
Abstract
Background
Acute pulmonary embolism (APE) as a common cardiopulmonary disease is associated with a high mortality rate. Therefore, its rapid and accurate diagnosis remains a medical challenge. The present study aimed at providing a new electrocardiogram (ECG) model for easy and rapid estimation of the probability of APE through ECG findings.
Method
This retrospective study was conducted on 319 patients suspected of APE that were admitted to Shahid Chamran and Al-Zahra Hospitals in Isfahan during 2017–2023. Patients’ demographic, clinical, and 16 ECG findings were extracted from their medical records. Other standard criteria such as Wells, Geneva, and Daniel were also calculated.
Results
In this study, an ECG-predictive model, called TRIAGE score, was proposed comprising three ECG findings including
Conclusion
The TRIAGE score, which integrates ECG findings (tachycardia, RBBB, and inverted T-waves in leads V1–V4) with patient characteristics (age, gender, edema), shows promising specificity in diagnosing APE. At a cut-off score of ≥4, it demonstrated statistically significant diagnostic performance compared to existing criteria such as Wells, Geneva, Daniel, and d-dimer levels. These findings suggest the TRIAGE score may serve as a useful adjunct in the early assessment of APE, particularly in settings where advanced imaging is not readily available.
Introduction
Acute pulmonary embolism (APE) is a common cardiovascular disease associated with high mortality. Rapid diagnosis of this disease is one of the main concerns of physicians, especially emergency medicine specialists as more than 50% of these patients’ deaths occur before the time of diagnosis. 1
Considering the rapid use, availability, cost-effectiveness, and non-invasiveness features, electrocardiography (ECG) is the initial diagnostic action performed in the emergency department (ED) for patients suspected of APE. 2 ECG seems to be a suitable diagnostic tool for cases suspected of APE due to the strong association of ECG changes with hemodynamic collapse and right ventricular dysfunction.3–6 According to the European Society of Cardiology (ECE) guidelines, 12-lead ECG can be used to estimate the probability of APE; however, it lacks standardization. 7
Other standard criteria, measurement of various markers, and various imaging methods such as Wells criteria, Geneva criteria, D-dimer, lower limb ultrasound, and echocardiography are also available for diagnosing APE, do not include the use of ECG, depend on the patient's current clinical condition and previous history, and in some cases, can cause difficulties or errors for physicians in diagnosing APE.8–11
In response, Daniel et al (2001) reported an ECG-based scoring system that could predict the severity of pulmonary arterial hypertension (PAH) and the degree of perfusion defect on ventilation-perfusion lung scanning. 11 However, few studies have evaluated the use of ECG abnormalities for assessing clot burden, hemodynamic status, right ventricular function, survival rate, and management of acPTE patients.
In this regard, some studies aimed at achieving criteria based on 12-lead ECG findings to estimate the probability of APE and introduced new criteria and compared their diagnostic value with that of the standard criteria such as Wells, Geneva, and Daniel.12–16
While previous studies conducted in various countries focused on individual aspects of ECG findings, the primary objective of this study was to develop a new, localized scoring system that integrates multiple ECG findings to facilitate the rapid assessment of APE probability.
Materials and Methods
Study Design and Setting
This retrospective study was carried out at Al-Zahra and Shahid Chamran hospitals in Isfahan, Iran, over the period from 2017 to 2023. The research was formally registered with the Ethics Committee of Isfahan University of Medical Sciences.
Study Participants
From an initial dataset of 389 patients, the study ultimately included 319 individuals suspected of acute pulmonary embolism (APE). The sample size was calculated based on a 95% confidence level, 80% statistical power, and previously reported ECG diagnostic sensitivity of 79.08%, 15 considering an APE incidence rate of 0.5% and a margin of error of 0.09.
Inclusion was based on the documentation of clinical symptoms indicative of APE—such as acute shortness of breath, chest pain, hemoptysis, syncope, or persistent cough—as recorded in medical records. Patients were excluded if they had prior cardiac dysfunction, left bundle branch block (LBBB), severe underlying pulmonary conditions such as emphysema or pneumonitis, chronic thromboembolic pulmonary hypertension, pacemaker implantation, history of antiarrhythmic drug use, electrolyte disturbances, or metabolic acidosis. Additionally, 70 patients (18%) were excluded due to pre-existing cardiac conditions, severe pulmonary disease, incomplete ECG data, or confounding comorbidities. Cases with missing records or absent ECG strips were replaced to maintain sample integrity. The final cohort comprised 319 participants who met all inclusion criteria.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki (World Medical Association [WMA], 2013) and was approved by the Research Ethics Committee of Isfahan University of Medical Sciences (Approval No: IR.MUI.MED.REC.1403.145). The ethics committee approved the use of anonymized data without requiring patient consent, as the data did not permit individual identification. Additionally, legislation on data safety and confidentiality was strictly followed.
Data Collection
Demographic and clinical information, including age, gender, smoking status, drug use, and past medical history (eg, diabetes, hypertension, recent surgery/fracture, previous PE/DVT, dyspnea, chest pain, edema, and D-dimer levels), was recorded at hospital admission. Diagnostic criteria for APE, such as Wells, Geneva, and Daniel scores,9–11 were calculated and categorized as follows:
Wells: < 4 (low probability), ≥ 4 (high probability). Geneva: < 10 (low probability), ≥ 10 (high probability). Daniel: < 10 (low probability), ≥ 10 (high probability).
ECG findings were also reviewed and recorded, encompassing 16 parameters: sinus tachycardia, complete/incomplete right bundle branch block (RBBB), inverted T-waves (V1-V4, inferior leads), right axis deviation, dominant R wave in V1, right atrial enlargement, clockwise rotation, atrial tachycardia, T-wave inversions of varying depths in V1-V3, S wave in lead I, Q wave in lead III, T-wave inversion in lead III, and S1Q3T3 pattern.
Data Analysis
Data were processed using SPSS (Ver. 26) and presented as mean ± standard deviation (SD) or frequencies (%). Univariate logistic regression identified associations between APE and factors such as demographic, clinical, and ECG findings. Multivariate logistic regression with a forward conditional approach was used to determine predictors for APE. ROC analysis assessed the diagnostic performance of the standard criteria (Wells, Geneva, Daniel, and D-dimer with a cut-off of 500 ng/ml). Diagnostic metrics such as sensitivity, specificity, positive/negative likelihood ratios, and the area under the curve (AUC) were reported. Statistical significance was set at p < 0.05.
Results
Based on CTPA reports of 319 patients studied, 163 (51.1%) and 156 (48.9%) were diagnosed without and with APE, respectively.
In the APE group with a mean age of 56.02 ± 16.82 years, 59 (37.8%) and 97 (62.2%) cases were female and male, respectively. In the non-APE group with a mean age of 49.14 ± 17.93 years, 110 (67.5%) and 53 (32.5%) cases were female and male, respectively. Statistically, the incidence of APE was more common among men and at older ages (P value < 0.001).
Edema and history of previous DVT or PE had a direct and significant association with the incidence of APE (P value < 0.05). However, smoking, drug use, symptoms such as dyspnea, chest pain, and history of HTN, DM, and surgery or fracture were not significantly associated with the incidence of APE (P value >0.05). ECG findings revealed that sinus tachycardia, complete/incomplete RBBB, inverted TW in the right precordial leads (V1-V4), atrial tachycardia, and TW inversion in lead V2 (1-2 mm vs 0) were independently, directly, and significantly associated with APE (P value < 0.05). However, they were not significantly associated with other ECG findings (P value > 0.05). Moreover, the Wells score (OR(95% CI): 1.732 (1.084–2.767)), the modified Geneva score (OR(95% CI): 2.771 (1.731–4.435)), Daniel score (OR(95% CI): 2.892 (1.381–6.058)), and D-dimer level with a cut-off point of 500 ng/ml (OR(95% CI): 4.745 (1.896–11.875)) had a direct and significant association with the incidence of APE (P value < 0.01) (Table 1).
Results of Univariate Logistic Regression Addressing the Association of Each Factor with APE.
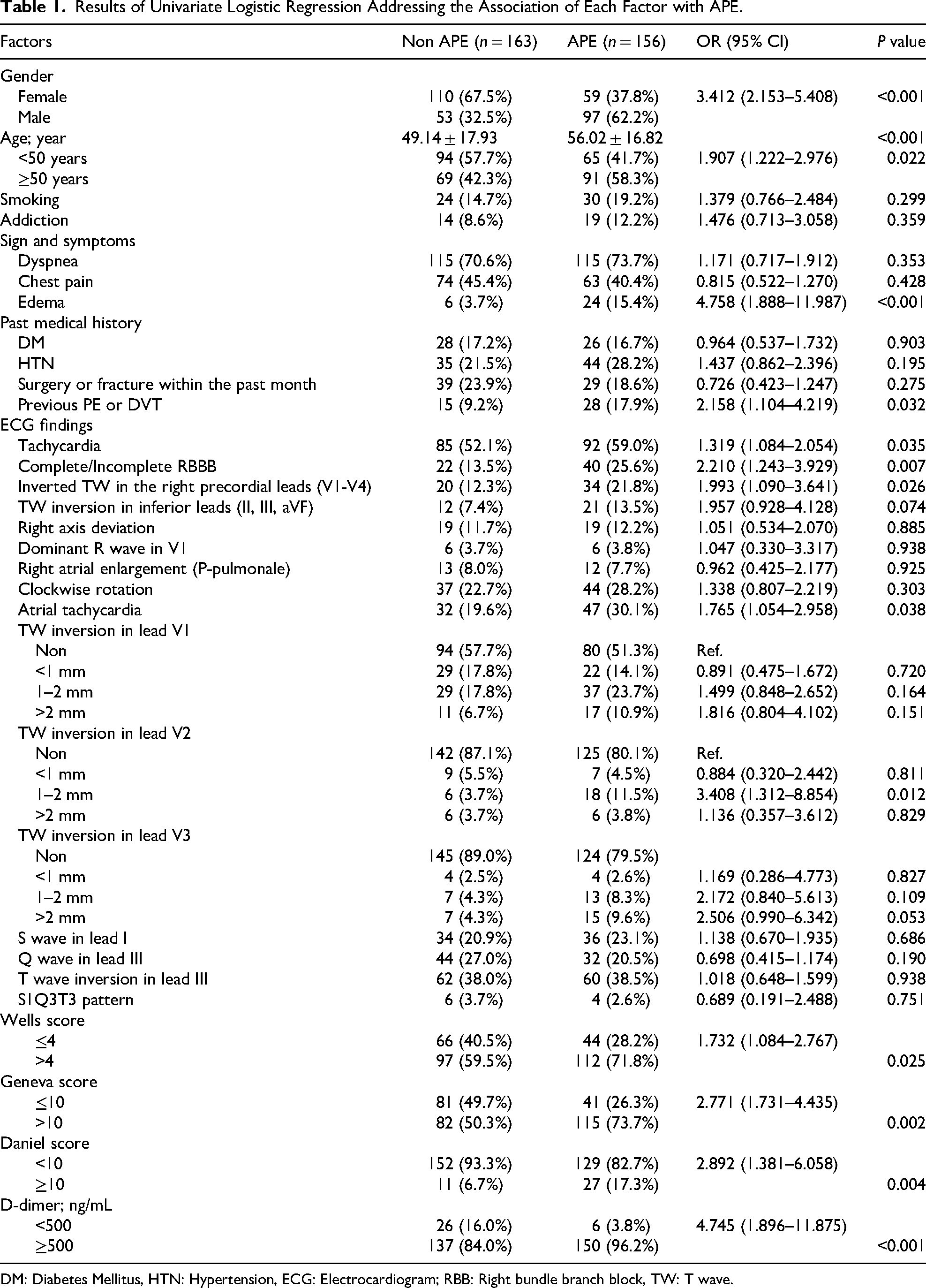
DM: Diabetes Mellitus, HTN: Hypertension, ECG: Electrocardiogram; RBB: Right bundle branch block, TW: T wave.
Development of the TRIAGE Scoring System:Through a multivariate logistic regression analysis, this study identified six significant predictive factors associated with APE, comprising three ECG findings—Tachycardia, RBBB (complete/incomplete), and Inverted T-waves in the right precordial leads (V1-V4)—and three baseline patient characteristics—Age, Gender, and Edema. Each factor demonstrated a direct and statistically significant relationship with APE, with odds ratios ranging from 1.873 to 5.504 (P value < 0.05). Combining these predictors resulted in the development of the TRIAGE score, a novel diagnostic tool that integrates both clinical and ECG parameters.
The ROC analysis confirmed the diagnostic efficacy of the TRIAGE score, particularly at cut-off points of ≥3 and ≥4, with sensitivity and specificity values that outperformed existing criteria, including the Wells, Geneva, and Daniel scores, as well as D-dimer levels. The TRIAGE score's superior diagnostic accuracy and high specificity underscore its potential as a reliable and practical alternative for rapidly assessing the likelihood of APE, especially in settings with limited access to advanced imaging modalities.
Table 2 introduces a multivariate regression-based ECG predictor model called TRIAGE score, which contains three ECG findings and three baseline characteristics. In detail, three ECG findings including tachycardia, RBBB (complete/incomplete), and inverted TW in the right precordial leads (V1-V4) with OR of 1.989, 1.873, and 2.376, respectively as well as patients’ baseline characteristics comprising age, gender, and edema with OR of 2.144, 4.070, and 5.504, respectively, had a direct and significant association with the incidence of APE (P value < 0.05) (Table 2).
Results of Multivariate Logistic Regression Evaluating the Predictive Factors of APE.

TRIAGE is a scoring system obtained from multivariate logistic regression in predicting APE.
*: Complete/Incomplete RBBB, RBB: right bundle branch block; TW: T wave.
To further evaluate the diagnostic contribution of individual predictors, we calculated their respective AUC values. Tachycardia, RBBB, inverted T-waves, age, and edema each demonstrated modest discriminatory ability when assessed independently. However, when combined, their predictive performance improved substantially, yielding a notably higher composite AUC. These values are presented in Appendix 1, providing a more granular view of the model's components and reinforcing the additive value of integrating clinical and electrocardiographic features.
The evaluation of the diagnostic value of the TRIAGE scoring system, both with and without baseline characteristics, showed significant effectiveness in predicting APE. At a cut-off point of ≥3, the sensitivity and specificity were 80.77% and 50.31%, respectively, while a cut-off point of ≥4 yielded sensitivity and specificity of 44.23% and 86.50%, respectively (P value < 0.001). Comparatively, the Wells score demonstrated a sensitivity of 71.79% and specificity of 40.49%, the Geneva score had sensitivity and specificity of 73.72% and 49.69%, respectively, and D-dimer at a threshold of 500 ng/ml showed high sensitivity of 96.15% but low specificity of 15.95% (P value < 0.05). In contrast, the Daniel score did not exhibit significant diagnostic value in predicting APE (P value = 1.101) (Table 3).
Results of ROC Analysis Evaluating the Diagnostic Value of APE Predictive Criteria.
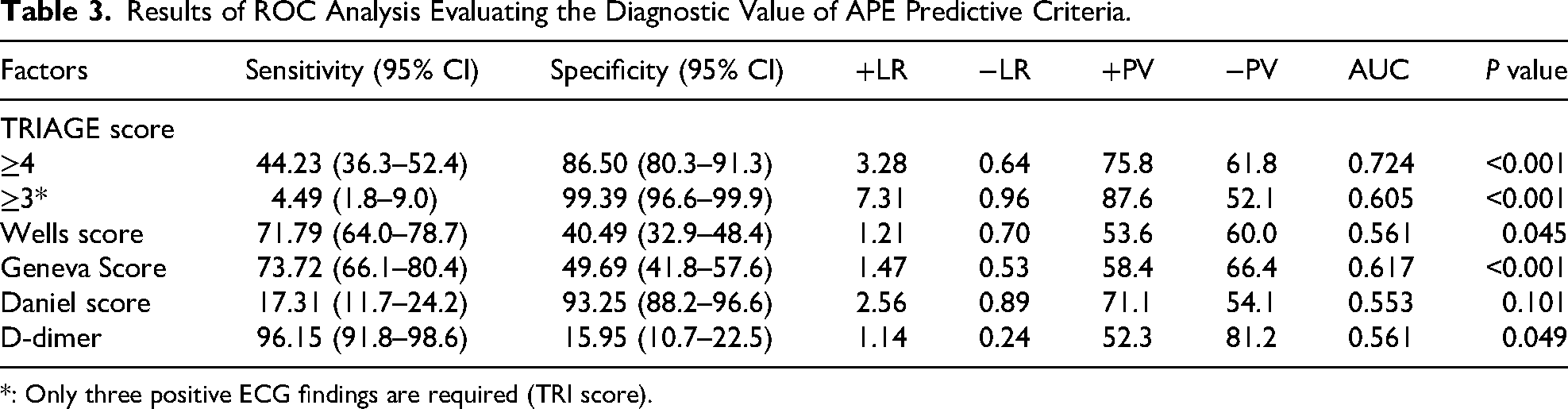
*: Only three positive ECG findings are required (TRI score).
In addition to sensitivity and specificity, we calculated the negative predictive value (NPV) and positive predictive value (PPV) for each tool. D-dimer demonstrated the highest NPV (81.2%), supporting its utility in ruling out APE. The TRIAGE score (cut-off ≥4) showed a strong PPV (75.8%) but a lower NPV (61.8%), indicating its greater suitability for confirming disease. Wells and Geneva scores yielded moderate NPVs (60.0% and 66.4%, respectively), while the Daniel score had limited utility due to low sensitivity and NPV (54.1%) (Table 3).
Additionally, a comparison of the newly developed ECG scoring system, the TRIAGE score, with other established criteria demonstrated that it possesses a significantly greater diagnostic value than the Wells, Geneva, Daniel scores, and D-dimer levels (P value < 0.001) (Figure 1).
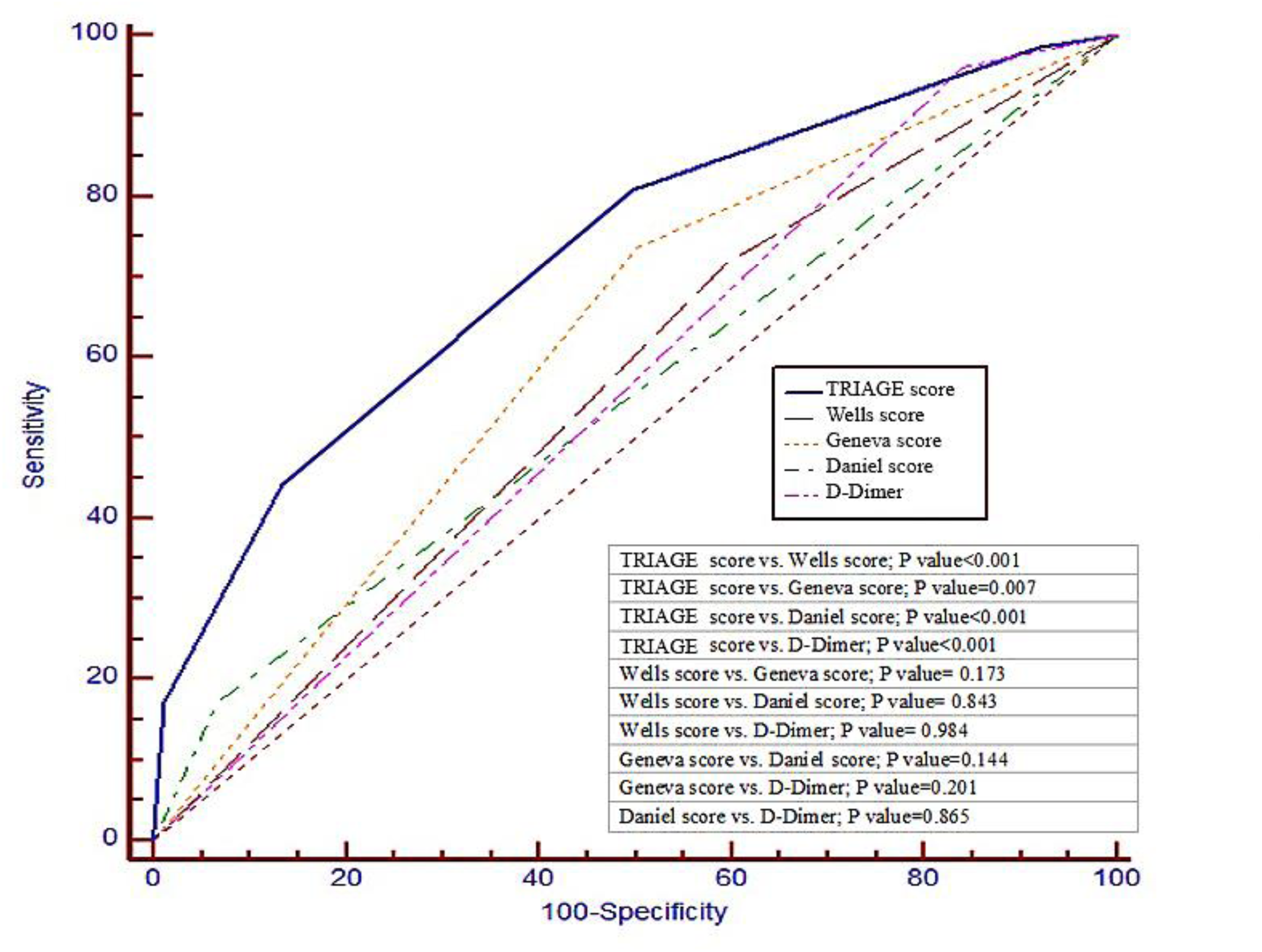
ROC Curve Comparing the Diagnostic Value of APE Predictive Criteria.
Discussion
In this study, 16 ECG findings were evaluated for their relevance in diagnosing APE, leading to the development of a new scoring system. Key ECG findings—tachycardia, RBBB (complete/incomplete), and inverted T-waves in the right precordial leads (V1-V4)—were identified as significant predictors. Additionally, three basic patient characteristics—age, gender, and edema—were directly and significantly associated with APE. These combined factors form the TRIAGE scoring system. Notably, if all three ECG parameters are positive, the specificity reaches an impressive 99.39%, significantly raising the likelihood of an APE diagnosis. Furthermore, even when incorporating patient characteristics alone, the specificity remains high, emphasizing the robustness of the TRIAGE criterion.
In this regard, Vereckei et al developed a new score called nECG to estimate the probability of APE. The mentioned criterion consisted of 5 ECG criteria including (1) S1Qinferior Tinferior or S, +T wave inversion in leads V1-3, (2) primary ST segment elevation in the inferior leads and/or lead aVR and/or leads V1-3 or T wave inversion in the inferior leads and/or leads V1-3¬, (3) QR or qR complexes or R/S > 1 in leads V1, (4) Terminal r’ wave in leads aVR and/or S1, S2, S3 syndrome and/or S wave in leads aVL, V4-6 and/or fragmented or slurred QRS complexes in lead aVR leads V1-3 and/or inferior leads, and (5) primary ST segment elevation and/or QS or QR complexes in leads RV4-6, which best identified the key pathogenetic stages of APE. The results of their study showed that the diagnostic value of nECG had a sensitivity of 98.7%, a test accuracy of 84.4%, and a likelihood ratio (LR) of 0.019 and was superior to other standard criteria (such as Wells and Geneva criteria). In addition, the specificity of nECGs was 69% lower than that of the Daniel-ECG and Wells scores. The mentioned difference was not statistically significant and was superior to the Geneva score. 12
The key distinction between the mentioned study and the current study lies in the TRIAGE criterion, which exhibits exceptionally high specificity and surpasses all previously established standard criteria. Similarly, Wang et al developed the CHARIS model, incorporating factors such as COPD, CHF, CHD, HTN, atrial arrhythmias/AF, RBBB, RAD, inverted T-waves, and the S1Q3T3 pattern to evaluate the Qanadli score. Their findings demonstrated that the CHARIS algorithm effectively identified acPTE patients with significant thrombus burden even prior to imaging diagnosis. 1
In the same vein, Su et al also introduced a new ECG model called SPPH-ECG consisting of 14 ECG findings that were not included in the previously introduced ECG scores. The SPPH-ECG model had a superior AUC (0.8741), sensitivity of 79.08%, and test accuracy of 79.42%. They used the logistic regression formula to determine their benchmark score and showed that the cut-off point of 0.3228 could correctly diagnose acPTE with a probability of more than 42%. The study compared the diagnostic value of the ECG model with that of the other ECG scoring models (Daniel-ECG score) and the most common prediction models (Wells and Geneva score). In this comparison, the AUC of the new SPPH-ECG model was significantly higher than that of the other standard criteria such as Geneva, Wells, and Daniel, indicating the better performance of this model. Moreover, they stated that the Geneva criterion had the highest specificity level of 100%. Therefore, the SPPH-ECG model in combination with the Geneva scoring system can more accurately diagnose APE. 15
Notably, the TRIAGE criterion developed in this study consists of just six components: three ECG findings and three baseline patient characteristics, scored using a simple binary system (0 and 1). This simplicity and reliance on fewer ECG parameters enhance its practicality and ease of use. Furthermore, the TRIAGE criterion, whether applied with or without baseline patient characteristics, demonstrated the highest specificity among diagnostic tools. Importantly, it achieves this accuracy independently, without needing to be combined with other standard criteria like the Geneva score to improve diagnostic performance.
To further elucidate the contribution of each component, we calculated the individual AUC values for tachycardia, RBBB, inverted T-waves, age, and edema. While each predictor demonstrated modest discriminatory ability on its own, their combined AUC was notably higher, reinforcing the additive value of integrating clinical and electrocardiographic features. These results support the rationale for composite modeling, particularly in emergency settings where multifactorial assessment enhances diagnostic precision. The individual and combined AUC values are detailed in Appendix 1.
Previous research has demonstrated a higher prevalence and greater number of ECG changes in patients with massive pulmonary embolism, suggesting a correlation between ECG abnormalities and PE severity. Among the most significant findings were ST-segment depression with concurrent elevation, negative T-waves in leads V1–V3, and electrocardiographic indicators of right ventricular strain. These features may serve as valuable markers for assessing the severity of embolic burden. 16 In alignment with these observations, the 2024 SCST guidelines advocate for systematic ECG interpretation incorporating signs of right heart strain—such as ST-segment changes and T-wave inversions in the right precordial leads—reinforcing the diagnostic utility of these patterns in evaluating suspected cases of PE. 17
In our study, inverted T-waves in the right precordial leads V1-V4 were identified as a key ECG finding in APE patients. These changes reflect right ventricular ischemia or stress, resulting from altered depolarization and repolarization of the heart muscle due to pressure on the right ventricle. Additionally, inverted T-waves in these leads are often observed in conjunction with other ECG findings, such as the SIQ3T3 pattern, RBBB, and sinus tachycardia. Notably, RBBB and tachycardia also showed significant associations with APE in our analysis.18–20
Moreover, several studies have recognized that patients with APE often exhibit ST-elevation (STE) in leads V1–V3.21–25
Numerous justifications have been provided as the leading cause of right precordial lead STE that is attributed to the right ventricle transmural ischemia in most of the cases. 18 The underlying mechanism for RV transmural ischemia development in APE still remains ambiguous although some explanations have been proposed in this respect. Enough systolic pressure cannot be generated by the RV during RV dilation and failure. As a result, the acute increase in afterload cannot be overcome and in turn leads to an increased RV oxygen demand and a remarkable decrease in pulmonary perfusion. The mentioned outcomes along with a leftward shift of the interventricular septum decrease the left ventricular preload, coronary flow, and the cardiac output and can result in the ensuing hypoxia and severe RV transmural ischemia, causing STE in leads V1–V3/V4.26–30Recent ESC guidelines also highlight the diagnostic relevance of ST-elevation equivalents and dynamic ECG changes, reinforcing the importance of early recognition of right ventricular ischemia in suspected APE cases. 31
Atrial arrhythmias and specifically atrial fibrillation, which may be associated with APE, can be caused by neurohormonal activation, tricuspid valve insufficiency, and acute RV failure. 7 In this regard, according to a large study, 24% of patients with APE had atrial fibrillation. 32
It should be noted that in our study, patients with APE had no evidence of history of heart disease and only the three ECG items mentioned in this study played a significant role in the diagnosis of APE.
Other studies have explored machine learning-based models utilizing ECG signals to enhance APE screening. Three distinct machine learning models were developed to estimate the probability of PE. One model relied solely on ECG waveform data (ECG model), another used only patient clinical data, including demographics, laboratory results, respiratory factors, and comorbidities (EHR model), while the third combined both ECG waveform data and clinical information (fusion model). The results demonstrated that the fusion model, with an AUC of 0.81, outperformed the ECG and EHR models, which achieved AUCs of 0.59 and 0.65, respectively. Additionally, the fusion model surpassed other conventional diagnostic criteria. The researchers concluded that deep learning approaches integrating ECG waveforms with traditional clinical data can significantly improve the specificity of PE diagnosis in patients with moderate suspicion of the condition. 13 The 2025 ACS guidelines underscore the need for integrated diagnostic strategies beyond ST-elevation, aligning with the TRIAGE model's combined use of waveform and clinical data to enhance specificity. 33
The modeling results of the referenced study align with the findings of the present study, where the TRIAGE score, comprising ECG findings along with basic patient characteristics (age, gender, and edema), demonstrated the highest specificity. Additionally, the TRIAGE score showed a significantly higher diagnostic accuracy (65.36%) compared to other methods such as the Wells, Geneva, Daniel, and D-dimer criteria, with the highest AUC (0.724).
Although the AUC of 0.724 does not indicate excellent discrimination, it reflects acceptable diagnostic performance in emergency settings. As noted by Çorbacioğlu and Aksel (2023), AUC values between 0.7 and 0.8 are considered moderately accurate and clinically useful when interpreted in context. 34
Notably, the Daniel criterion lacked significant diagnostic value in identifying APE, while the Wells criterion and D-dimer (above 500 ng/ml) displayed borderline significance. The Geneva criterion, with a sensitivity of 73.72% and specificity of 49.69%, was effective in diagnosing APE.
In contrast to existing tools, which rely on high sensitivity, the new TRIAGE score is distinguished by its high specificity, enabling more definitive diagnoses of APE. Tools such as the Wells, Geneva, and D-dimer tests, due to their high sensitivity, often diagnose APE in over 50% of suspected cases. This can result in emergency bed overcrowding, prolonged waiting times for CTA, unnecessary radiation exposure, and increased financial burden. The simplicity of the TRIAGE scoring system, requiring neither specialized expertise nor imaging, makes it particularly advantageous. Its high specificity reduces false positives, facilitating more accurate diagnosis and faster treatment management for APE patients in the emergency department.
In this context, the negative predictive value (NPV) becomes particularly relevant. Our analysis showed that D-dimer, with its high sensitivity (96.15%) and NPV of 81.2%, remains the most reliable tool for ruling out APE. Conversely, the TRIAGE score (cut-off ≥4) demonstrated a strong PPV (75.8%) for confirming disease but a lower NPV (61.8%), making it more suitable for rule-in scenarios. These findings support a two-step diagnostic strategy: using D-dimer to exclude APE and the TRIAGE score to confirm it, thereby optimizing resource allocation and minimizing unnecessary imaging.
Although the TRIAGE score achieved the highest diagnostic accuracy among the evaluated tools, its AUC of 0.724 reflects moderate discriminatory ability. While not outstanding, this level of performance remains clinically meaningful in emergency settings, where rapid decision-making is essential. The associated confidence interval (0.697-0.795) is reasonably narrow, supporting acceptable discriminative power.
Limitations
This study offers encouraging findings regarding the potential utility of the TRIAGE scoring system; however, several limitations should be acknowledged. First, the retrospective design restricted the analysis to data available in patients’ medical records, which may have introduced selection bias and limited the scope of clinical variables. Although a substantial number of records were reviewed across two hospitals, only a subset of patients met the inclusion criteria, which could affect the generalizability of the results.
Second, the performance of the TRIAGE model has not been evaluated in specific patient subgroups, such as individuals with left bundle branch block (LBBB), pre-existing cardiac dysfunction, severe pulmonary disease, or a low clinical probability of PE. These populations may exhibit distinct ECG features or pathophysiological profiles that could influence the model's diagnostic accuracy.
Third, while this study involved data from two clinical centers, the findings would benefit from validation in larger, prospective cohorts across diverse geographical and clinical settings. Multi-center studies incorporating varied patient demographics are essential to strengthen the reliability and external validity of the TRIAGE score.
Fourth, obesity was not included in the regression analysis due to inconsistent documentation of BMI-related data in the retrospective records. This omission limits the model's ability to evaluate obesity as a potential predictor of thromboembolic risk. Future research should consider systematic inclusion of BMI or obesity indices to enhance the predictive accuracy and clinical relevance of TRIAGE.
Lastly, the current model primarily addresses acute presentations of PE. Its diagnostic performance in detecting chronic or subclinical forms of PE remains uncertain and warrants further investigation. Prospective studies targeting these specific domains will be necessary to fully elucidate the scope and applicability of the TRIAGE scoring system in broader clinical contexts.
Conclusion
This study presents the TRIAGE score as a novel diagnostic approach that integrates ECG findings—tachycardia, RBBB (complete/incomplete), and inverted T-waves in leads V1–V4—with patient characteristics including age, gender, and edema. At a cut-off score of ≥4, the TRIAGE model demonstrated high specificity in identifying APE and performed favorably when compared with established criteria such as Wells, Geneva, and Daniel. Notably, when all three ECG parameters were present (score = 3), the model achieved 100% specificity within the study sample. These findings suggest the TRIAGE score could serve as a practical and accessible tool in resource-limited environments, potentially supporting timely APE diagnosis and guiding clinical decision-making when imaging modalities are unavailable or delayed.
Implications for Practice
Accurate Diagnosis: TRIAGE score offers high specificity, outperforming other criteria like Wells, Geneva, and Daniel.
Improved ED Workflow: Simplifies diagnosis, reduces delays, minimizes ED crowding, and optimizes patient management.
Use in Resource-Limited Settings: Effective alternative when advanced tools like CTA or D-dimer are unavailable.
Insights on RV Dysfunction: Highlights ECG findings (eg, inverted T-waves, RBBB) linked to right ventricular stress, aiding targeted treatments.
Supports Timely Therapy: Ensures rapid initiation of appropriate interventions, improving patient outcomes.
Prevents Overuse of Resources: Reduces false positives, unnecessary imaging, and associated costs.
Potential Broader Applications: Validating TRIAGE in diverse patient groups could expand its diagnostic utility.
Encourages Future Research: Advocates for studies on simple, non-invasive ECG-based scoring systems.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251391143 - Supplemental material for TRIAGE Scoring System: Advancing ECG-Based Early Detection of Acute Pulmonary Embolism
Supplemental material, sj-docx-1-cat-10.1177_10760296251391143 for TRIAGE Scoring System: Advancing ECG-Based Early Detection of Acute Pulmonary Embolism by Mehdi Nasr Isfahani, Azardokht Rahiminik, Zahra Molaei and Faezeh Tabesh in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Abbreviations
Acknowledgments
The authors wish to thank the emergency department staff at Shahid Chamran and Al-Zahra hospitals for their support during data collection. Special thanks are extended to Dr Asieh Maghami Mehr for her expert assistance in data preparation and manuscript refinement.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki (World Medical Association [WMA], 2013) and was approved by the Research Ethics Committee of Isfahan University of Medical Sciences (Approval No: IR.MUI.MED.REC.1403.145). The ethics committee approved the use of anonymized data without requiring patient consent, as the data did not permit individual identification. Additionally, legislation on data safety and confidentiality was strictly followed.
Author Contributions
M.N.I., A.R.N., and F.T. contributed to the conception and design of the work. M.N.I., A.R.N., and F.T. contributed to data interpretation, drafting, and critical revision of the paper. Z.M. helped with data collection and provided the initial draft of the manuscript. All authors read and approved the final version of the article.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was not funded by any organization. The authors wish to thank Vice Chancellery for research at Isfahan University of Medical Sciences for providing support for this research with project No. 3403168.
Declaration of Conflicting Interests
The authors declare that they have no conflicts of interest.
Data Availability
Data are available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.