
Abstract
In the United States, the Food and Drug Administration (FDA) has allowed makers of biologic therapies to use the abbreviated new drug application, which does not require safety and efficacy studies. Instead this relies on proving equivalency with the original compound and demonstrating in vitro activity and similar pharmacodynamics. In the United States, a low-molecular-weight heparin, enoxaparin, was recently approved in a generic format through the abbreviated new drug application. We present a patient treated with branded enoxaparin for 4 years with no complications. After the switch to the generic enoxaparin, the patient developed 2 life-threatening hemorrhages within 4 months of the initiation of the compound. This case suggests that the FDA should follow the European Medicine Administration (EMA) guidance by tightening its approval process for generic bioequivalents and requiring studies demonstrating similar safety and efficacy as the parent compound, prior to approval of a generic biologically active compound.
Case
A 63-year-old female with stage IV colon cancer with metastases to the lungs and liver was initially referred to our university system’s oncology clinic in early 2007. At that time, she was found to have bilateral pulmonary emboli (PE) in addition to a history of a deep venous thrombosis (DVT). She was placed on therapeutic enoxaparin (Lovenox[R], Sanofi-Aventis, Paris, FR). She also had an inferior vena cava filter placed in preparation for a surgical procedure. Multiple studies demonstrated resolution prior to an incidental new PE on a routine restaging scan in April 2009. This was managed by her local practitioner, and she was continued on her therapeutic-dosed enoxaparin.
Enoxaparin became generic and interchangeable in July 2010. In October 2010, she was admitted for a large, left breast hematoma without any evidence of preceding trauma. Her hemoglobin was found to be 8.4 g/dL from 11.3 g/dL from the previous month. Her international standardized ratio (INR) was 1.2 and her partial thromboplastin time (PTT) was 42. She had a large ecchymosis on her left breast and an underlying large hematoma with ultrasonographic dimensions of 13.5 × 5.4 × 9.4 cm. She was hospitalized and after discharge she was restarted on her enoxaparin injections, given her high risk for thrombosis. In early November, she developed left side foot drop, paresthesias, and vaginal bleeding. Her hemoglobin had dropped to 6.4 g/dL from 10.7 g/dL 2 days previously. Her coagulation parameters were not significantly changed, and her platelets were within the normal range. A computed tomography (CT) scan of the lower extremity revealed hematomas in the following locations with maximum dimensions: gluteus medius—14 × 6.5 cm; quadratus femoris—4.5 × 3.1 cm; adductor magnus—6.5 × 9.5 cm; hamstring compartment—10 × 5 cm (Figure 1). Several days after stopping anticoagulation and aggressively transfusing the patient, the patient’s respiratory status deteriorated and she became unstable, chose comfort care, and passed. An autopsy was declined by the family.
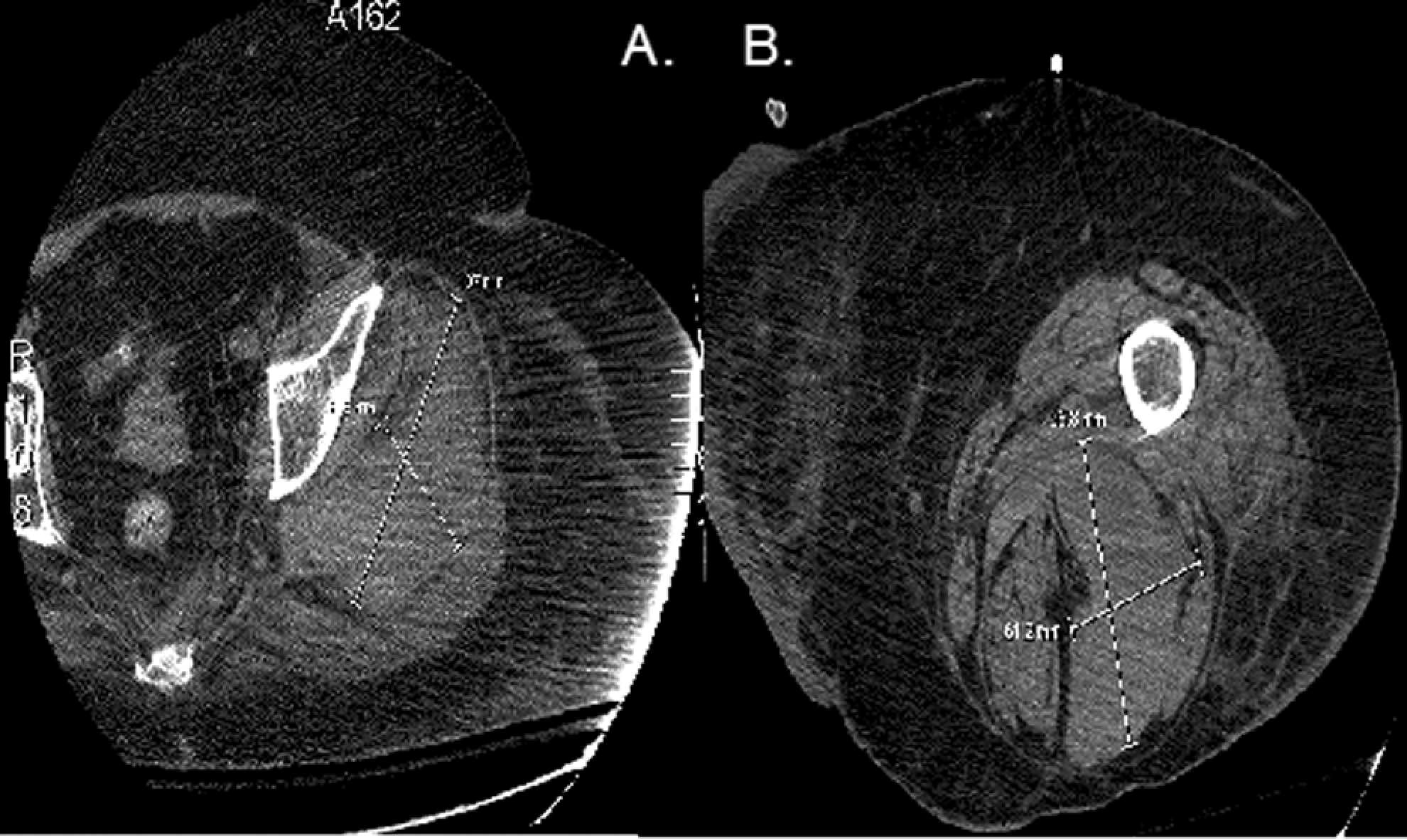
Computed tomography (CT) scan of the femur revealed 4 separate hematomas developing. A, A 9.5 cm × 6 cm hematoma in the adductor compartment. B, A 6.5 cm × 14 cm hematoma overlying the gluteus medius.
Discussion
In the United States, the generic version of enoxaparin manufactured by Sandoz and Momenta Pharmaceuticals was initially approved in July 2010, under the Food and Drug Administration’s abbreviated new drug application. This was 4 months prior to this patient’s second and most significant hemorrhage. This application grants FDA approval of equivalence to generic medications without necessitating clinical therapeutic equivalence trials. This application was originally intended for nonbiologic compounds, in which one could prove the equivalent molecular structure. However, for new classes of biological compounds, there is not one defined molecule or if there is, a variety of posttranscriptional changes may be made without clear recognition of this fact. The European Medicine Administration (EMA) demands clinical therapeutic trials to determine bio-similarity before granting pharmacologic equivalence to a generic compound. Enoxaparin was the first of the generic low-molecular-weight heparins (LMWHs) approved for use and one of the first biological agents to be approved under this process in the United States, 1 which may set a concerning precedent for both consumer safety and value.
Enoxaparin is produced by depolymerization of unfractionated heparin’s 48 disaccharide variants from porcine intestinal mucosa. However, the branded product has never been fully characterized and instead is listed as a mean molecular mass of 4.5 kDa, with multiple polysaccharide chains having undefined lengths and compositions. In approving the generic enoxaparin, the FDA accepted studies demonstrating in vitro function, similar production practices, and similar pharmacodynamics in healthy volunteers. 2 Evidence of in vivo efficacy and safety are implied based on the previous assertions of the FDA-abbreviated new drug application. This runs counter to the EMA who has still not approved a generic LMWH.
Within the 7 branded LMWHs in Europe and the United States, there is no therapeutic interchangeability, despite the similarity of the compounds. Of the few head-to-head trials, dalteparin and enoxaparin were dosed at 0.8 mg/kg versus 1 mg/kg to gain the same therapeutic result in acute coronary syndromes. Notably these compounds only differ in a nitrous acid digestion versus an alkaline hydrolysis, respectively. 3
There are significant concerns with the lack of oversight of generic enoxaparin formulations including differences in potency, immunogenicity, pharmacodynamics, and potential drug interactions. 4 Up to 17 generic formulations had been developed and marketed in the developing world, and several have already been voluntarily withdrawn due to adverse reactions and widely varying compositions. 5 Several trials with crossover pharmacodynamic studies have been conducted, which have shown no significant difference in activated PTT (aPTT) activity, thrombin time, however, in 1 study there were some slight differences in factor Xa activity.6,7 In other studies, there were differences in thrombin and factor Xa activity between some of the generic formulations, and differences in heparinase-I degradation of the formulations. 7 Another difficulty is finding the most effective way to measure biological activity of these compounds. One article asserts that measuring factor Xa and thrombin levels may not be predictive of pharmacodynamics in these heterogeneous compounds. 8
Hereby, we present the first published report of a temporal association with initiation of generic enoxaparin and development of multiple life-threatening hematomas. Unfortunately, factor Xa and IIa levels were never assessed, given the rapid deterioration of the patient’s status after her second hematoma. Thereby, the evidence in this case is considered at best circumstantial. We hope to add this to the growing body of literature that suggests that the FDA described sameness between biologic compounds based on pharmacodynamics and in vitro activity is insufficient when the active compound has never been fully defined nor purified. Generic equivalents clearly can be established for defined compounds such as warfarin; however, a burden of proof should be placed on manufacturers attempting to provide substitutes of agents such as LMWH and other biologics. Further post-market analysis needs to be performed to assess the reproducibility, efficacy, and safety of this generic formulation. Future generic biologic therapies should undergo more rigorous proof of efficacy and safety to ensure that they truly mimic the most important character of the original compound: its safety.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.