
Abstract
Studies about violence against women specific to the Chilean population are scarce. As a result, government treatment programs lack a local perspective. Predictor variables were analyzed in the mental health of Chilean women who have survived intimate partner abuse. Two hundred and two women who made regular visits to public Women’s Centers participated in the study; on average, they had survived 11 years of abuse. Logistic regression analyses were conducted to determine what variable/s in the history of violence best predicted the mental health variables. Among other protective factors, an increase in both resilience and the time since the last violent episode yielded a reduction in levels of general psychological distress (B = –1.836, p < .001 and B = 1.117, p < .001 respectively), post-traumatic stress disorder (B = –1.243, p = .002 and B = 1.221, p < .001 respectively), and depression (B = –1.822, p < .001 and B = 1.433, p < .001 respectively). The study also noted risk factors such as a high level of additional stressors, which in turn led to increased levels of general psychological distress (B = 1.007, p = .005), post-traumatic stress disorder (B = 0.928, p = .013), and depression (B = 1.061, p = .016). The Women’s Center is the place where women feel most supported. To improve the effectiveness of treatments at these centers and aid in the recovery of women who have suffered from intimate partner violence, the predictive factors significantly related to mental health should be taken into account. This means prioritizing cases where the last episode of violence was more recent, addressing additional stressors, and promoting resilience.
Introduction
Intimate partner violence against women (IPVAW) is a major public health concern and a violation of women’s human rights (Lutwak, 2018). Worldwide, almost one-third (30%) of women who have been in a relationship have experienced physical and/or sexual violence by an intimate partner (World Health Organization, 2019). In Latin America, little up-to-date information is available on the prevalence of IPVAW due to a lack of studies done with valid and reliable instruments/scales (United Nations Development Programme, 2017). According to available data, between 8% and 52% of women in different countries of the region (an average of 28%) have suffered violence at the hands of a male partner. In Chile, 4 out of 10 women had suffered psychological violence by their partner; 1 in 4, physical violence; and 1 in 10, sexual violence, according to the National Women’s Service (Servicio Nacional de la Mujer, or SERNAM, 2009). Additionally, 15.1% of young women stated they had been the victim of physical violence in their romantic relationships (Viejo et al., 2018). A total of 43 women were murdered by their intimate partners in 2020 and, by May 2021, another 16 victims had been recorded, with another 63 cases of attempted murder, according to the National Service for Women and Gender Equality (Servicio Nacional de la Mujer y la Equidad de Género, or SERNAMEG, 2021). Approximately one woman is killed by her intimate partner per week (Lafontaine et al., 2018).
IPVAW has extensive repercussions and affects a woman’s physical, mental, sexual, and reproductive health (Lutwak, 2018). In terms of mental health, this type of violence often leads to depression and post-traumatic stress disorder (PTSD) (Fernández-Sánchez & López-Zafra, 2019; Jonker et al., 2019; Vilariño et al., 2018). Depression, a disorder characterized by feelings of sadness, loss of interest or pleasure, feelings of guilt or a lack of self-esteem, sleep disorders or loss of appetite, trouble sleeping, and difficulty concentrating (American Psychiatric Association, 2013), can lead to the social isolation of the victims of violence (Cody et al., 2017). PTSD is an anxiety disorder in which a person has been exposed to one or more traumatic events involving death or the threat of death or bodily harm to themselves or others, and has responded with intense fear or desperation (American Psychiatric Association, 2013). As part of this disorder, the person relives the traumatic event and goes to great lengths to avoid any reminders of the trauma (Costa & Canossa, 2018; Fernández-Sánchez & López-Zafra, 2019). Depression and stress symptoms usually coexist in a common state of emotional suffering known as general psychological distress (Arvidsdotter et al., 2016). People suffering from this mental health problem also present somatic complaints, chronic illnesses, and syndromes that cannot be medically explained.
Women who have been exposed to IPVAW have different rates of mental health (symptoms of depression, PTSD, or general psychological distress). From an ecological perspective, the difference lies in the myriad factors that may be mediating the trauma (Carlson & Dalenberg, 2000). Factors that influence violence include a dominant male figure in the family and a personal history of violence at the level of microsystem (the immediate environment where the victim copes); isolation of the woman and her family at mesosystem level (relationship between microsystems) and exosystem level (other factors that influence the microsystem, such her partner’s job); and machismo at the level of macrosystem (social and cultural conditions, traditions) (Heise, 1998). To understand the different responses women have to violence, the individual and her environment are seen from a dynamic, mutually reciprocal point of view (Lazarus & Folkman, 1984). Protective factors are those which reduce the harmful effects on women’s mental health, while risk factors worsen it.
Among the protective factors at the individual level, we find the developmental level of the victim (Arbach & Bobbio, 2018; Carlson & Dalenberg, 2000) and resilience, understood as the human’s ability to adapt, find meaning in traumatic experiences, and achieve personal growth (Tsirigotis & Łuczak, 2018). Higher resilience is associated with better mental health and fewer pathologies (Crann & Barata, 2015; de la Rosa et al., 2016; Fernández-Sánchez & López-Zafra, 2019; Jose & Novaco, 2016). At micro and mesoystem level, perception of support—understood as the way someone considers that their friends, family and/or other sources of material, psychological and/or general help (Ioannou et al., 2019)—is a protective factor against depression (Costa & Canossa, 2018; Zapor et al., 2018), as is economic independence (Arbach & Bobbio, 2018; Costa & Canossa, 2018; Zapor et al., 2018).
In terms of the risk factors for mental health among women who experience IPVAW, the time since the last episode of violence, the length of trauma exposure, the severity of the trauma (Carlson & Dalenberg, 2000), the type of violence experienced (with sexual violence having the greatest impact on a woman’s mental health (Domenech & Sirvent, 2017; Jonker et al., 2019), the types of violence suffered in childhood, and prior and subsequent life events were all prominent at microsystem level. At micro, meso, and exosystem levels, risk factors are additional stressors to the violence itself, such as not having a stable job or having children in their care, and their severity (Arbach & Bobbio, 2018; Costa & Canossa, 2018; Zapor et al., 2018). Stress is here conceptualized as a relationship between the person and the environment, in which the person evaluates whether she has sufficient resources and whether her well-being is jeopardized (Lazarus & Folkman, 1984). At macrosystem level, social context was found to be a potential risk factor (Arbach & Bobbio, 2018).
In Chile, several studies have examined IPVAW and its consequences on women’s health. Ceballo et al. (2004) interviewed 215 women living on the outskirts of Santiago; according to their results, IPVAW was a cause of deteriorating health among victims. Based on studies on psychosocial profiles Calquín and Chávez (2007) concluded that most victims of physical abuse aggravated by the use of a firearm were young housewives who had not finished high school. Illanes et al. (2007) showed a high prevalence of sexual violence in a sample of women from the city of Temuco; the authors linked this violence to symptoms of PTSD. In another study on pregnant women in a neighborhood in the city of Santiago, Crempien et al. (2011) found that 30.1% had suffered some type of violence during their current pregnancy. Among these women, 53% stated that their intimate partner was the perpetrator, and 42% suffered from general psychological distress, with symptoms of anxiety or depression. Three years later, in a literature review of Chilean studies on mental health and IPVAW, León et al. (2014) concluded that only 11 studies examined IPVAW and its repercussions for women’s health, though none discussed protective or risk factors.
Therefore, there is no up-to-date Chilean research focusing on the potential effect of predictive role of protective and risk factors on the mental health of IPVAW survivors. To address this gap, this study aims to analyze predictive variables for symptoms of depression, PTSD, and general psychological distress among Chilean women who have survived partner abuse. By identifying meaningful variables, better treatments could be offered to IPVAW victims (Lutwak, 2018), thus aiding in their recovery from the trauma of violence at the hands of a current or former partner.
Method
This research is a correlational cross-sectional (transversal) survey study. The relational study examining predictive factors and mental health of IPVAW survivors involved a semi-structured interview with the participants along with four scales completed at one sitting.
Participants
SERNAM is the government agency responsible for training, consultation, and public policy advocacy related to intimate partner abuse in Chile. As part of IPVAW prevention, every city has a Women’s Center for walk-in consultations that provides psychological and social support, guidance, legal assistance, group therapy, and, at some locations, individual therapy.
Cluster sampling was used for the study in which five of these Women’s Centers from the Metropolitan Region of Chile were selected at random. The inclusion criteria of the participants (Chacón-Moscoso et al., 2016) included age (18 or older), having suffered partner violence by a male partner (former or current), being a regular visitor to one of the selected Women’s Centers between 2009 and 2011, and volunteering to participate.
In total, 202 women were recruited. The age of the women ranged from 19 to 71 (M = 40.3 years old, SD = 11.70), and 99% had children, 47% of which had either one or two children. In terms of other sample features, 54% were married, 38% had completed elementary school, 30% were housewives, and 64% self-reported low socioeconomic status. In terms of their first contact with the centers, 35.6% arrived on their own accord, while the rest came as referrals from another social program. Family healthcare centers, hospitals, or mental healthcare centers made the referral in 20.8% of the cases; the courts, mainly family or supervisory courts, 23.8%; and neighborhood social programs, the police, or women’s neighborhood workshops, 19.8%.
Procedures
After the main researcher contacted SERNAM in 2009 to request access to several Women’s Centers in the Metropolitan Region, the agency signed two letters of agreement authorizing the investigation (see Supplementary file 1). It also provided the complete list of Women’s Centers available (five were selected at random) and the full list of women currently being seen at these centers. All women were contacted and those meeting the inclusion criteria participated voluntarily after signing the informed consent letter (see Supplementary file 2), as required by Chilean law 20.120 and the Chilean Psychologist Association (Colegio de Psicólogos de Chile, 1999; Ministerio de Salud or Ministry of Health, 2006). The letter discusses ethical issues such as data confidentiality, the participant’s right to quit the study, and the right to refuse to answer any of the questions.
A pilot study was carried out with 20 women who were seen at two of the selected Women’s Centers. It was useful to assess whether they understood the questions and the time they took to answer.
The evaluation procedure, which included an ad hoc structured interview and four scales (see the Instruments section), was done face-to-face and individually between the same interviewer and each woman to assure confidentiality of highly personal information. The procedure was the same for both the interview and the scales: the interviewer asked each question, the woman answered verbally, and the interviewer took notes. There were a total of 176 questions. Answering all these questions took between 90 minutes and two hours. In order to guarantee the confidentiality of the data, each participant was assigned a code.
Measures and Instruments
The most prevalent variables were chosen according to the literature. The protective factors measured were, at the individual level, resilience; and at micro and mesosystem level, perception of support. The risk factors considered were, at microsystem level, the time since the last episode of violence, the length of trauma exposure (duration of the violence defined as the number of years in a violent relationship), and the type of violence experienced (physical, psychological and/or sexual); and at micro, meso, and exosystem levels, additional stressors. In terms of mental health, depression, PTSD, and general psychological distress were measured.
The protective and risk factors (with the exception of resilience) were assessed with an ad hoc structured interview. Resilience and mental health characteristics (i.e., general psychological distress, PTSD, and symptoms of depression) were measured with questionnaires. Information about the concrete instruments used to measure these variables are presented below.
The had hoc structured interview (see Supplementary file 3) started with nine sociodemographic questions. It continued with questions aimed at assessing the history of the violence (time since the last episode of violence, length of trauma exposure, and type of violence experienced), perception of support, and additional stressors.
History of violence. Women were asked about the number of years they had experienced abuse, and the amount of time since the last violent episode. Additionally, in order to gauge the type of violence women had suffered during the last year, they were asked to rank the frequency of a list of 22 incidents on a scale of 0 (never) to 3 (always or almost always); the sum of items assessing each type of violence was then divided by the number of items and multiplied by 100. The aim was to facilitate a comparison of different types of violence, given that the number of items varied for each type: 10 items for physical violence, 9 for psychological violence, and 3 for sexual violence. For instance, items to measure physical violence suffered included “pushing” and “threatening you with a firearm”; to measure psychological violence, “verbally threatening to mistreat, harm, or torture you”; and to measure sexual violence “Forcing you to have sexual relations or perform other sexual acts you do not want either by direct threat or by inducing a fear of retaliation” (Labra, 2014).
Perception of social support. Women also were asked to gauge their perception of social support both during the violence and at present with 21 items on a Likert-type scale of 1 (lowest level of perceived support) to 4 (the highest level). Perceived support was classified as emotional, informational, or tangible and assessed for six categories: family, friends, neighbors, police, professionals, and the Women’s Center. The total scores obtained in each of the six categories yielded values ranging between 6 and 24.
Additional stressors. This risk factor was measured with 12 items about stressful events women were experiencing during the last year on a scale of 0 (did not happen) to 2 (occurred and had a considerable impact). Some examples of items were “death of a relative or someone close,” “illness of a relative or someone close,” or “personal legal problems.” The sum of the 12 items yields a total score, ranging from 0 to 24 points.
Resilience. The Saavedra and Villalta resilience scale SV-RES (2008; see Supplementary file 4), which draws on Grotberg’s model (2006), is formed by 60 items ranging from 1 (strongly disagree) to 5 (strongly agree). Examples of items are “I am a hopeful person” and “I have reliable personal relationships.” The sum of all items yields a total score ranging from 60 to 300. The higher the score, the greater the resilience. In the case of Chile, the psychometric results of this scale were adequate, with a Cronbach’s alpha of 0.96 and a validity correlation coefficient of 0.76 using the Connor and Davidson Resilience Scale CD-RISC (some examples of items of this scale are “I see the funny side of things” and “I try my best every time”).
General psychological distress. The 12-item General Health Questionnaire (GHQ-12; see Supplementary file 5) (Araya et al., 1992; Goldberg & Williams, 1988) detects the severity of mental problems over the past two weeks; it is a screening for psychological distress and can be applied to both clinical and non-clinical populations. Each of the 12 items present four response options, two of which indicate that the situation is stable (and assigned a value of 0), and two others indicating maladjustment (assigned a value of 1). The sum of all items yielded a total score of 0–12. Higher scores indicate more distress. If the total was 5 or more, a more in-depth evaluation is recommended. In Chile, Araya et al. (1992) validated the questionnaire with a Cronbach’s alpha of 0.902, a validity coefficient of 0.76, a specificity of 0.73, and an error margin of 0.26.
PTSD. The Severity Scale for Symptoms of PTSD (Escala de Gravedad de Síntomas del Trastorno de Estrés Postraumático, or EGSTEP; see Supplementary file 6) (Echeburúa et al., 1997) is a clinician-administered instrument involving a structured interview that evaluates the symptoms and intensity of PTSD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria. Its 17 items have four response options from 0 (no symptoms) to 3 (a lot), yielding total scores that range from 0 to 51 (higher values indicating greater severity of PTSD). The test-retest reliability of the instrument was 0.89 and an analysis of internal consistency yielded a Cronbach’s alpha of 0.92.
Symptoms of depression. Beck’s Depression Inventory (BDI; Beck et al., 1979; see Supplementary file 7) is a self-report inventory to measure symptoms of depression in normal and clinical populations. For this study, the 21-item self-assessment version adapted to Spanish by Vázquez and Sanz (1997) was utilized (It obtained a Cronbach’s alpha of 0.90.). Each item has four response options from 0 (least severe) to 3 (most severe), yielding total scores that range from 0 to 63, where higher values indicate higher levels of depression.
Data Analysis
Descriptive statistics were performed using SPSS Statistics 21. Percentages and means were used to describe women’s sociodemographic characteristics, history of violence, perceived support, resilience, and mental health. Cronbach’s α was used to calculate the reliability of the scales and subscales used. Values of 0.7 or higher were considered appropriate. Given that the variables did not meet the normality assumption, non-parametric tests were developed. Spearman’s correlations (r) were run to determine the relationship between the mental health indicators (general psychological distress, PTSD, and symptoms of depression) and the variables related to the women’s history of violence (duration of the violence, types of violence, and time since last violent episode occurred), the level of additional stressors, and the women’s perception of support.
Finally, considering non-parametric data distribution, with a similar data distribution of independent variables in skewness and kurtosis, and following the recommendations of the authors of the original scales to dichotomize the dependent variables, all variables were dichotomized as follows. The median was treated as a cut-off point, that is, years experiencing abuse (0 = lower, 1 = higher); time since last violent episode (0 = more time passed, 1 = less time passed); and quantity of stressful events and their impact on a woman’s life (0 = lower, 1 = higher). Additionally, following the recommendation of the authors of each scale, cut-off points were established as follows: resilience (percentile 26 was the cut-off point, 0 = higher, 1 = lower); general psychological distress (a cut-off point of 5, 0 = does not present a disorder; 1 = may present a disorder); PTSD (a cut-off point of 15, 0 = does not appear to be suffering from PTSD, 1 = may be suffering from PTSD); and depression (a cut-off point of 17, 0 = does not appear to be suffering from depression, 1 = may be suffering from depression). Logistic regression analyses were then conducted to determine what protective and risk factors best predicted the mental health variables.
Results
Predictive Factors
Characteristics of the Women in the Study.
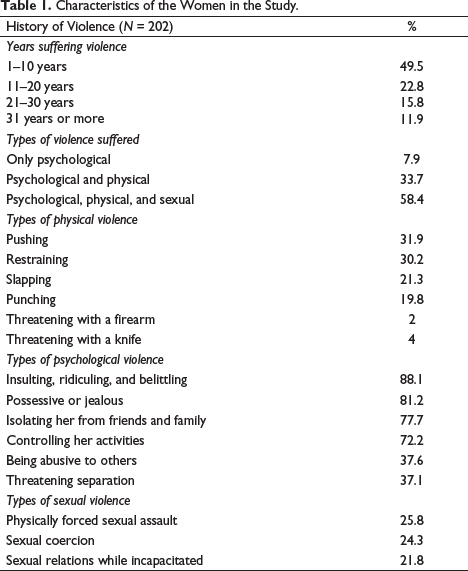
In terms of psychological abuse, the most commonly occurring behaviors reported by the women were insulting, ridiculing, and belittling (88.1%); being possessive or jealous (81.2%); isolating her from friends or family (77.7%); and controlling her activities (72.2%). In terms of the frequency of different acts of sexual violence, the results are relatively homogeneous and include physically forced sexual assault (25.8%), sexual coercion (25.8%), or sexual assault while incapacitated (21.8%).
Characteristics of Women’s Support Network.
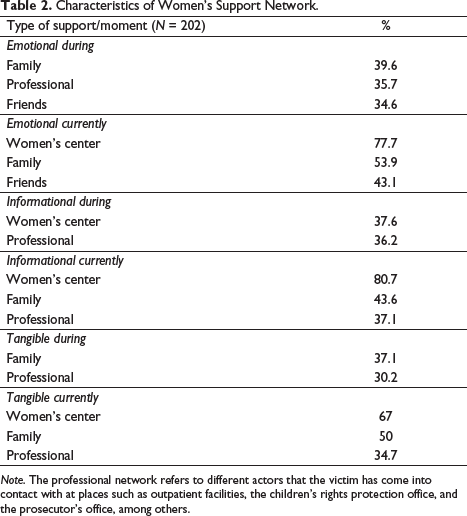
Note. The professional network refers to different actors that the victim has come into contact with at places such as outpatient facilities, the children’s rights protection office, and the prosecutor’s office, among others.
In terms of additional stressors, having young children to care for, family conflicts, economic troubles, and family illnesses were the most frequently mentioned.
Reliability
In the sample, all the scales had appropriate reliability values, with excellent results for the SV-RES (α = 0.97), the EGSTEP (α = 0.918), and the BDI (α = 0.911), and a very good result for the GHQ-12 (α = 0.892).
Mental Health
In terms of general psychological distress, 58.9% of the women were experiencing distress, and a great percentage of the women (69.3%) were found to be suffering from PTSD. With regard to the diagnostic categories of depression, 22.3% were not experiencing depression; 19.8% were experiencing mild depression; 27.2%, moderate depression; and 30.7%, severe depression.
Predictive factors of Mental Health
Spearman’s Correlation on the Relationship between Mental Health Indicators and Protective and Risk Factors.
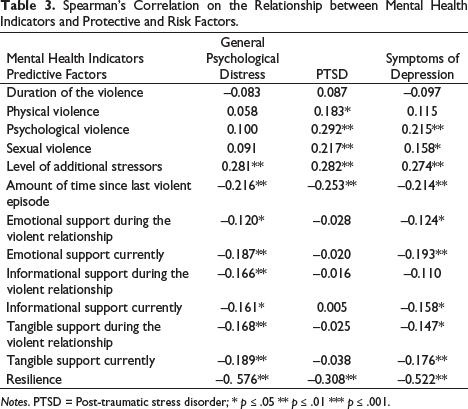
Notes. PTSD = Post-traumatic stress disorder; * p ≤ .05 ** p ≤ .01 *** p ≤ .001.
Logistic Regression Analyses between General Psychological Distress, PTSD, Symptoms of Depression, and Protective and Risk Factors.
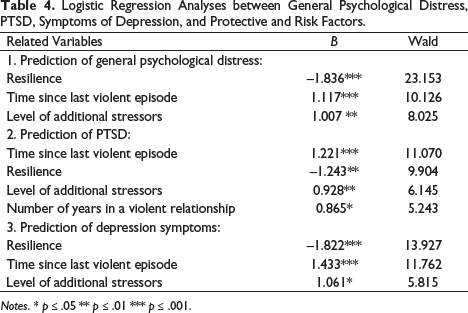
Notes. * p ≤ .05 ** p ≤ .01 *** p ≤ .001.
Time since the last violent episode significantly predicted PTSD (B = 1.221, p < .001), after controlling the effect of the other variables. PTSD is also significantly predicted by resilience (B = –1.243, p = .002), the level of additional stressors (B = 9.28, p = .013), and the duration (in years) of the violent relationship (B = 0.865, p = .022).
Resilience significantly predicted symptoms of depression, controlling the effect of the other variables (B = –1.822, p < .001). Time since the last violent episode (B = 1.433, p < .001) and the level of additional stressors (B = 1.061, p = .016) were two additional variables that proved significant predictors of depression.
Discussion
The average time the participants had spent in a violent relationship was 11 years. Most had experienced all three types of violence (physical, psychological, and sexual) in their relationships. Additionally, high levels of additional stressors were found. The highest percentage of current perceived social support (emotional, informational, and tangible) was the Women’s Center (SERNAM), which implies that these institutions play an important role for recovery from IPVAW.
The Chilean women who participated in this study had high levels of depression, PTSD that reflected the violence they had experienced and, in general, deteriorated mental health. This concurred with findings in other international studies on women who experienced violence at the hands of a current or former partner, such as in Spain, Portugal, or the United States (Costa & Canossa, 2018; Lutwak, 2018; Vilariño et al., 2018), and specifically in Chile (Ceballo et al., 2004; Illanes et al., 2007; León et al., 2014; SERNAM, 2009).
For the 202 women screened as part of this study, general psychological distress was shown to correlate significantly and positively with the level of stressors, but not with the level of physical, psychological, or sexual violence. This could suggest that IPVAW affects general psychological distress, regardless of the type or level of violence suffered. The results of Ceballo et al. (2004) concur with those presented in this study and in other international works (Costa & Canossa, 2018; Zapor et al, 2018). Psychological distress correlated significantly and negatively with the time since the last violent episode and with levels of social support. These results concur with other international studies (Costa & Canossa, 2018; Zapor et al, 2018) and that of Crempien et al. (2011), who found that 42.2% of a sample of pregnant Chilean women suffered from general psychological distress.
With regard to PTSD symptoms, this significantly and negatively correlated with the time since the last violent episode, though not with the level of the different types of social support, thus diverging from other international studies (Costa & Canossa, 2018; Zapor et al, 2018). The differences between the findings of this study and the one by Costa and Canossa (2018) may be due to the instrument, given that the Portuguese study utilized The Social Provisions Scale-10 item (SPS10). Comparing with Zapor et al. (2018), different findings may be attributed to differences in the sample (the Portuguese sample consisted of shelter residents). Additionally, PTSD correlated significantly and positively with all levels of abuse and the level of stressors. According to the results of a study by Illanes et al. (2007) on a Chilean sample, PTSD is more severe among the women subjected to sexual violence (Domenech & Sirvent, 2017; Jonker et al., 2019).
With regard to symptoms of depression, this significantly and positively correlated with psychological abuse, sexual abuse, and the level of stressors, but not with the type of physical abuse, indicating that any type of physical abuse can cause depression. These results are similar to those of Ceballo et al. (2004). Depression significantly and negatively correlated with the time since the last violent episode and with all levels of support, except for the informational support perceived during the abusive relationship. These data have been corroborated by other international investigations that emphasize how psychological symptoms increase in response to a perception of little social support (Costa & Canossa, 2018; Zapor et al., 2018).
Therefore, in general, it is possible to affirm that certain levels of mental health symptoms significantly correlate with the types of abuse suffered, as it was found in Ceballo et al. (2004) in another Chilean sample. The factor of time since the last violent episode is clearly a significant predictor variable. When more time has passed since the last episode of violence, mental health symptoms have diminished, probably because the woman has had more time to reflect on the situation (Lazarus & Folkmann, 1984). Additional stressors also correlate with high indices of impaired mental health, as can be seen in similar results by Ceballo et al. (2004) in another Chilean sample. The study also confirmed that high levels of resilience predict low levels of psychological symptoms, as noted in other international studies from countries like Spain, Portugal, and the United States with a sample representing white/European, Caribbean, South Asian and Latin American women (Costa & Canossa, 2018; Crann & Barata, 2015; Fernández-Sánchez & López-Zafra, 2019).
Another question examined in the study was whether any mental health symptoms correlated significantly with the duration of the abusive relationship; according to the findings, none did. In this regard, Arbach and Bobbio (2018), Carlson and Dalenberg (2000) and Patró (2006) noted that the impact of traumatic experiences depends more on the intensity of the event than its duration. This could explain why the mental health variables did not significantly correlate to duration in this study. Additionally, the duration of violence may not correlate with PTSD because the women counted only the number of years the relationship lasted, though in many cases these women continued to experience aggressions after the end of the relationship.
In terms of the strengths of this study, the interview procedure was homogeneous for all participants. Since all the women had experienced trauma and thus merited a respectful setting ethically aligned with work with traumatized individuals, all interviews were one on one. Furthermore, this study is the first to report on the different mental health dimensions of Chilean women at government-run walk-in treatment centers considering the duration of the relationship, the type of violence, perceived social support, additional stressors, and the resilience that women present.
The study has certain limitations that should be considered. The data was gathered between 2009 and 2011, though the results obtained are similar to those of more recent studies (e.g., Viejo et al., 2018). In addition, because it is a cross-sectional study, few inferences can be made in terms of time or causal relations. The women recruited for the study visited walk-in treatment centers, which means the results cannot be extrapolated to the population living in shelters or outside of these centers. In addition, it was limited to the city of Santiago, meaning that any extrapolation to women in other regions of Chile would overlook rural/urban and regional variables. Finally, variables had to be categorized because the data did not meet parametric assumptions, suggesting that detailed information could have been lost.
For future research, crosschecking information with sources other than the victim and a larger sample size would be important. Violence against women is a mental health issue as demonstrated once again in this study, and the particularities of Chilean women must be considered in order to better serve them. Accordingly, there is a pressing need to continue researching this group, differentiating, for example, between women in Chilean cities who are living in a shelter, those going through legal proceedings (García-Jiménez et al., 2020), or women with disabilities (del Río et al., 2013). In addition, as pointed out by Vilariño et al. (2018), it is interesting to consider that the mental health of IPVAW victims may also be impacted by other events like legal proceedings, making it necessary to explore other stressors. Finally, the poor mental health indicators reveal a need for more research to evaluate the efficacy of the services provided at the Women’s Centers.
In terms of the implications for practice of this study, victimization by gender violence should not be seen only as a legal or social problem but also as a public health problem given the extent and severity of mental health damage, physical injuries, and the impact on other family members (Vilariño et al., 2018). The results of this investigation can contribute to improve the treatment for women receiving outpatient care at the SERNAM Women’s Centers, and its effectiveness. Some variables should be included when designing treatments that promote the recovery of women IPVAW survivors. Concretely, time since the last violent episode should be considered a priority criterion given that, when the trauma is recent, the woman is more negatively affected. Additionally, acting on additional stressors such as the lack of a stable job, support network, and childcare, among others, represent a fundamental strategy in the recovery of IPVAW survivors (Costa & Canossa, 2018; Zapor et al., 2018). Furthermore, personal resilience (Lutwak, 2018) should be promoted in order to help protect people against trauma (de la Rosa et al., 2016; Fernández-Sánchez & López-Zafra, 2019; Jose & Novaco, 2016). If these variables are not taken into account in technical guidelines, there is a risk that treatment may not be effective, and women may even be referred to other healthcare centers. In such cases, a woman is obliged to tell her story over and over again, thus running the risk of secondary victimization. In addition, these findings can be extrapolated to other women who have experienced violence by a current or former partner, thus providing useful information for different centers that promote trauma recovery. In summary, more treatments focused on strengthening the mental health and considering the history of violence, support, stressors, and resilience of IPVAW survivors are needed in Chile, as well as school programs to increase awareness from an early age and prevent this type of violence.
Supplemental Material
sj-pdf-1-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-1-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-2-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-2-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-3-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-3-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-4-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-4-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-5-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-5-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-6-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-6-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Supplemental Material
sj-pdf-7-jiv-10.1177_08862605211042810 – Supplemental material for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile
Supplemental material, sj-pdf-7-jiv-10.1177_08862605211042810 for Predictive Factors of Mental Health in Survivors of Intimate Partner Violence in Chile by Paloma Labra-Valerdi, Salvador Chacón-Moscoso and Susana Sanduvete-Chaves in Journal of Interpersonal Violence
Footnotes
Acknowledgments
We are very grateful to the Ministry of Women and Gender Equality (SERNAMEG). We would also like to thank Wendy Gosselin for the English translation and the readers whose contributions helped us substantially improve this work. Finally, we owe this study to the women who agreed to be part of our research, came to the outpatient centers to recover from the damage of IPVAW and wanted to help other women in similar circumstances.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was funded by Beca Presidente, a Chilean grant for graduate students abroad. Additional funding came from the Fondo Nacional de Desarrollo Científico y Tecnológico FONDECYT Regular, CONICYT, Chilean government (ref. no. 1190945); Programa Operativo FEDER Andalusia 2014-2020, Board of Andalusia, Spain (ref. US-1263096); and VI Plan Propio de Investigación y Transferencia (VIPPITUS), Universidad de Sevilla, Spain (ref. VIPP PRECOMPETI 2020/1333).
Supplemental Material
Supplemental material for this article is available online.
Supplementary file 1. Letters signed by SERNAM (English translation and original Spanish version)
Supplementary file 2. Informed consent letter (English translation and Spanish version)
Supplementary file 3. Structured interview (English translation and Spanish version)
Supplementary file 4. Resilience Scale SV-RES (Saavedra & Villalta, 2007) (English translation and Spanish version)
Supplementary file 5. General Health Questionnaire (GHQ-12) (Araya et al., 1992) (English translation and Spanish version)
Supplementary file 6. Severity Scale for Symptoms of Post-traumatic Stress Disorder (EGSTEP) (Echeburúa et al., 1997) (English translation and Spanish version)
Supplementary file 7. Beck’s Depression Inventory (BDI) (Beck et al., 1979) (open access English version and Spanish version)
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.