
Abstract
Canadian Indigenous women often experience severe partner violence and child abuse, but few studies holistically examine risk and protective factors and evidence of resilience that affect their well-being. This mixed-methods secondary analysis explored the experiences of 40 Canadian Indigenous abused women. Risk factors included intimate partner violence (IPV), childhood abuse, poverty, colonization, and disability. Protective factors included formal and informal support, community support, spirituality, and childhood residence. Evidence of resilience is from interview quotes and none of the measures of depression, mental distress, and posttraumatic stress disorder was in the clinical range. Despite significant IPV and childhood abuse, the women's resilience is highlighted.
In Canada, intimate partner violence (IPV) against Indigenous women is a significant issue, with IPV rates three times higher than non-Indigenous women (21% to 7%; Brownridge, 2008; Johnson, 2006). Further, Indigenous women across North America are commonly abused by severe and potentially life-threatening forms of violence such as being strangled, having a gun or knife used against them, and being sexually assaulted or stalked (Brownridge, 2008; Guggisberg, 2019; McKinley, 2022; Romans et al., 2007). They are more likely to have been injured because of their partners' physical assaults, to have needed medical attention, and less likely to maintain their daily routines (Johnson, 2006).
Further, Johnson (2006) concluded that Indigenous women were more likely to be afraid that their partner might kill them as compared to non-Indigenous women. Indeed, Indigenous women were 8 times more likely to have been murdered by their intimate partners than non-Indigenous women (Brownridge, 2008; Johnson, 2006). Finally, women who leave abusive partners are at significant risk of continued harm, yet the risks of leaving are even greater for Indigenous women. Brownridge (2006a) estimated that 45.5% of Indigenous women have been abused by former partners compared to 9.8% of non-Indigenous women.
While Indigenous people generally have higher rates of mental health problems than non-Indigenous Canadians (Nelson & Wilson, 2017; Söchting et al., 2007), the few studies about Indigenous women affected by IPV also suggest significant mental health difficulties such as depression (Evans-Campbell et al., 2006; Schultz et al., 2021), posttraumatic stress disorder (PTSD) and psychological distress (Tutty et al., 2020). Several qualitative studies (Burnette & Cannon, 2014; Hoffart & Jones, 2018) describe such mental health problems as PTSD, depression, and suicidal ideation.
Speculation about what factors place Indigenous women at greater risk for IPV concurs that the legacy of colonization is central, by disrupting traditional values and culture, using residential schools to break down family life, spiritual beliefs, and languages, systemic discrimination, and racism (Andersson et al., 2010; Baskin, 2012, 2020; Brave Heart et al., 2011; National Inquiry into Missing and Murdered Indigenous Women and Girls, 2019; Olsen Harper, 2011; Wilk et al., 2017; Williams et al., 2019). As one example, while only 5% of Canadian children are Indigenous, they represent 22% of substantiated child maltreatment cases. Indigenous children are overrepresented in the child protection system (Blackstock et al., 2004), being 12 times more likely to be placed in foster care than non-Indigenous children (Trocmé et al., 2010). Considering both child maltreatment and IPV against Indigenous women (21%), many have experienced trauma in their lifetimes, the effects of which are typically cumulative (Collin-Vezina et al., 2009; Finkelhor et al., 2007; Söchting et al., 2007).
In summary, authors agree that colonization is central to abuse against Canadian Indigenous women by disrupting traditional values and culture, using residential schools to break down family life, spiritual beliefs, and languages, as well as systemic discrimination, and racism (Andersson et al., 2010; Brownridge, 2008; Johnson, 2006; Olsen Harper, 2011). The current secondary analysis examined the experiences of 40 Indigenous Canadian women abused by intimate partners, looking at the broader contexts of their lives including issues of mental health, colonization, risk and protective factors, and evidence of resilience.
The Ecosystemic Framework of Historical Oppression, Resilience, and Transcendence
Specific to Indigenous peoples, Burnette and Figley (2017) developed the “Ecosystemic Framework of Historical Oppression, Resilience, and Transcendence” in research related to Indigenous peoples in the United States. It considers both oppressive historical conditions, such as colonization, and those of the present, such as discrimination, in explaining the current problem of IPV. Similar to Heise's (1998) ecological framework, the framework proposes nesting risk and protective factors at the individual level with those at the couple and family level, which are, in turn, embedded within those at the level of community and culture, which are embedded within those at the societal level (Burnette & Figley, 2017). It can be applied in the Canadian context as it allows for variation in the specifics of both historical and local conditions.
Risk factors emanate from a variety of sources that could occur anywhere in one's environment including the individual, family, and community/society (Luthar & Cicchetti, 2000). Indigenous people tend to experience greater risk factors than non-Indigenous Canadians (Olsen Harper, 2011). Peoples of Indigenous backgrounds have additional risks associated with genocide, historical and current colonialism, racialized violence, stereotyping, systemic oppression, and social exclusion (Brave Heart et al., 2011; Burnette, 2016; Olsen Harper, 2006, 2011; Pedersen et al., 2013). These risk factors represent traumatic circumstances, suggesting that the respondents have experienced polyvictimization and intergenerational trauma. Brave Heart et al. (2011) state that Indigenous peoples are facing historical trauma, which is defined as “cumulative emotional and psychological wounding across generations … which emanates from massive group trauma” (p. 283).
Western scholars identify protective factors in three categories: individual, family, and community (Anderson et al., 2012; Luthar & Cicchetti, 2000; Olsen Harper, 2011). Yet, for Indigenous peoples, protective factors need to be viewed relationally and holistically (Olsen Harper, 2011; Ungar, 2013). In two American studies, Anderson et al. (2012) and Humphreys (2003) examined the resilience of Indigenous women abused by their intimate partners. Individual protective factors were the women's sense of spirituality, strength, determination, intelligence, and ability to problem-solve. As Anderson et al. (2012) concluded, the participants’ belief in a higher power helped them deal with their suffering and believe that their lives had a greater purpose. Emotional support from family members was also a protective factor. At the community level, protective factors included emotional support from friends and employers, as well as formal support services from domestic violence and mental health services.
Several scholars focus on culture and diversity as protective factors (Burnette, 2018; Olsen Harper, 2011; Tousignant & Sioui, 2009; Ungar, 2013), suggesting that how families and communities respond to trauma-related symptoms is influenced by what the culture values and determines as relevant. Hence, the social environment is considered to have a pivotal role in what protective factors promote resiliency (Tousignant & Sioui, 2009).
With the potentially devastating negative impacts of IPV, child abuse, and colonization on the mental health of Indigenous women, it would be simple to stereotype them as all having significant issues that impact their lives. Nevertheless, many Indigenous women are resilient and lead successful, fulfilling lives, an issue that is rarely addressed, exceptions being Burnette, (2018), Burnette and Hefflinger (2017), and Yuan et al. (2015).
The Concept of Resilience
Many individuals with traumatic personal histories live healthy lives. This observation has given rise to research into resilience, defined as “a dynamic process wherein individuals display positive adaptation despite experiences of significant adversity or trauma” (Luthar & Cicchetti, 2000, p. 858; Anderson et al., 2012; Humphreys, 2003). Luthar and Cicchetti (2000) clarify that resilience does not refer to individual or personality characteristics, but to two constructs within a single term. The construct of adversity, or risk, refers to “negative life circumstances … associated with adjustment difficulties” (p. 858); while “positive adaptation” (also called protective factors) refers to people's ability to be socially competent or successful, appropriate to “stage-salient developmental tasks” (p. 858) whether one is a child or adult.
The resilience of women abused by intimate partners has been studied quantitatively (Carlson et al., 2002; Fedina et al., 2021; Howell et al., 2018; Shilpa & Suman, 2020), qualitatively (Crann & Barata, 2021; Crawford, 2009) and using mixed methods (Anderson et al., 2012). According to Crann and Barata (2016), resilience is determined by three indicators: “the absence of psychopathology (e.g., lack of a clinical diagnosis or scoring below the clinical cutoff on a measure of psychopathology), the presence of resilience proxy measures (e.g., factors associated with resilience, such as self-efficacy or hardiness), and resilience scale scores (e.g., Connor-Davidson Resilience Scale)” (p. 854). Some focus only on protective factors in determining women's resilience after IPV (Anderson et al., 2012; Carlson et al., 2002; Crann & Barata, 2016, 2021; Howell et al., 2018), several noting that risk factors for IPV have been studied extensively.
Among Indigenous people, resilience is viewed holistically by one's ability to achieve balance and is encompassed in spirituality, which reaffirms the interconnection of all life (Olsen Harper, 2011). In summary, protective factors that influence the resilience of Indigenous peoples include identity, family, community, traditional culture, traditional spirituality, healing ceremonies, oral traditions, and wisdom of elders (Burnette, 2018; Olsen Harper, 2011; Tousignant & Sioui, 2009).
Rationale for the Current Study
While considerable research on the characteristics and consequences of IPV for Indigenous women has been conducted, few take a broad ecological perspective that examines issues beyond the individual characteristics of the women. Researchers studying the mental health of Indigenous women affected by IPV seldom use standardized mental health measures (exceptions being Evans-Campbell et al., 2006 and Schultz et al., 2021). Some measures have the advantage of clinical cut-off scores that specify when symptoms are serious enough to require clinical intervention, but these were rarely used (an exception being Giesbrecht et al., 2022). Most IPV measures do not have cut-off scores that differentiate serious IPV from several instances of violence, except for the Composite Abuse Scale (Hegarty et al., 2005) used in the current study and by Tutty et al. (2020) and Giesbrecht et al. (2022). Further, researchers seldom consider the context of colonization on abused Indigenous women except Ogden and Tutty (2023), Burnette (2016), and Mckinley et al. (2021).
Resilience has only recently become of interest to scholars of partner abuse against Indigenous women, except for studies by Burnette (2018), Burnette and Hefflinger (2017), McKinley et al. (2021), and Yuan et al. (2015). Burnette and Figley's (2017) “Ecosystemic Framework of Historical Oppression, Resilience, and Transcendence” implies the need to examine these concepts concurrently, a complicated prospect, perhaps except in qualitative studies. This was the intent of the current secondary research, which has access to considerable information such as demographics, quantitative measures of IPV and mental health and well-being, and themes from qualitative interviews with 40 Indigenous women. These variables will be examined descriptively for their fit with the risk and protective factors and evidence for resilience discussed previously.
Method
Participants were recruited from agencies that provide services to abused women across the three Canadian prairie provinces. The inclusion criteria were women who were: (a) 18 years or older; (b) have experienced IPV in the previous 5 years; (c) not suffering from a major mental health problem that would impair their comprehension or memory such as hallucinations; and (d) not currently in crisis, defined as the last IPV incident was at least 3 months ago.
Mixed-methods studies include both quantitative and qualitative components (Bergman, 2011; Doyle et al., 2016). The quantitative component consisted of in-depth surveys and self-report measures to assess health, mental health, and well-being. Several questions were about the women's satisfaction with social support from friends and family, community support and spirituality (see Table 3). Trained interviewers conducted the surveys with participants every 6 months over 3½ years.
Questions on Social Support, Community, and Spirituality.a
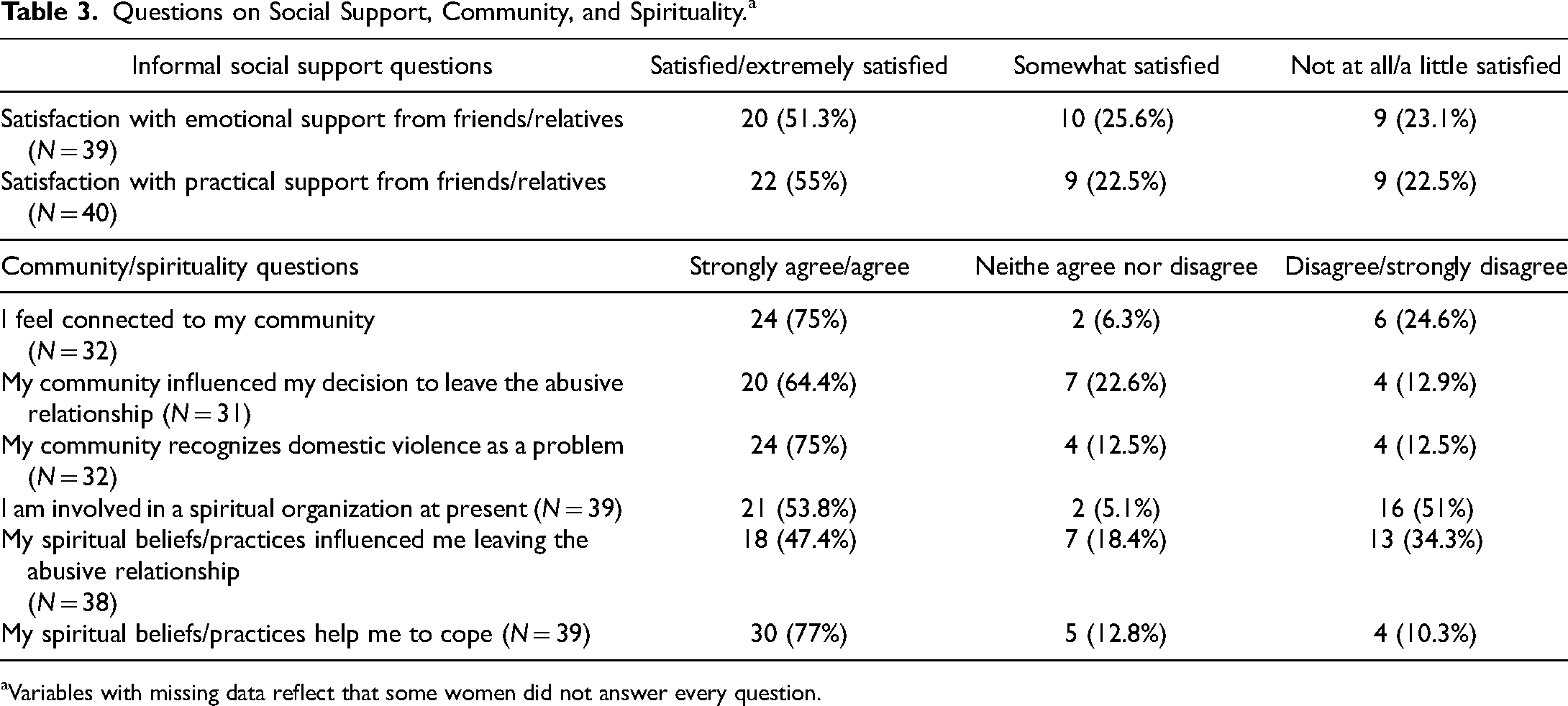
Variables with missing data reflect that some women did not answer every question.
Semistructured qualitative interviews were conducted with a subsample of 91 women, 40 of whom were Indigenous, the focus of the current analysis. Whenever possible, the research assistants (all female) who administered the survey questions also conducted the interviews, which were tape-recorded and transcribed verbatim. Each participant was asked about her relationship with her abusive partner, how she coped, whether she had support, what her life is like now, and what she envisioned for her life in the next 5 years. If Indigenous women did not mention the influence of their racial background, the following was asked, “You haven’t said whether being Indigenous was part of the violence you experienced. If yes, tell me more.” Notably, the interview guide did not include questions about historical oppression or resilience.
Standardized Measures
The Composite Abuse Scale (CAS; Hegarty et al., 2005) is a 30-item self-report measure of partner violence with four subscales: Severe Combined Abuse, Emotional Abuse, Physical Abuse, and Harassment as well as a Total CAS score. The items reference whether partners took certain actions (past 12 months), and the frequency of such actions on a 6-point Likert scale of never (0), only once (1), several times (2), once per month (3), once per week (4), or daily (5). Scores for the subscales and total measure are summed for a total score of from 0 to 150 (Hegarty et al., 2005) with higher scores indicating more serious IPV. The clinical cut-off for the entire scale is 3 to 7 (Hegarty et al., 2005). The CAS has strong criterion and construct validity, as well as internal reliability (α = 0.85); the subscales also have a Cronbach's alpha of 0.85 or above (Hegarty et al., 2005). Cronbach's alpha in the original study (N = 665) is .93.
The Symptom Checklist-10 (SCL-10; Nguyen et al., 1983) is a short form of the SCL-90 which assesses mental health and distress. The 10 items of the SCL-10 ask participants to rate their level of distress in the past week on a Likert scale from never (0) to extremely (4) on six depression items, two somatization items and two phobic/anxiety items. Item scores are summed with a range from 0 to 40, with higher scores indicating more distress. Müller et al. (2010) suggested a clinical cutoff of 14.2. The measure has strong validity and reliability (Müller et al., 2010; Nguyen et al., 1983). Cronbach's alpha in the original study with 665 women is .89.
The Center for Epidemiologic Studies Depression Scale 10 (CESD-10) is a 10-item scale, used to measure participants’ level of depression. Respondents rated how each of the 10 items influenced them in the past week using a 4-point Likert scale from rarely (0) to most of the time (3) with a possible score range of 0 to 30, in which higher scores indicate increased depression symptoms (Andresen et al., 1994). The CESD-10 has been shown to have good reliability and validity (Andresen et al., 1994). Internal consistency and test–retest reliability are good (Björgvinsson et al., 2013). Cronbach's alpha in the original study (N = 665) is .84. Björgvinsson et al. (2013) suggest that a cutoff of 15 has the best “sensitivity” and “specificity” (p. 434).
The PTSD Checklist (PCL; Blanchard et al., 1996) was designed to screen for PTSD. It consists of 17 items, five of which address reexperiencing symptoms, three items regarding avoidance or numbing, and two items about hyperarousal. Participants rate how much they have been bothered in the past month by that symptom on a Likert scale from not at all (0) to extremely (4). Item scores are summed with a range from 0 to 68, with higher scores indicating more PTSD. The PCL has demonstrated validity and reliability (Blanchard et al., 1996; Wilkins et al., 2011). Cronbach's alpha in the original study (N = 665) is .92. Blanchard et al. (1996) suggest a cut-off score of 44.
Well-being was assessed by the Quality of Life (QOL) Questionnaire (Andrews & Withey, 1976). The original 25-item scale was shortened by Sullivan and Bybee (1999) to nine items measuring satisfaction with the overall QOL (i.e., How do you feel about life as a whole?) and satisfaction with areas in life (i.e., How do you feel about yourself; your personal safety; the amount of fun and enjoyment you have?). Items are rated on a 7-point scale (1 = extremely pleased; 7 = terrible) and are summed and reverse-scored (range of 0 to 63), with higher scores indicating better QOL. Cronbach's alpha for QOL in the original study (N = 665) is .84.
Data Analysis
The demographic information and scores on the standardized measures were used descriptively to add context to the qualitative analysis of the 40 interviews. Qualitative secondary analysis reuses interviews (Heaton, 2008), providing the opportunity to access hard-to-reach populations or discuss sensitive topics without added intrusion (Long-Sutehall et al., 2010).
The interviews were analyzed by the first author as her dissertation research, using inductive analysis to create the themes. This process was described by Patton (2002) as, “findings emerge out of the data, through the analyst's interactions with the data, in contrast to deductive analysis where the data are analyzed according to an existing framework” (p. 453). First-level coding was conducted first, which entails word-by-word scrutiny of the narratives to identify prominent themes and subthemes (Braun & Clarke, 2006). Second-level coding followed, which examines the themes and subthemes to identify similarities, differences, and gaps using the constant comparative method (Thorne, 2000). NVivo 11 was used to manage the data.
As suggested by Heaton (2008), the four criteria outlined by Lincoln and Guba (1985) of credibility, dependability, confirmability, and transferability were used to establish trustworthiness, meaning that one can have confidence that the study was conducted ethically and fairly; that the findings accurately represent the respondents’ experiences; and that the researcher's interpretations are credible (Padgett, 1998). In the current analysis, the detailed quotes were considered in context to ensure that the women's views were accurately represented (credibility and dependability). They were then triangulated by source (more than one respondent raised similar issues), analyst (a peer also analyzed the interviews for consistency), and negative case analysis (no or few contradictions of the issue). Triangulation was also used to establish dependability. Confirmability was established through triangulation and negative case analysis. Transferability means that the themes are presented in enough detail to consider whether they could be applied to similar respondents who were not interviewed.
Results
This section first presents the results from the demographics and standardized mental health/well-being measures, then three qualitative themes of colonization issues, accessing formal services, and evidence of resilience, each of which emerged from the interview narratives.
Women's Demographic Profiles.a
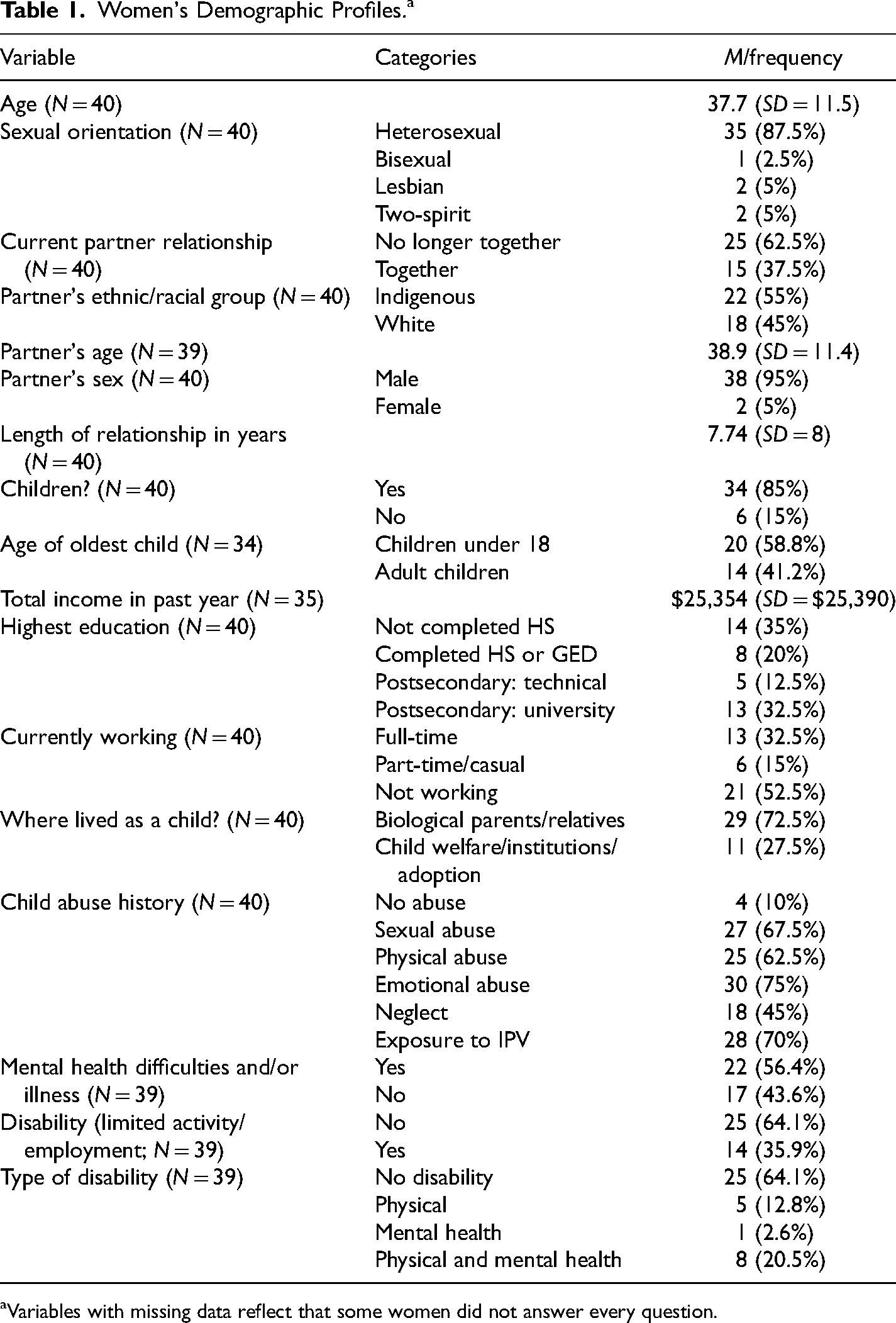
Variables with missing data reflect that some women did not answer every question.
The women's highest level of education varied; 14 (35%) had not completed high school, while 18 (45%) had attended postsecondary institutions. Of the 35 women who reported their income in the past year, these ranged from $451 to $100,000, with a mean of $25,354. Slightly over half of the women (21 or 52.5%) were not currently working, while 13 (32.5%) worked full-time and 6 (15%) worked casual or part-time.
Regarding their childhoods, almost three-quarters (72.6%) had resided with their nuclear families (26) or relatives (3). Of the other 11 women, seven (17.5%) had been involved with the child protection system, foster care, and/or the criminal justice system, and three (7.5%) had attended residential schools. Almost all (36) disclosed serious childhood maltreatment. While 22 women identified physical or mental health conditions, only 14 described these as limiting their activities or employment, the defining feature for disabilities.
Women's Scores on Abuse and Mental Health Indices.a
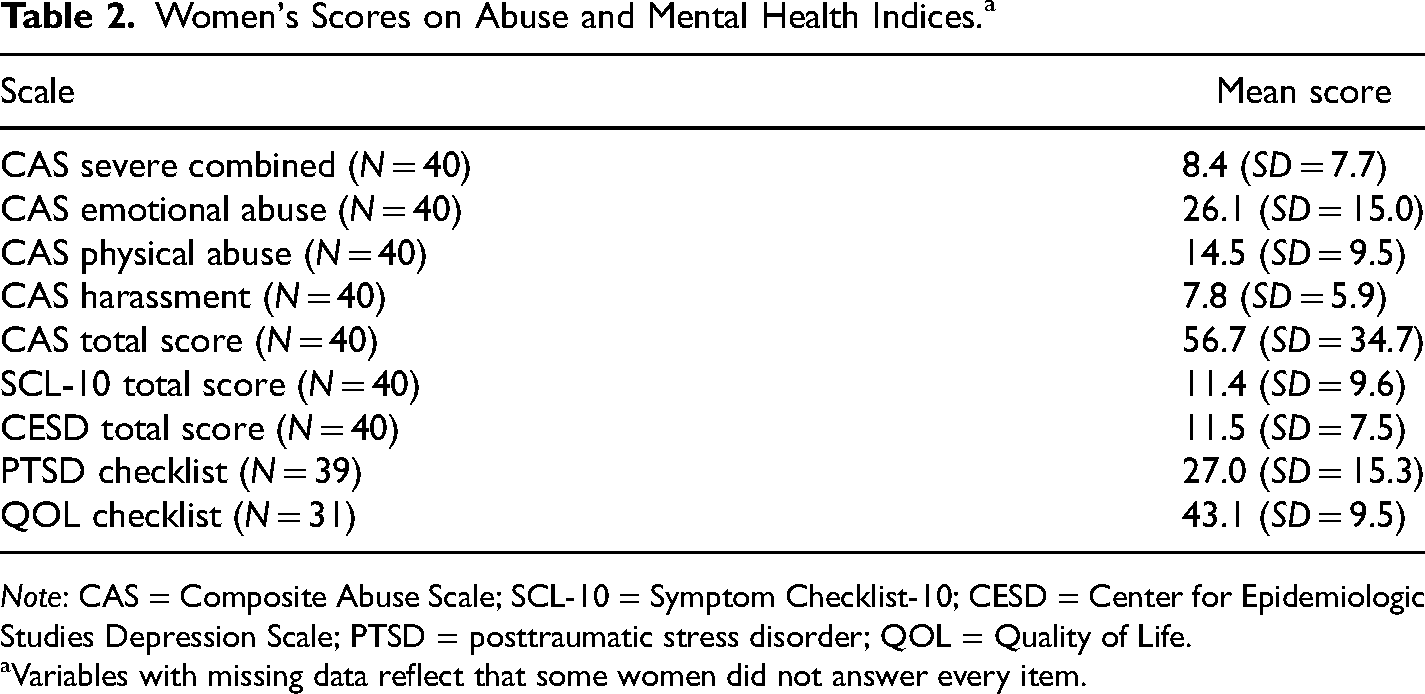
Note: CAS = Composite Abuse Scale; SCL-10 = Symptom Checklist-10; CESD = Center for Epidemiologic Studies Depression Scale; PTSD = posttraumatic stress disorder; QOL = Quality of Life.
Variables with missing data reflect that some women did not answer every item.
A little more than half the women (53.8%) were currently involved in a spiritual organization, although they were not asked to specify what that consisted of, whether organized religions or Indigenous beliefs. Eighteen women (47.4%) noted that their spiritual beliefs were influential in their leaving the abusive relationship. Thirty women (77%) identified their spiritual beliefs or practices as helping them to cope.
I’m happy with my life right now. I’m glad that I’m alive, my children are with me and I’m so glad that I made the choice not to be in that relationship. I have so much planned for my future right now. You have the strength to carry on. It's inside every person if they’re willing to take the step to healing, the step to nonviolence.
Discussion
The results are discussed in the context of a holistic model of the well-being of these Indigenous women, considering risk and protective factors as well as evidence of resilience (see Figure 1). The variables considered risk factors in the model are mostly quantitative from the survey questions and include poverty (income), continuing to live with an abusive partner (yes/no), disability (yes/no), child abuse (yes/no), and the severity of the IPV (CAS scores). The one qualitative risk factor variable is the theme of colonization. Protective factors such as satisfaction with informal support, community support, spirituality, and childhood residence (with family or not) are all from the quantitative survey. Accessing services (formal support) was a qualitative theme.
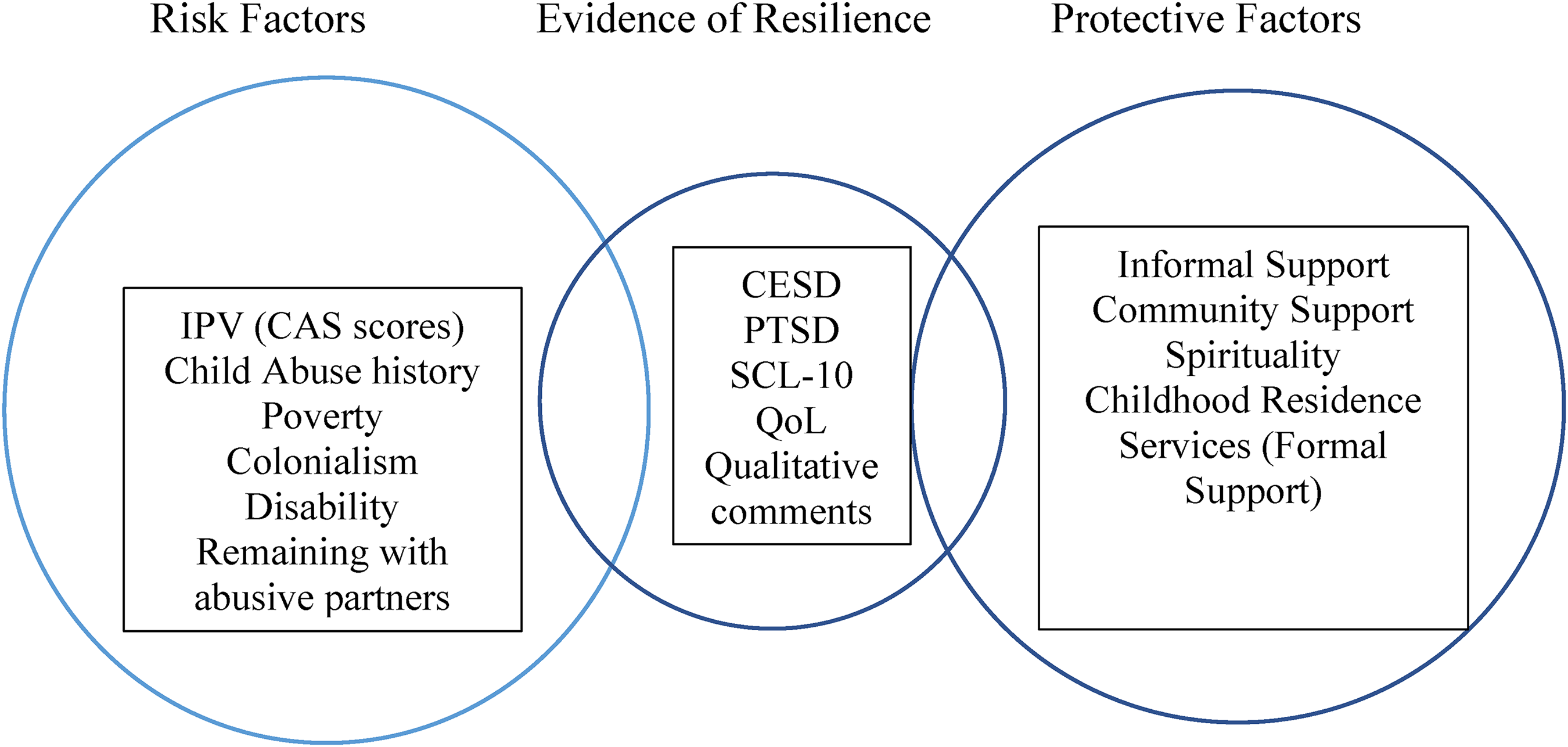
A Holistic Model of Risk and Protective Factors for the Well-being of Indigenous Women Survivors of IPV.
Evidence of resilience largely comes from the qualitative themes. The scores on the mental health measures could have been considered as risk factors if the average scores had been in the clinical ranges, suggesting the need for counseling. As these were not in the clinical ranges, despite the considerable severity of the risk factors, we consider these as evidence of resilience (congruent with Crann and Barata, 2021).
Dominant Canadian society not only supported colonialism and racism through legislation, residential schooling, and genocide but also embedded stereotyping, systemic oppression, and racism in many institutions and organizations the women accessed in their search for help and support (Baskin, 2020; National Inquiry into Missing and Murdered Indigenous Women and Girls, 2019; Williams et al., 2019). In the interviews with 32 of the 40 women (80%), the women described colonization, intergenerational abuse, and intimate abuse by their partners. Six of the 40 women (15%) had lived in residential schools, and another seven (17.5%) highlighted how it had impacted their parents and/or grandparents.
Most of the women's experiences of adversity began with childhood abuse, with almost two-thirds having been sexually and physically abused, factors typically associated with mental health problems that often extend into adulthood (Brownridge et al., 2017; Chmielowska & Fuhr, 2017; Domhardt, 2015; Heidinger, 2021). Moreover, many women in the current study had experienced multiple forms of child abuse, called polyvictimization (Finkelhor et al., 2007), which is related to an increased likelihood of adverse effects in adulthood including PTSD.
In the current study, the mean scores of all the CAS subscales were above the clinical cut-offs indicating significant IPV, similar to other studies of abused Indigenous women (Brownridge, 2008; Guggisberg, 2019; McKinley, 2022; Romans et al., 2007). The severity of the physical and emotional abuse and sexual assaults from abusive partners represent significant risk factors (Heidinger, 2021; Hoffart & Jones, 2018). Moreover, leaving an abusive partner places women at greater risk for more severe physical and sexual violence for all women, but women of Indigenous origins in particular (Brownridge et al., 2008; Pederson et al., 2013). In the current study, 37.5% of the women still lived with their abusive partners. In the original larger study, more Indigenous women (22.6% of 292) remained with partners than non-Indigenous women (14.3% of 294; Tutty et al., 2020). Dickson-Gilmore (2014) argues that women in Canadian Indigenous cultures experience pressure to keep their families intact, which could at least partly explain this dynamic. Nevertheless, remaining with abusive partners has consistently been seen as a risk factor for future IPV (Smye et al., 2021) and is considered one in the current model.
Having a disability is also a risk factor for IPV and more severe abuse (Brownridge, 2006b; Heidinger, 2021; Tutty, Radtke, Ateah, et al., 2021). A little more than one-third (14 or 35%) of the 40 women reported medical conditions that constitute disabilities as they limited the woman's activity and/or employment.
Similar to Crawford et al. (2009), the women's use of formal resources represents a protective factor that we considered in assessing their well-being. A number had accessed emergency and second-stage VAW shelters (62.5%) and 70% had accessed community counseling services. Almost half of the women (42.5%) had sought traditional cultural teachings and ceremonies to assist them in healing from their partners’ abusive behaviors, some in combination with mainstream counseling approaches (Ogden & Tutty, 2024). Accessing Indigenous healing practices such as talking with elders, traditional teachings, oral traditions, ceremonies, and connection with nature and the land has been identified as a protective factor by several authors (Burnette & Hefflinger, 2017; Olsen Harper, 2011; Ward et al., 2021; Williams et al., 2019). These ideas highlight the significance of the women in the current study connecting (or reconnecting) to Indigenous cultures and healing practices (Brave Heart et al., 2011; National Inquiry into Missing and Murdered Indigenous Women and Girls, 2019; Olsen Harper, 2011). From a relational perspective, it highlights the healing and connection that the women found in the natural world, emphasizing the healing they found in honoring and integrating their physical, emotional, and spiritual aspects. It also highlights the women's determination and commitment to healing because most women were not raised with traditional healing practices; they sought this out as adults.
Despite the severe intimate partner abuse and other risk factors, additional evidence for resilience is provided by the fact that the respondents were generally functioning well on the mental health and qualitative of life measures. On average, the women were not experiencing clinically significant symptoms of psychological distress, depression, or PTSD (suggested by Crann & Barata, 2021 as a sign of resilience). Their scores were consistent with and somewhat less dysfunctional than the total sample of 291 Indigenous Healing Journey participants (Tutty et al., 2020) but neither sample scored over the clinical cutoffs (i.e., SCL-10 total = 11.4 vs. 13.5; CES-D total = 11.5 vs. 12.2; PCL = 27 vs. 27.4).
Of note, there is a paucity of quantitative research on the mental health of Indigenous women abused by intimate partners, however, with the exception of Tutty et al. (2020, Tutty, Radtke, Thurston, et al., 2021), several studies showed significant associations of IPV with depression, but these did not use standardized measures with clinical cutoff scores to more accurately diagnose mental health functioning (Evans-Campbell et al., 2006; Schultz et al., 2021), except Giesbrecht et al. (2022).
That the women were not, on average, experiencing clinically significant mental health distress differs from some literature on IPV and the mental health of Indigenous women. For example, a global systematic review conducted by Chmielowka and Fuhr (2017) linked Indigenous women's experience of IPV with depression and PTSD, which they saw as further exacerbated by poverty, discrimination, and substance abuse. Certainly, a proportion of the women in the current study were in the clinical ranges on depression, PTSD, and mental health functioning, just not the majority. These results suggest the importance of not stereotyping Indigenous women as necessarily having mental health issues. This is supported by Brennan's 2011 study of victimized Indigenous women across Canada, which stated that 90% of the respondents self-reported their mental health as “good” or “very good” (p. 11).
To summarize, some scholars argue that the more risk factors one experiences, the greater the likelihood of negative outcomes; and the more protective factors, the more likely one has positive outcomes (Olsen Harper, 2011). It is notable that, despite serious risk factors, the women in the current study identified important protective factors. We suggest that they were remarkably resilient given that the mental health measures were not on average in the clinical ranges of psychological distress, depression, or PTSD, consistent with the larger sample of Indigenous women in the Healing Journey study (Tutty et al., 2020). This supports the idea that resilience is not simply about the number of risk or protective factors but reflects a deeper and more complex concept.
Implications for Practitioners and Researchers
The experiences of the 40 Indigenous women abused by their intimate partners suggest that it is essential that social workers and other counselors understand both intimate partner abuse, the devastation of Indigenous cultures through colonization, and that Indigenous cultures have survived despite colonization (Kirmayer et al., 2009). The respondents experienced traumatic experiences including their partner's abusive behavior, polyvictimization, and intergenerational trauma. Yet the women's average scores on the PTSD checklist were not in the clinical range that would suggest a PTSD diagnosis. Counseling that addresses resilience and is strengths-based is recommended (Yuan et al., 2015).
With the exception of the current research, the few quantitative studies conducted on the mental health of Indigenous women used measures without clinical cut-off scores (i.e., Evans-Campbell et al., 2006; Schultz et al., 2021), an exception being Giesbrecht et al. (2022). The advantage of more carefully choosing measures with clinical cut-offs is illustrated in being able to identify when women are not significantly affected by mental health symptoms (Tutty, Radtke, Ateah, et al., 2021). Further, more study of the resilience of Indigenous women is needed to counterbalance the tendency to focus only on trauma and mental health without acknowledging these women's strengths.
Limitations and Strengths of the Current Study
A limitation of the current analysis is that data from the primary society was collected between 2007 and 2009, which raises the question of relevancy, especially since the publication of the National Inquiry into Missing and Murdered Indigenous Women and Girls (2019). Nevertheless, few recent studies have studied the experiences of Canadian Indigenous women abused by intimate partners in such a complex manner, or with regard to their resilience.
In the current study, evidence of resilience considered information from both the qualitative and quantitative data. Notably, the study might have included a measure of resilience, such as the Connor-Davidson Resilience Scale (Connor & Davidson, 2003) or the Brief Resilience Scale (Smith et al., 2008) to directly assess the concept, as Humphries did in 2003. However, these measures conceptualize resiliency as a personal, psychological trait that entails an “ability to bounce back.” The current analysis moves beyond an individual focus, using a more culturally appropriate, ecological model to assess the resilience of Indigenous women abused by partners (i.e., Luthar & Cicchetti, 2000; Ungar, 2013). Importantly, as well, the study assessed both protective factors and risk factors, different from early research on the resilience of abused women with IPV that assessed only risk factors (i.e., Humphries, 2003) and other research that only examined protective factors (i.e., Anderson et al., 2012; Crann & Barata, 2016, 2021; Howell et al., 2018). We argue both are needed for a comprehensive analysis of resilience.
Almedom and Glandon (2007) critique the sole use of mental health measures to establish resilience, identifying the need for “a multimethod and multilevel study design that combines both qualitative and quantitative techniques” (p. 127). We used a broader analysis of community and societal factors, that also included mental health measures on depression, psychological distress, and PTSD, each of which resulted in average scores below clinical cut-offs. The QOL scale can be considered a measure of well-being that adds to our ability to consider resilience. None of these mental health measures provided norms specific to Indigenous peoples, identical to other studies that used similar measures with Canadian Indigenous populations (Giesbrecht et al., 2022; Schultz et al., 2021; Varcoe et al., 2017).
One might criticize the use of Western societal mental health measures as not fitting with Indigenous concepts of health and well-being, which are less individually focused and represent a substantially different worldview (Gone, 2022). The current study looks beyond individual mental health to consider societal and community concerns fit an Indigenous perspective. Nonetheless, Canadian researchers have used similar mental health measures in analyzing both generic- and Indigenous-specific interventions for Indigenous women (Evans-Campbell et al., 2006; Giesbrecht et al., 2022; Schultz et al., 2021; Varcoe et al., 2017).
A standardized measure of social support in the original study would have added to our understanding of these women's lives. Qualitatively, it should also be noted that the interview questions and probes did not focus specifically on issues of residential schools, racism, discrimination, or resilience. That these themes emerged in the interviews is important, but since this information was not gathered systematically, the number of women who experienced these likely underestimates these widespread societal traumas for Indigenous peoples.
The women were recruited through shelters and community agencies, which suggests that those who chose to participate may have higher resilience than those who did not seek assistance for IPV. As such, the sample may not be representative of Indigenous women abused by intimate partners in the Canadian prairies.
Only two interviewers (who conducted five interviews) and neither of the two women coauthors are Indigenous, which might have affected both the interview process and the data analysis. Nevertheless, the respondents were persistent about placing their partner's abusive behavior in context by sharing the violence they had experienced throughout their lives, as well as the oppression and racism, and pieces of their Healing Journeys in depth.
A strength of this study is its focus on Canadian Indigenous women who have survived IPV, an important group that has not received sufficient research attention. We provide important details about their experiences and what risk and protective factors and resilience influence their well-being. Incorporating cultural values and diversity of Indigenous peoples into the concept of resilience, mitigates some critiques of resilience from authors like Olsen Harper (2011), Tousignant and Sioui (2009), and Ungar, (2013), allowing us to understand the experiences of the 40 Indigenous women more comprehensively.
Conclusion
There is a paucity of research on the experiences of Indigenous women who have been abused by their intimate partners and who live in Canada's prairie provinces. Given the serious risk factors most had endured, their resilience was notable: even though the women faced numerous risks, in general, they maintained their mental health and well-being. The women shared intimate details of their lives, including sensitive information about their relationships with family and abusive partners. It is important that the complexity of their lives is understood, and respected. Only then can we create practices, programs, and services that are truly useful. Taking such steps can help us move toward creating a more equitable, decolonized society.
Footnotes
Acknowledgments
This research is based on Cindy Ogden's doctoral dissertation for the Faculty of Social Work, University of Calgary, “Services and Indigenous Healing Practices to Address Intimate Partner Violence Against Indigenous Women in the Canadian Prairie Provinces.” Deepest gratitude to her defense committee: Drs Leslie M. Tutty, David Este, Wilfreda Thurston, Anne-Marie McLaughlan, Katrina Milaney, and Dianne Hebert-Murphy. Thanks to the Healing Journey study team with coprincipal investigators: Dr E. Jane Ursel and Marlene Bertrand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.