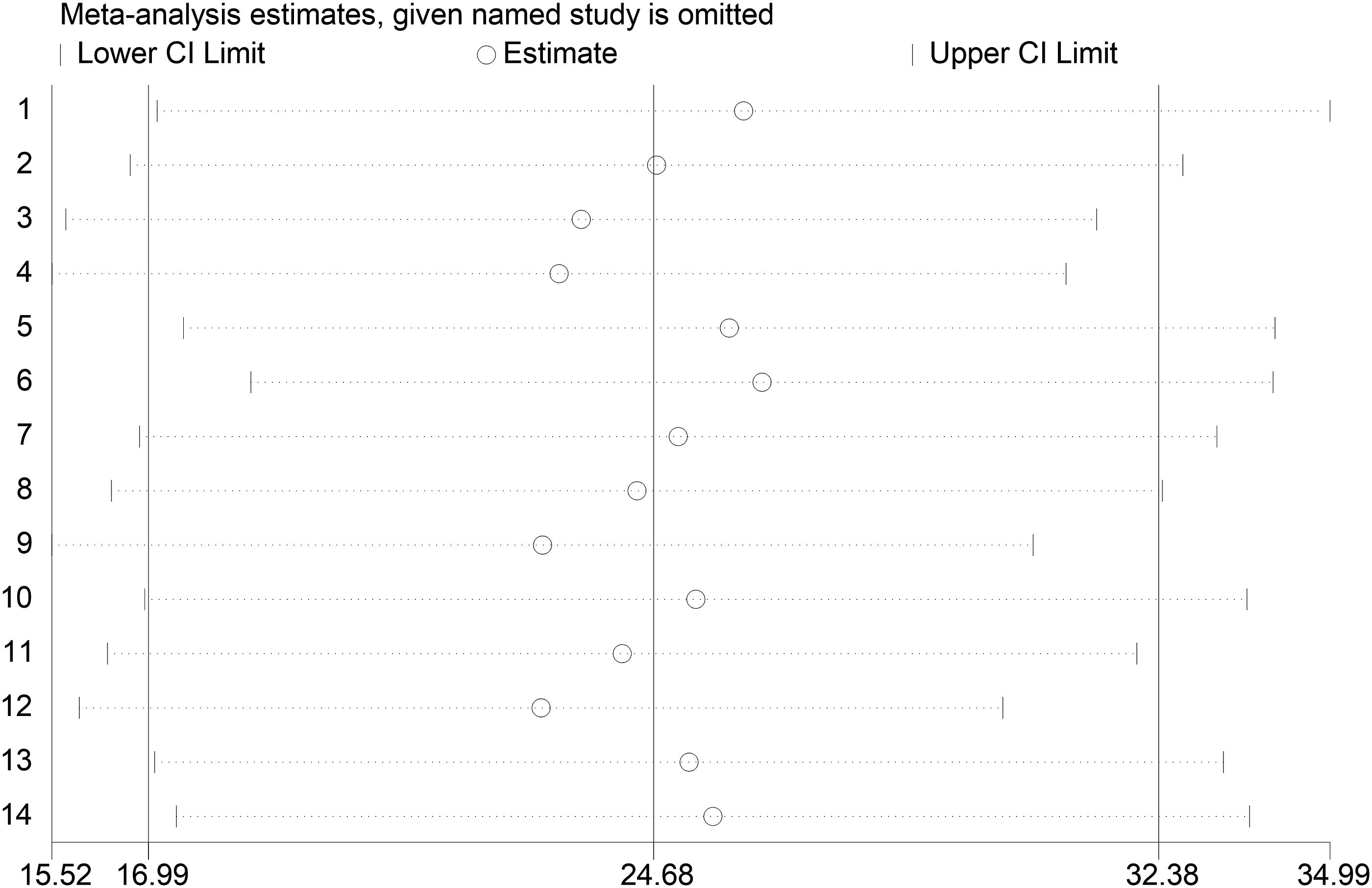
Associated factors of any mental illness among children in Ethiopia
Our research identified four predictive factors associated with mental illness in Ethiopian children:
Sexual abuse history
Four studies (Shiferaw et al., 2018; Mulu et al., 2022; Alenko et al., 2020; Fekadu et al., 2006) with 2,319 respondents were included to assess the association between childhood sexual abuse and mental illness among children in Ethiopia. The results showed that children who experienced abuse were 5.65 times more likely (OR:5.65; 95% CI:4.32-7.39) to experience mental illness than their counterparts (Figure 6(a)). Associated factors of any mental illness among Ethiopian children.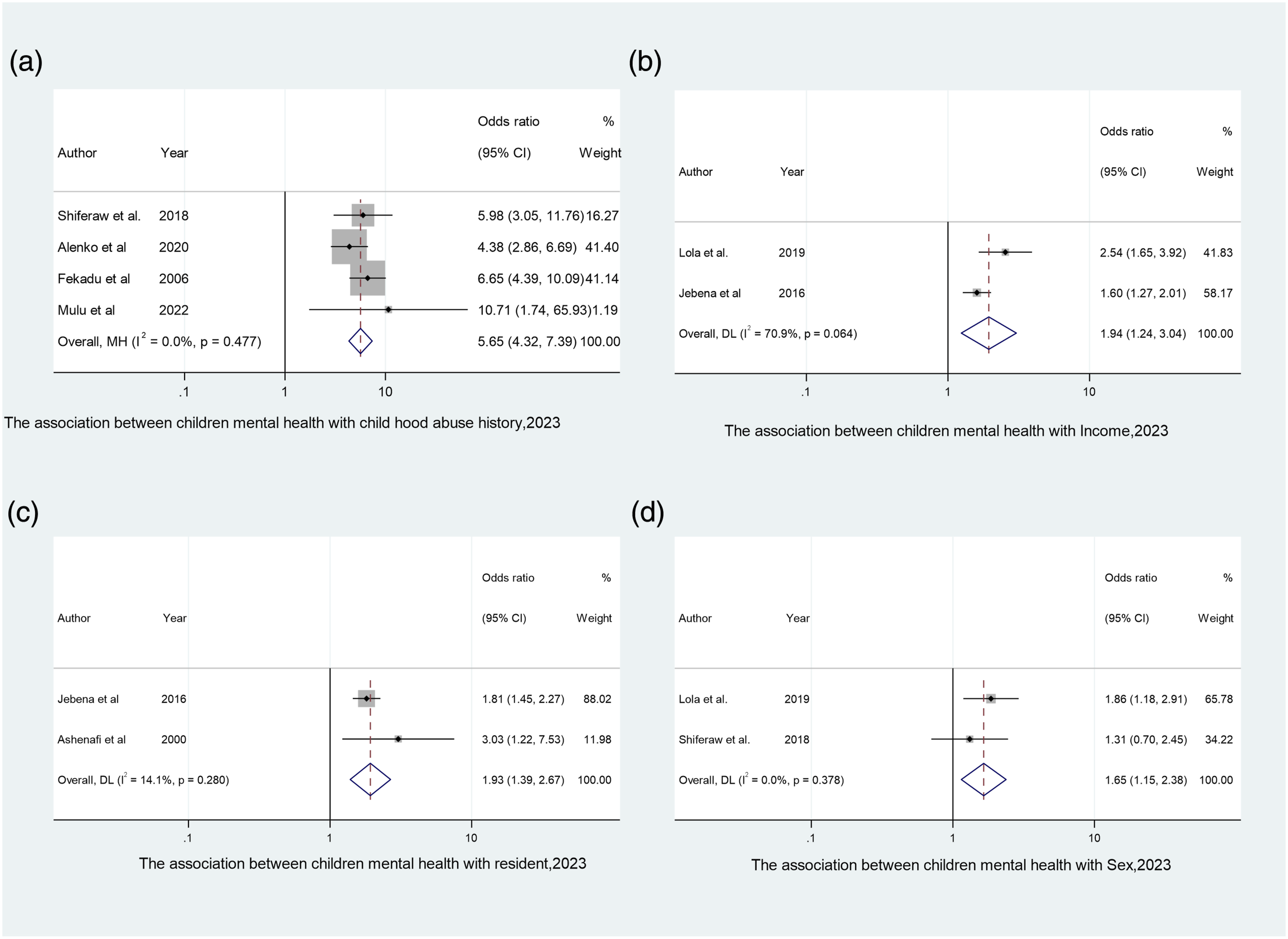
Parental socio-economic status
Two studies (Lola & Belete, 2019; Jebena et al., 2016) with 2,823 respondents were included to assess the association between socio-economic status and mental illness among children in Ethiopia. The results showed that children from low socio-economic status were 1.94 times more likely (OR:1.94; 95% CI:1.24-3.04) to experience any mental illness than children come from high socio-economic status (Figure 6(b)).
Resident and any mental illness among children
Two studies (Ashenafi et al., 2000; Jebena et al., 2016) with 2,998 respondents were included to assess the association between area of residence and mental illness among children in Ethiopia. The results showed that children who reside in urban areas were 1.93 time more likely (OR:1.93; 95% CI:1.39-2.67) to experience mental illness than children who resides in rural areas (Figure 6(c)).
Gender and any mental illness among children
Two studies (Lola & Belete, 2019; Shiferaw et al., 2018) with 1,522 respondents were conducted to assess the association between gender and mental illness among children in Ethiopia. Male children were 1.65 times more likely (OR:1.65; 95% CI:1.15-2.38) to experience any mental illness than female children (Figure 6(d)).
Discussion
The overall prevalence of mental illness in children was 26.25% (17.56–34.93%). This finding was higher than that of systematic reviews conducted in Europe and 11 high-income countries, which found that the pooled prevalence of any mental disorder was 15.5% (95% CI 9.4–24.5%, I2 = 99.8%) and 12.7% (95% CI 10.1%–15.9%, I2 = 99.1%), respectively (Sacco, 2022; Jenny Lou, 2022). This disparity may be related to socio-demographic differences and standard living conditions, as Europe and other industrialized countries have different childcare systems than Ethiopia.
However, the prevalence in this study was lower than that of a systematic review conducted in France, which reported a pooled prevalence of mental illness among children of 49% (43%–54%) (Bronsard et al., 2016). This discrepancy may be due to socio-demographic differences and the influence of Coronavirus Disease 2019 (COVID-19) in European countries Since this study included all researches conducted at and before 2023.
In this study, the pooled prevalence of ADH among children was 8.16% (95% CI: 4.51%–11.82%). This result was slightly higher than that of systematic reviews conducted in China, Europe, and other high-income nations, which found that the national-pooled prevalence of ADHD in children was 5.7% (95% CI: 4.9%–6.6%), 2.9% (95% CI: 1.2%–6.9%), and 3.7% (95% CI: 2.3%–5.7%), respectively (Lian et al., 2013; Sacco, 2022; Jenny Lou, 2022). In addition to socio-demographic variables and sample size discrepancies, this gap may be attributed to differences in research design and ADH evaluation techniques
In this review, the pooled prevalence of EBPs was found to be 27.19% (95% CI: 17.76%–36.60%). This is greater than the prevalence of EBPs reported by teachers in Nepal (15.4%), whereas the previously reported parental rate was 19.1% (Mahat et al., 2021). This disparity may be caused by socio-economic differences and discrepancies in the techniques used to assess EBP. In comparison, the prevalence of EBP was found to be 41.4% in a study conducted in northern Uganda (Jörns-Presentati et al., 2021). This disparity may be attributed to socio-demographic differences.
The pooled prevalence of depression was 35.30% (95% CI: 26.57%–44.04%). This finding was higher than studies conducted in South Africa and on child welfare in industrialized countries, Ireland, and Europe, which indicated a lifetime prevalence of depression among children of 2.6%, 18%, 20.8%, and 1.7%, respectively (Jörns-Presentati et al., 2021; Sacco, 2022; Bronsard et al., 2016; Lynch et al., 2022). This disparity could be attributed to socio-demographic differences and standard living circumstances.
Male sex has been linked to mental disorders in Ethiopian children. In keeping with this finding, systematic studies conducted in the Middle East, United States, Belgium, and United Kingdom indicated that boys are more likely to suffer from mental illness (Dimitry, 2012; Martin & Hadwin, 2022; Van Droogenbroeck et al., 2018; Yoon, 2022). This might be because boys have a greater tendency to struggle with anger, engage in risky behaviors, and attempt suicide than girls. Teenage girls are more likely to want to express their emotions by crying or interacting with their peers, whereas teenage boys have more difficulty articulating their sentiments and prefer to separate themselves from others when they worry too much(Otten et al., 2021).
Children from families with lower socio-economic status were more likely to suffer from mental illness than those from families with higher status. Similarly, a study conducted in Norway (Kinge et al., 2021), a systematic review conducted in low- and middle-income countries (Ribeiro et al., 2023), and a systematic review conducted during the COVID-19 pandemic (Stracke et al., 2023) all found that children’s mental health was related to their parents' socio-economic status. This could be because a low socio-economic status causes social stress and stigma, both of which contribute to poor mental health.
This systematic review and meta-analysis also revealed that children living in cities were more likely to suffer from mental illness than those living in rural areas. Studies undertaken in Denmark (Engemann et al., 2019), Berlin (Gruebner et al., 2017), and Brussels (Pelgrims et al., 2021) also revealed that living in cities was connected with mental disorders in children. This could be because urban settings are associated with several risk factors for mental illness such as noise, environmental pollutants, criminal activity, and hazardous substances.
Children who had previously been abused were more likely to develop mental illnesses than their peers. Studies conducted in Canada (Su et al., 2022), the USA (Lippard & Nemeroff, 2020), China (Zhao, 2019), and Korea (Ha & Kim, 2023) also found that survivors of child abuse were more likely to experience mental illnesses. Abuse can cause survivors to experience feelings of loneliness, anxiety, and insecurity, which can lead to lasting psychological consequences such as academic difficulties, a lack of self-worth, sadness, and trouble in forming and sustaining relationships (Khoury et al., 2010).
Limitations of the study
This systematic review and meta-analysis had some limitations. Our study only included cross-sectional studies that is impossible to establish a cause-and-effect relationship or to analyze behaviors across time. It is advised that cohort and case–control studies be done.
Conclusion and recommendations
There was a high frequency of mental disorders among children. In Ethiopia, a history of child abuse, low socio-economic status, urban residence, and male sex were all associated with childhood mental illness. Interventions focusing on gender equality education, supporting children from low socio-economic backgrounds, and creating a healthy atmosphere for children living in urban areas are recommended. Additionally, the government might support organizations that help children who have been victims of child abuse, and a strong legislative body should be established to punish child abuse.
Footnotes
Acknowledgments
We would like to thank all the authors of the primary studies analyzed in this research.
Author Contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.