
Abstract
Deep vein thrombosis (DVT) poses a significant global health challenge that affects patients’ physical function and symptom burden. Evidence on the health-related quality of life (HRQoL) of patients with DVT remains scarce in Ethiopia. This study aimed to assess DVT-specific quality of life and associated factors among patients with DVT. A hospital-based cross-sectional study was conducted at Tikur Anbessa Specialized Hospital, Ethiopia, in which 123 adults with confirmed DVT were recruited. Data were collected using the Amharic version of the Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Symptoms (VEINES-QOL/Sym) questionnaire, supplemented with clinical and demographic data. VEINES-QOL/Sym scores were standardized to T-scores (mean = 50, SD = 10), with raw scores scaled 0-100 (higher values indicated better HRQoL). Data were analyzed using Statistical Package for the Social Sciences version 28. Binary logistic regression was used to identify factors associated with HRQoL, with statistical significance set at P < .05. Among 123 patients (73.2% provoked, 93.5% unilateral DVT), VEINES-QOL ranged 33.4-59.6 and VEINES-Sym 26.7-58.7, both with a mean value of 50. Longer time since diagnosis was significantly associated with improved QoL (AOR = 1.922; 95% CI 1.155-3.199; P = .012), while proximal DVT (AOR = 0.240; P = .008), combined proximal/distal DVT (AOR = 0.136; P = .014), and post-thrombotic syndrome (PTS) (AOR = 0.108; P = .017) predicted poorer outcomes. In conclusion, VEINES-QOL/Sym scores indicated average QoL with modest improvement over time. Routine HRQoL assessment, PTS prevention, and improved monitoring, adherence, and patient education are recommended to strengthen DVT care in Ethiopia.
Keywords
Introduction
Deep vein thrombosis (DVT) is a serious medical condition characterized by the abnormal formation of blood clots in the deep veins, typically in the legs. DVT can lead to complications such as swelling, pain, and redness, and if left untreated, it may result in a potentially fatal condition called pulmonary embolism (PE).1–3 Collectively, DVT and PE are known as venous thromboembolism (VTE), which represents a significant global health burden, affecting over one million people annually in Europe alone and ranking as the third most common cardiovascular disease worldwide.2,3 Beyond the acute morbidity and mortality associated with DVT, it can also cause long-term complications such as PTS, reported in 20%-40% of patients. 4 PTS can lead to chronic leg pain, swelling, ulcers, and significant impairment in mobility and daily functioning. 5 These long-term consequences often persist even after clinical recovery, making patient-reported outcomes an essential component of evaluating long-term disease impact in DVT patients.6,7 While general instruments such as the SF-36 and EQ-5D measure overall HRQoL, disease-specific instruments like the VEINES-QOL/Sym provide targeted insight into symptom burden and functional limitations related to venous disorders. 8
In Ethiopia, DVT remains under-recognized and under-studied, with challenges such as delayed diagnosis, limited awareness, and inadequate healthcare infrastructure compounding its impact. While recurrence and clinical predictors of DVT have been studied locally, 9 there is a critical lack of evidence on HRQoL outcomes in Ethiopian patients. This gap is significant given that systemic resource constraints and psychosocial stressors, like fear of recurrence and limited support, may further impair QoL.3,10
International findings support the importance of contextual factors in determining HRQoL outcomes for DVT patients. For example, VEINES-QOL/Sym scores were significantly lower among Norwegian patients with PTS (mean: 40.6 vs 54.2, P < .001), 11 and similar reductions were reported in studies from China, Pakistan, and Europe, where PTS, anxiety, physical inactivity, and anticoagulation challenges were key predictors of poor outcomes.1,3,7,12 This study aims to address this evidence gap by assessing HRQoL and its associated factors among DVT patients in Ethiopia, providing critical insights for patient-centered care, policy development, and locally relevant interventions to improve outcomes in low-resource settings.
Methods
Study Setting
The study was conducted at Tikur Anbessa Specialized Hospital (TASH) in Addis Ababa, Ethiopia, which provides advanced medical care, including the diagnosis and treatment of VTE. TASH was chosen based on high patient volumes and capacity to manage DVT cases, offering an ideal setting to evaluate HRQoL and associated factors among patients with DVT.
Study Design and Period
A cross-sectional design was employed between January 23 to May 05, 2025, to evaluate the HRQoL and its determinants among patients with DVT using structured interviews and reviews of patient medical records.
Source and Study Population
The source population for this study included all patients with a confirmed diagnosis of DVT who were attending the hematology clinic of TASH. The study population consisted of those patients who met the inclusion criteria and received care during the study period.
Eligibility Criteria
The study applied clear inclusion and exclusion criteria to identify eligible participants. Adult patients (≥18 years) with confirmed DVT, receiving follow-up at the hematology clinic of TASH, and who provided informed consent were included in the study. Patients who were unable to complete the HRQoL assessment or who declined or withdrew consent were excluded from the study.
Sample Size Determination and Sampling Techniques
The study targeted the entire accessible population of deep vein thrombosis (DVT) patients who met the eligibility criteria and visited the hematology clinic at the Tikur Anbessa Specialized Hospital (TASH) during the data collection period. Eligible patients were consecutively recruited throughout the data collection period (January 23 to May 05, 2025), which resulted in a final sample of 123 participants. 13
Data Collection and Procedures
The HRQoL of study participants was evaluated using the VEINES-QOL/Sym questionnaire. This is a validated 26-item, patient-reported instrument developed through the Venous Insufficiency Epidemiological and Economic Study. It is designed specifically for individuals with DVT and measures the impact of the condition on symptoms, daily activities, and overall QoL. 13 The questionnaire produces two summary scores: VEINES-QOL for QoL and VEINES and Sym for symptom severity by assigning numerical values to responses and summing raw scores. The VEINES-QOL/Sym tool was developed in English through international collaboration, informed by literature review, existing measures, and expert input. It assesses four dimensions: symptoms, activity limitations, psychological effects, and changes in leg performance over the past year.14–16 In addition to the HRQoL data from this questionnaire, the researchers also collected clinical and demographic information from the hospital's electronic health record system.
Data Quality Management
The study followed a rigorous process to develop, translate, and validate its data collection tools. The VEINES-QOL/Sym questionnaire, which has proven reliability and responsiveness, was first translated into the local Amharic language and then back-translated to ensure accuracy of the translation. A team of senior clinical pharmacists and hematologists reviewed all the instruments to assess content validity and clarity. The tools were also pre-tested on 5% of patients who were not included in the final study sample. The data collectors received thorough training, and daily supervision was provided to ensure consistent, unbiased, and complete data collection, with any issues promptly resolved.
Data Analysis
Data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS) version 27. The VEINES-QOL/Sym questionnaire includes 26 items that were standardized using z-scores, followed by conversion into T-scores (mean = 50 and SD = 10), as described in previous validation studies. To ensure proper scoring given the varying number of response categories across items, three items (Q3, Q6, and Q7) were reverse coded according to the published scoring protocol, and the resulting summary scores were converted to a standardized 0-100 scale.15,16 the. For regression analysis, the continuous VEINES-QOL scores were dichotomized at the sample median to create a binary outcome variable, as applied in similar DVT studies. Binary logistic regression analysis was then used to identify predictors of lower disease-specific quality of life. Variables with a P-value less than .25 in the univariate (crude) analysis were included in a multiple logistic regression model to adjust for potential confounding effects. Statistical significance was set at P < .05. Among screened individuals, 123 met all eligibility criteria and completed the VEINES-QOL/Sym questionnaire without missing responses. For other variables, missing data were minimal and are reported in the descriptive tables.
Ethical Considerations
Ethical clearance was obtained from the Ethical Review Committee (ERB/SOP/0425/17/2025) of the School of Pharmacy, College of Health Sciences, Addis Ababa University, Ethiopia. Informed written consent was obtained from all participants before data collection. Confidentiality was maintained by anonymizing data using coded identifiers. Importantly, participants were informed of their right to withdraw from the study at any point without any consequence.
Results
Participant Recruitment and Flow Diagram
A total of 158 patients with a diagnosis of DVT were screened during the study period. Of these, 14 were excluded due to being under 18 years old, 10declined participation, and 11 withdrew consent. Thus, 123 patients met the eligibility criteria and were included in the final analysis (Figure 1). All included participants completed the VEINES QOL/Sym instrument with no missing outcome data. Missing data for covariates were minimal (<5%) and are reported in the respective tables. Figure 1 presents the flow of participants through the study in accordance with STROBE guidelines.

Flowchart showing participants' recruitment, eligibility screening, and inclusion in the final analysis.
Socio-Demographic Characteristics of the Patients
The study included 123 patients diagnosed with DVT. The participants had a mean age of 49.4 years (SD = 14.3), with ages ranging from 18 to 80 years. Notably, 67.5% of the study participants were female. Regarding marital status, the majority (74.8%) of the participants were married. Regarding educational attainment, 22% of participants had a degree or higher and 28.5% had completed secondary school. The majority (94.3%) of the participants lived with their families. Monthly income was less than 5250 Birr in 41.4% of the respondents. Furthermore, 67.5% of the participants used community-based health insurance to obtain medical care (Table 1).
Sociodemographic Characteristics of Study Participants.

Clinical Characteristics of Study Participants
The average duration since DVT diagnosis was 4.76 years (SD = 5.3), with a range from 0.25 to 22 years. Notably, patients diagnosed within the last year accounted for 35.8% of the study participants. Most of the DVT cases were provoked (73.2%) and unilateral (93.5%). The DVT was most commonly located in the distal (46.3%) or proximal (43.1%) veins. Complications were present in 40.7% of the participants, with recurrent DVT (26.0%) and pulmonary embolism (8.9%) being the most frequent. Comorbidities were found in a majority (82.9%) of the study population. The most common comorbidities were cancer (32.5%), hypertension (19.5%), and diabetes (13.0%). The details were presented in Table 2.
Clinical Characteristics of Study Participants.

*Include: Aspirin, enoxaparin, unfractionated heparin ** include: Seizure, visual impairment, benign prostatic hyperplasia, TB, anemia, allergic sinusitis, irritable bowel syndrome, interstitial pulmonary disease
Key VEINES-QOL/Sym Findings in Patients with DVT
Overall, the findings show that patients with DVT experienced a wide and heterogeneous range of leg symptoms and functional impacts across the different HRQoL domains evaluated. The detailed key findings from each item level are summarized below.
Symptom frequency over the past 4 weeks: Leg swelling was frequent, with 26.8% of patients reporting a daily occurrence and additionally 26.8% experiencing it several times a week. In contrast, symptoms like night cramps, restless legs, and throbbing were rarely reported, with over 70% of participants never experiencing them. Burning and itching sensations were present daily in 12.2% and 8.9% of patients, respectively, while more than half never experienced them. Tingling had a more even distribution across the frequency scale.
Time of day when leg problems are most intense: Nearly half of the participants (45.5%) reported that their symptoms were most intense at any time of day; however, a notable portion (14.6%) indicated never experiencing intense leg problems.
Current leg problem compared to the past year: Approximately one-third of participants (28.5%) reported that they did not have a leg problem one year ago. Among those who did, 23.6% felt their condition was “much better,” and 12.2% said it was “somewhat better.” Additionally, 22.0% noted that their leg problem had remained “about the same” compared to one year prior.
Effect of leg problem on routine daily and social activities: Regarding leg problem impact on social and recreational activities, 41.5% of participants reported being significantly limited in long-standing leisure or social activities, while 27.6% experienced mild limitations. Similarly, long-sitting activities were affected, with 22% of participants stating they were limited “a lot” and 40.7% “a little.”
Impact of leg problems on daily activities in the past 4 weeks: Daily functioning was commonly affected, with 51.2% reporting reduced time spent on activities, 41.5% feeling they could do less than they wanted to, 64.2% saying it depended on the activity type, and 62.6% having to put more effort into tasks.
Leg problem interference with social activities: In the past four weeks, 51.2% said leg problems did not interfere with social activities at all, while 18.7% experienced “quite a bit” of interference and 13.0% reported “extreme” interference.
Severity of leg pain in the past 4 weeks: Pain severity varied, with 23.6% reporting no pain, 21.1% very mild, and 27.6% mild pain. However, 13.0% had moderate pain, and 14.6% experienced severe to very severe pain.
Self-feelings due to leg problems over the past 4 weeks: The majority did not feel irritable (71.5%), like a burden (68.3%), or worried about bumping into things (69.9%). Nevertheless, some respondents expressed concern about their leg appearance, which influenced their clothing choice. The full set of item-level responses to all domains is presented as Supplementary Table S1.
HRQOL in Patients with DVT Using VEINES-QOL/Sym
The VEINES-QOL T-scores ranged from 33.4 to 59.6, with a mean of 50.0 (SD = 6.61), skewness of −0.364, and kurtosis of −0.681, indicating a slightly left-skewed and relatively flat distribution. Moderate variability was observed, with standard deviations ranging from 6.6 to 6.9 (Figure 2).

VEINS-SYM-T score.
The VEINES-SYM T-scores ranged from 26.73 to 58.73, with a mean of 50.00 (SD = 6.86), skewness of −0.736, and kurtosis of 0.112. The histogram shows a slight left skew, but overall, distribution approximates normality, indicating an acceptable spread of symptom burden across the study participants (Figure 3).

VEINS-SYM-T score.
The standardized VEINES-QOL and VEINES-SYM scores displayed distributions that were roughly normal. The distribution appears roughly symmetrical with mild negative skewness, suggesting generally normal distribution of QoL scores in the sample.
Factors Associated with HRQOL in Patients with DVT
After adjusting for potential confounders, the study findings revealed several important associations between clinical factors and the HRQoL of the DVT patients. Specifically, longer duration since DVT diagnosis was significantly associated with better VEINES-QOL scores (AOR: 1.922; 95% CI: 1.155-3.199; P = .012), suggesting that HRQoL tended to improve over time (Table 3).
Multivariable Logistics Regression for Predictors of Lower VEINES-SYM Scores.
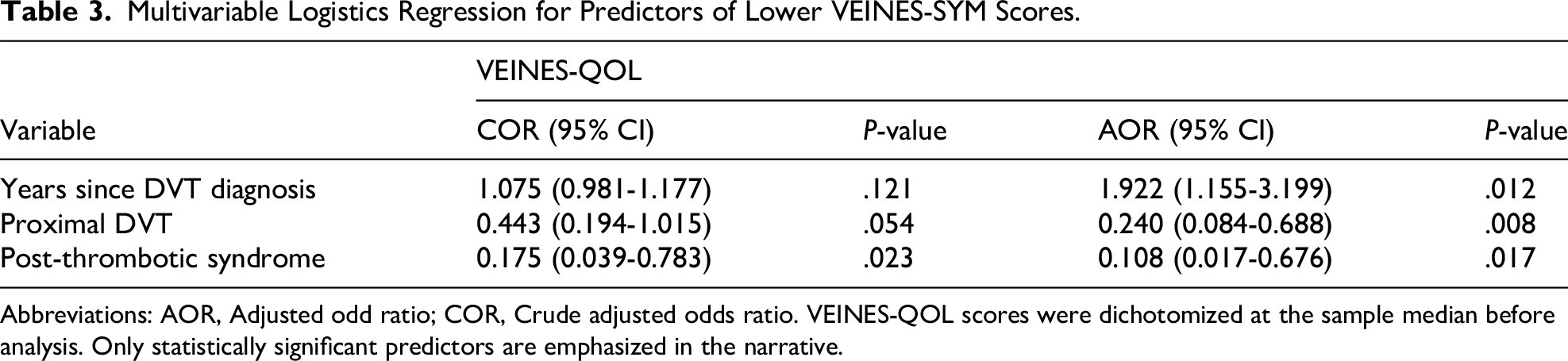
Abbreviations: AOR, Adjusted odd ratio; COR, Crude adjusted odds ratio. VEINES-QOL scores were dichotomized at the sample median before analysis. Only statistically significant predictors are emphasized in the narrative.
Furthermore, proximal DVT location was also significantly associated with poorer HRQoL compared to distal or atypical DVT locations (AOR: 0.240; 95% CI: 0.084-0.688; P = .008), indicating that patients with distal or atypical DVT had better QoL (AOR: 0.136; 95% CI: 0.028-0.666; P = .014). Additionally, the presence of PTS was also strongly associated with lower VEINES-QOL scores (AOR: 0.108; 95% CI: 0.017-0.676; P = .017). Other variables initially considered, such as recent hospitalization, diabetes mellitus, and provoked etiology, did not remain statistically significant after adjustment, suggesting that their effects may be confounded or mediated by other underlying factors.
Discussion
This cross-sectional study assessed HRQoL among patients with DVT using the validated VEINES-QOL/Sym instrument. Multivariate analysis revealed that a longer time since diagnosis was significantly associated with better QoL, suggesting a gradual recovery over time. This finding aligns with a Canadian study that reported a mean VEINES-QOL improvement of 4.9 points over two years, indicating progressive HRQoL improvement following acute DVT. 5 However, the wide variability in time since DVT diagnosis, ranging from less than a year to over 20 years, introduces substantial heterogeneity. Recent studies suggest that symptom burden and perceived QoL often improve over time, particularly within the first few years post-event. 17 This variability should be considered when interpreting the magnitude and direction of associations found in this study. Similar recovery trends were observed in the large PREFER-VTE study conducted in seven European countries, where patients experienced significant gains in QoL outcomes over 12 months, 6 and in a Norwegian population where VEINES-QOL scores improved over time, particularly in patients without PTS. 11 The improvement may reflect functional recovery, psychological adaptation, or symptom resolution facilitated by treatment interventions. Despite these gains over time, our findings indicate that HRQoL remains impaired in many patients. This is consistent with studies from other settings. For example, Norwegian patients with DVT scored significantly lower than matched controls on the EQ-5D (0.79 vs 0.90), 11 and Pakistani patients—especially those with PTS—also reported reduced HRQoL using VEINES-QOL. 12
In our cohort, patients with PTS had a mean VEINES-QOL score of 44.97 compared to 50.35 in those without PTS. This is in line with a prior report where PTS patients scored 45.8 versus 52.1 in non-PTS patients, 5 and with findings from Pakistan showing a median score of 42 (IQR: 34-47) in PTS versus 57 (IQR: 50-58) without PTS (P < .001). 12 PTS is a chronic and often under-recognized consequence of DVT that significantly impairs function and quality of life. It is characterized by symptoms such as pain, swelling, heaviness, and skin changes in the affected limb. Readers unfamiliar with PTS may refer to a recent review summarizing its clinical presentation and management. 18 Huang et al also noted that severe PTS is linked to markedly worse QoL. 1 These consistent results across diverse settings emphasize that PTS is a critical determinant of reduced well-being in DVT patients, likely due to its chronic, disabling symptoms—leg pain, swelling, heaviness, and skin changes—that interfere with mobility and daily functioning5,19
Thrombus location also emerged as an important predictor of HRQoL. Patients with proximal or combined proximal and distal DVT had significantly lower VEINES-QOL scores than those with isolated distal DVT. In our study, proximal DVT patients scored 48.29 versus 51.30 in distal DVT. Comparable results were reported in Pakistan, where proximal and iliofemoral DVT cases had a median VEINES-QOL score of 33 (IQR: 29-46) compared to 55 (IQR: 44-58) for other sites. 12 Proximal thrombosis has been linked to worse outcomes due to greater thrombus burden, higher risk of reflux, venous hypertension, and complications such as PTS. 20 These pathophysiological consequences may explain the greater symptom burden—pain, swelling, skin changes—and subsequent QoL decline, as also observed in Chinese patients with extensive thrombi. 1
Some previous studies have identified demographic factors, such as age and sex, as HRQoL predictors. For instance, Huang et al reported lower QoL in older patients, 1 and Norwegian researchers found lower scores in women compared to men (45.2 vs 49.3, P = .01), though this difference disappeared after adjustment. 11 In the present study, factors such as sex, marital status, education, employment status, and provoked etiology were not significantly associated with HRQoL after adjustment. This finding differed from some prior research, which may be due to differences in sample size, population characteristics, or the mediating influence of PTS, which might attenuate associations with other factors.
Strengths and Limitations of the Study
This study is the first in Ethiopia to assess HRQoL in DVT patients using the validated VEINES-QOL/Sym instrument. This provided locally relevant evidence in a setting where such data are scarce. The use of multivariate analysis allowed the identification of independent predictors, offering valuable insights that can inform targeted patient management. However, the study had several limitations that should be noted. The cross-sectional design precludes causal inference, and the single-center setting may limit the generalizability of findings. The relatively small sample size could reduce statistical power and precision of the analyses. Recall bias is possible in self-reported measures used, and the lack of a control group prevents direct comparison with the general population. Another important limitation is the potential for survivorship or selection bias. Given the extended follow-up period for many participants, those with more severe illness, terminal complications, or who died earlier may not have been captured. As a result, this study may underestimate the long-term burden of DVT by primarily representing patients who were healthier and able to return for follow-up.
Conclusions
The findings indicate that HRQoL is moderately to significantly reduced in DVT patients attending the hematology clinic of TASH, particularly those with proximal or combined DVT and PTS. Interestingly, the study did not find independent associations between certain clinical variables, such as recurrent DVT and comorbidities like diabetes, and reduced HRQoL. This suggests that the effects of these factors may be mediated through complications like PTS. Additionally, the researchers observed a positive association between time since diagnosis and improved QoL, highlighting the importance of long-term care strategies. Based on these results, the authors recommend incorporating regular HRQoL evaluations using the VEINES-QOL/Sym tool into the routine follow-up care for patients with DVT, prioritizing the prevention and treatment of PTS, and improving long-term monitoring, treatment compliance, and patient education to enhance DVT management. The authors also suggest informing national guidelines for DVT care in Ethiopia by conducting additional research on broader clinical and psychosocial factors.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251408062 - Supplemental material for Health-Related Quality of Life and Associated Factors Among Patients with Deep Vein Thrombosis at a Tertiary University Teaching Hospital in Ethiopia
Supplemental material, sj-docx-1-cat-10.1177_10760296251408062 for Health-Related Quality of Life and Associated Factors Among Patients with Deep Vein Thrombosis at a Tertiary University Teaching Hospital in Ethiopia by Yeabsira Endale, Melaku Tileku and Amha Gebremedhin, Tamrat Assefa Tadesse in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors thank all study participants for their time and willingness to participate, the nursing staff at the hematology clinic of the hospital for facilitating data collection, and the data collectors for their valuable contributions.
Authors’ Contributions
YE and TAT contributed to the study conception, design, data collection, and data analysis and preparation of first manuscript draft. MT and AG contributed to methodology development, critical manuscript review, and validation of findings. TAT and AG led conceptualization, drafting, and final revision of the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.