
Abstract
Introduction
According to the current European Society of Cardiology (ESC) guidelines reaching the diagnosis of acute pulmonary embolism (APE) requires a multistep approach which includes plasma
The purpose of this study was to establish and detect the optimal prognostic cutoff point for plasma DD levels measured during diagnostic evaluation in predicting in-hospital complications to further improve the prognostic value of sPESI by combining it with DD levels measured during diagnostic workup. This modification could aid clinical decision-making. For example, patients classified as low risk could be discharged early or managed entirely as outpatients, especially in the era of novel direct anticoagulants, whereas patients estimated as high risk may benefit from a more intensive care. This approach would be of value especially in the plentiful sPESI ≥1 subgroup, where the estimated morality is 8.9%, and an augmented identification of truly low-risk patients would lead to shortened hospital stay and a reduction in supplementary tests. 9
Methods
Study Design
A single-center study based on the post hoc analysis of a prospective observational cohort of consecutive patients hospitalized with APE, with symptoms suggestive of APE lasting no longer than 14 days, who underwent plasma DD testing as part of the diagnostic workup, followed by multislice computed tomography (MSCT) of pulmonary arteries in the evaluation for APE, between January 2013 and June 2016. Patients were treated according to contemporary ESC guidelines.
Imaging Studies
Acute pulmonary embolism was confirmed by contrast-enhanced MSCT when thromboemboli were visualized at least at the level of segmental pulmonary arteries and in 1 case of inconclusive MSCT findings with a positive ultrasonographic lower limb venous compression test. Data were collected from patient records. Multislice computed tomography angiography was performed using 64-row Toshiba Aquilion (Toshiba Medical Systems, Otawara, Japan) or 16-row GE LightSpeed Pro systems (General Electric Medical Systems, Waukesha, Wisconsin). The ultrasonographic lower limb compression test was performed with Philips XD11XE system (Philips Medical Systems, Best, the Netherlands) using a linear transducer (L12-3) according to the standard protocol.
Transthoracic echocardiography for right ventricular dysfunction (RVD) was defined as right/left ventricle diameter ratio ≥0.9 from the 4-chamber apical view, a cutoff point which is in concordance with ESC guidelines on APE and guidelines of the American Heart Association on the management of pulmonary embolism. 1,11 All examinations were performed by a physician certified in echocardiography during the first 24 hours from admission using the Philips iE33 or Philips HD11XE system (Philips Medical Systems).
Biochemical Analysis
Plasma DD concentrations were quantitatively measured during diagnostic workup using an automated enzyme-linked fluorescent assay with a reference range of values up to 500 ng/mL (VIDAS DD Exclusion; bioMerieux, France). High-sensitive troponin T (hsTnT) was assayed at admission and measured using an automated quantitative electrochemiluminescence immunoassay (Roche Elecsys, Mannheim, Germany). Myocardial injury was diagnosed when hsTnT >0.014 ng/mL.
Simplified Pulmonary Embolism Severity Index
The sPESI score was calculated by the attending physician or assessed post hoc using the following parameters acquired at baseline: age >80 years, history of cancer, history of chronic cardiopulmonary disease, heart rate ≥110 bpm, systolic blood pressure <100 mm Hg, and oxygen saturation <90%. Patients with zero points were classified as low risk, patients who scored 1 point or above as high risk. 9
The Study End Points
The study end point comprised in-hospital serious adverse events (SAEs) defined as: death, hemodynamic deterioration requiring rescue thrombolysis or need for cardiopulmonary resuscitation, or major bleeding defined according to the International Society on Thrombosis and Haemostasis. 12
Statistical Analysis
In this exploratory study, data are expressed as parameter or median followed by interquartile range. Kolmogorov-Smirnov test was used to identify continuous variables with a skewed distribution which were then compared using the Mann-Whitney U test or χ2 test. Kruskal-Wallis test was used to compare means in more than 2 patient groups. All tests were 2-sided. For all performed tests P values of < .05 were considered significant. Receiver operating characteristic (ROC) analysis was used to determine the area under the curve (AUC) for DD levels in regard to serious adverse in-hospital events. The first cutoff level for DD characterized by a 100% negative predictive value (NPV) for SAE was chosen, the second DD cutoff value was determined with Youden index and was used for the calculation of the Cox proportional hazard model. Univariable analysis in regard to in-hospital complications using the Cox proportional hazard model was performed. Next, the prognostic relevance of covariates was assessed using a multivariable model with forward and backward stepwise selection (P value for inclusion .05, P value for exclusion .15). Finally, the net reclassification improvement (NRI) was calculated for DD levels as described by Pencina et al. 13 All analyses were performed using the STATISTICA 13 data analysis software system.
Results
The final analysis comprised 270 patients (143 female [53.3%], median age 66 years [25th-75th percentile, 49-81]) diagnosed with APE. According to the ESC guidelines, 54 patients were classified as low risk of early mortality, 198 patients as intermediate risk, and 18 patients as high risk. A total of 165 (61%) patients had a sPESI score of above zero. The flow of patients is presented in Figure 1. A full study group characteristic is presented in Table 1. There were 25 SAEs (14 deaths, 10 successfully treated hemodynamic deteriorations, 1 bleeding complication) of which 24 occurred in the sPESI ≥1 group.
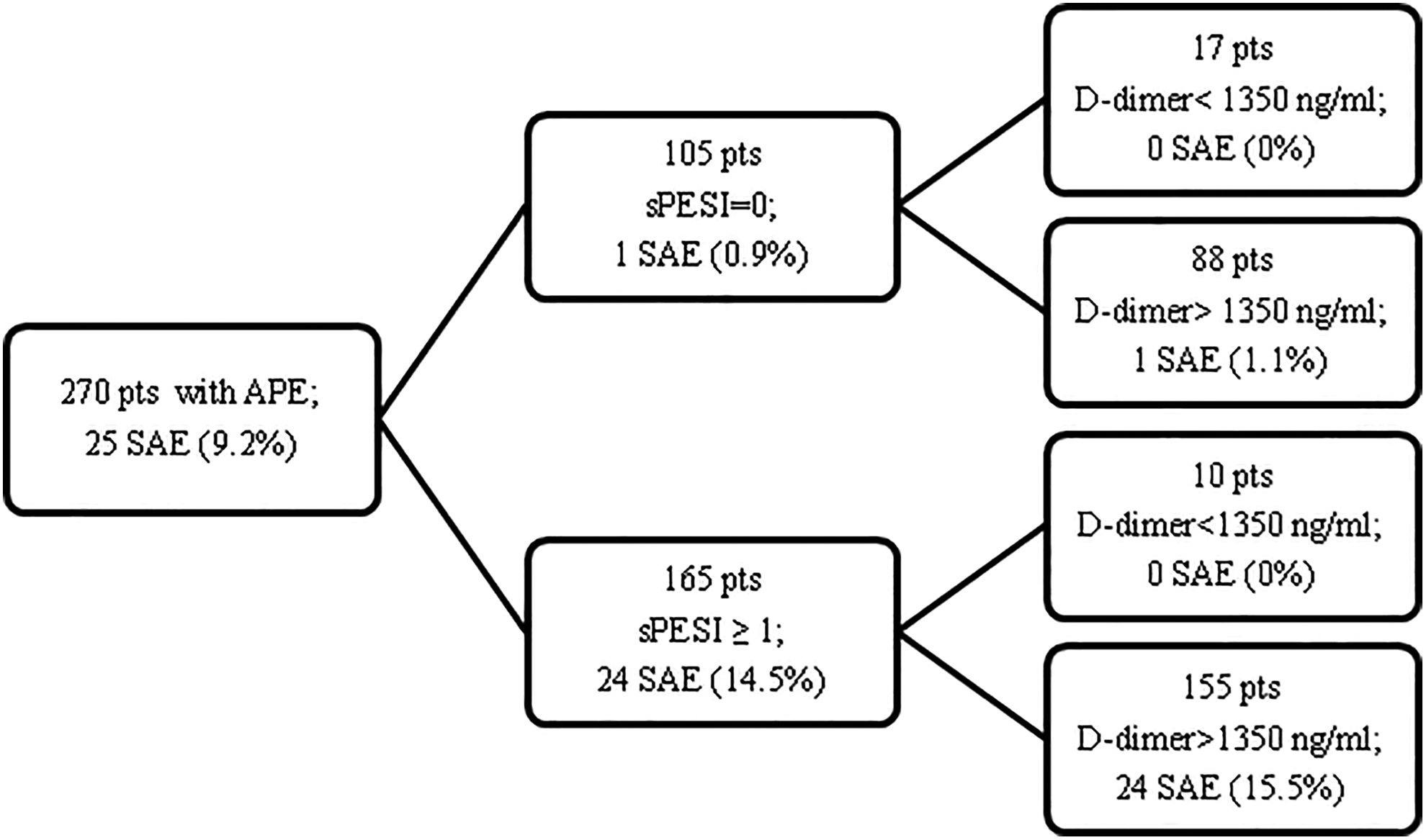
Flow of patients in the study. Adding
Characteristic of Patients in the Study Group.a
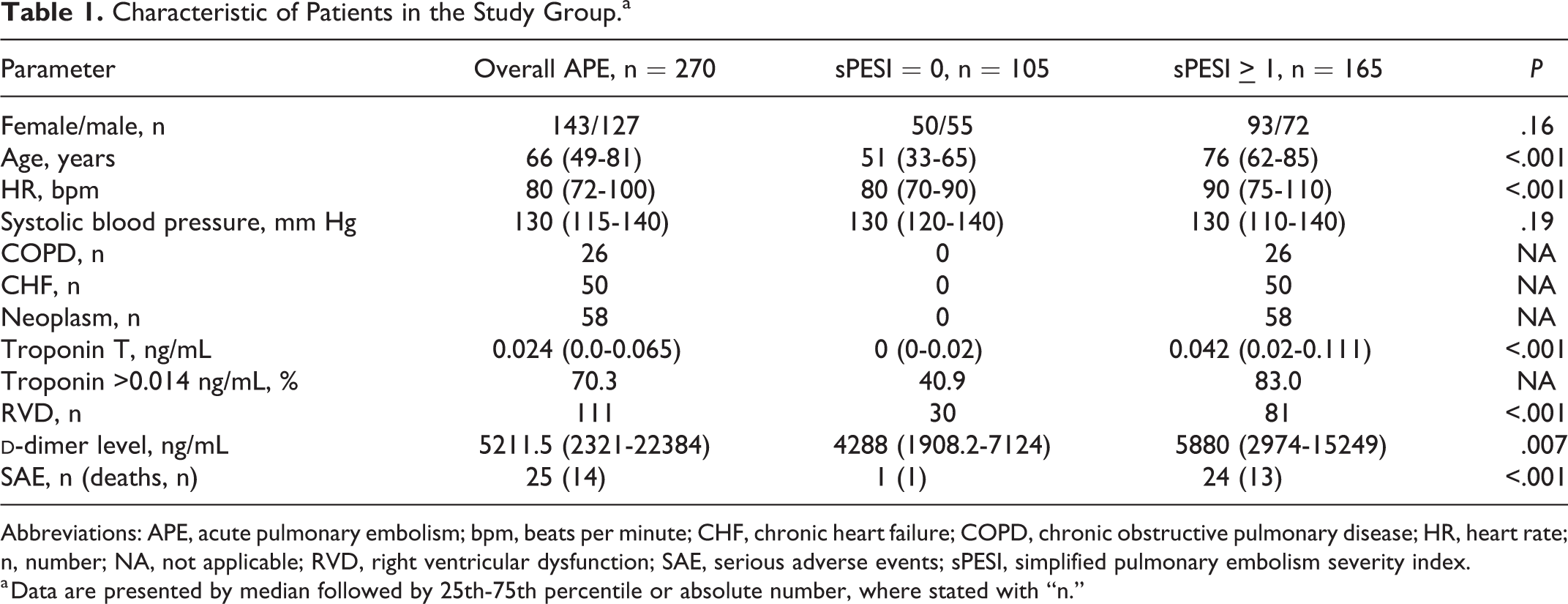
Abbreviations: APE, acute pulmonary embolism; bpm, beats per minute; CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; HR, heart rate; n, number; NA, not applicable; RVD, right ventricular dysfunction; SAE, serious adverse events; sPESI, simplified pulmonary embolism severity index.
a Data are presented by median followed by 25th-75th percentile or absolute number, where stated with “n.”
High-risk patients had significantly higher DD levels than intermediate and low-risk patients (8469.5 ng/mL, 5418 ng/mL, and 2613.5 ng/mL, respectively, P <.001), as shown in Figure 2. The median DD level in the sPESI ≥1 group was significantly higher than in the sPESI = 0 group, 5880 ng/mL (2974-15249 ng/mL) versus 4288 ng/mL (1908-7124 ng/mL), respectively, P = .007 (Figure 3). Moreover, DD levels were elevated in 111 patients with RVD at TTE when compared to patients with preserved RV function (6012 ng/mL [2810-16 018 ng/mL] vs 4476 ng/mL [2486-7631 ng/mL], P = .04) and were higher in 175 patients with signs of myocardial injury (hsTnT > 0.014 ng/mL; 6346 ng/mL [3566-18558.5 ng/mL] vs 2751 ng/mL [1681-5236 ng/mL], P <.001). Importantly, DD levels were higher in patients with SAE than in patients with a benign course, 7247 ng/mL (4553-27750 ng/mL) versus 5156 ng/mL (2149-11229 ng/mL), P = .004 (Figure 4). Area under the curve in ROC analysis of DD levels for SAE was 0.672 (95% CI 0.559-0.785), P = .003 (Figure 5). The NPV of sPESI was 99%. We identified the DD level of 1350 ng/mL with a NPV of 100% for SAE which allowed for the exclusion of 11 patients (6.6%) with sPESI ≥1 and identified the single patient who experienced an SAE (death) from the low-risk group. Finally, the NRI for DD levels above 1350 ng/mL and sPESI ≥1 versus standalone sPESI ≥1 was calculated, NRI = 0.085, Standard Error = 0.042, P = .04. Youden index was used to determine the optimal cutoff point for DD levels in the regression models. Results for the univariable regression model for SAE are shown in Table 2. Results of the exploratory multivariable regression model for SAE are shown in Table 3.
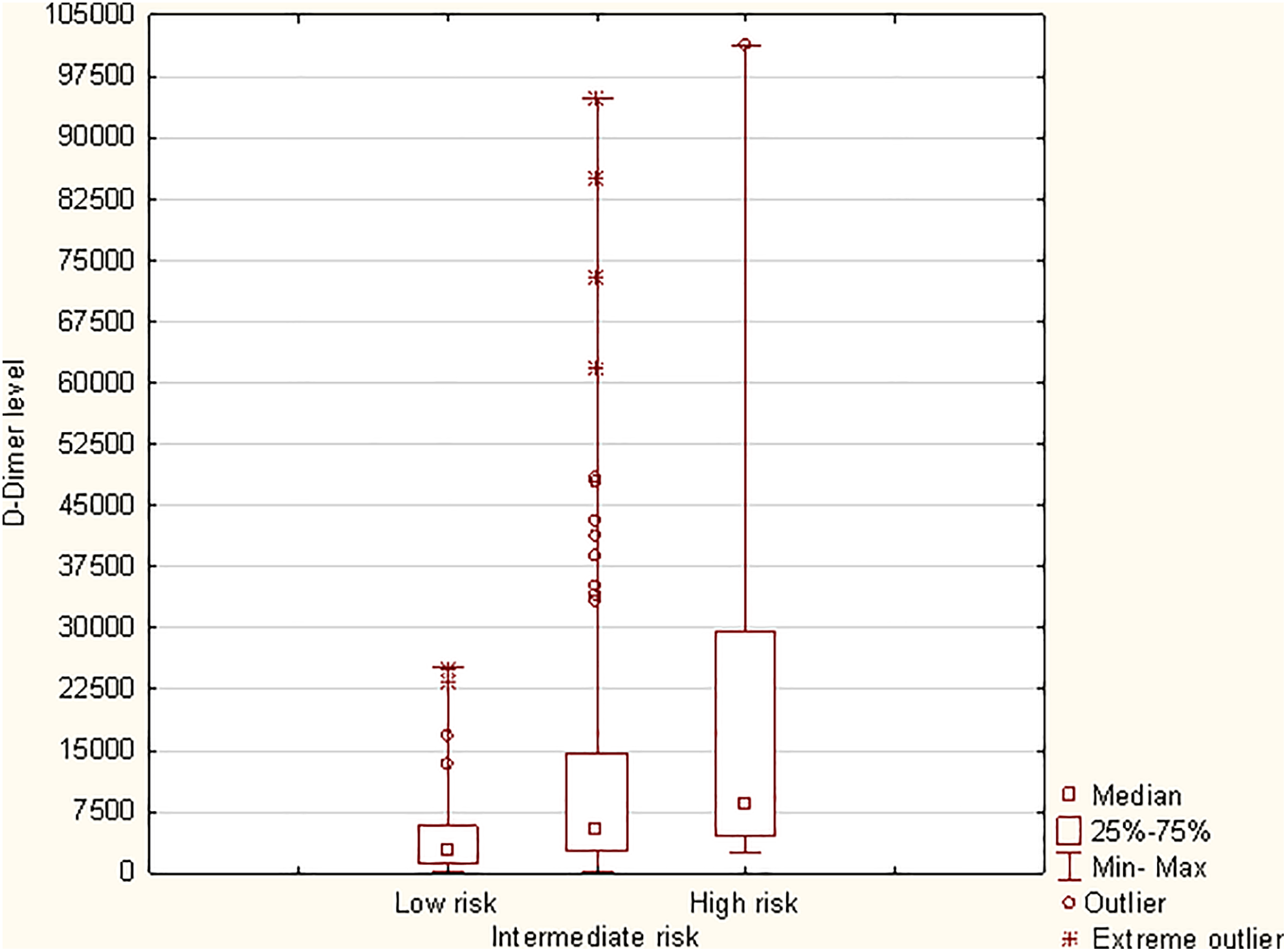
Median
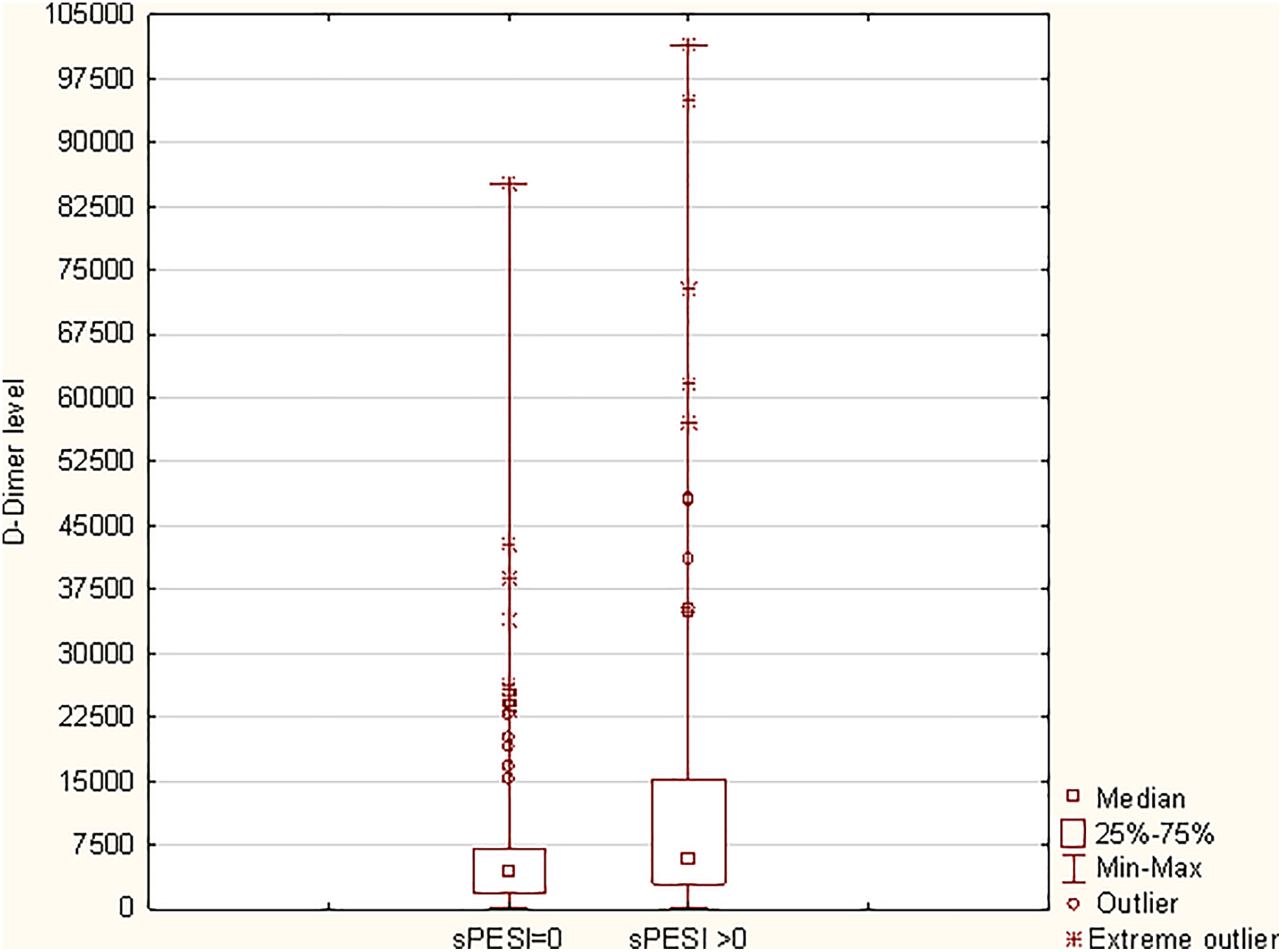
Median
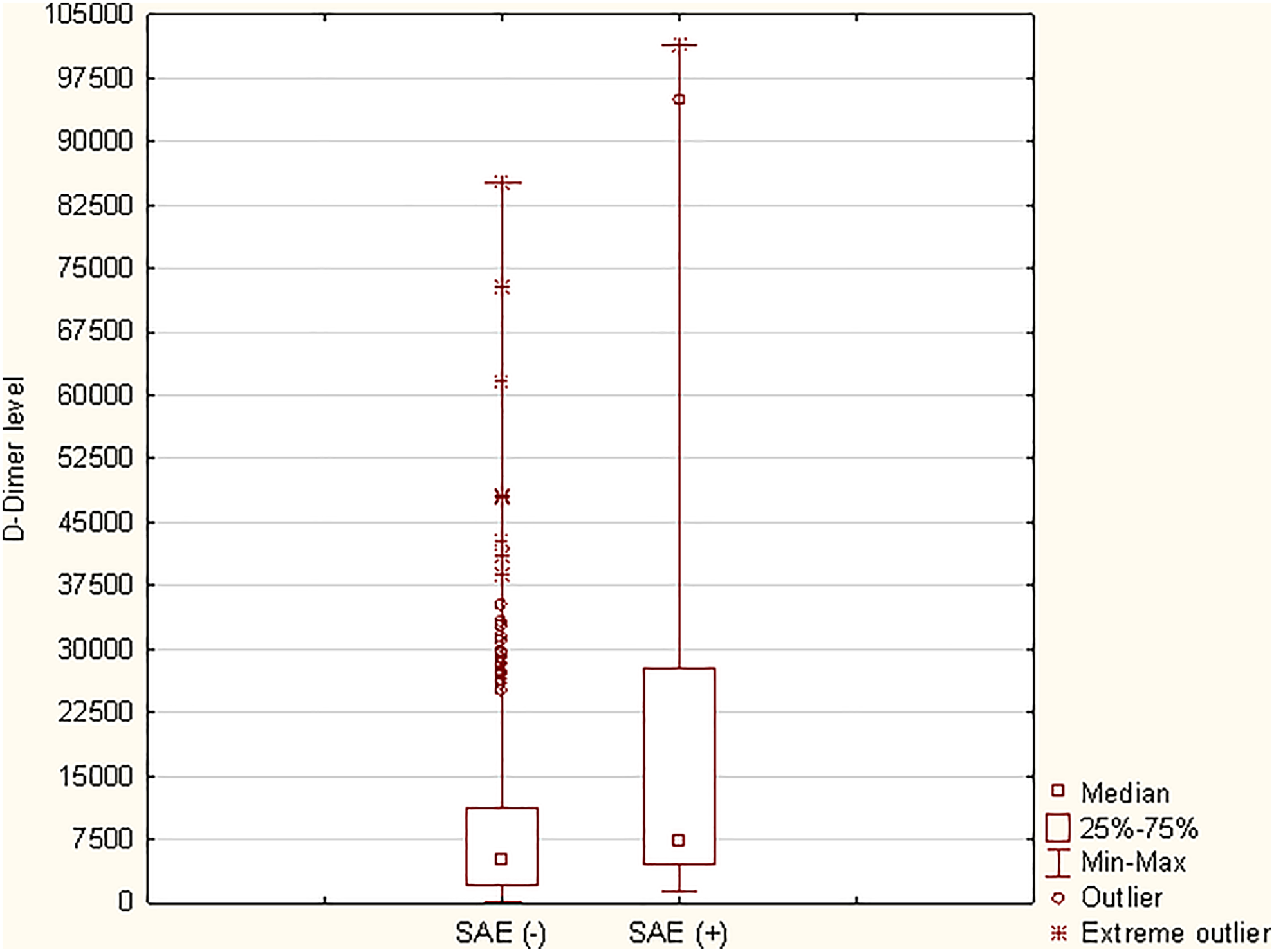
Median
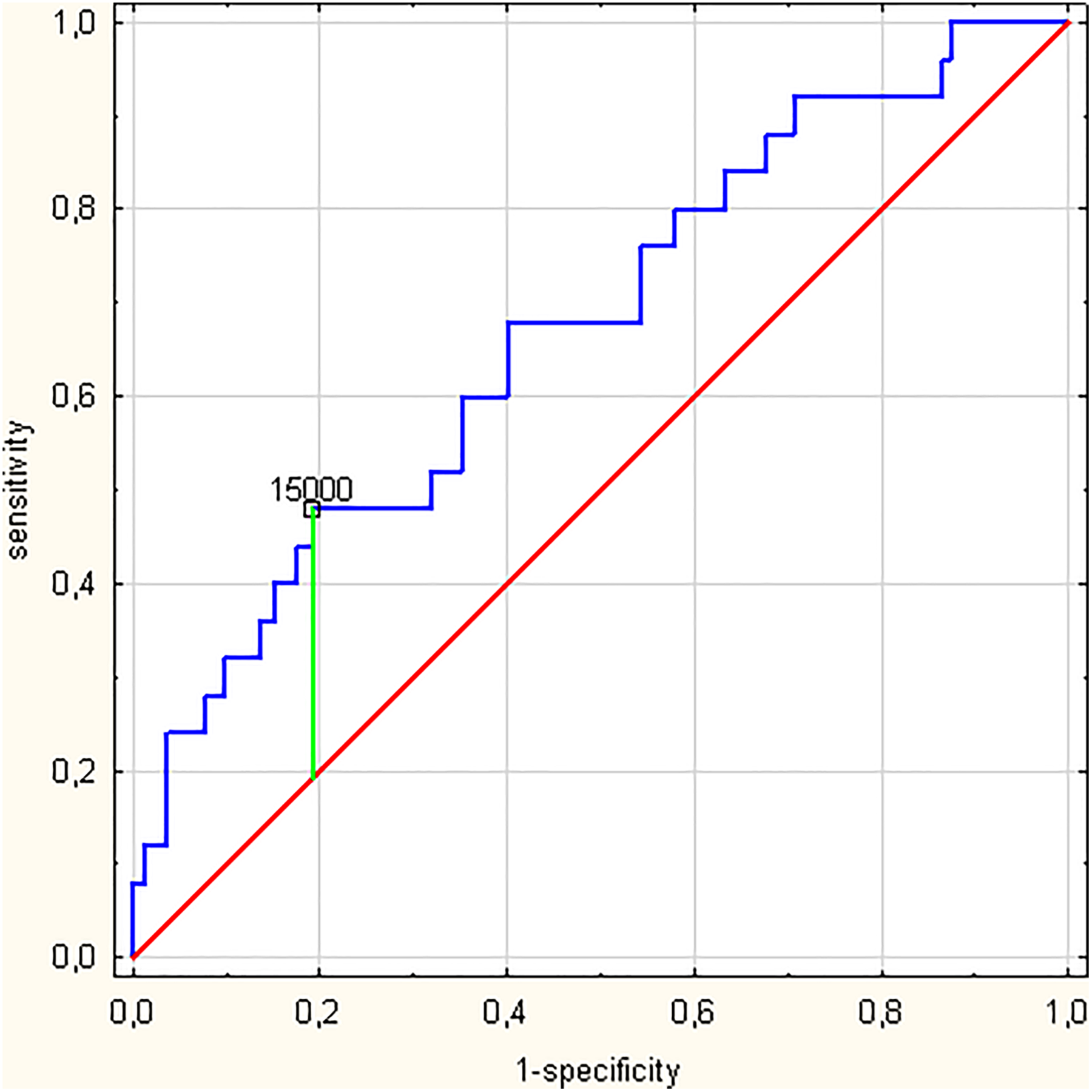
Receiver operating characteristic (ROC) analysis for
Predictors of In-Hospital Adverse Outcomes by Univariable Cox Proportional Hazard Regression Analysis.a
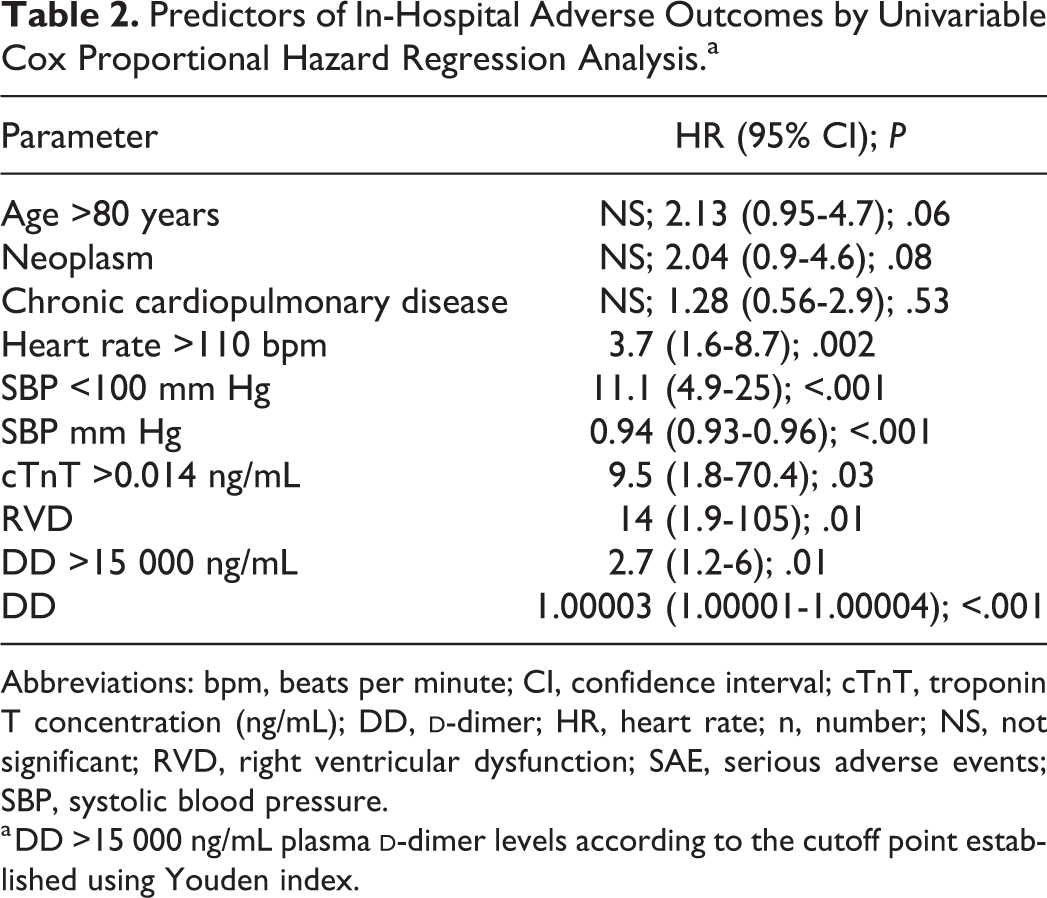
Abbreviations: bpm, beats per minute; CI, confidence interval; cTnT, troponin T concentration (ng/mL); DD,
a DD >15 000 ng/mL plasma
Predictors of SAE by Multivariable Logistic Regression Analysis.
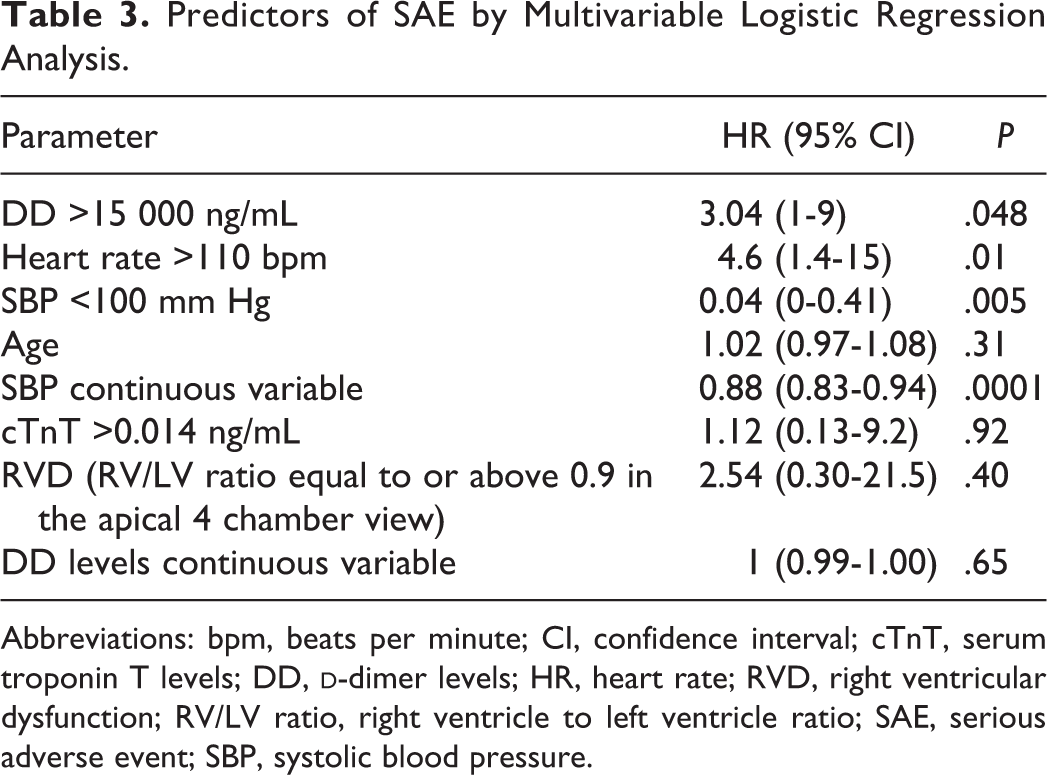
Abbreviations: bpm, beats per minute; CI, confidence interval; cTnT, serum troponin T levels; DD,
Discussion
The management of APE depends on the risk of early mortality, which is mostly related to the hemodynamic status, presence of comorbidities, and the severity of RV strain. Patients classified as low risk of early mortality may benefit from oral anticoagulation administered even as outpatient treatment. Identification of these low-risk patients is currently based largely on the sPESI score, which classifies approximately 30% as low risk, leaving the majority of patients in the non-low-risk group. 9,10 Thus, the aim of this study was to examine the usefulness of adding DD to sPESI in risk stratification to better identify truly low-risk patients.
In this study, DD levels were related to the severity of APE. Specifically, we found that significantly higher plasma DD levels were observed in patients with RVD assessed by imaging studies, in those with elevated biomarker concentrations, in those with a higher risk of early mortality according to the ESC criteria, and in those with sPESI ≥1. The association between higher pulmonary artery clot burden, more proximal clot location, and higher levels of DDs has been reported. 14 –17 However, in these studies, a cutoff point ranging from 2000 to 3000 ng/mL was proposed. Correspondingly, the positive correlation between increased plasma DD levels and RVD in imaging studies (both computed tomography and echocardiography) has been described. 18 –21 Since there is no gold standard for the echocardiographic definition of RVD, various aforementioned authors have demonstrated the association with a wide set of parameters, among them are systolic tricuspid annular velocity, RV systolic pressure and estimated pulmonary vascular resistance, RV to left ventricle ratio, and myocardial performance index, with authors noting plasma DD levels of 3000 ng/mL, higher than in this study, as a cutoff point.
Moreover, our findings confirm the link between increased plasma DD levels and SAEs; however, unlike in previous reports, in this study, a lower cutoff point for DD of 1350 ng/mL was associated with the occurrence of in-hospital SAEs. 5 –8 Importantly, in our study, elevated DD levels significantly predicted in-hospital SAE with AUC 0.672. Moreover, higher DD levels significantly increased the risk of in-hospital complications in the univariable analysis, moreover in a multivariable model, DD levels above 15 000 ng/mL were found to be an independent risk factor for SAEs. Furthermore, the DD level below 1350 ng/mL demonstrated a 100% NPV for SAE. This cutoff point allowed for the identification of 1 patient originally allotted to the low-risk group according to sPESI (0 points) who died. It is worth underlining that employing plasma DD levels in the prediction of SAE alone, in this study, was not reliable, as shown by the unsatisfactory AUC. This may be attributed to the many physiological and pathological states, present in cohort, which increase plasma DD concentrations (ie, age, cancer). On the other hand, the combination of sPESI = 0 and plasma DD levels below 1350 ng/mL allowed for the identification of all patients with a benign course and when both criteria were applied, 6.6% of patients with sPESI scores of above 0 were reclassified as low risk. Thus, sPESI in combination with DD levels below the threshold of 1350 ng/mL may more accurately identify patients with benign clinical course and who are potential candidates for outpatient treatment.
To the best of our knowledge, there is only one other report examining the value of adding plasma DD levels to sPESI assessment, in which Polo Firz et al describe a similar beneficial finding, but in an older group of patients aged 65 years old and above. 7 There is also 1 study which identified a pulse rate above 100/min and DD levels above 3000 ng/mL as risk factors upon multivariate analysis of adverse events during the first 10 days of hospitalization. 8 We tested and confirmed that a pulse rate above 110/min is a significant predictor of SAE. Other published reports centered around the addition of different biomarkers to sPESI to guide outpatient treatment are focused on established prognostic markers routinely assessed as a second step, such as the plasma concentration of troponin T and troponin I, rather than plasma DDs, a marker routinely used for diagnostic purposes. 20 –23
The ESC guidelines state that low-risk patients, defined as those with an sPESI score of 0 may be eligible for out-patient treatment. In this study, increased DD levels measured during diagnostic workup showed a positive correlation with RVD and the plasma concentration of hsTnT. The strategy of combining sPESI with DD levels showed 100% sensitivity in identifying patients who experienced SAE. On the other hand, no patient with a DD level of below 1350 ng/mL experienced a complicated course, irrelevant of the sPESI score.
Recently, a number of novel anticoagulants, which do not require international normalized ratio (INR) monitoring have become widely available. Thus, the possibility of early discharge or outpatient management has become more accessible. Augmenting sPESI with DD levels could aid decision-making regarding the type of treatment. For example, patients classified as low risk could be eligible for shorter hospital stay or at-home treatment, whereas patients estimated as high risk may benefit from more intensive monitoring. Moreover, the notion that a test used for diagnostic workup could be added to established methods of prognostic assessment and consequently improve risk stratification is of interest, as this strategy would not increase costs and could fine-tune picking patients for outpatient treatment, which in turn is more financially appealing than in-hospital management.
Study Limitations
The main limitation of this study is the relatively low number of included patients, low number of SAEs, and its retrospective nature. Moreover, consecutive patients, regardless of the risk of early mortality defined according to the ESC criteria were included, as at our institution in all cases of APE, the concentration of DDs in the plasma is assayed. Thirdly, we used a single criterion for RVD (right to left ventricular end-diastolic diameter ≥0.9) and did not compare this result with the MSCT. The final multivariate model included a number of variables, which were selected based on statistical significance in the univariable analysis and background knowledge of predictors of complicated outcome in APE. However, such a broad approach may lead to model overfitting, especially in this case of a relatively small number of patients who reached the study end point. However, we must underline the exploratory nature of this study. Finally, only 1 type of DD assay was employed in this study.
Conclusion
Plasma DD levels measured during diagnostic evaluation for APE show prognostic value.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.