
Abstract
Background
Previous studies have demonstrated the potential benefits of the routine use of batroxobin in treating cerebral venous thrombosis (CVT). However, there is still a need to discuss how to achieve maximum clinical effectiveness when using batroxobin for CVT correction. Therefore, this study aimed to analyze the efficacy and safety of individualized batroxobin strategies in treating CVT.
Methods
This observational clinical study analyzed data from 41 patients with acute CVT. The patients were divided into two groups based on their batroxobin treatment strategies: the individualized group (batroxobin used more than 5 times, n = 16) and the standard group (batroxobin used 3 times, n = 25). The degree of recanalization and attenuation of segmental stenosis were analyzed using MRBTI. The incidence of bleeding events was also analyzed.
Results
The individualized group had significantly higher odds of achieving recanalization (14/16) [adjusted OR (95%CI) of 2.96 (1.30-6.71)] and greater attenuation of segmental stenosis [adjusted OR (95%CI) of 2.16 (1.04-4.49)] compared to the standard group (17/25). There was no statistically significant difference in the incidence of bleeding events between the individualized and standard groups (P > 0.05).
Conclusions
This observational study suggests that an individualized batroxobin strategy may be more effective than the standard approach in promoting cerebral venous thrombosis (CVT) recanalization and reducing CVT-induced stenosis. Further clinical trials are needed to confirm the potential benefits of this individualized therapeutic strategy.
Introduction
Cerebral venous thrombosis (CVT) induced ischemic or hemorrhagic brain lesions are a significant subtype of stroke, predominantly affecting young adults and middle-aged individuals, and diagnosis and treatment of CVT are challenging.1–4 In addition to being universally endorsed as the primary standard treatment for CVT, standard anticoagulation therapy is further enhanced by the combination with intravenous batroxobin which has been confirmed as a more productive and safe therapy in promoting acute CVT rapid recanalization, reducing CVT-induced cerebral ischemic and hemorrhagic brain lesions, and mitigating secondary cerebral venous stenosis associated with CVT.5–8 Batroxobin, derived from Bothrops atrox moojeni venom, functions as a thrombin-like serine protease. 9 Typically used for the treatment of cerebral arterial thrombosis and prevention of restenosis post-arterial stenting, batroxobin has demonstrated its efficacy as a defibrinogenating agent.10–13 In our previous studies on the use of batroxobin combined with anticoagulation to correct acute CVT, we followed the routine strategy for batroxobin administration in arterial disease treatment. This involved an initial dosage of 10 BU, followed by two times of 5 BU every other day.10,11 Timely recanalization of the involved cerebral venous sinuses following thrombosis has been confirmed as an effective way to inhibit or decrease CVT-related brain lesions and achieve favorable functional outcomes.14–16 Poor recanalization increases the risk of recurrent CVT, CVT-related stenosis, and chronic intracranial hypertension. While improving prognosis remains the primary objective in treating CVT, increasing the degree of recanalization is equally important in reducing the risk of subsequent adverse events. The result of the peripheral blood test also indicated soluble thrombus after three administrations of batroxobin. Additionally, research on batroxobin for arterial disease treatment has shown positive clinical outcomes with a secure safety profile for multiple doses.11,13,17 Therefore, we hypothesized that increasing the frequency of batroxobin administration might obtain better outcomes on CVT recanalization than the routine strategy during the acute stage. Herein, we aimed to identify this hypothesis in an observational clinical study.
Methods and Materials
Subjects Collection
In this observational study, we analyzed patients with imaging-confirmed CVT admitted to Xuanwu Hospital of Capital Medical University from July 2011 through July 2023. The diagnostic criteria of CVT were primarily confirmed through magnetic resonance black-blood thrombus imaging (MRBTI), magnetic resonance venography (MRV), or computed tomographic venography (CTV), as outlined in previous literature. 6 The inclusion and exclusion criteria for this study were as follows:
Inclusion criteria:
Confirmed diagnosis of CVT. Age ranging from 18 to 80 years. First-time confirmation of CVT diagnosis at our institution. Initiation of anticoagulation treatment immediately upon CVT diagnosis. Batroxobin intravenous infusion performed during standard anticoagulation.
Exclusion criteria:
Patients who underwent endovascular treatment or thrombolysis (such as recombinant tissue plasminogen activator and urokinase) before admission or during hospitalization; Subjects without complete data, including demographic data, treatment methods and imaging data; Baseline plasma fibrinogen < 1 g/L.
Intervention and Grouping
All patients underwent standard anticoagulation immediately after confirming their CVT diagnosis. Meanwhile, they underwent intravenous infusion of batroxobin [Batroxobin injection (produced by Beijing Tuobixi Pharmaceutical Co., Ltd, the approval number was H20031074)] after signing the informed consent at admission.
Standard group: Patients underwent batroxobin three times. The initial dosage was 10 BU, followed by 5 BU every other day for two additional times.
Individualized group: Patients underwent batroxobin intravenous infusion more than 3 times. The initial dosage of batroxobin was determined based on the patient's baseline fibrinogen value: If the baseline value of fibrinogen before batroxobin use ranged from 1 to 3 g/L, the first dosage administered was 5 BU; if it exceeded 3 g/L, the initial dosage was set at 10 BU in order to maintain a lower cut-off value of fibrinogen above 1.0 g/L during batroxobin administration. The total number of episodes of batroxobin use exceeded 5 times. Since 2020, our research center has been conducting experiments with individualized medication regimens using batroxobin under strict monitoring of laboratory indicators. The patient had not been screened or met any specific criteria.
Outcomes
The primary outcomes encompassed the degree of recanalization assessed through TOF MRV and the degree of segment-stenosis attenuation evaluated using MRBTI. The recanalization degree was graded into four classes: Class 0: complete non-recanalization; Class 1: partial recanalization of one or more occluded sinuses with improved collateral flow; Class 2: complete recanalization of one sinus but persistent occlusion of the other sinuses; and Class 3: complete recanalization of all occluded sinuses. Class 2 and 3 were identified as recanalization, while Class 0 and 1 were defined as non-recanalization. The stenosis attenuation was ranked into four classes according to the variation of stenosis extent from baseline to follow-up on MRBTI maps. Class 0: exacerbation (thrombus increased); Class 1: no change or mild recovery (thrombus reduced <30%); Class 2: moderate recovery (thrombus reduced by 30%-60%); and Class 3: obvious or complete recovery (thrombus reduced by 60%-100%). Of the four classes, class 2 and class 3 were identified as stenosis attenuation.
The secondary outcomes comprised the ratio of patients with recanalization measured by TOF MRV, patients with stenosis attenuation, and the ratio of segments with stenosis amelioration (thrombus reduced > 30%). The assessment focused on the most severe section of multi-stenosis within one segment. Two experienced independent readers conducted the imaging evaluation.
All images were retrospectively reviewed in a randomized, blinded fashion by two independent radiologists who had respective seven years (D.Z.) and ten years (R.M.) of experience in diagnosing CVT. They were blinded to general information, clinical data, and conventional images. In addition, source images and multiplanar reconstruction images were used for more precise thrombus evaluation. In case of disagreement between the two readers, a third radiologist with 11 years of experience (XM.J.) resolved it. The safety endpoint was determined based on the ratio of hemorrhage occurrence, defined as the number of patients with new hemorrhage and hemorrhage expansion on brain CT/MRI images relative to the total number of patients. The ratio of hemorrhage aggravation was defined as the number of patients with hemorrhage expansion on brain CT/MRI images versus the sum of patients without hemorrhage expansion and those with hemorrhage expansion. Hemorrhage expansion in this study was defined as an increase of ≥3 mL or >33% of primary hematoma volume on the follow-up CT image, aligning closely with criteria used in previous studies. 18
Statistical Analysis
Baseline demographic and clinical characteristics were summarized using standard descriptive statistics. Ordinal logistic regression was employed to analyze the entire improvement spectrum, expressing the effect size as a crude common odds ratio (OR). The Fisher’s exact test and the Mann-Whitney U test were used to investigate differences between proportions and medians. Multivariate analyses, including logistic regression and linear regression models, were conducted to control for confounding effects. Independent variables were selected based on previous reports on risk factors associated with low recanalization rates. Due to the evident correlation between different groups and the number of episodes of batroxobin use, separate regression models were constructed for other groups and the number of episodes of batroxobin use in order to assess their independent effects on outcomes. The results were presented as OR with corresponding 95% confidence intervals (95% CI). Statistical significance was considered at a two-sided P-value < 0.05. All analyses were performed using IBM SPSS Statistics, version 24 (IBM Corp).
Results
Baseline Characteristics
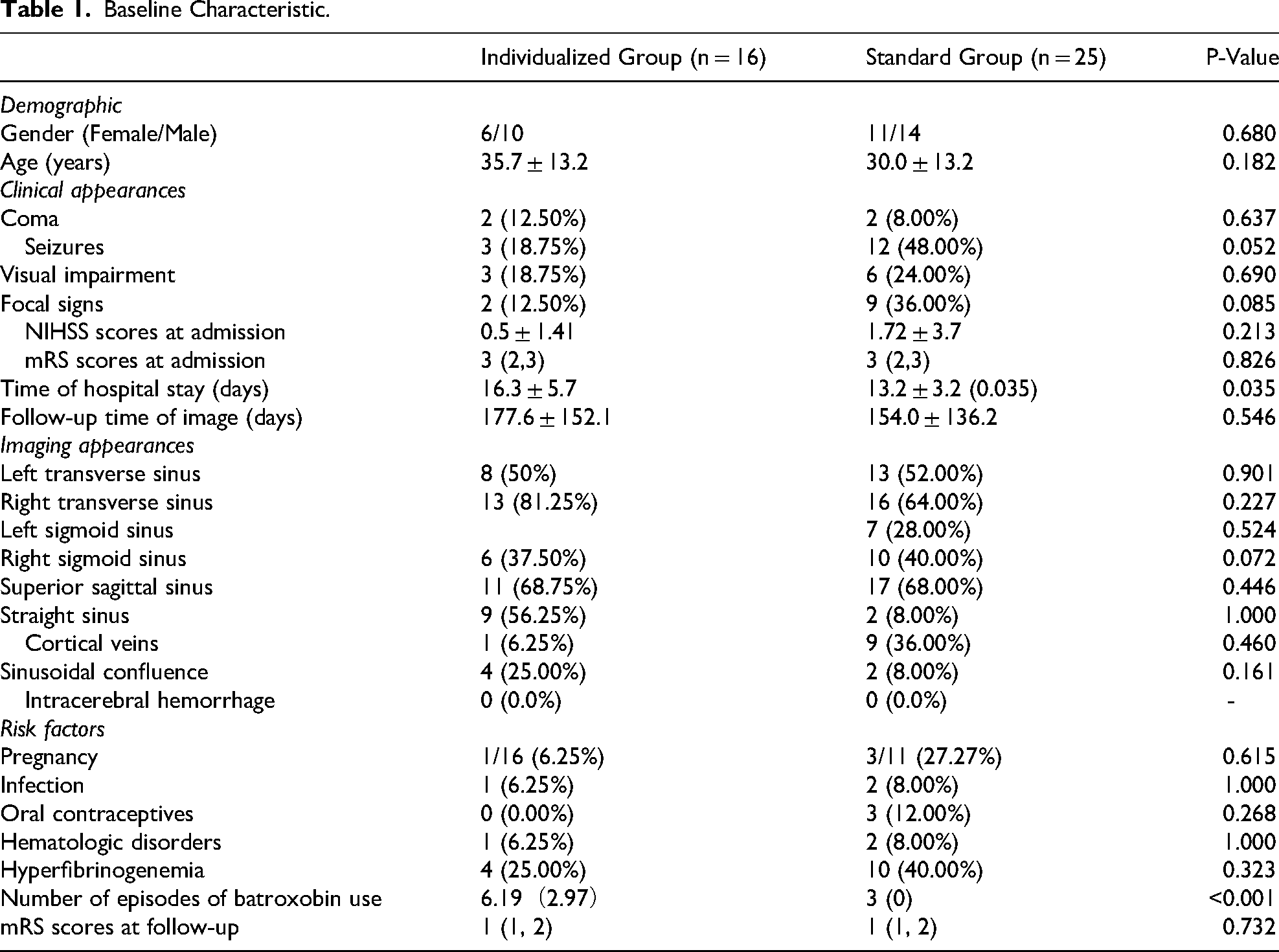
Forty-one patients diagnosed with acute CVT and underwent batroxobin in combination with anticoagulation were screened for eligibility. Among them, 16 patients underwent the individualized batroxobin strategy, while 25 underwent the standard batroxobin strategy. Details are displayed in Table 1. A total of 132 segments exhibited thrombus, with 56 segments in the individualized group and 76 segments in the standard treatment group. The mean (SD) number of episodes of batroxobin use in the two groups was 3 (0) and 6.19 (2.97), respectively. Baseline data, including demographics, risk factors, imaging appearance, and clinical manifestations, were comparable among all patient cohorts without any significant differences.
Baseline Characteristic.
Primary Outcomes
According to the recanalization criteria outlined using TOF MRV, the recanalization degree at follow-up was significantly higher in the individual group compared to the standard group, irrespective of confounder adjustment [unadjusted OR (95%CI) of 2.320 (1.183-4.545), P = 0.014; adjusted OR (95%CI) of 2.959 (1.305-6.7111), P = 0.009]. Evaluation by MRBTI follow-up revealed a more pronounced relief of segment-stenosis in the individualized group compared to the standard group [unadjusted OR (95%CI) of 2.330 (1.192-4.554), P = 0.013; adjusted OR (95%CI) of 2.164 (1.043-4.486), P = 0.038] (Figure 1).

The raw distribution of the follow-up recanalization (individualized group vs standard group); the segment-stenosis extent attenuation (individualized group vs standard group).
Regression analysis demonstrated that patients with a higher number of episodes of batroxobin use exhibited a better recanalization degree [unadjusted OR (95% CI) 1.466 (1.403-1.537), P = 0.017; adjusted OR (95%CI) was of 1.327 (1.047-1.682), P = 0.019]. Results from regression analysis without adjustment for confounding factors indicated that an increased number of episodes of batroxobin use led to greater attenuation in segment-stenosis [unadjusted OR (95%CI) of 1.226 (1.016-1.578), P = 0.035]. Still, no significant difference was observed after adjustment. [adjusted OR (95%CI) of 1.241 (0.999-1.542), P = 0.51] (Figure 1).
Secondary Outcomes
Of the 41 subjects enrolled, 87.5% of cases (14/16) in the individualized group exhibited recanalization on TOF MRV, while only 68.0% (17/25) of the standard group showed similar findings. Additionally, in the individual group, 93.8% (15/16) of cases demonstrated stenosis improvement ≥30% on follow-up MRBTI maps, while only 76% (19/25) in the standard group showed stenosis improvement. Similarly, among the 131 involved stenotic segments, the ratio of segments with stenosis extent improvement was 83.9% (47/56) in the individualized group and only 61.8% (47/76) in the standard group. The only significant difference among the three outcomes mentioned above was the ratio of segments with stenosis extent improvement between the two groups [unadjusted OR (95% CI) of 3.526 (1.320–9.419), P = 0.012; adjusted OR (95% CI) of 4.267 (1.297-14.038), P = 0.017]. Regression analysis showed that the rate of segments with stenosis relieved in the individualized group was higher than that in the standard group. The results are presented in Table 2.
Results of Secondary Outcomes.
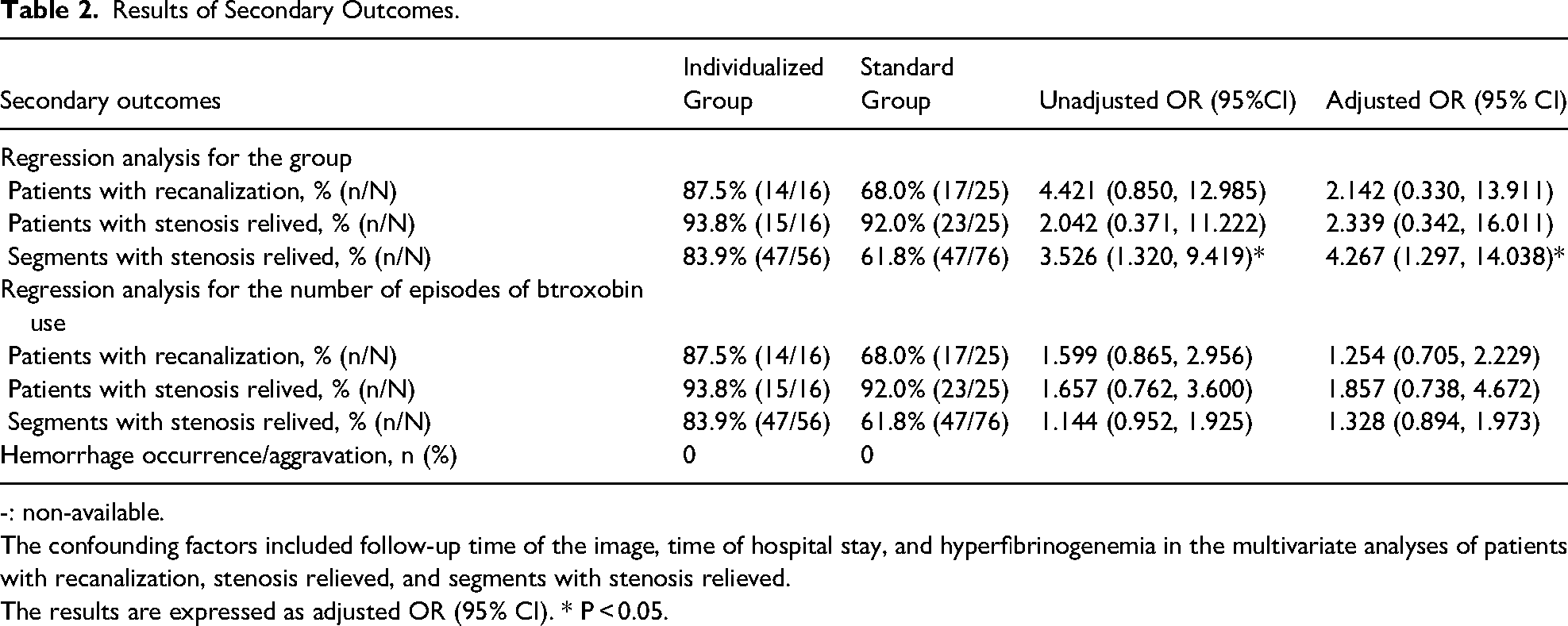
-: non-available.
The confounding factors included follow-up time of the image, time of hospital stay, and hyperfibrinogenemia in the multivariate analyses of patients with recanalization, stenosis relieved, and segments with stenosis relieved.
The results are expressed as adjusted OR (95% CI). * P < 0.05.
Safety Outcomes
No adverse events (eg, anaphylaxis, microbleeds, cerebral hemorrhage) were observed in any patient during hospitalization or during outpatient follow-up.
Discussion
As previously mentioned, this study was designed to investigate whether individual batroxobin use in combination with anticoagulation treatment can enhance the recanalization of CVT compared to standard batroxobin use combined with anticoagulation. Our findings indicated that CVT patients who received the individual batroxobin strategy achieved more significant benefits in both rapid recanalization and attenuation of CVT-related segment-stenosis of venous sinuses when compared to those receiving standard batroxobin use. Figure 2 shows a CVT patient treated with anticoagulation combined with individualized batroxobin, and follow-up imaging shows a very satisfactory recanalization result.

Case presentation on the efficacy of individualized batroxobin strategy in treating cerebral venous thrombosis. A 35-year-old female patient was diagnosed with extensive cerebral venous sinus thrombosis. Enhanced magnetic resonance black-blood thrombus imaging (MRBTI) (A) demonstrated significant thrombosis in the superior sagittal sinus and straight sinus (indicated by red arrows). After admission, anticoagulation therapy combined with batroxobin was administered. A follow-up examination one week later revealed a reduction in the thrombosis of the superior sagittal sinus and a significant decrease in the straight sinus thrombosis (B, indicated by red arrows), as shown by enhanced mrbti. During the hospital stay, the patient underwent a total of 5 Batroxobin treatments (10-5-5-5-5-BU). One month after treatment, a follow-up enhanced MRBTI showed that the thrombosis in the superior sagittal and straight sinus had essentially resolved (C, indicated by red arrows). Meanwhile, monitor the value of D-dimer at 12 h after every time of batroxobin infusion dynamically. Withdrawal criteria were elevated D-dimer to return to a nearly normal level.
Batroxobin is a thrombin-like serine protease extracted from Bothrops atrox moojeni venom, serving as a defibrinogenating agent recently employed in the treatment of CVT.7,8,19 In clinical settings, it is well-known that continuous elevation of D-dimer levels indicates the presence of soluble thrombi to some extent, and plasma D-dimer levels remarkably increase during cross-linked fibrinolysis induced by Batroxobin.20–22 Figure 3 shows the diagram of the thrombolytic mechanism of batroxobin. We can intuitively know how various factors change after the use of batroxobin. When monitored serum fibrinogen and D-dimer dynamically during batroxobin use, we found the presence of soluble thrombus even after three times of batroxobin use. Therefore, we increased the number of episodes individually according to the results of plasma D-dimer after each time of batroxobin use. Our results confirmed that as the number of episodes of batroxobin use increased, the thrombus load in patients with CVT gradually diminished, leading to a significant enhancement in recanalization and attenuation of thrombus-induced cerebral venous sinus stenosis. The sensitivity analysis further validated these findings. However, in a clinical setting at present, most patients might not receive sufficient duration or dosage adjustments with batroxobin to achieve the therapeutic objective - a downward trend in serum D-dimer values. Due to a lack of guidelines regarding batroxobin usage for CVT management at present time, its usage still follows protocol: a total of 3 times (10BU, 5BU, 5BU) on arterial disease. This limitation may cover the contribution of batroxobin on CVT, as thrombosis in the venous system has been confirmed as a continuous process, which may need repeated thrombolysis and long-term anticoagulation. The results of this study revealed that the strategies of batroxobin for treating CVT should differ from those used for arterial disease; the high frequency of batroxobin administration may provide greater benefit in achieving rapid recanalization.

Diagram of the thrombolytic mechanism of batroxobin.
Numerous factors influence the functional outcomes of patients with CVT, with the speed and degree of recanalization playing a pivotal role. 23 Swift and optimal recanalization of CVT poses a significant challenge, particularly in cases of severe CVT. Endovascular interventions, such as intravascular thrombolysis or thrombectomy, offer effective means to recanalize affected sinuses in CVT patients rapidly. However, these interventions carry an elevated risk of adverse events, including cerebral hemorrhage, compared to anticoagulation therapy alone, which may counterbalance the potential benefits of rapid recanalization.24,25 Contrastingly, batroxobin demonstrates effectiveness and safety simultaneously. Batroxobin exerts its antithrombotic effect through two mechanisms. Firstly, it exhibits a tenfold higher affinity for binding fibrinogen compared to thrombin, leading to a reduction in circulating fibrinogen levels, inhibition of fibrin formation, and prevention of thrombus elongation. 20 Additionally, batroxobin stimulates the production of tissue plasminogen activator (tPA) while attenuating the activation of tissue plasminogen inhibitor (PAI).21,22,26 Consequently, the combined use of batroxobin and anticoagulant drugs enhances the antithrombotic pathway of thrombolysis based on anticoagulation, thereby increasing the likelihood of cerebral venous sinus recanalization. Moreover, the indirect thrombolytic effect of batroxobin reduces the risk of bleeding compared to direct intravascular thrombolytic interventions. Combined with the unique features of CVT formation, an individualized treatment strategy utilizing batroxobin may provide a safe and practical benefit in CVT correction.
Conclusion
This observational study suggests that an individualized batroxobin strategy may be more effective than the standard approach in promoting CVT recanalization and reducing CVT-induced stenosis. Further clinical trials are needed to confirm the potential benefits of this individualized therapeutic strategy.
Limitation
There were some limitations in this study. Firstly, the small sample size undermines the study's reliability and calls for future well-designed large-scale trials. At the same time, this study was a real-world study, which may have introduced other biases. Future studies should have rigorous designs such as prospective controlled experiments Secondly, the criteria for the number of episodes of batroxobin use in each patient need to be further defined. Thirdly, this study was conducted as a real-world study only; strong evidence from a multi-center randomized controlled study is essential and currently ongoing. Moreover, since most enrolled patients underwent MRBTI only twice in this study, more sequential MRBTI imaging should be acquired to evaluate more precisely how batroxobin could accelerate the recanalization in CVT patients. Although there was no difference in follow-up time between the two groups and multivariate analysis adjusted for this confounding factor, bias still existed in this study, and the conclusions need further determination.
Footnotes
Abbreviations
Acknowledgments
We want to thank all patients and doctors who participated in this study for their cooperation.
Ethics Approval and Patient Consent Statement
This study was approved by the Institutional Ethics Committee of Xuanwu Hospital, Capital Medical University, and was conducted in accordance with the guidelines of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to any study procedures.
Consent for Publication
Consent for publication was obtained from all participants prior to any study procedures.
Author Contribution
DL, XH, and XZ contributed equally to this work. DL wrote the first draft of the manuscript; ZW, RW, XZ, MW YG, and XH performed the material preparation, data collection, and statistical analysis; DZ, RM, and XJ contributed to imaging assessments; RM wrote sections of the manuscript and contributed to manuscript revision; RM contributed conception and design of the study; RM takes full responsibility for the data, the analyses and interpretation, and the conduct of the research. All authors read and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China [grant numbers 82171297 and 82101390].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability and Materials
The datasets used and/or analyzed during the current study are available from the corresponding authors upon reasonable request.