
Abstract
Background
Tranexamic acid (TA), a synthetic lysine derivative, is known for its antifibrinolytic effect and potential to reduce bleeding in surgeries like arthroplasty, cardio-aortic procedures, and liver transplantation. This meta-analysis seeks to provide robust clinical evidence on TA's effectiveness in reducing blood loss and transfusion needs during orthotopic liver transplantation.
Methods
The systematic review and meta-analysis included the relevant randomized controlled trials (RCTs) retrieved from PubMed, EMBASE, Web of Science, Cochrane, and SCOPUS databases until August 2024. The meta-analysis was done using (RevMan 5.4.1). PROSPERO ID: CRD42024589151.
Results
Our meta-analysis of seven RCTs with 1875 patients found no significant differences between TA and control groups in total red blood cell units transfused (MD: −3.74 units; 95% CI [−8.49, 1.01]; P = .12), perioperative transfusions (MD: −0.42 units; 95% CI [−3.17, 2.32]; P = .76), or overall blood loss (MD: −167.81 mL; 95% CI [−415.29, 79.67]; P = .18).
For safety outcomes, TA was associated with a higher rate of venous thromboembolism events (RR: 1.71; 95% CI [1.01, 2.87]; P = .05; event rate: 4.89% vs 2.91%), while no significant differences were found in other surgical complications (RR: 1.12; 95% CI [0.92, 1.37]; P = .26).
Conclusion
TA does not reduce blood loss or the need for postoperative transfusions in orthotopic liver transplantation and may raise thrombotic risk. Caution is required to interpret these results due to variations in the study/hospital-specific transfusion protocol details. Larger studies are needed to confirm these findings, and future research should explore the effects of multiple dosing regimens on blood loss and transfusion requirements.
Introduction
Liver resection is the preferred treatment for patients with primary or metastatic liver malignancies. This major abdominal procedure results in 15% to 25% of patients requiring postoperative blood transfusions.1,2 Intraoperative blood loss and transfusion are key risk factors for postoperative mortality, strongly associated with long-term cancer recurrence and reduced survival.2-5 Blood transfusions also increase the risk of transmitting infectious diseases and can elevate postoperative morbidity.6,7
Orthotopic liver transplantation (OLT) poses the highest demands on clinical transfusion services among all solid organ transplants, 8 as it is a complex procedure requiring extensive dissection and suturing of major vascular structures, leading to significant blood loss. 9 In addition to surgical blood loss, liver disease is linked with multiple hemostatic disturbances that contribute to nonsurgical bleeding, including platelet deficiencies, coagulation factor deficits, and increased fibrinolysis. 10 Kang et al reported that 82.5% of OLT patients exhibited hyperfibrinolytic activity in at least one blood sample. 11
Since fibrinolytic activation is a major contributor to bleeding during OLT, antifibrinolytic agents, such as tranexamic acid (TA), may positively impact perioperative bleeding.12-14 TA, a synthetic lysine derivative, has been shown to reduce bleeding in various surgeries, including arthroplasty, cardio-aortic surgery, and liver transplantation, due to its antifibrinolytic properties.15-17
Tranexamic acid directly inhibits plasminogen by occupying its lysine-binding sites, thereby blocking its conversion to plasmin and preventing the subsequent breakdown of fibrin into degradation products. It also exerts a protective effect on platelets.15-17 High doses of TA (40 mg) have demonstrated efficacy in reducing intraoperative blood loss and perioperative transfusion requirements. 18 Lower doses (5 mg) reduced fibrinolysis 19 and blood loss 20 but had no impact on transfusion needs; however, large doses may elevate the risk of thrombosis. 18 Numerous studies indicate that TA administration during liver transplantation and open-heart surgery is associated with an increased risk of thrombosis and thromboembolism. 21
This systematic review and meta-analysis aim to provide robust clinical evidence on using TA to reduce blood loss and transfusion requirements during OLT.
Methodology
Protocol Registration
This systematic review and meta-analysis used the PRISMA statement 22 and the Cochrane Handbook for meta-analyses and systematic reviews. 23 This review has been submitted to PROSPERO and published under CRD42024589151.
Data Sources & Search Strategy
We searched PubMed (MEDLINE), Scopus, Web of Science (WoS), EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) databases until August 25, 2024. Following designing the query, we changed the search terms and keywords according to each database: (“Tranexamic acid” OR “TXA”) AND (“Hepatectomy” OR “Liver resection” OR “Segmentectomy” OR “trisectionectomy” OR “Sectionectomy” OR “lobectomy” OR “Surgery” OR” graft*’ OR “Transplant*” OR “operative”) AND (“liver” OR “Hepatic”)
Eligibility Criteria and Study Selection
We included studies that followed the following Population, Intervention, Comparison, Outcomes and Study criteria: population (patients 18 years of age or older and scheduled to undergo liver resection (open or minimally invasive), intervention (TA), comparison (placebo), and outcomes: our primary outcomes are (red blood cell transfusion 7 days interval before and after surgery, red blood cell units transfused, number of patients receiving perioperative transfusions, postoperative red blood cell units transfused per participant, total intraoperative plus postoperative blood loss). Secondary outcomes were safety outcomes reported during the follow-up period (rate of venous thromboembolism (VTE), surgical complications, and postoperative mortality).
Studies included were randomized clinical trials (RCT). The exclusion criteria for the papers were as follows: The following categories of studies are not regarded as unique: (1) non-human and in vitro experiments; (2) studies with overlapping or duplicate datasets; (3) book chapters, reviews, comments, letters to the editor, and guidelines; and (4) studies not published in English.
Study Selection
The online Covidence tool was used to conduct the review. Once duplicates were removed from the records, two of four (W.S., A.A., AM
Data Extraction
After acquiring the complete texts of the pertinent publications, we carried out a pilot extraction to precisely set up the data extraction sheet. The Excel (Microsoft, USA) structured data extraction sheet comprises three sections. The first section contained a summary of the features of the included studies, including the (study ID, the country, the study design, the inclusion criteria of the RCT, the total population of the RCT, the dose, and duration of the intervention regimen, the primary outcome, the procedure, endpoint, and the follow-up period). In the second section, the participants’ baseline data was presented (age, gender, body mass index, diagnosis, medical history, preoperative coagulation lab values, hospital and intensive care unit stay duration, and procedure duration). The third part included efficacy data. Three reviewers (AM
Risk of Bias and Certainty of Evidence
Using the Cochrane RoB2 method,
24
three reviewers (AM
Statistical Analysis
We used the 5.4.1 version of the Review Manager (RevMan) software. 25 The risk ratio (RR) and mean difference (MD) and their associated 95% confidence interval (CI) were used to evaluate the dichotomous outcomes and continuous outcomes, respectively. We used a random-effects model to handle potential heterogeneity and take into consideration differences in study designs and participant characteristics. The I-squared statistic, which measures the proportion of overall variability in effect estimates across studies attributable to heterogeneity instead of chance, was used to assess heterogeneity. For the I-squared statistic to show significant heterogeneity, we took a significance level of P ≤ .1 into consideration. The between-study variance (tau-squared) in the random-effects model was estimated using the Der Simonian and Laird method. The P-value below .05 indicated statistical significance for the total effect size.
Results
Search Results and Study Selection
Seven hundred thirteen studies were screened and assessed based on their titles and abstracts during the search process. Twenty-four articles moved on to full-text screening once (453) duplicates and (236) irrelevant studies were excluded. Finally, we included seven RCTs18-20,26-29 (Figure 1).

PRISMA Flow Chart of the Screening Process.
Characteristics of Included Studies
Seven RCTs with 1875 patients were analyzed and conducted across seven countries: India, Canada, Spain, North America, the USA, Taiwan, and the UK. The studies exclusively investigated the use of TA among adult patients undergoing liver resection. The included participants’ comorbidities, baseline characteristics, and details of the RCTs are listed in (Tables 1 and 2).
Summary Characteristics of the Included RCTs.

Abbreviations: RCT, randomized controlled trial; TA, tranexamic acid; TEG, thromboelastography; CLI, clot lysis index; FDP, fibrin degradation products; RBC, red blood cells; FFP, fresh frozen plasma; OLT, orthotopic liver transplantation; ESLD, end-stage liver disease; ICU, intensive care unit; ITU, intensive therapy unit; AP, antiplatelet.
Transfusion and Protamine Administration Guidelines are shown in the supplementary file.
Where mortality was reported.
Baseline Characteristics of the Participants.

Abbreviations: TA, tranexamic acid; NA, not available; SD, standard deviation; BMI, body mass index; ICU, intensive care unit; Hb, hemoglobin.
Risk of Bias
Four studies demonstrated a low risk of bias. At the same time, three raised some concerns, particularly regarding the randomization process, bias due to deviations from intended interventions, or bias in selecting reported results (Figure 2).

Quality Assessment of Risk of Bias in the Included Trials. A Schematic Representation of Risks (Low = Red, Unclear = Yellow, and High = Red) for Specific Types of Biases of Each of the Studies in the Review.
Primary Outcomes
TA was associated with a significant increase in postoperative red blood cell units transfused (MD: 0.34 units; 95% CI [0.25, 0.42]; I² = 0%; P < .00001) (Figure 3A). However, no significant difference was observed between the TA and control groups in overall red blood cell units transfused (MD: −3.74 units; 95% CI [−8.49, 1.01]; I² = 35%; P = .12) (Figure 3B), perioperative units transfused (MD: −0.42 units; 95% CI [−3.17, 2.32]; I² = 57%; P = .76) (Figure 3C), number of patients receiving perioperative transfusions (MD: 0.81 patients; 95% CI [0.50, 1.31]; I² = 81%; P = .39) (Figure 4A), postoperative transfusions (MD: 0.23 units; 95% CI [0.00, 15.13]; I² = 89%; P = .49) (Figure 4B), or total intraoperative plus postoperative blood loss (MD: −167.81 mL; 95% CI [−415.29, 79.67]; I² = 86%; P = .18) (Figure 4C).

Forest Plot of the Primary Outcomes (A. Postoperative Red Blood Cell Units Transfused, B. Overall Red Blood Cell Units Transfused, C. Perioperative Units Transfused).
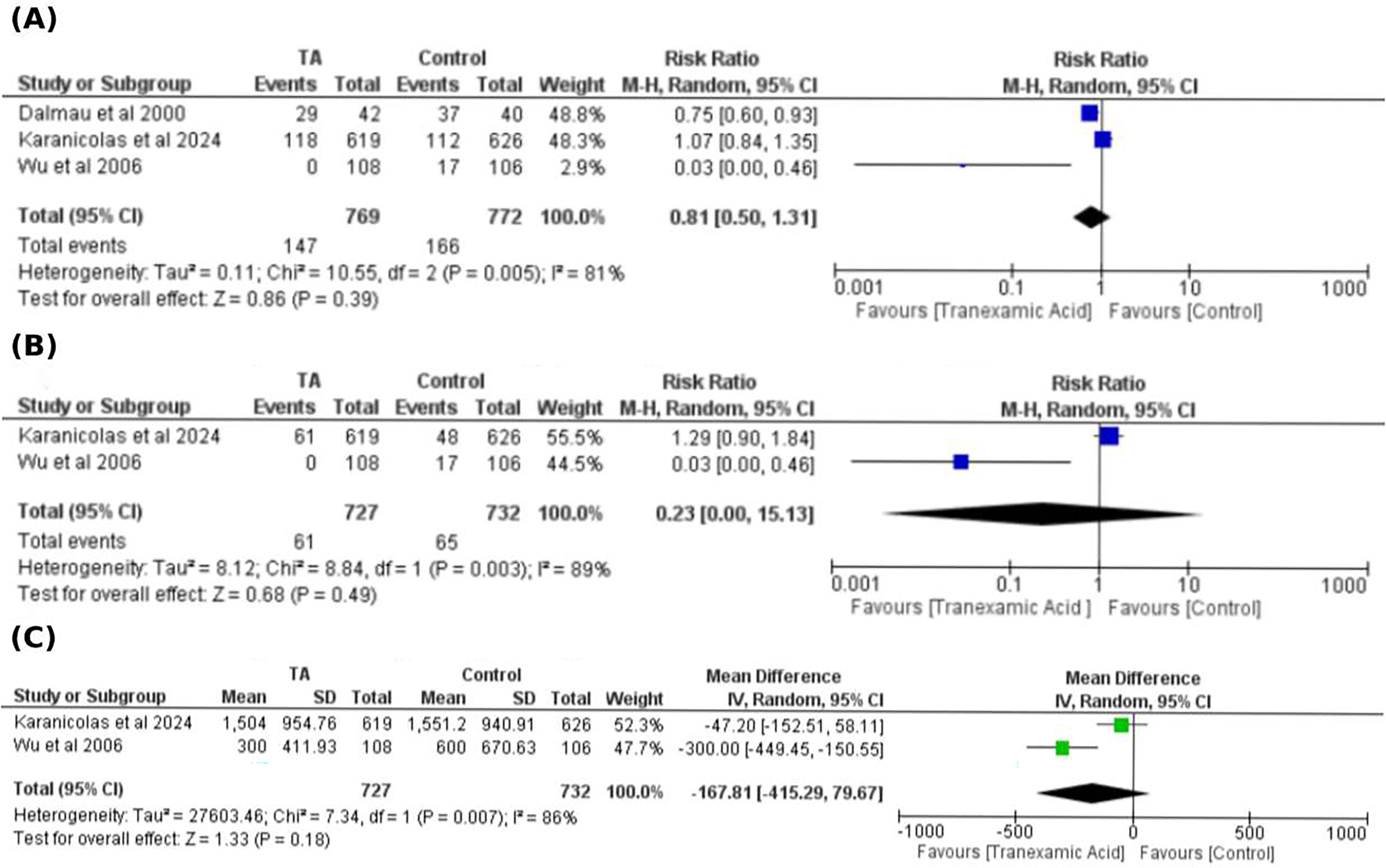
Forest Plot of the Primary Outcomes (A. Number of Patients Receiving Perioperative Transfusions, B. Postoperative Transfusions, C. Total Intraoperative Plus Postoperative Blood Loss).
The results were homogeneous for postoperative red blood cell units per participant (P = .58; I² = 0%) and overall transfusion units (P = .22; I² = 35%). In contrast, perioperative red blood cell units transfused showed moderate heterogeneity (P = .10; I² = 57%); excluding Dalmau et al (2000) 27 resolved this heterogeneity without altering the overall findings (Table 3). Patients receiving perioperative transfusions exhibited high heterogeneity (P = .005; I² = 81%), which persisted despite sensitivity analyses (Table 3). Finally, postoperative transfusions (P = .003; I² = 89%) and total intraoperative plus postoperative blood loss (P = .007; I² = 86%) demonstrated substantial heterogeneity; sensitivity analyses were not feasible due to the limited number of studies.
Sensitivity Analysis for Red Blood Cell Units Transfused and Number of Patients Receiving Perioperative Transfusions.

Abbreviations: TA, tranexamic acid; MD, mean difference; RR, risk ratio; CI, confidence interval; df, degree of freedom.
Safety Outcomes
TA significantly increased VTE (RR: 1.71; 95% CI [1.01, 2.87]; I² = 0%; P = .04), with event rates of 4.89% for TA versus 2.91% for control (Figure 5A). No difference was observed between TA and control groups in surgical complications (RR: 1.12; 95% CI [0.92, 1.37]; I² = 10%; P = .26; event rates: 39.22% vs 34.64%) (Figure 5B) or postoperative mortality (RR: 0.98; 95% CI [0.56, 1.72]; I² = 4%; P = .95; event rates: 2.72% vs 2.72%) (Figure 5C).

Forest Plot of the Safety Outcome (A. Rate of Venous Thromboembolism, B. Surgical Complications. C. Postoperative Mortality).
Results were homogeneous for any adverse events (P = .58; I² = 0%), VTE (P = .92; I² = 0%), surgical complications (P = .29; I² = 10%), and postoperative mortality (P = .37; I² = 4%).
Discussion
We conducted this systematic review and meta-analysis to compare the efficacy and safety of TA versus placebo during and after OLT. Our findings indicate that TA was associated with a significant increase in postoperative red blood cell transfusion requirements and a higher rate of VTE. However, the apparent rise in postoperative transfusions was driven mainly by a single large trial, representing a potential source of bias that should be explicitly acknowledged. Also, there was no difference between the TA and the control groups regarding the overall total number of red blood cell units transfused, number of perioperative red blood cell units transfused, the number of patients who receive perioperative red blood cell transfusion, total intraoperative plus postoperative blood loss, any surgical complications and the rate of postoperative mortality.
Liver transplant has become the most effective treatment for end-stage chronic liver disease, with one-year survival rates ranging from 80% to 90%. 14 Control of hemorrhage is a significant concern of liver resection. Many factors can induce hemorrhage during OLT, including liver mobilization and dissection of tumors with the surrounding organs.30,31
The hyperfibrinolytic activity begins immediately after hepatectomy and becomes the most predominant on the first day postoperatively. The effect gradually starts decreasing from the third postoperative day and returns to the baseline level on postoperative day 7.32,33 Many strategies, materials, and devices have been suggested to reduce the requirements of blood during liver resection, such as preoperative self-blood donation with or without the use of erythropoietin,4,34 intraoperative hemodilution before liver transection 35 and restrictive blood transfusion policy.30,36 However, these strategies and devices have pros and cons. These strategies are either complex and challenging to perform or require high costs. Moreover, some techniques, such as parenchymal compression, are challenging for centrally located tumors.31,36
TA is a direct plasminogen inhibitor. It prevents the plasmin-mediated conversion of fibrinogen to fibrinogen split products.11,16,17 It was found by Wu et al 2006; that the amount of operative blood loss was significantly decreased with the use of TA. 29 It was also found by Dalmau et al that prophylaxis with TA was associated with some improvement in fibrinolysis, significant intraoperative decreases in RBC (red blood cells) use, and a greater number of patients without any RBC transfusion. However, they found no difference in transfusion requirement during the first 24 h postoperatively. 27
In Kaspar et al, 19 a small dose of TA (2 mg) inhibited fibrinolysis but did not show any positive effects on blood transfusion. This indicates that a small dose of TA has no clinical advantage. Kang et al 37 also found that a dose of 250–500 mg of TA effectively treats severe fibrinolysis, with a second dose needed in the most serious cases during OLT.
These findings align with recent trials in traumatic brain injury, 38 cardiac surgery, 39 and, most recently (POISE-3), a range of non-cardiac surgeries. 40 In these large studies, TA significantly reduced bleeding, the need for blood transfusions, and disability resulting from bleeding.
On the other hand, in a recent trial by Karanicolas et al 2024 involving 1245 patients, there was no difference between TA and placebo groups regarding the overall total number of red blood cell units transfused and total intraoperative plus postoperative blood loss. 28 These results are in concordance with the results of our analysis, which found no difference between TA and placebo regarding the total number of red blood cell units transfused and total intraoperative plus postoperative blood loss. Our results are also confirmed by another recent trial that used prophylactic TA to prevent obstetrical hemorrhage after cesarean delivery. This trial found that administration of TA did not lower the risk of maternal death or blood transfusion (RR = 0.89 [95% CI, 0.74-1.07]). 41 A large recent meta-analysis 42 also confirmed that TA was effective in reducing total blood loss for a cesarean birth (MD = −2.11 mL, 95%CI [−3.09 to −1.14], P < .001).
The differing results between OLT and procedures like neurosurgery or cardiac surgery likely reflect the source of bleeding: in liver resections, hemorrhage typically originates from large-caliber vessels, whereas in soft-tissue, bone, pericardial or brain operations the blood loss is more often a diffuse “ooze.” Thus, while tranexamic acid may curb microvascular or general oozing, it may be far less effective when true arterial or venous vessel bleeding is the primary issue. 28
Our analysis showed that thromboembolic events were higher in the TA group. The VTE rate in individual studies was similar between TA and placebo groups.19,27-29 Multiple reports of intravascular thrombus formation were associated with surgical procedures in which antifibrinolytic drugs were used.43-45 Therefore, using small doses of antifibrinolytics may have an advantage over high doses in preventing such lethal complications.
In a systematic review including 197 trials comparing systemic TA with placebo or no study intervention, the risk of any adverse event (RR = 1.05, [95%CI,0.99-1.12]) and VTE (RR = 0.95 [95%CI,0.78-1.15]) were similar in cardiac surgery patients. 46
It should be noted that advanced cancer, a major risk factor for VTE, increases the baseline risk of VTE, so the increased risk of VTE with TA use is augmented. 47 Boylan et al 18 did not report any thrombosis incidence in their study; this may be due to heparin administered 4 h after completion of the hepatic arterial anastomosis or due to small sample size, but it raises the probability that heparin use may be beneficial to decrease the incidence of VTE if TA is used during or after surgical procedures.
Lastly, it is important to highlight various methodologies of administration of TA in the studies included. Early investigations often used a bolus followed by a continuous infusion. For instance, Yassen et al (1993) 20 administered a 10 mg/kg loading dose at the start of the anhepatic phase, followed by 3 mg/kg/hr until ITU transfer. Boylan et al (1996) 18 employed a continuous infusion of 40 mg/kg/hr (up to a maximum total dose of 20 g). Other studies, such as Dalmau et al (2000) 27 and Kaspar et al (1997), 19 also used continuous infusion protocols, with rates ranging from 2 mg/kg/hr to 10 mg/kg/hr. Allanki et al (2008) 26 explored two distinct regimens within the same trial: one group received repeated bolus doses (10 mg/kg every 6-8 h), while another received a bolus (10 mg/kg) followed by a continuous infusion (5 mg/kg/hr) until early reperfusion. Wu et al (2006) 29 administered a 500 mg bolus just before surgery, then 250 mg every six hours for three days. More recently, Karanicolas et al (2024) 28 used a standardized approach consisting of a 1 g bolus in 10 mL normal saline, followed by a maintenance infusion of 1 g in 250 mL normal saline. Due to these variations, we did not perform a sub-group analysis based on the dose.
It is worth noting that previous meta-analyses on TA in various patient populations have reported favorable outcomes. For example, a large meta-analysis by Al-dardery et al 42 involving 18,649 patients found that TA reduced total blood loss and the incidence of postpartum hemorrhage in women undergoing cesarean or vaginal births, although the dosages used in the 59 RCTs were not specified. In cardiac surgeries, Guo et al 48 evaluated different dosing regimens and administration methods of TA and found that perioperative blood loss and reoperation rates were significantly reduced without affecting mortality, myocardial infarction, stroke, pulmonary embolism, or renal dysfunction. Interestingly, they also reported that TA was effective in both on-pump and off-pump surgeries. While topical application did not reduce the need for transfusions, intravenous administration—whether as a bolus injection alone or as a bolus followed by continuous infusion—was effective. Additionally, high-dose intravenous TA did not further decrease the transfusion rate compared to a low-dose regimen but did increase the risk of seizures by 4.8 times, with no seizures observed in the low-dose group. 48 These findings highlight the ongoing efforts to optimize TA administration protocols for improved efficacy and safety.
Strength and Limitations
Although this systematic review and meta-analysis showed the beneficial use of TA during and after OLT to reduce blood loss and the need for transfusion, it is not without limitations. First, the analysis combines a small number of studies with limited participant numbers, potentially affecting the robustness of the findings. Therefore, the high statistical significance for some outcomes, such as the number of postoperative red blood cell units transfused, was driven by a single study for which the transfusion protocol, even if reported in Table S1, may not be fully understood or known.
Second, the studies included used different doses, limiting the generalizability of the results, as higher doses might have yielded more beneficial effects. Moreover, our analysis did not differentiate between autologous blood transfusions, which are typically reinfused routinely, and allogenic transfusions, which are mainly employed when excessive blood loss occurs. Variations in transfusion protocols across studies or hospitals could have influenced the outcome data, particularly when one large study disproportionately drives the overall meta-analysis results. Third, some concerns of quality were found in three out of four studies included, mainly in the randomization process, in addition to the heterogeneity observed in some outcomes such as preoperative units transfused, number of patients receiving preoperative/postoperative transfusions, and total intraoperative plus postoperative blood loss.
Future research should standardize transfusion protocols to better isolate and understand the impact of these different strategies.
Conclusion
In conclusion, TA does not reduce blood loss or the need for postoperative blood transfusions during OLT and may increase the risk of thrombotic complications. Due to variations in the study/hospital-specific transfusion protocol details and other limitations highlighted, results should be interpreted cautiously and used alongside other forms of evidence to make informed decisions. Further studies with larger sample sizes are needed to confirm these findings. Future research should consider using multiple dosing regimens to determine if higher doses could positively impact blood loss and transfusion requirements.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251342467 - Supplemental material for Tranexamic Acid in Patients Undergoing Liver Resection: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-cat-10.1177_10760296251342467 for Tranexamic Acid in Patients Undergoing Liver Resection: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials by Mohammad Tanashat, Basma Badrawy Khalefa, AlMothana Manasrah, Husam Abu Suilik, Mohamed Abouzid, Wafaa Shehada, Ahmed Almasry, Ibrar Atiq and Mohamed Abuelazm in Clinical and Applied Thrombosis/Hemostasis
Footnotes
ORCID iDs
Author Contributions
(M.T.) conceived the idea. (M.T. and M.A.azm) designed the research workflow. (M.T. and M.A.azm) searched the databases. (W.S., A.A., and AM
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.