
Abstract
Clopidogrel is usually discontinued 5–7 days before elective surgery to reduce the risk of bleeding. However, the perioperative safety of patients receiving low-molecular-weight heparin (LMWH) bridging therapy or continuing clopidogrel therapy remains unknown. We identified patients who received clopidogrel for cardiovascular diseases and underwent elective surgery at a large central hospital in China between June 2022 and January 2024. The primary endpoints were perioperative blood transfusion events and bleeding-related reoperations. A total of 62 patients who received clopidogrel and underwent abdominal surgery were included in this study. Based on the preoperative clopidogrel therapy strategy, patients were categorised into three groups: the LMWH bridging group (clopidogrel withdrawal followed by LMWH bridging therapy for 5-7 days; n = 22), the no-bridging group (clopidogrel withdrawal for 5-7 days; n = 26), and the continued group (clopidogrel therapy maintained; n = 24). Perioperative blood transfusion rates were higher in the LMWH bridging and continued groups. However, there was not a significant distinction (P = .197). Additionally, hospital stay length, bleeding-related reoperation, and 3-month mortality were similar across the groups (P > .05). No patients experienced myocardial infarction or stroke within 3 months post-procedure. Patients who received preoperative LMWH bridging therapy or continued clopidogrel therapy had a slightly higher risk of perioperative bleeding. These findings need to be confirmed by further randomised controlled trials.
Keywords
Introduction
The prevention of perioperative bleeding and thromboembolic events, especially in patients taking antithrombotic drugs before surgery, continues to present a challenge to clinicians. 1 Clopidogrel can be used for acute coronary syndrome after percutaneous coronary intervention as well as intracranial stent implantation and is among the most commonly used antiplatelet drugs in clinical practice.2,3 Although current guidelines recommend discontinuing clopidogrel 5–7 days before surgery, 4 there is no firm evidence supporting the benefits of this regimen for patients undergoing non-cardiac surgery. The guideline-recommended time windows are based on drug pharmacokinetics, and whether discontinuing clopidogrel in patients with hypercoagulability raises the chance of thrombotic events is still unknown.
The use of low-molecular-weight heparin (LMWH) as a bridging agent is supported by guidelines for patients on long-term vitamin K antagonists (eg, warfarin) who require temporary interruption of anticoagulation for surgery or invasive procedures. However, its role in the context of antiplatelet therapy, such as with clopidogrel, remains controversial.5,6 This controversy arises primarily from the distinct mechanisms of action of these agents. LMWH exerts its anticoagulant effect by inhibiting factor Xa and thrombin, whereas clopidogrel is an antiplatelet agent that blocks the P2Y12 receptor on platelets, thereby preventing platelet aggregation. The lack of mechanistic overlap raises concerns about the efficacy and safety of substituting one for the other. Despite these concerns, there may be specific clinical scenarios where LMWH bridging could be considered in patients on antiplatelet therapy. For example, in patients with recent coronary stent implantation or acute coronary syndrome who require urgent non-cardiac surgery, the perioperative management of antiplatelet therapy is particularly challenging. Discontinuing clopidogrel in these high-risk patients may increase the risk of stent thrombosis or other ischemic events, whereas continuing it may elevate the risk of surgical bleeding. In such cases, LMWH bridging may be explored as a potential alternative, though careful consideration of the risks and benefits is essential.
Current guidelines generally recommend against the use of LMWH as a bridging agent in the context of antiplatelet therapy, emphasising the importance of individualised risk assessment and multidisciplinary decision-making. 5 However, the evidence supporting these recommendations remains limited, highlighting the need for further research to clarify the role of LMWH bridging in specific high-risk populations. Therefore, in this study, we compared the perioperative bleeding risk of patients undergoing abdominal surgery with LMWH bridging therapy, clopidogrel discontinuation for 5–7 days, and continuation of clopidogrel and analysed their perioperative outcomes.
Methods
Patient Classification
We included patients who underwent abdominal surgery at a large central hospital in China between June 2022 and January 2024. All patients received long-term antiplatelet therapy with clopidogrel before surgery, and general anaesthesia was administered to all patients. The mean duration of clopidogrel therapy before surgery was 30 months (range: 6-95 months). Among the study cohort, 26% of patients were on dual antiplatelet therapy (DAPT), combining clopidogrel with aspirin, whereas the remaining 74% received clopidogrel monotherapy. The decision to use DAPT or monotherapy was based on the underlying clinical condition and relevant guidelines at the time of treatment initiation. The exclusion criteria were intracranial, intraspinal, and intraocular surgery, use of other anticoagulant drugs, and severe blood diseases.
Based on the preoperative clopidogrel therapy strategy, patients were categorised into three groups: the LMWH bridging group (clopidogrel withdrawal followed by LMWH bridging therapy for 5–7 days), the no-bridging group (clopidogrel withdrawal for 5–7 days), and the continued group (clopidogrel therapy maintained). Group assignment was determined by the clinical judgment of the treating physician, considering factors such as bleeding risk, thrombotic risk, and surgical urgency. This study was designed as a pilot investigation. Given the exploratory nature of this research and the lack of prior data on this specific population, a formal sample size calculation was not initially performed. However, based on similar studies in the literature and practical considerations, we aimed to enrol a minimum of 20 patients per group to ensure a reasonable distribution of baseline characteristics and facilitate preliminary comparisons.
The hospital ethics committee gave its approval for this study. Every participant in the study signed an informed consent form after being fully educated about the trial's procedures. The Chinese Clinical Trial Registry website has this trial recorded (ChiCTR1900028558).
Data Collection and Perioperative Management of Patients
Data on patient age, gender, body mass index (BMI), American Society of Anaesthesiologists (ASA) classification score, concomitant diseases, and smoking history were collected. Preoperative examinations included haemoglobin (Hb) level, platelet count (PLT) and other laboratory data. In addition, thromboelastography (TEG) was completed 1 h before the patient received anaesthesia. The TEG indicators included K, R, alpha angle, and MA. Finally, the length of hospital stay, perioperative blood transfusion events, and bleeding-related reoperations were recorded. Adverse events, including mortality, venous thromboembolism (VTE), myocardial infarction, and stroke within 3 months postoperatively, were documented during follow-up.
Patients treated with LMWH bridging therapy were subcutaneously administered LMWH after discontinuation of clopidogrel 5–7 days before surgery and 12 h before surgery. The LMWH dose was 100 IU/kg twice daily, initiated 48 h before surgery and resumed 24 h postoperatively. Preoperative renal function was assessed, and LMWH doses were adjusted for patients with impaired renal function. If there were no major bleeding complications, all patients resumed oral antiplatelet therapy within 24 h after surgery. Indications for perioperative transfusion were determined by consensus between the anaesthesiologists and surgeons based on perioperative Hb levels and intraoperative vital signs. At our institution, the transfusion threshold was an Hb level below 8 g/dL.
Statistical Analysis
The Shapiro-Wilk test was used to check for normality in the statistical analysis, which was conducted using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). The mean ± standard deviation (
Results
Patient Characteristics and Surgical Procedures
According to the inclusion criteria, 62 patients were enrolled in this study, with 26, 22, and 14 patients assigned to the LMWH bridging, no-bridging, and continued groups, respectively. Among the enrolled patients, the average age was 62.52 years, with the oldest being over 80 years old. No significant differences in age, sex ratio, ASA classification, BMI, concomitant diseases, or smoking history were observed between the three groups (P > .05; Table 1). The types and numbers of procedures performed in the three groups are shown in Table 2.
Patient Demographics. [n (%),

Abbreviations: ASA, American Society of Anaesthesiologists Physical Status Classification; BMI, body mass index.
List of Surgical Procedures by Group.

Preoperative Examinations and TEG Parameters
Upon comparing the preoperative Hb, PLT, traditional coagulation indices, and TEG indices between the three groups, no significant differences in Hb, PLT, PT, INR, or DD were observed (P > .05). However, the APTT and MA of the three groups differed significantly (P = .032; P = .042; Table 3).
Comparison of Preoperative Examinations and TEG Parameters Among the Three Groups. [M (Q1, Q3),

Abbreviations: TEG, thromboelastography; Hb, haemoglobin; PLT, platelet count; APTT, activated partial thromboplastin time; PT, prothrombin time; DD, D-dimer; FIB, fibrinogen; INR, International standardised ratio.
Perioperative Outcomes
Compared with patients in the no-bridging group, those in the LMWH bridging and continued groups had a higher incidence of perioperative blood transfusion; however, the difference was not statistically significant (P = 0.197). In addition, no significant differences were found in the length of hospital stay, reoperation, or mortality among the three groups (P > .05). During the 3-month follow-up, no patients experienced myocardial infarction, stroke, or VTE. The results for all perioperative periods are presented in Table 4.
Three-Month Perioperative Outcomes. [n (%), M (Q1, Q3)].
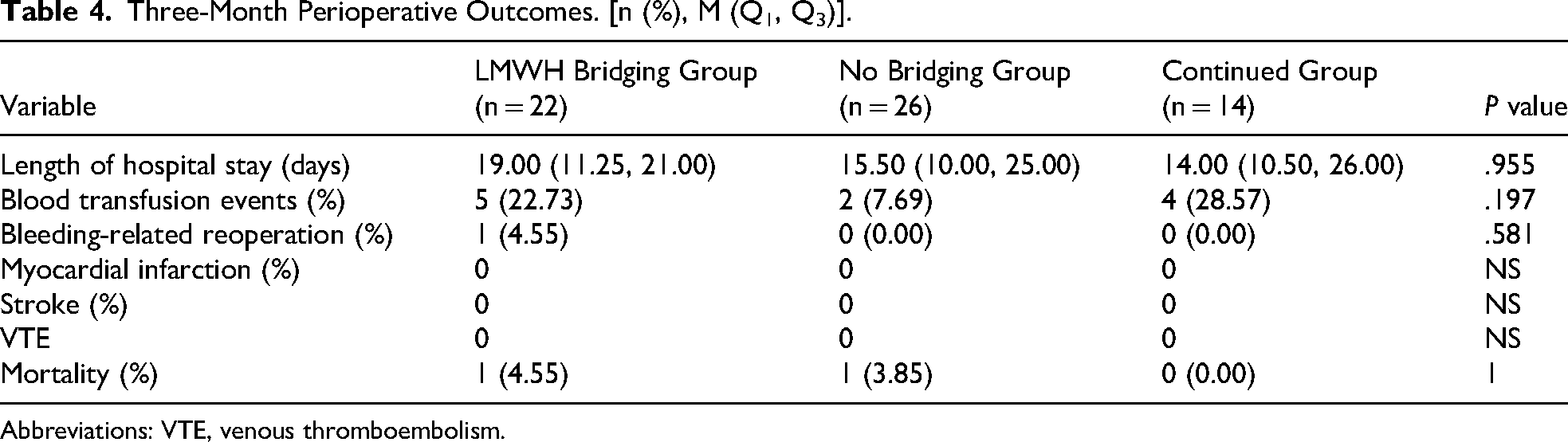
Abbreviations: VTE, venous thromboembolism.
Discussion
In this study, we tested the hypothesis that LMWH bridging therapy or uninterrupted clopidogrel therapy raises the possibility of perioperative bleeding among patients experiencing abdominal surgical procedures. Our findings did not show that LMWH bridging therapy or continued clopidogrel treatment significantly raises the possibility of perioperative bleeding among patients experiencing abdominal surgical procedures. We assessed the risk of perioperative bleeding in three groups: continuation of clopidogrel, discontinuation of clopidogrel, and LMWH bridging therapy. As far as we know, this is the first study that investigates three clopidogrel discontinuation strategies before abdominal surgery.
In the current research, we discovered that among the 62 patients undergoing abdominal surgery, those who received LMWH bridging therapy or continued clopidogrel had a higher incidence of perioperative transfusion events than those who discontinued clopidogrel preoperatively; however, this difference was not statistically significant. Although previous studies compared patients who did not receive clopidogrel,7,8 patients in the control group did not continue to receive clopidogrel after surgery, and delayed bleeding and embolic events usually occurred in the postoperative period. In addition, we found statistically significant variations in APTT in each group. In comparison to the other two groups, we found statistically substantial modifications in the bridging therapy group, which may be related to changes in heparin treatment after admission. We also found a significant difference in preoperative MA among the TEG indicators in the three groups. The MA in the TEG index is affected by platelet function, 9 suggesting that the continuous use of antiplatelet drugs during the perioperative period affects platelet function, and the discontinuation of clopidogrel before surgery can restore platelet function. Based on our data, this degree of platelet function restoration did not lead to a catastrophic thromboembolic event.
Clopidogrel is an effective antiplatelet drug for treating cardiovascular and cerebrovascular diseases, which is essential for treating acute myocardial infarction and preventing cerebral thrombosis.10–12 Currently, the perioperative benefits and risks of direct discontinuation of clopidogrel or heparin bridging therapy before surgery in patients undergoing overtime clopidogrel treatment remain unclear. In a randomised controlled trial involving 43 general surgery procedures, clopidogrel was not linked to a significant risk of perioperative bleeding during elective general surgery. 13 According to a retrospective analysis of 104 patients experiencing abdominal procedures, the majority of bleeding events were effectively managed by blood transfusions, despite the fact that using clopidogrel within 7 days of surgery raised the risk of postoperative bleeding. 14 Despite their relatively small sample size, the findings of these studies strongly suggest that preoperative continuation of clopidogrel is unlikely to increase the risk of perioperative bleeding in general surgery.
In addition, whether patients treated with clopidogrel require heparin-bridging therapy before surgery remains unclear. Although bridging therapy with LMWH can reduce thromboembolic events and benefit patients, 15 recent studies reported that bridging anticoagulation strategies increase the risk of bleeding without a clear benefit in reducing thromboembolism.16–18 Patients in our study did not report myocardial infarction or cerebrovascular events. Nonetheless, research indicates that asymptomatic periprocedural myocardial infarction may occur in as many as 50% of patients. 19 Considering the occurrence of major perioperative adverse cardiovascular events with clopidogrel discontinuation, we believe it is best to avoid stopping clopidogrel for general surgical treatments with little chance of blood loss, especially during the critical period after coronary intervention. For patients at high risk for embolism, even if antiplatelet drugs are discontinued during the perioperative period, bridging therapy is still recommended.20,21
Our study has some limitations. All patients were from a single centre, and the sample size was small. To further validate our findings, future studies should include a larger sample size. In addition, despite preoperative platelet function analysis using TEG, dynamic testing and analysis of intraoperative and postoperative platelet functions were not performed to identify patients at a higher chance of bleeding. Clopidogrel, an ADP-receptor antagonist, also has a relatively long half-life. 22 Surgical treatment results in significant trauma, intense stress, and rapid changes in coagulation function. In addition, there are differences in primary diseases, CYP2C19 gene polymorphisms, liver and kidney function, and other factors that directly lead to differences in the efficacy of different patients receiving conventional doses of clopidogrel.23,24 Thus, as perioperative coagulation monitoring and platelet function tests become more accurate and readily available, the importance of these tests in our patient group will grow, helping reduce the likelihood of bleeding and thrombotic complications in high-risk patients. 25 Individualised guidance based on precise monitoring provides the optimal time to discontinue clopidogrel therapy.
Conclusion
Our findings suggested that patients who underwent abdominal surgery and received preoperative LMWH bridging therapy or continued clopidogrel therapy had a slightly higher risk of perioperative bleeding. However, this difference was not statistically significant. Our study provides evidence for a strategy for clopidogrel discontinuation before abdominal surgery. These findings need to be confirmed by further randomised controlled trials.
Footnotes
Author Contributions
Bangsheng Hu: Writing – review & editing, Formal analysis. Junsheng Chen: Writing – original draft, Data curation. Shuai Han: Formal analysis, Data curation. Zeping Dai: Supervision, Project administration. Ju Gao: Methodology, Funding acquisition.
Consent to Participate
All participants included in the study were informed about the whole trial process and signed informed consent.
Consent for Publication
Written informed consent was obtained from all participants enrolled in this study. All data were anonymized, and no personally identifiable information is included in the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the hospital ethics committee (ChiECRCT20190238).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This work was funded by Natural Science Foundation of China (82172190); Research Foundation of Science and Technology Bureau of Anhui Province (201904a07020026); The Young and Middle-aged Research Foundation of Wannan Medical College (WK2023ZQN48).