
Abstract
Objective:
In this discussion, we build the case for why climate change is an emerging threat to perinatal mental health.
Method:
A search of current literature on perinatal and maternal mental health and extreme weather events was conducted in PubMed/MEDLINE and Web of Science databases. Only articles focusing on maternal mental health were included in this narrative review.
Results:
The perinatal period represents a potentially challenging timeframe for women for several reasons. Necessary role adjustments (reprioritization), changes in one’s ability to access pre-birth levels (and types) of social support, fluctuating hormones, changes in body shape, and possible complications during pregnancy, childbirth, or postpartum are just a few of the factors that can impact perinatal mental health. Trauma is also a risk factor for negative mood symptoms and can be experienced as the result of many different types of events, including exposure to extreme weather/natural disasters.
Conclusion:
While the concepts of “eco-anxiety,” “climate despair,” and “climate anxiety” have garnered attention in the mainstream media, there is little to no discussion of how the climate crisis impacts maternal mental health. This is an important omission as the mother’s mental health impacts the family unit as a whole.
Keywords
The perinatal period is a time of increased vulnerability to negative mood symptoms due to various changes within the mother and her environment (Barkin et al., 2010). Fluctuations in hormone levels, changes in body shape, and potential complications during pregnancy, childbirth, or the postpartum period are just a few biological factors that can negatively impact mood (Hartley et al., 2017; Yim et al., 2015). Socially and psychologically, the mother is adapting to new circumstances, including potential modifications in her ability to access adequate social support and disruption in her prebirth activities (Barkin et al., 2014). Likely, her daily routine is either temporarily or permanently upended to support and nurture a new life.
For these reasons and more, perinatal mood and anxiety disorders (PMADs) are the most common complication of childbirth with upward of one in five women affected (Wisner et al., 2013). Although PMADs is an umbrella term that refers to several conditions including perinatal obsessive-compulsive disorder, posttraumatic stress disorder, and postpartum psychosis (Center for Women’s Mood Disorders, 2022), perinatal depression and anxiety are by far the most common maladies ranging from 10% to 20% (Van Niel & Payne, 2020) and 16% to 17% (Fairbrother et al., 2016) impacted, respectfully. PMADs are also associated with considerable cost to society and public health burden; a recent study by Mathematica indicated a cost of $14.2 billion for untreated PMADs for all U.S. births in 2017 (“New Study Uncovers the Heavy Financial Toll of Untreated Maternal Mental Health Conditions,” 2019). Stated differently, the average cost for each affected (but untreated) mother-child dyad was estimated at US$32,000.
Among the myriad risk factors that predispose women to the development of PMADs is having experienced trauma (de Graaff et al., 2018). While there are various types of life events that qualify as traumatic (Weathers et al., 2013), the focus of this discussion is trauma borne of exposure to extreme weather events (EWEs; Table 1). EWEs are becoming more frequent, intense, and difficult to predict as the climate crisis progresses (Barkin et al., 2021). Experts have described climate change (Table 1) as the “greatest threat to global public health (Atwoli et al., 2021), and the United Nations Refugee Agency estimates that 24.9 million individuals were displaced (worldwide) due to extreme weather in 2019; this number is expected to grow to 200 million each year by 2050 without swift intervention (Gaynor, 2020). In addition, the Office of the United Nations High Commissioner for Human Rights (OHCHR) estimates that women comprise approximately 80% of those displaced (Office of the United Nations High Commissioner for Human Rights, 2022). Disruption of social support networks, health care, employment, and childhood education are all possible downstream effects that exact a significant toll on mental health (Clark-Ginsberg et al., 2021).
Glossary of Climate Change-Related Concepts.
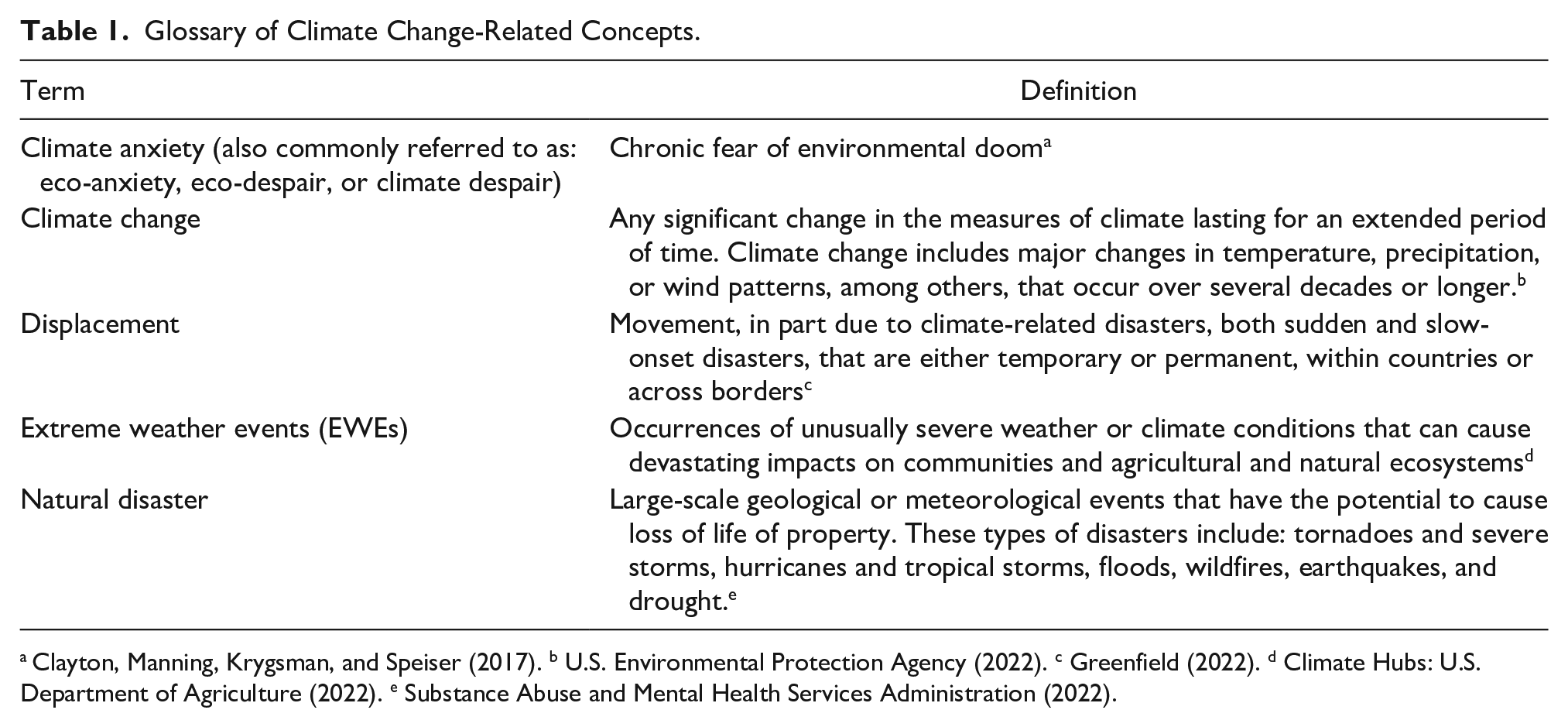
While concepts such as, “eco-anxiety,” “eco-despair,” and “climate anxiety” (Table 1) now have a presence in the mainstream media (Simon & Schneider, 2022; Thompson, 2021), the pool of related, peer-reviewed research is still relatively shallow. In terms of the mental health effects of climate change, the child population has been a primary focus (Barkin et al., 2021), while the impacts on pregnant and postpartum women have exacted less attention. Coincidentally, this is a common complaint of perinatal mental health researchers who have referred to the mother as the wrapper that gets “tossed aside” once the baby (the candy) is delivered (Barkin et al., 2022). However, in regard to climate, it is a mistake to only partially examine the plight of perinatal women as the mother’s health and well-being are inextricably linked to family health (Barkin & Wisner, 2013). In addition, as presently discussed, the available data suggests a significant impact of EWE exposure on perinatal mental health and warrants further investigation and investment (Harville, Xiong, & Buekens, 2010; Verstraeten et al., 2020). Considering that nurses constitute the largest subgroup of the global health care workforce (Veenema et al., 2017) and are consistently rated as the most trusted class of professional (Gaines, 2022), they have the potential to make unique contributions to curtailing the climate crisis. Nurses could leverage their collective voices to advocate for both improved disaster preparedness protocols/infrastructure and stronger environmental policies (Veenema et al., 2017). The growing recognition of eco-anxiety and despair is particularly relevant to psychiatric nurse practitioners who are in a position to directly affect related patient care. Pertaining to this discussion, the term “EWE” refers to a wide range of potential weather events including extreme heat, drought, flooding, wildfires, and storms (Veenema et al., 2017).
EWE-Exposed Women Have Explicitly Described Their Worries
In several qualitative studies, women who were exposed to EWEs during pregnancy identified and described specific fears and anxieties that impacted their mood during or after the event (Badakhsh et al., 2010; Giarratano et al., 2019; Sato et al., 2016). As seen below, women cited a vast array of concerns, highlighting the complexities in enduring a natural disaster (and potential displacement;
disruption of life during pregnancy
health of the developing fetus
newborn health
general uncertainty
“destruction of normalcy”
fears of food insecurity
threatened access to health care (both prenatally and for the family)
financial and housing worries
worry about family separation
the evacuation process
sanitary conditions in evacuation centers
The fact that women have expressed fears regarding personal and family health is unsurprising as women are most often the primary family health advocates and caregivers (Barkin et al., 2010). This drive to safeguard one’s self and family may also (at least partially) explain why women have repeatedly been identified as leaders in the fight against climate change (Peel et al., 2022; Sengupta, 2021; UN Women, 2022).
Negative Mental Health Impacts Have Been Quantified in the Perinatal Population
The available quantitative data also indicates an association between EWE exposure and negative mental health outcomes. Relative to the child population (Barkin et al., 2021) and in general, EWE-related posttraumatic stress (PTS)/posttraumatic stress disorder (PTSD) has not been extensively studied in the perinatal population. This may be partially attributed to an overwhelming focus on the constructs of maternal distress and stress surrounding disaster recovery (King et al., 2015; King & Laplante, 2005) and the more pervasive societal issue of inadequate interest in maternal mental health (Barkin et al., 2022). However, as one would expect, there are indications that PTS/PTSD is also experienced by pregnant and postpartum women who have endured extreme weather (Harville, Xiong, & Buekens, 2010; Verstraeten et al., 2020). In fact, Verstraeten et al. (2020) found that, of 200 wildfire survivors, 50% qualified as “possible” or “probable” for PTSD; the participants were either pregnant or in the early postpartum when they experienced the Fort McMurray Wood Buffalo wildfire in Alberta, Canada. However, Harville et al. (2010a) note that level of personal resilience is protective against the development of PTSD (Harville, Xiong, Buekens, Pridjian, & Elkind-Hirsch, 2010b).
Heightened levels of depression and anxiety have also been observed in the perinatal population; this effect is most pronounced where exposure level is greatest (Brock et al., 2015; Ehrlich et al., 2010; Paquin et al., 2021). Specifically, those who incur greater loss and have a more intense experience are at increased risk of impaired mood including depression and anxiety. Being in close proximity to the event (e.g., wading through flood waters, inhaling wildfire smoke), experiencing negative health and/or economic setbacks, and disruption of social support networks are common, distressing events associated with natural disaster exposure (Barkin et al., 2021).
There is also a growing body of evidence that supports an association between EWE-related maternal stress/distress and an array of negative child health outcomes (Dancause et al., 2011, 2015; Laplante et al., 2015; Nguyen et al., 2018). Specifically, maternal stress/distress (in the context of disaster) has been linked to childhood adiposity (Dancause et al., 2011, 2015; Kroska et al., 2017; Liu et al., 2016), poorer infant temperament (Laplante et al., 2015), impaired cognitive/motor development (Cao et al., 2014; Moss et al., 2017; Simcock et al., 2017, 2018), and HPA-axis dysregulation (Nguyen et al., 2018). These findings are complementary of the broader perinatal mental health literature in which postpartum depression has been linked to negative behavioral and cognitive (child) outcomes from infancy through the school-aged years (Bernard-Bonnin, 2004; Wisner et al., 2013).
Conclusion and Next Steps
EWE exposure represents a trauma that can instigate negative mood symptoms and compound the already challenging transition to motherhood. As a result, our changing climate is highly relevant to clinicians including obstetric and pediatric providers who are tasked with evaluating women for perinatal depression and anxiety. As the effects of climate change continue to broaden geographically, more patients will be affected, requiring providers to screen for mental wellness and adjust their advisement and approaches with environmental factors in mind. Women who have experienced displacement may require care from providers outside of their medical home. However, evidence to inform a standard approach to tackling the downstream effects of displacement in the perinatal period is lacking.
Established organizations with effective programs for supporting women in the perinatal period such as Postpartum Support International (PSI, 2021) should consider the incorporation of climate change into their programming/strategic planning. For example, PSI is the facilitator of 20+ support groups including those designed for Black moms, South-Asian moms, teenage moms, military moms, neonatal intensive care unit parents, queer and transgender parents, and women who have experienced pregnancy/infant loss. Mothers with obsessive compulsive disorder, postpartum psychosis, and other mood symptoms are also supported by PSI; a support group for women displaced due to climate change could be added to this collection of tools. Given the importance of personal resilience in the recovery process (Barkin et al., 2021; Sprague et al., 2015), new tools/supports should foster improved coping skills and positive reframing of the event.
In addition, as part of a U.S. Health Resources and Services Administration (HRSA) funded collaboration, PSI has launched the National Maternal Mental Health Hotline (“HHS Launches New Maternal Mental Health Hotline,” 2022). The toll-free hotline is available 365 days a year, 24/7, and in English and Spanish languages. HRSA administrator Carole Johnson stated in a 2022 press release, “we are creating a safe space for expecting and new moms who are experiencing maternal depression, anxiety or other mental health concerns to have confidential conversations and get the support they need” (U.S. Department of Health & Human Services, 2022). Both peer support groups and the National Maternal Mental Health Hotline could be leveraged (or tailored) to support women who have survived extreme weather events in the perinatal period. Considering the scale of the climate crisis and its potential to impact human health and women in particular (Haigh & Vallely, 2010), plans for future mental health programming should be designed with climate change (as a risk factor) in mind.
Leveraging the Trusted Voice of Nurses in the Communication of Climate-Related Health Risks
Nurses have been ranked as the most honest and ethical professionals for 20 consecutive years (Gaines, 2022). Consequently, they have the potential to play a powerful role in educating the public (and other providers) regarding the health risks associated with climate change/extreme weather (Barkin et al., 2022). In terms of current advocacy efforts, the Alliance of Nurses for Healthy Environments (2021) has partnered with Health Care Without Harm (2021) to educate other providers regarding the related health risks (Nurses Climate Challenge, 2021), which are broad in range and impact multiple organ systems (Schraufnagel et al., 2019). To ensure that future nurses are well-versed regarding the physical and mental health effects of climate change, related content should be considered for infusion into the core nursing curriculum; to date, climate change has not been given adequate attention in this capacity (Lopez-Medina et al., 2019). Furthermore, leadership at all institutions that train health professionals, including schools of public health, should strongly consider adding climate-related courses into their academic offerings.
Due to their role in assessing, diagnosing, and treating mental illness (American Association of Nurse Practitioners, 2019), psychiatric nurse practitioners have the opportunity to broach topics (with their patients) that influence both mental health and physical health. For example, perinatal women should be counseled regarding the impacts of extreme heat on both mood (Clayton et al., 2017) and pregnancy/birth outcomes (Barreca & Schaller, 2019; Olson & Metz, 2020; Poursafa et al., 2015). Similar to the “Whole of Government” approach, the entire health care workforce should likewise be engaged in the fight against what has been repeatedly described as, “the greatest threat to human health in recorded history”—the climate crisis (United Nations, 2021).
Footnotes
Acknowledgements
The authors would like to acknowledge the unwavering support of the Georgia Clinicians for Climate Action (GCCA), the Medical Society Consortium on Climate and Health, Georgia Interfaith Power & Light (GIPL), and the Southeast Climate & Energy Network (SCEN).
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data; drafted the manuscript or critically revised the manuscript; gave final approval of the version that was submitted for publication; and agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received funding from the Georgia Department of Public Health to support this work.