
Abstract
Background
There is no cumulative evidence supporting the role of coagulation indices in mortality among the critically ill patients with atrial fibrillation (AF).
Methods
The data were derived from the MIMIC-III database, which included a total of 2284 individuals. We explored the association between coagulation indices and mortality using multivariable correction analysis.
Results
2284 participants were included in the study with a median age of 71.29, and 1476 participants were male (64.62%). The median levels of coagulation indices -PTT, PT, INR PT and fibrinogen were 44.14 s, 16.95 s, 1.67 and 277.8 mg/dL, respectively. After adjusting for confounding factors, there were still strong positive correlations between coagulation indices and mortality (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality), (all P < 0.001). In addition, stratified analysis showed that gender as a covariate affected the association between PTT and mortality; age, valvular disease, statins, heparin and aspirin were covariates that affected the association between fibrinogen and mortality
Conclusions
Our study is the first to indicate that there is a positive correlation between coagulation indices (PTT, PT/INR PT, fibrinogen) and mortality in critically ill patients with AF.
Introduction
Many critically ill patients, have preexisting atrial fibrillation (AF), and as a common complication of critical illness, new-onset AF is also common in the intensive care unit (ICU).1,2 The all-cause mortality is significantly increased in AF patients, the common causes of which are heart failure, malignant tumor, infection/septicemia and stroke.3‐5 Based on the increased risk of mortality in patients with AF, further identification of risk factors related to mortality in these patients will help to improve the prognosis.
AF increases the risk of ischemic stroke and systemic circulatory artery embolism, and coagulation disorders play an important role in thrombosis. Prothrombin time (PT), partial thromboplastin time (PTT), international normalized ratio (INR) and fibrinogen are common clinical coagulation indices, that are often used to evaluate changes in coagulation function. PT mainly represents the extrinsic and final common pathways of coagulation function, while PTT mainly represents the intrinsic pathway. 6 Fibrinogen is the main structural component of blood clots. Studies have shown that coagulation disorders caused by severe trauma or infection can lead to organ failure, thus increasing the mortality of patients.7,8 Bayir et al showed that the level of PT was associated with mortality in patients with brain trauma, 9 while another study showed that the PTT value was associated with mortality in patients with severe head injury. 10 A retrospective study of 314 trauma patients analyzed coagulation-related factors from 4 to 24 h after admission, and the results showed that the level of fibrinogen was an independent predictor of death. 11
Current studies have mainly shown that coagulation indices are associated with mortality in patients with infection and trauma, but the relationship between coagulation indices and mortality in critically ill patients with AF remains unclear. Since AF patients are more likely to suffer from coagulation disorders, for example, enhanced platelet aggregation and coagulation, 12 we conducted a retrospective study to explore the potential correlation between coagulation indices and mortality in ICU AF patients.
Materials and Methods
Database Source
The data in the present study were obtained from the MIMIC-III database, 13 a freely available database, that contains information from 46,520 patients admitted to the Beth Israel Deaconess Medical Center (BIDMC) from 2001 to 2012. 13 The MIMIC-III database was approved to be established by the Institutional Review Boards (IRBs) of the Massachusetts Institute of Technology (MIT) and BIDMC. The database includes demographic data, laboratory tests, fluid balance data, vital status and blood gas analysis data, discharge summaries, electrocardiography, imaging examinations, and diagnostic information. Our study included ICU patients diagnosed with AF using the diagnosis codes from the International Classification of Diseases, Ninth Revision (ICD-9). The study was conducted in accordance with the Declaration of Helsinki, which was consistent with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 14
Coagulation Indices and Mortality
The coagulation indices used in this study were from the initial record of patients when entering the ICU. The endpoints of the study were defined as hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality after the date of ICU admission. In detail, hospital mortality was defined as death during hospitalization in the ICU. The 7-day mortality, 30-day mortality, and 1-year mortality were defined based on the time from the discharge date to the date of death.
Confounding Variables
The admission information of each patient from the MIMIC-III was extracted by Structured Query Language. The following confounders were considered, demographic data (age and gender), laboratory results [white blood cell count (WBC), red blood cell count (RBC), platelet count (PLC), hemoglobin, serum creatinine, and blood urea nitrogen], medication records [β receptor blockers (βRBs), statins, nitrates, warfarin, and heparin], and clinical comorbidities [hypertension, chronic heart failure (CHF), valvular disease, chronic kidney disease (CKD), stroke, diabetes, chronic bronchitis, depression, and malignancy].
Statistical Analysis
In this study, all statistical analyses were conducted using SPSS 26.0 and EmpowerStats 3.0. Categorical data were presented as percentages. Continuous data with normal distribution were expressed as mean ± standard deviation (SD), while those with non-normal distribution were reported as median (interquartile range, IQR). Restrictive logistic regression models were then applied to determine whether coagulation indices were independently associated with endpoints (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality) after adjusting for potential confounders. The crude model was fitted without adjustment for any potential confounders. Model 1 was adjusted for age and gender. Model 2 was adjusted for Model 1 plus hypertension, chronic heart failure (CHF) and valvular disease. Model 3 was adjusted for Model 2 plus stroke, diabetes, chronic kidney disease, chronic bronchitis, depression, and malignancy. Furthermore, an interaction analysis was conducted to determine the impacts of belonging in various subgroups, classified by gender, age, hypertension, CHF, valvular disease, and medication (statins, heparin and aspirin).
Results
Characteristics of the Participants
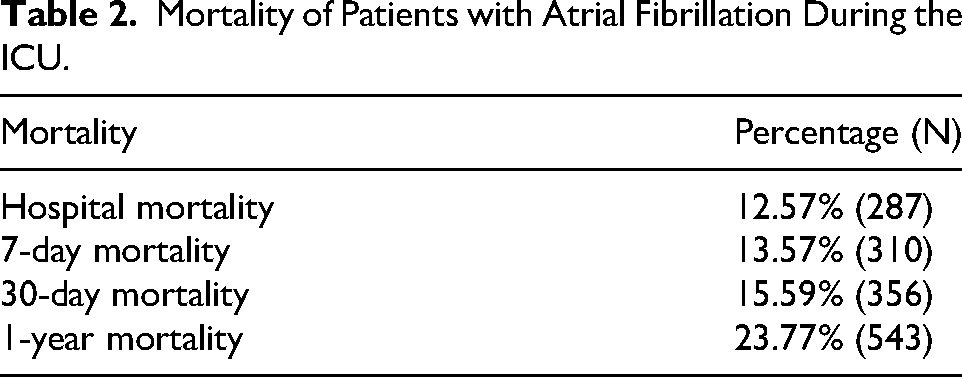
A total of 2284 participants were included in this study, with a median age of 71.29 years and 1476 males (64.62%), and the average time of stay in the ICU was 7.03 days. The median levels of PTT, PT, INR PT and fibrinogen were 44.14 s, 16.95 s, 1.67 and 277.8 mg/dL, respectively. The proportions of in-hospital, 7-day, 30-day, and 1-year mortality were 12.57% (287), 13.57% (310), 15.59% (356) and 23.77% (543), respectively. More information including comorbidity, other blood biomarkers and medication in the ICU is described in detail in Table 1. The mortality of patients with atrial fibrillation during the ICU is described in Table 2.
Clinical Characteristics of Patients with Atrial Fibrillation During the ICU.
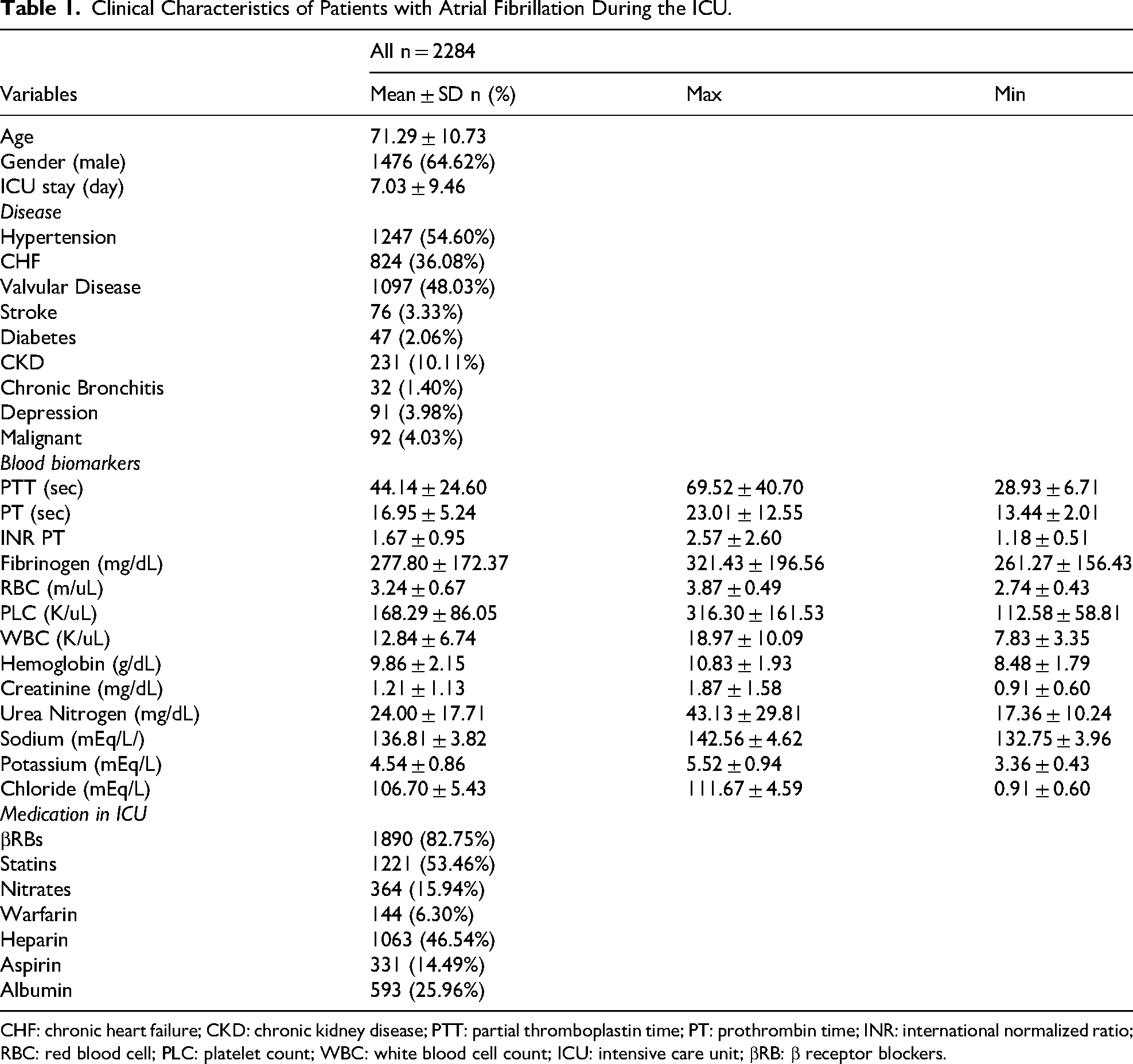
CHF: chronic heart failure; CKD: chronic kidney disease; PTT: partial thromboplastin time; PT: prothrombin time; INR: international normalized ratio; RBC: red blood cell; PLC: platelet count; WBC: white blood cell count; ICU: intensive care unit; βRB: β receptor blockers.
Mortality of Patients with Atrial Fibrillation During the ICU.
Multiple Logistics Analysis for the Relationship Between Coagulation index and Mortality
As shown in Table 3, in the crude model, the results showed that PTT, PT, INR PT and fibrinogen were significantly associated with mortality (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality),respectively (all P < 0.001). After adjusting for confounding factors such as age, gender and diseases (hypertension, CHF, valvular disease, stroke, diabetes, CKD, chronic bronchitis, depression and malignant), there were still strong positive correlations between coagulation indices and mortality (Model 3). Elevated PTT level was associated with increased risks of hospital mortality (PerSD OR = 1.320, 95% CI 1.187–1.467, P < 0.001), 7-day mortality (PerSD OR = 1.338, 95% CI 1.207–1.482, P < 0.001), 30-day mortality (PerSD OR = 1.334, 95% CI, 1.207–1.474, P < 0.001), and 1-year mortality (PerSD OR = 1.317, 95% CI, 1.198–1.488, P < 0.001). Elevated PT level was associated with increased risks of hospital mortality (PerSD OR = 1.321, 95% CI 1.193–1.462, P < 0.001), 7-day mortality (PerSD OR = 1.331, 95% CI 1.202–1.474, P < 0.001), 30-day mortality (PerSD OR = 1.365, 95% CI, 1.228–1.517, P < 0.001), and 1-year mortality (PerSD OR = 1.400, 95% CI, 1.255–1.563, P < 0.001). Elevated INR PT level was associated with increased risks of hospital mortality (PerSD OR = 1.401, 95% CI 1.229–1.598, P < 0.001), 7-day mortality (PerSD OR = 1.409, 95% CI 1.237–1.605, P < 0.001), 30-day mortality (PerSD OR = 1.369, 95% CI, 1.205–1.554, P < 0.001), and 1-year mortality (PerSD OR = 1.419, 95% CI, 1.247–1.614, P < 0.001). Elevated fibrinogen level was associated with increased risks of hospital mortality (PerSD OR = 1.533, 95% CI 1.371–1.713, P < 0.001), 7-day mortality (PerSD OR = 1.539, 95% CI 1.379–1.716, P < 0.001), 30-day mortality (PerSD OR = 1.506, 95% CI, 1.354–1.675, P < 0.001), and 1-year mortality (PerSD OR = 1.580, 95% CI, 1.426–1.751, P < 0.001).
Multiple Logistics Analysis for Relationship Between Coagulation index and Mortality.

Crude Model: No adjustment.
Model 1: Adjusted for age and gender.
Model 2: Adjusted for age, gender and cardiovascular diseases (Hypertension, CHF and Valvular Disease)
Model 3: Adjusted for age, gender and diseases (Hypertension, CHF, Valvular Disease, Stroke, Diabetes, CKD, Chronic Bronchitis, Depression and Malignant).
CHF: chronic heart failure; CKD: chronic kidney disease; PTT: partial thromboplastin time; PT: prothrombin time; INR: international normalized ratio.
Multiple Logistics Analysis for the Relationship Between PTT and Mortality by Stratified Analysis
Gender, age, comorbidity and medication were taken as the stratified variables to further explore the relationship between PTT and mortality, as shown in Table 4. The results showed that gender had a modification effect on the associations between PTT and hospital mortality, 7-day mortality, 30-day mortality and 1-year mortality (all interactions P < 0.05). In male patients, PTT was significantly associated with hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality (all P < 0.001), but in female patients, PTT was only associated with 1-year mortality (P < 0.05). Interestingly, the correlations between PTT and mortality (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality) disappeared in patients taking aspirin (all P > 0.05).
Multiple Logistics Analysis for Relationship Between PTT and Mortality by Stratified Analysis.

Adjusted for age, gender, diseases (Hypertension, CHF, Valvular Disease, Stroke, Diabetes, CKD, Chronic Bronchitis, Depression, Malignant).
P#: interaction P value * < 0.05, ** < 0.001, #>0.05.
CHF: chronic heart failure; CKD: chronic kidney disease; PTT: partial thromboplastin time.
Multiple Logistics Analysis for the Relationship Between PT, INR PT and Mortality by Stratified Analysis
As shown in Supplementary Table 1–2, we found that gender, age, hypertension, chronic heart failure, valvular disease, statins, heparin and aspirin had no modification effects on the associations between PT, INR PT and hospital mortality, 7-day mortality, 30-day mortality and 1-year mortality (all interactions P > 0.05).
Multiple Logistics Analysis for Relationship Between Fibrinogen and Mortality by Stratified Analysis
In Table 5, the results showed that age and valvular disease had modification effects on fibrinogen and hospital mortality, 7-day mortality and 30-day mortality, and chronic heart failure, statins, heparin and aspirin had modification effects on fibrinogen and hospital mortality, 7-day mortality, 30-day mortality and 1-year mortality (all interactions P < 0.05).
Multiple Logistics Analysis for Relationship Between Fibrinogen and Mortality by Stratified Analysis.

Adjusted for age, gender, diseases (Hypertension, CHF, Valvular Disease, Stroke, Diabetes, CKD, Chronic Bronchitis, Depression, Malignant).
P#: interaction P value * <0.05, ** <0.001, # >0.05.
CHF: chronic heart failure; CKD: chronic kidney disease.
Discussion
In this study of 2284 participants, we found positive relationships between PTT, PT/INR PT, fibrinogen and the end points (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality). Gender, age, comorbidity and medication had no modification effects on the associations between PT/INR PT and mortality, while the correlation between fibrinogen and mortality was more easily modified. To the best of our knowledge, we are the first to find these associations between coagulation indices and mortality in critically ill patients with AF.
Patients with AF have a higher risk of stroke and systemic embolic events (SSEs). For general patients with AF, anticoagulants are needed to prevent stroke and SSE, but anticoagulants are associated with a higher risk of bleeding. 15 ICU patients with AF often have more complex conditions, and anticoagulants are used more cautiously. Approximately half of the patients included in this study used heparin, and only approximately 6.30% of patients used warfarin. ICU patients have a higher risk of venous thromboembolism, and when complicated with AF, it aggravates the poor prognosis, so more attention should be given to coagulation indices. Previous studies have shown that PTT, PT/INR PT and fibrinogen are associated with in-hospital mortality, our results show similar correlations, and our study further explored possible modifiers.16‐20
PTT reflects the intrinsic pathway of the coagulation cascade, which is affected by coagulation disorders and defects within the endogenous pathway. 21 It has been found that the mortality rate of trauma patients with prolonged PTT admission is significantly higher than that of patients without prolonged PTT, 16 and emergency patients with prolonged PTT have a higher early mortality rate. 22 In addition, prolonged PTT is an independent risk factor for in-hospital mortality at emergency department admission. 23 The above evidence is consistent with our findings, and our results further suggest that prolonged PTT is associated with an increased risk of long-term mortality. Interestingly, further stratified analysis showed that gender modified the correlations between PTT and the end points (hospital mortality, 7-day mortality and 30-day mortality,). Specifically, in female patients, the positive correlation between PTT and the above mortality rates disappeared. There are few reports about the influence of gender on PTT. A study explored the effects of patients who were firefighters on procoagulant responses and compared these responses between male and female firefighters, and the study found that the PTT of female and male firefighters were decreased by 9.0% and 7.7%, respectively. 24 This suggests that women may have a tendency to have a shorter PTT than men under stress, which may partially explain our results. The underlying reasons need to be further studied.
PT reflects the state of the exogenous coagulation system. To facilitate comparative analyses between different hospitals or laboratories, PT values are often converted to INR PT. 18 Although INR is primarily used to monitor anticoagulation in patients on warfarin therapy, it remains a standardized measure that can reflect coagulation status across broader patient populations, including those not on anticoagulation. In this paper, PT and INR PT show similar positive correlations with the end points (hospital mortality, 7-day mortality, 30-day mortality, and 1-year mortality). Walsh et al observed that there was a strong independent correlation between prolonged PT and increased likelihood of death in the ICU, 18 which is consistent with our findings. Through further stratified analysis, we found no modifiers for the association between PT/INR PT and mortality, suggesting that PT/INR PT may be stable indices for critically ill patients with AF, and prolonged PT/INR PT indicates a higher risk of mortality, which requires more aggressive intervention and treatment.
Fibrinogen is an important part of the coagulation system, participates in thrombosis and is a biomarker of the inflammatory response.25,26 Yuan et al observed that in coronary artery disease patients undergoing PCI, especially those with diabetes or prediabetes, fibrinogen was positively associated with long-term all-cause mortality and cardiac mortality. 27 A report from the NHANES study also showed that fibrinogen could contribute to all-cause and cardiac mortality at follow-up. 28 Our results showed that fibrinogen is associated with an increased risk of mortality during hospitalization and follow-up. Furthermore, we found that the relationship between fibrinogen and mortality was modified by a variety of factors, such as age, previous history of vascular disease, and use of statins, heparin, and aspirin.
For critically ill patients complicated with AF, advanced age is a risk factor for increased mortality, so it is well understood that age is one of the modifier factors. For patients with preexisting vascular disease, this implies a higher risk of cardiovascular and cerebrovascular events, so it is well understood that fibrinogen is associated with a higher risk of mortality in this group of patients. Interestingly, our results show that fibrinogen is associated with a higher risk of mortality in patients treated with statins or aspirin, but is associated with a lower risk of mortality in patients taking heparin. Some previous studies may partly explain these phenomena. Some studies have shown that statins can increase fibrinogen levels. Bordbar et al found that the fibrinogen levels in statin users were higher than those in fibrate/niacin users. 29 Adams et al analyzed 1001 patients who took statins, and after adjusting for cardiovascular risk factors, the fibrinogen levels in statin users were significantly higher than those in nonusers. 30 Another study showed that patients using rosuvastatin had increased fibrinogen levels compared to nonstatin users. 31 These studies suggest that the use of statins may increase fibrinogen levels, thereby exacerbating the effect of fibrinogen on mortality. The effect of aspirin on fibrinogen is not very clear at present, and only in vitro experiments have found that aspirin can promote fibrinogen acetylation.32,33 Therefore, the specific mechanism of the modification effect of aspirin on fibrinogen and mortality that we observed still needs to be further explored. For heparin, a study showed that treatment with low molecular weight heparin (LMWH) combined with amikacin significantly reduced fibrinogen levels in ICU patients with severe pneumonia compared to amikacin alone. 34 Another study found that LMWH treatment can promote fibrinolysis in patients with COVID-19. 35 The above studies suggest that the use of heparin may reduce the level of fibrinogen and, therefore, may explain why fibrinogen is associated with a higher risk of mortality in patients without heparin.
Identifying patients with abnormal coagulation profiles may allow for earlier risk stratification and inform decisions regarding therapeutic intensity, such as anticoagulation management, hemostatic support, or closer hemodynamic monitoring. Future research should aim to validate these findings through large-scale, prospective clinical studies and to determine whether targeted interventions based on coagulation status can improve patient outcomes.
This study has several strengths. First, our study data came from the MIMIC-III database, 13 which provides high-quality data and guarantees the reliability of our conclusions. Second, we adjusted and stratified the relevant medical and treatment histories to further enhance the reliability of the conclusions. Finally, for the first time, we found a positive correlation between coagulation indices and mortality in critically ill patients with AF, providing a basis for the clinical management of these patients.
Our study also has some limitations. First, although the models were carefully adjusted for many potential confounders, regression analysis cannot eliminate unknown or unmeasured variables. The overfitting of regression analysis models may contribute to deviating from the research hypothesis, and it is possible to conservatively underestimate the relationship between coagulation indices and mortality. Second, the MIMIC database lacks detailed information on disease classification and patients’ pathological status, for example, the types of AF. Consequently, it was unable to perform further subgroup analysis. Third, we have no imaging data on the heart structure of the patient, which is also related to the risk of mortality, so we could not adjust for that. Nevertheless, we adjusted the models for as many relevant variables as possible to ensure the reliability of the results.
Conclusions
Our results show that after adjusting for possible confounding factors, there is a positive correlation between coagulation indices (PTT, PT/INR PT, fibrinogen) and mortality in critically ill patients with AF.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251375839 - Supplemental material for The Association between Coagulation Indices and Mortality in Critically Ill Patients with Atrial Fibrillation: A Retrospective Study
Supplemental material, sj-docx-1-cat-10.1177_10760296251375839 for The Association between Coagulation Indices and Mortality in Critically Ill Patients with Atrial Fibrillation: A Retrospective Study by Zixi Huang, Hualong Liu, Fengchuan Huo, Jiaxing Huang, Ying Huang, Jinzhu Hu and Zhenyan Xu in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The author Hualong Liu (certification number: 43151599) for obtaining the original data from the MIMIC-III database and providing it to us for analysis.
Ethical Considerations
The data used in this study has been approved by the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center (BIDMC) Institutional Review Board.
Consent to Participate
All data are from publicly available and anonymous databases and do not require informed consent from patients.
Author Contributions
ZY.X., ZX.H. and JZ.H. contributed to the design of the article, HL.L. obtained the original data, ZX.H. was responsible for data collection and writing, Y.H. and HC.F. participated in the data analysis, JX.H. participated in the writing, and ZY.X. was responsible for the revision of the full text. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China [grant numbers 82360171, 81860070, 82070350, 82460056], Jiangxi Provincial Academic and Technical Leaders Training Program in Major Disciplines [grant number 20232BCJ23028], Jiangxi Province Science Foundation for Distinguished Young Scholar [grant number 20202ACBL216001], and Jiangxi Provincial Main Discipline Academic and Technical Leader Training Program—Leading Talent Project [grant number 20204BCJ22029].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the original data are available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.