
Abstract
While population-based research confirms that women with disabilities abused by their intimate partners experience significant mental health issues, few studies compare this in intimate partner violence (IPV)-specific samples of women with or without disabilities and none analyze possible impacts based on disability type. This secondary mixed methods analysis examined 660 Canadian women (50.6% Indigenous, 43.1% White, and 6.1% visible minority) with respect to whether they reported having a disability that impacted their employability or daily living (291 or 44% yes; 369 or 56% said no). In the 291 women with disabilities, about one-third (30.7%) had a physical disability-only, one-quarter had a mental health disability-only, and 44.1% reported both physical and mental health disabilities. Women with mental health and both physical and mental health disabilities reported significantly more Severe Combined IPV on the Composite Abuse Scale, depression (CES-D-10; Center for Epidemiological Studies-Depression), psychological distress (Symptom Checklist Shortform-10; SCL-10; in the clinical range), PTSD symptoms (PTSD Checklist), and lower quality of life (Quality of Life Questionnaire or QoL-9) than women without disabilities. Education about disabilities is needed for IPV advocates and disability practitioners need education about IPV. Developing services specific to survivors of IPV with disabilities is recommended.
The serious nature and impact of intimate partner violence against women (IPV) has been acknowledged globally (World Health Organization, 2021). IPV includes physical, sexual, and emotional abuse against women by mostly male intimate partners, often usefully considered as “coercive control” (Stark & Hester, 2019). A small number of women are, sadly, murdered by their abusive partners, more than 1 in 10 homicides in the United States (Kafka et al., 2021), an issue of concern in Canada, the site of the current study, as well (Dawson, 2016; Johnson et al., 2019).
Women with disabilities are significantly more likely to report severe IPV in general population studies (Breiding & Armour, 2015; Brownridge, 2006; Coker et al., 2005; Hahn et al., 2014; Slayter et al., 2018) and meta-analyses (García-Cuéllar et al., 2023; Hughes et al., 2012). In contrast, a large study by Martin et al. (2006) in North Carolina concluded that women IPV survivors with disabilities were no more likely than women without to report physical violence only, however, four more times likely to have experienced a sexual assault, 44% of which were from a current or ex-partner.
Disabilities are chronic health conditions encompassing both physical and mental health concerns that result in limitations to daily activity or employment (Du Mont & Forte, 2014). The World Health Organization and World Bank (2011) uses a bio-psycho-social perspective of disability, citing Leonardi et al.’s (2006) definition as, “the umbrella term for impairments, activity limitations and participation restrictions, referring to the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors)” (p. 4). The current study adds to this discourse by descriptively examining the presence and type of disability and mental health symptoms of IPV survivors compared to those without disabilities in a large sample of Canadian women abused by intimate partners.
Theoretical Orientation: An Intersectionality Framework
Intersectionality is “a theoretical or analytical approach that simultaneously considers multiple categories of identity, difference, and inequality (such as gender, race, class, sexual orientation, disability, as well as others)” (Else-Quest & Shibley Hyde, 2016, p. 155). Originally developed as a counterpart to the notion that all women are at equal risk of IPV, intersectionality is a commonly used framework in IPV (Baird et al., 2021; Bent-Goodley, 2007), health (Hankivsky et al., 2010), and disability research (Cramer & Plummer, 2009; Liasidou, 2008; Lightfoot & Williams, 2009; Sasseville et al., 2022).
While gender and ethnic background are the most considered characteristics in intersectional analyses, disability (Ballan et al., 2017; Lightfoot & Williams, 2009) and child abuse history (Damant et al., 2008) are also variables that are especially relevant when studying IPV. Nevertheless, national studies that focus on racial background and IPV seldom use standardized assessments of mental health symptoms (e.g., Du Mont & Forte, 2014). Studies that focus on disability status and IPV may not collect information on race and ethnicity (e.g., Brownridge et al., 2022; M. M. Cohen et al., 2005; Du Mont & Forte, 2014; Yoshida et al., 2011), important to an intersectional analysis, an exception being Cimino et al. (2019).
Women Abused by Intimate Partner and Disabilities
Having a disability can leave women vulnerable to predation by IPV abusers (Ballan et al., 2014; García-Cuéllar et al., 2023; Iudici et al., 2019; Muster, 2021; Yoshida et al., 2011). Further, given the physical nature of much IPV, many women suffer long-term physical consequences (Dutton, 2009), which may or may not constitute disabilities. In a national U.S. study, Breiding and Armour (2015) found that women with disabilities were significantly more likely to report physical violence, stalking, and partner sexual assaults, a finding generally supported in U.S. population-based research (Hahn et al., 2014), in Canada (Brownridge, 2006), and globally (Gupta et al., 2023).
Others examine IPV in populations of women with disabilities (e.g., Ballan et al., 2014; Barrett et al., 2009; Du Mont & Forte, 2014; Yoshida et al., 2011). Some limit their study to specific disability subtypes such as developmental disabilities (Platt et al., 2017), physical disabilities (Nosek et al., 2006; Yoshida et al., 2011), mental health disabilities (Du Mont & Forte, 2014), Deaf women (Ballan et al., 2017; Mastrocinque, 2022), or activity limitations (Brownridge et al., 2016; M. M. Cohen et al., 2005, 2006).
As the IPV can be traumatic, many survivors are diagnosed with significant mental health conditions, including depression, anxiety, and posttraumatic stress disorder (PTSD; Brownridge et al., 2022; Coker et al., 2005; Ferrari et al., 2016; Perez & Johnson, 2008; Tutty, Radtke, Ateah, et al., 2021; White & Satyen, 2015; Woods, 2005). However, only some authors specify when these mental health issues can be considered disabilities (Brownridge et al., 2022; Coker et al., 2005; Mengo et al., 2020; Tutty, Radtke, Ateah, et al., 2021). Most studies on IPV and disability status do not address mental health issues or use standardized measures of mental health, exceptions being Hahn et al. (2014), Ford-Gilboe et al. (2015), and Wuest et al. (2010). Interestingly, as part of the same large study, Ford-Gilboe et al. (2015) and Wuest et al. (2010) examined populations of women with IPV and whether they reported a disability (similar to the current research) but neither study documented differences in mental health scores comparing whether or not the women had disabilities.
The type of disability in women abused by intimate partners, whether physical or mental health, has seldom been compared. An exception is the research by Ballan et al. (2014), who identified four forms of disability (physical—56.3%, psychiatric—71.8%, sensory—13.5%, and developmental—8.4%) in their sample of 888 women reporting IPV but used the information only descriptively.
A history of child abuse has also been correlated with mental health disabilities (often among survivors of child sexual abuse) or physical disabilities (often because of child physical abuse; Ballan et al., 2014) or both (Plummer & Findley, 2012). PTSD has often been associated with childhood abuse, especially child sexual abuse (Clemmons et al., 2007) and IPV (as noted previously). Given that many women experience both (Widom et al., 2014), the interconnections are important (Becker et al., 2010; Nicolaidis et al., 2009).
Rationale for the Current Study
Given that relatively few studies have focused on the mental health and well-being of women abused by intimate partners who have disabilities and that used standardized measures (exceptions being Hahn et al. (2014), Ford-Gilboe et al. (2015), and Wuest et al. (2010)), the current study explores this further with respect to a large sample of 660 abused Canadian women who participated in the “The Healing Journey” study. A large number of these were Indigenous women, a population identified as reporting significantly more IPV in Canadian population-based research (Statistics Canada, 2021). Heidinger (2021) notes that, “a significantly larger proportion of Indigenous women with a disability (74%) experienced IPV in their lifetime compared with Indigenous women without a disability (46%)” (p. 6). We compare the IPV, mental health, and demographic characteristics with respect to the type of disability versus no disability for the 291 women with disabilities compared to the 369 women without, a novel examination.
A book chapter using the same dataset (Owen & Ursel, 2020) analyzed the characteristics of abused women with both “chronic illnesses and disabilities” (N = 416), a broader definition than that used in the current analysis, which is specific to illnesses that affected employment or the activities of daily living (Du Mont & Forte, 2014). Owen and Ursel looked at a small number of variables: racial identity (no differences), child abuse (more women with disabilities reported this), whether the women saw the illness as caused by child (6.1%) or partner abuse (28.1%), and use of shelters and police services. While interesting, we argue that a more comprehensive examination of the data about women with disabilities is warranted.
Method
The data for this secondary analysis were from the “The Healing Journey,” a longitudinal, Canadian study with a convenience sample of 660 women who had experienced IPV in the three prairie provinces of Alberta, Saskatchewan, and Manitoba. The original study assessed characteristics of women abused by intimate partners including mental health and general well-being (Tutty, Radtke, Ateah, et al., 2021), experiences of mothering (Ateah et al., 2019; Nixon et al., 2017), and followed the women longitudinally over 2.5 years (Tutty, Radtke, Thurston, et al., 2021). Both academics and community agency personnel were part of a large research team. Data were collected in seven waves between 2005 and 2009, with one wave specific to an economic analysis (DeRiviere, 2014).
Study Participants
The research protocols were approved by the Research Ethics Boards of the six associated universities (Universities of Calgary, Manitoba, Regina, Brandon, Lethbridge, Winnipeg). Each province conducted an environmental scan of IPV-specific agencies (i.e., women’s shelters and counseling agencies) to cover urban, rural, and northern sites from which to recruit. On the basis of posters or referrals from agency staff, the women volunteered for the study as long as they fit the inclusion criteria of: minimum 18 years of age; the most recent incident of IPV no sooner than 3 months and no longer than 5 years prior; commitment to stay in the study for the full 2.5 years; and no debilitating mental health issues such as hallucinations or confusion that would prevent their responding to the complex study measures (no one was excluded for this). Honoraria ($50 CAN) were given to participants at each wave.
Demographics of the Total Sample
The 660 women respondents were an average age of 36.4 years (SD = 10.9), while their partner/ex-partners were an average of 38.7 years (SD = 11.2). The women’s racial backgrounds were 50.6% Indigenous, 43.3% White, and 6.1% visible minority, while the partner/ex-partners (N = 654) were White (47.6%), Indigenous (44.5%), and 8% visible minority. Most of the women (90.6%) had children. With respect to their highest level of education, 42.3% of the women had not completed high school, 21.1% had completed high school, while 36.7% had some post-secondary education, either in technical institutes (17.3%) or universities (19.4%). Their average total income in the past year was $21,693 (SD = $24,556); about half of the women’s incomes fall below the poverty line for that time in the three Canadian provinces (DeRiviere, 2014). This low yearly income is partly explained by the fact that the majority or women (61.5%) were not currently working, another 17.4% worked casually or part-time, and only 21.1% worked full-time. With respect to a history of child maltreatment, 21.1% reported none, 24.7% reported a child abuse history not including child sexual abuse, and over half (54.2%) reported having been sexually abused as children.
A comprehensive list of the self-reported medical conditions that fit the definition of a disability is beyond the scope of the current submission, especially because many women disclosed multiple conditions. Nevertheless, to highlight the serious and life-threatening nature of the disabilities, the most often mentioned physical conditions were back pain and spine and bone injuries (39), various forms of arthritis (26), Asthma/Emphysema/COPD (Chronic obstructive pulmonary disease) (26), irritable bowel syndrome/Crohn’s disease (26), chronic fatigue/fibromyalgia (25), and hepatitis C and HIV (19). Of the mental health disabilities, the most common were depression (98), PTSD/anxiety (65), and addictions (37). Also, 12 women mentioned bipolar disorder and 6 self-disclosed a diagnosis of borderline personality disorder.
Research Measures
Data in the original study were collected with respect to four major areas: demographic background and history of abuse, general functioning and service utilization, health, and mothering. The surveys included standardized measures as well as open- and closed-ended questions developed specifically for the study (all administered verbally by trained research assistants). The current secondary analysis used data from the first two waves of the Healing Journey study, which constitute the study baseline. The core demographics, including disability status, the severity of the IPV, and Quality of Life were obtained in Wave 1. Mental health measures were collected in Wave 2.
Intimate Partner Violence
The nature of the IPV was assessed by the Composite Abuse Scale (CAS; Hegarty et al., 2005), a 30-item self-report screening measure. The items reference whether partners took certain actions (past 12 months), and the frequency of such actions in a 6-point Likert scale of never (0), only once (1), several times (2), once per month (3), once per week (4), or daily (5). The four subscales are: Severe Combined Abuse (8 items; range of scores 0–40; suggested cutoff of 1), Physical Abuse (7 items; range of scores 0–35; cutoff of 1), Emotional Abuse (11 items; range of scores 0–55; cutoff of 3), and Harassment (4 items; range of scores 0–20; cutoff of 2). Scores for the subscales and total measure are summed for a total score of 0 to 150 (Hegarty et al., 2005) with higher scores indicating more serious IPV. The clinical cutoff for the entire scale is 7 (Hegarty et al., 2005). The CAS has strong criterion and construct validity, as well as internal reliability (α = .85); the subscales also have a Cronbach’s alpha of .85 or above (Hegarty et al., 2005). Cronbach’s alpha in the Healing Journey study is .93.
Intimate Partner Sexual Assault
Intimate partner sexual assault was determined by answers to item 7 from the CAS, “My Partner: Raped me.” In scoring the CAS, this item is included in the Severe Abuse subscale.
Disability
We asked the women to self-report physical and mental health conditions (whether or not diagnosed by medical personnel) and, to assess whether these constituted a disability, we asked whether these conditions affected their employability or the kind or number of daily activities (also termed “participation restrictions”), consistent with Leonardi et al. (2006). The women were also asked whether they attributed their disability to any form of abuse (IPV, child abuse, or both).
Child Abuse History
Child abuse history was collected via structured questions (yes/no answers): “Were you abused as a child or adolescent? (a) physical, (b) sexual, (c) emotional/psychological, (d) witnessing abuse among family members” (consistent with Elias et al., 2012).
Mental Health and Well-Being
The Symptom Checklist Short Form (SCL-10; Nguyen et al., 1983) is a screening tool to assess global mental health functioning and psychological distress in the previous week. Items (e.g., “In the past week, how much were you distressed by feeling lonely?”) are endorsed with a 0 to 4 Likert scale (0 = not at all; 4 = extremely). Item scores are summed with a range from 0 to 40, with higher scores indicating more distress. Higher scores indicate more distress. Published clinical cutoffs for the 10-item version were not found. However, since clinical cutoff scores are one standard deviation above the mean (Jacobson et al., 1984), we used Müller et al.’s data (2010) reporting a mean score of 7.8 (SD of 6.3), resulting in a clinical cutoff score of 14.2. Cronbach’s alpha in the Healing Journey study is .89.
The CES-D-10 (Center for Epidemiological Studies-Depression) is a short form of the CES-D-20 (Radloff, 1977) used to document depression symptoms in the previous week (Andresen et al., 1994). Ten items (e.g., “In the past week I was bothered by things that usually don’t bother me?”) are rated on a 0 to 3 Likert scale, with 0 as rarely or none of the time (<1 day)” and 3 as all of the time (5–7 days). Internal consistency and test-retest reliability are good (Björgvinsson et al., 2013). Cronbach’s alpha in the Healing Journey study is .84. Björgvinsson et al. suggest that a cutoff of 15 has the best sensitivity and specificity.
The PTSD Checklist (PCL; Blanchard et al., 1996) is a 17-item self-report questionnaire that measures PTSD symptoms in the past month. Items (e.g., “In the past month how much have you been bothered by repeated, disturbing memories, thoughts or images of abuse or violence?”) are endorsed with a 0 to 4 Likert scale with 0 meaning not at all and 4 meaning extremely. Item scores are summed with a range from 0 to 68, with higher scores indicating more PTSD. The PCL has demonstrated validity and reliability (Blanchard et al., 1996; Wilkins et al., 2011). Blanchard et al. recommend a clinical cutoff of 44. The scale has good psychometric properties (Cronbach’s α = .94; Blanchard et al., 1996). Cronbach’s alpha in the Healing Journey study is .92.
The original 25-item Quality of Life Questionnaire (Andrews & Withey, 1976) was shortened by Sullivan and Bybee (1999) to 9 items (QoL-9) measuring satisfaction with her overall quality of life (e.g., “How do you feel about life as a whole”) and satisfaction with particular areas (e.g., “How do you feel about yourself?; your personal safety?; the amount of fun and enjoyment you have?”). Items are rated on a 7-point scale (1 = extremely pleased, 7 = terrible) and are summed and reverse-scored (range of 0 to 63). Higher scale scores indicate better QoL. Cronbach’s alpha in the Healing Journey study is .84.
Quantitative Data Analysis
The demographic characteristics of the women and their scores on the CAS are presented descriptively. Demographic characteristics of the women and both whether they reported a disability, and the type of disability are compared using Pearson’s chi-square analysis, with effect sizes calculated with Phi or Cramer’s V. Standardized residuals were calculated to identify the category differences responsible for the statistically significant chi-square analysis (Field, 2009). Effect sizes were interpreted using Rea and Parker’s (1992) suggested benchmarks of under .10 as a “negligible” association; between .10 and under .20 as a “weak”; between .20 and under .40 as a “moderate”; and between .40 and under .60 as a relatively “strong” association (p. 203).
To examine differences by disability type (physical disability only vs. mental health disability only vs. physical and mental health disability) on the standardized measures, we used ANOVAs. When a significant F-test was identified, Bonferroni post hoc analyses were used to indicate between which of the three groups the significance lay (Field, 2009). For F-tests, eta-square (η2) is used to estimate effect sizes with η2 = .01 indicates a small effect; η2 = .06 indicates a medium effect; η2 = .14 indicates a large effect.
Qualitative Data Analysis
After being administered the CAS (which has no question specific to abuse with respect to having a disability), the women were asked an open-ended question about whether they had additional experiences or comments. The responses to this from the 291 women with disabilities were qualitatively analyzed for information about the nature of the IPV, especially whether the abuse was specific to having a disability.
We used descriptive qualitative health research to analyze the women’s comments about their partner’s abusive acts. This method is particularly appropriate for mixed methods research (Neergaard et al., 2009) and for “assessing, developing and refining interventions with vulnerable populations” (Sullivan-Bolyai et al., 2005, p. 127). Descriptive qualitative methods use the practicality of the research question as the guiding principle, rather than focusing on the epistemological confines of qualitative traditions such as phenomenology or grounded (Neergaard et al., 2009). The descriptive analysis followed established inductive content analysis processes (the meaning emerges from the narratives; Elo & Kyngäs, 2008; Sandelowski, 2000).
Results
Comparison between Women with No Disability and Type of Disability
As can be seen in Table 1, 369 women did not self-disclose a disability. Of the 291 women with a disability, about one-third (30.7%) had a physical disability only, one-quarter had a mental health disability only, and 44.1% self-reported having both a physical and a mental health disability. As compared to women without a disability, women with a physical and both a physical and mental health disability were significantly older than those without a disability and those with only a mental health disability, and the identical findings applied to the age of the partners. Women with mental health disabilities reported the lowest yearly income, which was significantly less than women with no disabilities. Fewer women with both physical and mental health disabilities and more women without disabilities currently worked full-time. Women with mental health-only disabilities were the least likely to be working full-time. A higher proportion of women without disabilities reported no child abuse or child sexual abuse. Two thirds (68%) of the women with disabilities perceived their disability as resulting from abuse (both childhood and IPV). More women with physical disabilities were unsure about whether they linked their disability to child abuse or IPV.
Comparison of Women’s Demographics by Disability Linked to Type of Disability (N = 660).
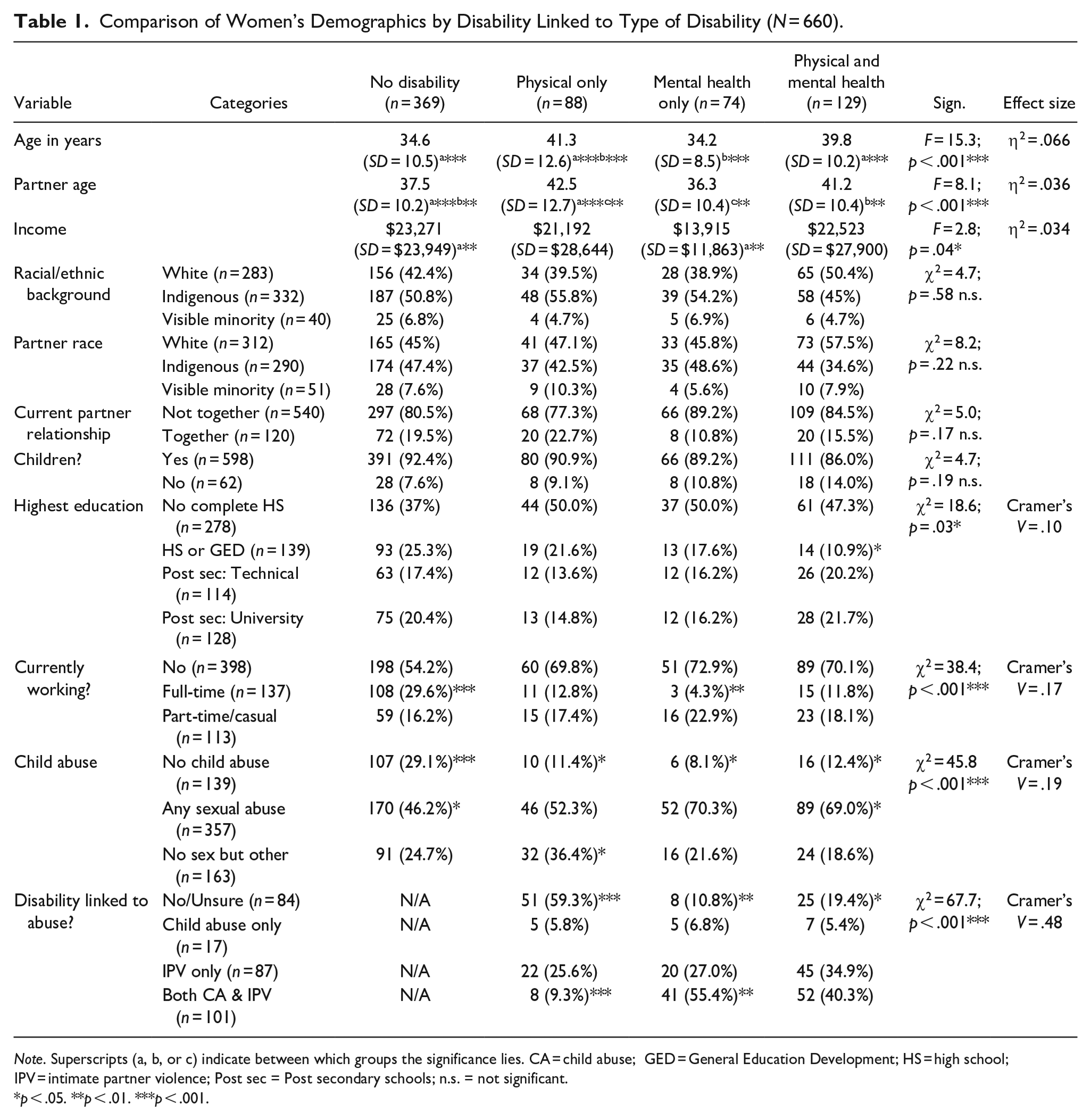
Note. Superscripts (a, b, or c) indicate between which groups the significance lies. CA = child abuse; GED = General Education Development; HS = high school; IPV = intimate partner violence; Post sec = Post secondary schools; n.s. = not significant.
p < .05. **p < .01. ***p < .001.
In Table 2, women without disabilities reported less serious IPV on most of the CAS subscales (with the exception of the Emotional subscale and the Harassment subscale in which women with mental health-only disabilities reported more serious harassment than women with physical-only disabilities). On the Severe Combined Abuse subscale, women without disabilities reported significantly less IPV than women with mental health-only or both physical or mental health-only disabilities but not different than women with physical disabilities-only. The Total CAS score was significantly lower (less IPV) for women without disabilities than for women with both physical and mental-health disabilities. Women with mental health or both physical and mental health disabilities were more likely to have been sexually assaulted by their partners than women with no disabilities or physical-only disabilities.
Scores on Standardized Measures by Type of Disability (N = 291).
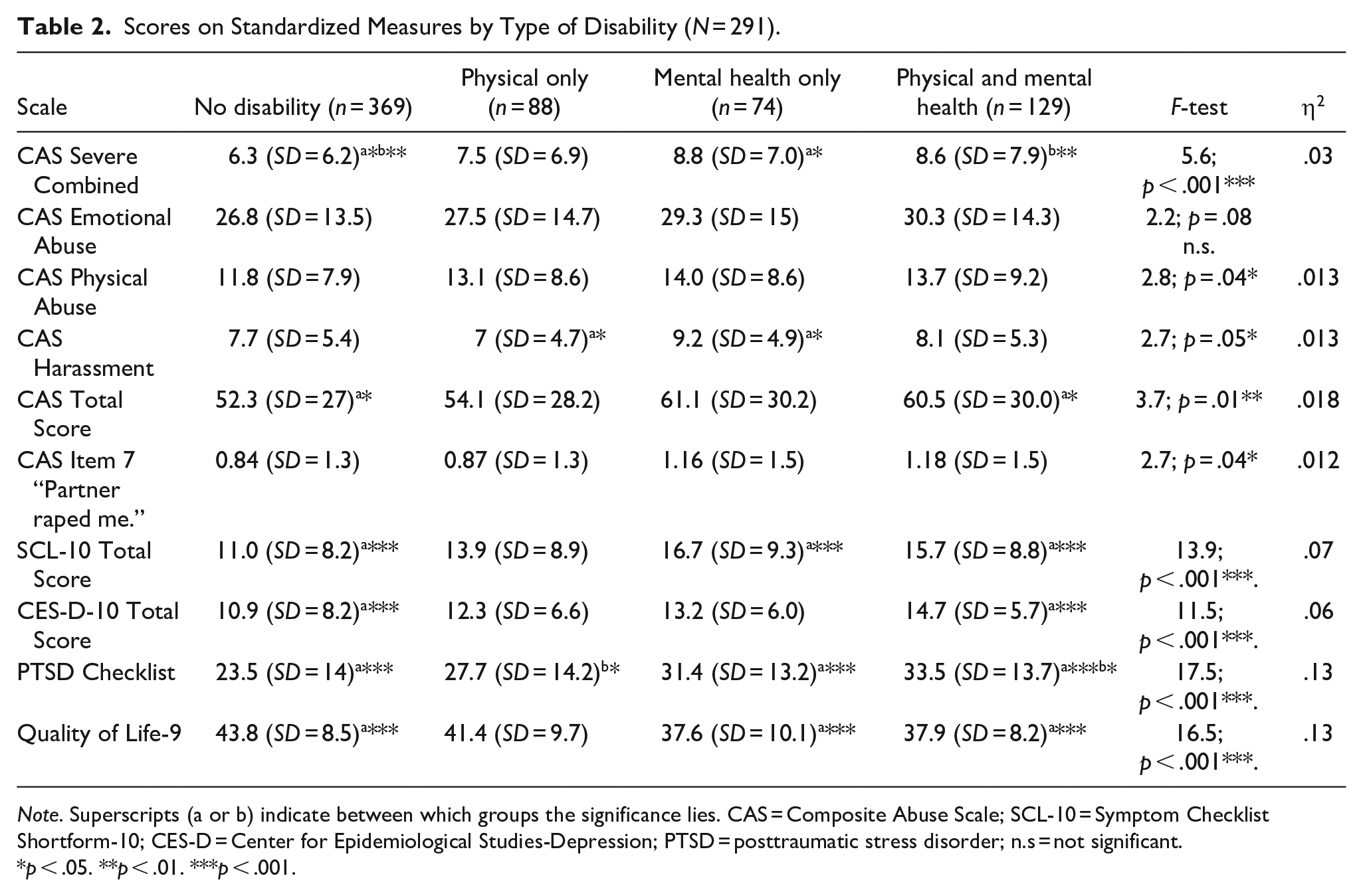
Note. Superscripts (a or b) indicate between which groups the significance lies. CAS = Composite Abuse Scale; SCL-10 = Symptom Checklist Shortform-10; CES-D = Center for Epidemiological Studies-Depression; PTSD = posttraumatic stress disorder; n.s = not significant.
p < .05. **p < .01. ***p < .001.
With respect to psychological distress as measured by the SCL-10, women without disabilities had significantly few symptoms than women with mental health and physical and mental health disabilities (the latter scored about the clinical cutoff). Women without disabilities reported fewer depression symptoms than women with both physical and mental health disabilities (although all scores were below the clinical cutoff). While the average scores on the PCL were also all below the clinical cutoff, women without disabilities reported the fewest symptoms as compared to women with mental health-only and physical and mental health disabilities. This pattern was also evident for scores on the Quality-of-Life measure (which has no clinical cutoff), such that women without disabilities reported the highest QoL compared to women with mental health-only and physical and mental health disabilities.
Qualitative Themes Regarding Abuse and Disability
The comments from the 291 women with disabilities were analyzed to explore the nature of the IPV and to examine whether any of their partner’s abusive actions seemed specific to their disability status. Some comments were short, others more comprehensive. The most frequently mentioned abuses were extreme control (103), threats to kill/hurt the woman and/or her loved ones (72), severe physical abuse (34), and sexual assaults/other forms of sexual abuse (24; note that a number of women documented more than one form of severe abuse).
With respect to extreme control, of the 103 comments, 25 referenced being locked in rooms or out of the house: “My ex-partner had locked my in a bedroom after he had beaten me;” “He had so much power he could lock me out of rooms, and I would have to beg for him to unlock the door and resolve things.” Comments about threats to kill/hurt the women or others she loved included the following: “Threatened me. Stated ‘hit and runs happen all the time.’ He said this when I threatened to leave him;” “He threatened to kill my family members. Said if we went to sleep, he would burn the house down.” “Out hunting, I became the hunted—threatened to shoot me.” “Would tell me I am one bullet away from dying.”
Examples of comments documenting severe physical abuse include the following: “Threatened me with scissors at my throat. Banged my head against a wall. Tried to choke me, punched me in the face. Lots of bruises—but not obvious; never my face;” “He has attempted to choke me on many occasions. He has choked me with phone cords. He hit me in the face with the butt of a gun causing permanent eye damage.” Comments regarding sexual assaults or other sexually abusive behavior included: “Forced me to have sex with ex-partner’s friends. He had sex with my friends in front of me,” “He brought pornography. He would pressure me to do some of the sexual acts in the book. I said no, and he would imply there was something wrong with me”; and “Locked us both in the bedroom and raped and beat me. Had sex with another woman, then came back and forced me to have sex.”
While the comments detailed significant IPV, relatively few were specific to the women’s disabilities. Of the 14 comments that referred to any disability, most were about the women’s medications, such as: “He often told me that I was a hinderance to him because he had to buy my pills.” “Threatened to take my meds (for a back injury);” “Didn’t want me taking antidepressants, I felt crazy without them.” “Kept my meds so I couldn’t take them.” “Stole my meds to get high so I couldn’t walk for 4 days”; and “Replaced my diabetes medication with extra strength Tylenol.”
Comments not specific to medication included the following: “If I didn’t do what he wanted he would punch or knee me in the abdomen. This was a big problem with my ileostomy; he would try to pull it off”; “Used my Bipolar diagnosis against me”; and “He would make me walk to the hospital with my bad back to punish me.”
Discussion
Consistent with the population-based studies comparing women with disabilities and IPV to women affected by IPV but no disability (Breiding & Armour, 2015; Brownridge, 2006; Coker et al., 2005; Hahn et al., 2014; Slayter et al., 2018), the women with mental health and both physical and mental health disabilities in the current study reported significantly more significant IPV than women with no disabilities, as measured by the CAS Severe Combined subscale and Total score. They also reported signifcantly more serious mental health concerns such as depression, PTSD, a lower quality of life, and more serious psychological distress (SCL-10), although only scores on the latter measure were in the clinical range. The IPV and mental health scores of the women with physical-only disabilities were more simlar to women without disabilities. Interestingly, though, unlike Heidinger (2021), there were no significant differences in the proportions of disability types for the Indigenous women as compared to White and visible minority women.
Although one might expect women with any mental health disabilities to report more symptoms on the depression, psychological distress, and PTSD measures, these scales measure symptoms in the last week or month (PCL) and are not directly linked to a diagnosis. Current depression, stress, or PTSD may be controlled by medication or changed life circumstances, supporting the rationale for conducting the current analyses.
Women with disabilities are often also disadvantaged by structural inequalities associated with race, gender, age, and socioeconomic status (Ballan et al., 2014), which could contribute to the poorer psychological well-being associated with women with both mental health and physical and mental health disabilities in our study. Fewer women with both physical and mental health disabilities had completed high school, and fewer women with mental health-only disabilities worked full-time. Similar to Martin et al. (2006) who found that women IPV survivors with disabilities were four more times likely to have been sexual assaulted by a current or an ex-partner, in our study, more women with mental health-only or both physical and mental health disabilitites endorsed the CAS item that they were raped by their partners.
The qualitative analysis of comments made by the women with disabilities adds context to the high CAS scores, providing examples of the nature the partner abusive acts and highlighting significant control, serious physical abuse, threats to kill or harm the women or loved ones, and sexual assaults. While a comparison was not made to the comments from the women without disabilities, a more detailed qualitative analysis of the comments from all 461 women who answered this question has been conducted to assess the extent to which the CAS addressed the severity and nature of the partner’s IPV (Tutty & Nixon, under review).
Clinical Implications
The current study confirms the importance of assessing for both IPV and disability status; however, a major problem is that neither focus is commonly taught in the professional education of social workers, psychologists, and health care workers (Black et al., 2010; Ruiz-Pérez et al., 2018; Sasseville et al., 2022; Slayter, 2009; Slayter et al., 2018). To corroborate this, women with disabilities have estimated that only 15% of health providers assessed them for IPV (Curry et al., 2011).
Similarly, when working with women abused by intimate partners, it is important for professionals to assess disability status. In focus groups with professionals, Lightfoot and Williams (2009) concluded that many lacked knowledge about disabilities. Similarly, Mengo et al. (2020) conducted a study of IPV providers examining knowledge and reactions to women with mental health disabilities, finding important gaps and opportunities for improvement.
We agree with Baladerian (2009) about the insufficient discussion of disability in the IPV literature, and the lack of services specific to women with disabilities and an IPV history (Lund, 2011; Namatovu et al., 2024), although some exist: Ballan et al. (2014) describe a non-residential domestic violence disability program and Ballan et al. (2017) describe an IPV program for Deaf women. Another exception is Ballan et al. (2017) who describe trauma-informed counseling for women with disabilities whose partners have abused them.
The current study supports the need for additional research on the complexities faced by women with disabilities who were also abused by intimate partners such as details about the assistance that they sought and the reception from both IPV advocates and disability professionals, similar to Curry et al. (2011). In agreement with the discussion about disability education (i.e., Lightfoot & Williams, 2009; Mengo et al., 2020), we recommend that IPV professionals be trained to assess for disability status and that professionals working with women with disabilities learn how to assess for IPV.
Study Strengths and Limitations
When using secondary data sources, one is limited by the nature of the original study, which, in this case, relied on a convenience sample of women from violence against women (VAW) shelters or counseling agencies. The current results are not generalizable to other disabled women abused by intimate partners from Canada’s prairie provinces, nor was the intent to imply cause and effect.
The women self-reported their physical and mental health conditions without confirmation through a formal diagnosis. Nevertheless, the disability community promotes self-identification as an accurate method of establishing disability status (Owen & Ursel, 2020).While the exclusion criteria mentioned women with no debilitating mental health issues, none were excluded based on this. We do not know why none of the women disclosed intellectual or developmental disabilities, but it is possible that these women were connected to disability services rather than IPV services.
Disability status might have been measured more comprehensively with a standardized measure. While comprehensive scales to categorize type of disability have now been published, such as the WHODAS 2.0 (Chen et al., 2022) or the Canadian Disability Screening Questions that identify difficulties related to hearing, vision, mobility, flexibility, dexterity, learning, developmental, memory, pain, or mental health (Savage, 2021, p. 4), neither was developed when the Healing Journey Study was conceptualized. As well, assessing disability though questions related to limitations to daily activity or employment is consistent with other IPV researchers (Barrett et al., 2009; Brownridge et al., 2022; M. M. Cohen et al., 2005; Du Mont & Forte, 2014; Yoshida et al., 2011).
Unlike the bulk of the research in disability and mental health, the current study used standardized measures with clinical cutoff scores to conceptualize mental health disorders (others include Hahn et al. (2014), Ford-Gilboe et al. (2015), and Wuest et al. (2010)), Further, the women were not asked a question specific to their partner’s abusive acts that directly affected their disabilities. This would be of interest in future research.
A strength of the current study is that the survey included questions that allowed us to identify disability based on employability and effects on daily function, consistent with the most common definition (Du Mont & Forte, 2014), as well as asking women whether they attributed their disabilities to any forms of abuse and whether the disability constituted physical-only, mental health-only, or a combination of both. This enabled statistical comparisons that have not previously been documented.
The study includes a large sample of Indigenous women, whose IPV with respect to disability has not previously been documented, even though several Canadian population-based or large studies on disability status have been conducted (i.e., Brownridge et al., 2022; Du Mont & Forte, 2014; Yoshida et al., 2011). Finding no significant differences in the proportion of Indigenous women with disabilities compared to other racial identity groups covered in the study is of interest, since, given their significant histories of child abuse and colonization (Burnette, 2016; Ogden & Tutty, 2023), one might have expected that a larger proportion would self-report disabilities.
Conclusion
The women abused by intimate partners involved in the “Healing Journey” study constitute a large sample from the Canadian prairie provinces, including more than half being of Indigenous populations, a group considered of particular importance given their over-representation in Canadian gender-based violence statistics. That 44% met the definition of having a disability is notable. The women’s willingness to disclose their experiences in detail, whether with respect to the sensitive issues of IPV or mental health concerns in response to standardized measures or to open-ended survey questions, is notable.
Footnotes
Acknowledgements
The CURA team: Dr. E. Jane Ursel and Marlene Bertrand (Manitoba Department of Family Services and Housing, MB) are the Co-Principal Investigators; Dr. Kendra Nixon, Dr. Christine Ateah, Dr. Janice Ristock; Dr. Lori Wilkinson; Colin Bonnycastle; Dr. Jocelyn Proulx (University of Manitoba); Dr. Johanna Leseho; Dr. Roberta Graham (Brandon University); Dr. Linda DeRiviere; Dr. Michelle Owen (University of Winnipeg); Anna Pazdzierski (Nova House, Selkirk, MB); Karen Peto (YWCA Brandon); Margaret Marin & Darlene Sutherland (Osborne House, Winnipeg); Dr. Mary Rucklos Hampton, Dr. Bonnie Jeffery; Dr. Darlene Juschka; Dr. Wendee Kubik (University of Regina); Dr. Stephanie Martin (University of Saskatchewan); Carol Soles (Prince Albert Emergency Shelter for Women); Debra George (Family Services Regina); Dr. Karen Wood (Tamara’s House, Saskatoon); Maria Hendrika (Provincial Association of Transition Houses Saskatchewan); Angela Wells (Family Support Centre, Saskatchewan); Dr. H. L. Radtke; Dr. Leslie M. Tutty; Dr. Wilfreda (Billie) Thurston; Dr. Erin Gibbs Van Brunschot (University of Calgary); Dr. Caroline McDonald-Harker (University of Alberta); Dr. Ruth Grant Kalischuk (University of Lethbridge); Jan Reiner & Carolyn Goard (Alberta Council of Women’s Shelters); Brenda Brochu (Peace River Regional Women’s Shelter); Kristine Cassie (YWCA Lethbridge); Pat Garrett (WINGS of Providence, Edmonton).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding from: Social Sciences and Humanities Research Council (SSHRC) Community University Research Alliance (CURA); Alberta Centre for Child, Family, & Community Research; Alberta Heritage Fund for Medical Research; the PrairieAction Foundation; and TransCanada Pipelines.