
Abstract
SARS-CoV-2 in COVID-19 triggers abnormalities in coagulation parameters that can contribute to thrombosis. The goals of this research were to determine the levels of fibrinogen, D-dimer and FDP in COVID-19 patients. Following a systematic study, among 1198 articles, 35 studies were included in the meta-analysis of fibrinogen levels in both severe and non-severe groups. The funnel plot, Egger’s regression asymmetry test, and Begg’s test used to measure the bias of publications. All meta-analysis performed by comprehensive meta-analysis version 2 (CMA2). The pooled findings of fibrinogen levels revealed a significant rise in fibrinogen levels in severe COVID-19 than non-severe patients with COVID-19. The D-dimer and FDP levels were significantly higher in severe patients than non-severe patients with COVID-19 were. The levels of fibrinogen, D-dimer, and FDP have increased significantly in ICU patients compared to non-ICU patients. Although, levels of clotting parameters do not always correlate with the severity of disease, these findings showed the diagnostic importance for fibrinogen, D-dimer, and FDP in COVID-19. The presence of a continuous rise in serial measurements of fibrinogen, D-dimer, and FDP may predict that patients with COVID-19 may become critically ill.
Introduction
In late December 2019, Wuhan, China, identified a disease that has widely spread across all continents. The World Health Organization (WHO) was named this infection as coronavirus disease 2019 (COVID-19) and named the cause of the infection severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 In February 11, 2021, the WHO announced 106,797,721 confirmed cases of COVID-19, and 2,341,145 deaths. 2 It is now considered a major threat to public health and the fifth global pandemic. COVID-19 has different symptoms, ranging from almost asymptomatic cases to serious lung injury and deadly thrombosis. 3 The most common symptoms of COVID-19 disease are fever, cough, and fatigue, progressive dyspnea caused by SARS-CoV-2. 4 –6 Organ failure is a common manifestation, which are associated with severe complications in patients hospitalized in an intensive care unit (ICU). 7 Further investigations were subsequently indicated that a cytokine storm’s release (proinflammatory cytokine including IL-6) could activate the coagulation cascade and trigger abnormal coagulation activity in the severe patient as macrothrombi in veins and arteries and thrombosis in vessel of various organs. 8,9 The elevated levels of fibrinogen, von Willebrand factor (vWF), factor VIII, fibrin degradation product (FDP) and thrombomodulin have documented in COVID-19. 10 –12 The deposit of fibrin molecules in lungs tissue (alveolar space and microvasculature) of dead patients with COVID-19 has reported. 13 –15 Nowadays, administration of low molecular weight heparin (LMWH) is a choice treatment in many medical centers. 16 –18 Growing documents are suggesting hypercoagulability persistence in patients with COVID-19 who are on anticoagulants. 19 –24
In addition, there is an important association between D-dimer and proinflammatory factors in hospitalized and critically ill patients with COVID-19, and the D-dimer test can predict thrombotic events. 25 A systematic analysis in COVID-19 patients found that increased D-dimer levels in these patients were associated with poor prognosis. 26 These dysregulation of coagulation factors may contribute in multiple ways to pathophysiology of COVID-19.
Fibrinogen is a glycoprotein formed in the liver and is an important coagulation factor in the common pathway of coagulation cascade. 27 Fibrinogen is a protein with high molecular weight in plasma and is known to be a biomarker of inflammation. 28 –30 Thus far, a comprehensive meta-analysis on fibrinogen level in patients with COVID-19 has not done. Filling the current knowledge gap seems to be a necessary step to make sense of pathophysiological alternations in COVID-19. Beside this, the levels of D-dimer and FDP in patients with COVID-19 were extracted from retrieved articles and meta-analysis was done for them to explore whether D-dimer and FDP levels in COVID-19 may be associated with severity of COVID-19.
Material and Methods
Data Source and Search Strategy
In this study, a literature review was conducted as a systematic search in 3 medical databases: PubMed, Scopus, and the Web of Science. To collect articles related to fibrinogen levels in COVID-19 patients, the keywords of “fibrinogen” or “fibrin” or “Coagulation factor I” and “COVID-19” or “SARS- CoV-2” were used. To further enhance productivity, a search was conducted by 2 separate authors (M R and Z Kh) on October 26, 2020. We entered all the articles into EndNote X8 reference manager software for review, and then deleted duplicate articles.
Study Selection and Eligibility Criteria
After removing redundant articles, the 2 first authors reviewed articles. At this point, review articles, letters, comments, and case reports were excluded from the list. Irrelevant articles removed after reading the titles or the abstracts. The remaining articles assessed for inclusion and exclusion criteria. The inclusion criteria were English language texts, and concomitant study on COVID-19 and fibrinogen. The exclusion criteria included inadequate pertinent information, less than 10 patients, the study on patients with concomitant occurrence of COVID-19 with inflammatory disorders such as any cancers, liver and kidney disease, diabetes, hypertension, etc. Since such inflammatory disorders can increase the levels of fibrinogen, D-dimer, and FDP in the plasma of patients. These inflammatory disorders can have interventional effect of the levels of fibrinogen, D-dimer, and FDP induced by SARS-CoV-2. Furthermore, the reference lists of each retrieved article were assessed for finding additional eligible documents. The mined data for analysis included demographic finding of patients, the severity of the COVID-19 disease, fibrinogen levels in various severity of COVID-19 infection. Furthermore, the reported levels of FDP and D-dimer were collected in patients with COVID-19.
Data Extraction and Quality Assessment
The 2 first authors independently extracted information from the articles into the Excel database. Data extraction included the first author’s name, study location, type of study design, type of the articles, sample size, severity criteria, fibrinogen levels, D-dimer and FDP levels if reported. The quality of the included articles assessed separately by 2 reviewers using the Joanna Briggs Institute (JBI) Appraisal Tool.
Data Synthesis and Analysis
The continuous data were described by the mean, standard deviation (SD), and standardized mean difference (SMD) with 95% confidence intervals (CI). Article data reported as medians and interquartile range, and means ± SD. Data were calculated by online software based on the method used by McGrath et al, Wan et al, and Luo et al. 31,32,33 All meta-analysis was performed by comprehensive meta-analysis version 2 (CMA2). I 2 -test measured heterogeneity between studies; I2 > 50% was considered as an increase in the degree of heterogeneity. A random-effects model was used to take into account variances (Table 3) within the studies and between studies. The funnel plot, Egger’s regression asymmetry test, and Begg’s test were used to evaluate the bias of publications. A 2-tailed P < 0.001 was considered statistically significant.
Results
Selection and Characteristics of the Articles
During the search carried out using a search strategy, 1198 articles were obtained, including 443 items from PubMed, 591 papers through Scopus, and 164 papers through the web of science. 686 articles existed following deletion of redundant articles. Subsequently, the articles were reviewed by title and abstract, which finally remained 132 papers. After reading the full text of the papers, 35 articles were chosen on the basis of the research requirements and consistency. Additionally, 5 articles were collected by reviewing the references list of the mined papers. Included 35 studies to evaluate fibrinogen levels between non-severe and severe cases, 5 between ICU and non-ICU patients (Figure 1). The characteristics of the included studies set out in Tables 1 and 2.
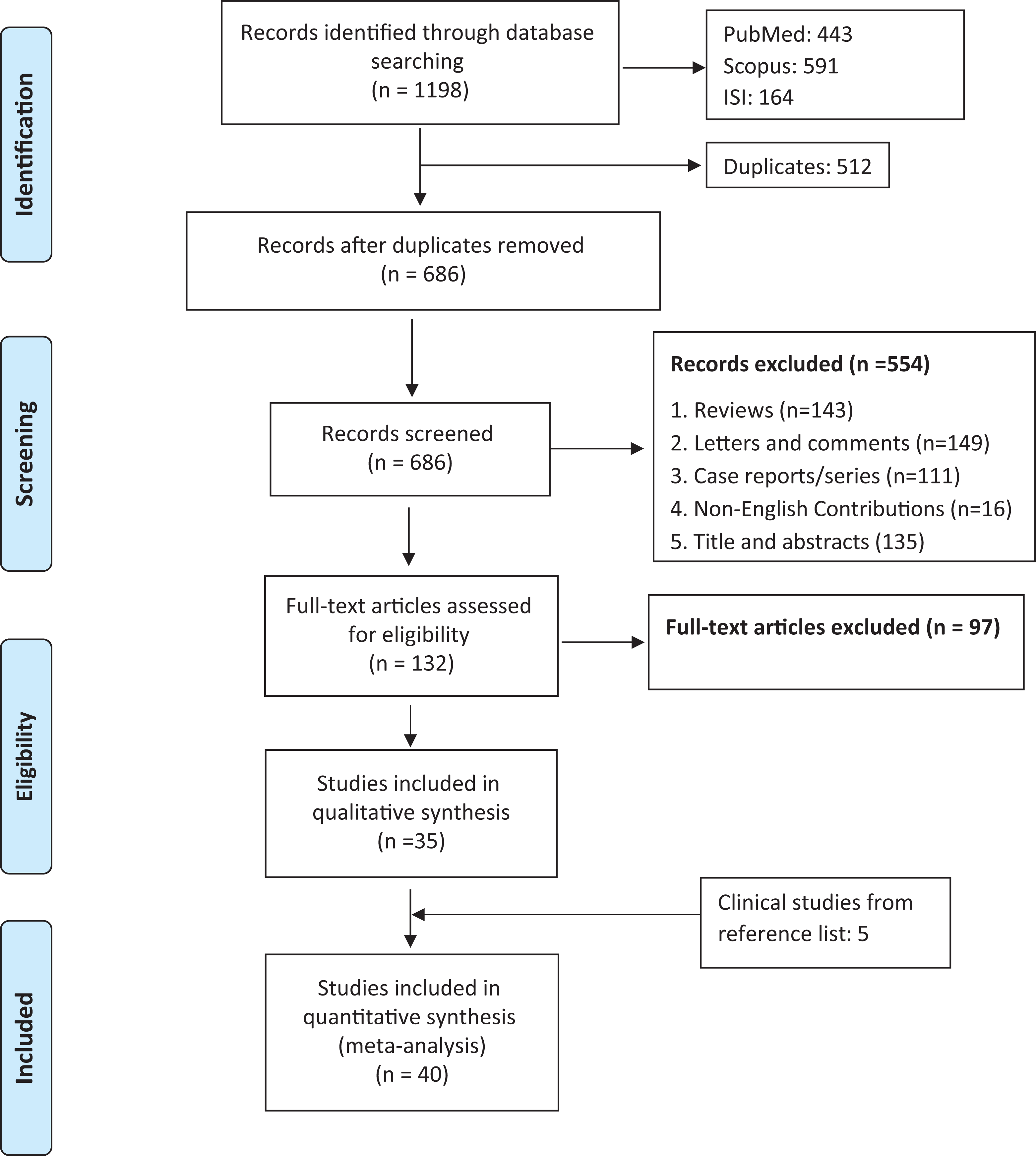
Flow-chart describing the literature study selection.a
Summary of Included Studies on Fibrinogen Level in Patients With Severe COVID-19 (on Admission).

a Data Reported as range, mean ± SD, or median (interquartile range).
Abbreviations: NR, not reported; N/A, Not applicable; NHC, National Health Commission of China; WHO, World Health Organization; RT-PCR, Real-Time Polymerase Chain Reaction; CT, Computed tomography; Ab, Antibody; Ref, Reference; ed, edit.
Summary of Included Studies on Fibrinogen Level in ICU and Non-ICU Patients With COVID-19 (on Admission).a

Abbreviations: NR, not reported; RT-PCR, Real-Time Polymerase Chain Reaction; Ref, Reference; ICU, intensive care unit.
a Data Reported as range, mean ± SD, or median (interquartile range).
Fibrinogen Level in Mild and Severe Cases with COVID-19
Thirty-five studies were used for the analysis of fibrinogen levels in both severe and non-severe groups 4,5,34 –65 (Table 1). Fibrinogen levels have been reported in 2207 severe patients with COVID-19 and 6057 non-severe patients with COVID-19. The performed analysis was consistent with the random model due to the high heterogeneity between studies (I2:82.9%; P < 0.00). The pooled results of fibrinogen levels in studies revealed a significant rise in fibrinogen levels in severe and non-severe patients with COVID-19 (SMD: 0.587 g/L; 95% CI: 0.445 - 0.730) (Figure 2). Overall, fibrinogen levels in severe COVID-19 patients were higher than non-severe COVID-19 patients.
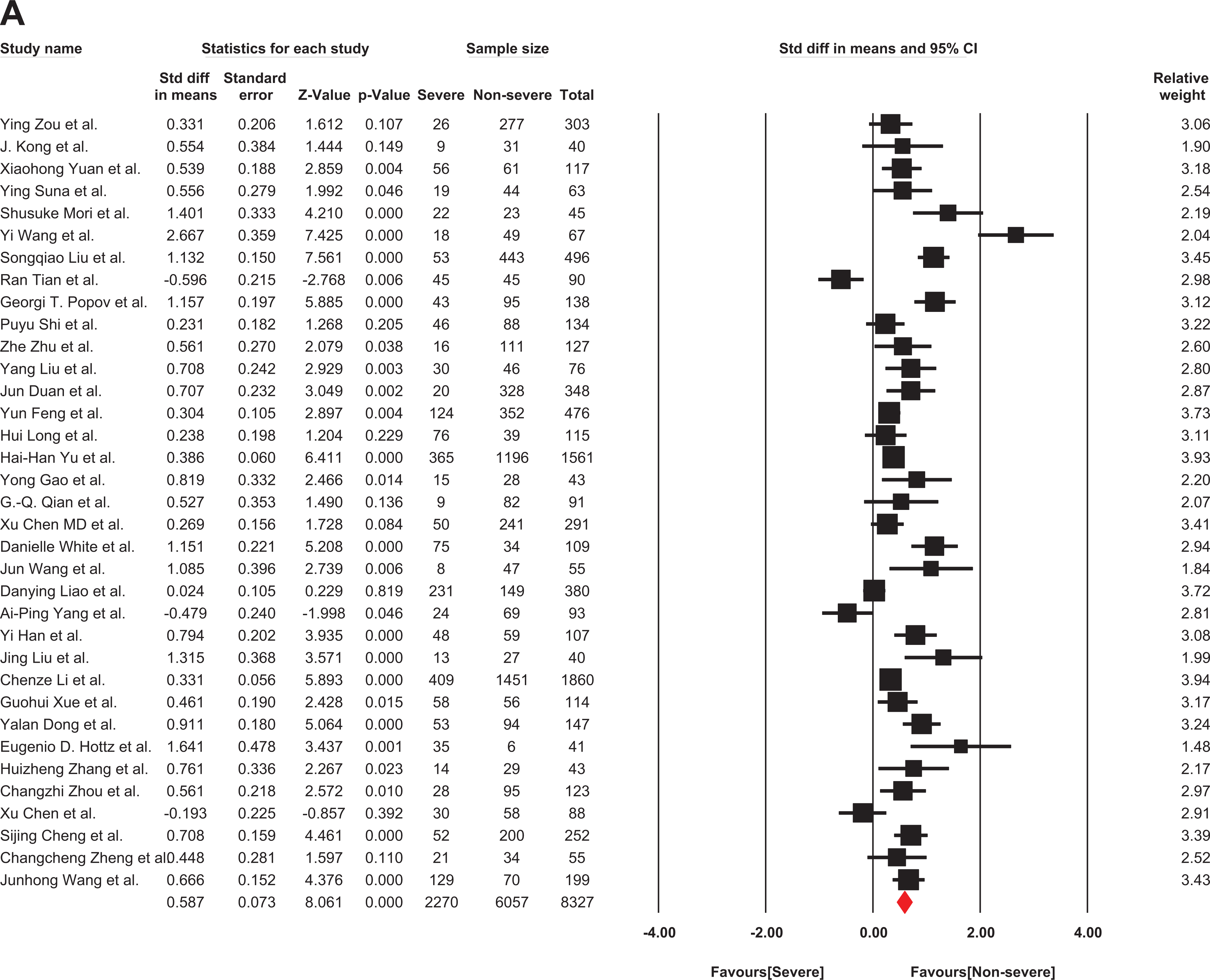
The forest plot of the difference in the fibrinogen between COVID-19 patients with non-severe or severe disease. Std indicates standard; COVID-19, coronavirus disease 2019.
Furthermore, D-dimer levels had reported in 34 publications, including 2260 severe and 6066 non-severe patients with COVID-19. The heterogeneity of the articles who reported D-dimer was high among studies (I2:78%; P < 0.00). Hence, the analysis was then conducted using a random model, which showed that the D-dimer level was significantly higher in severe patients than non-severe patients with COVID-19. (SMD: 0.859 μg/ml; 95%CI: 0.859 – 0.991) (Figure 3).
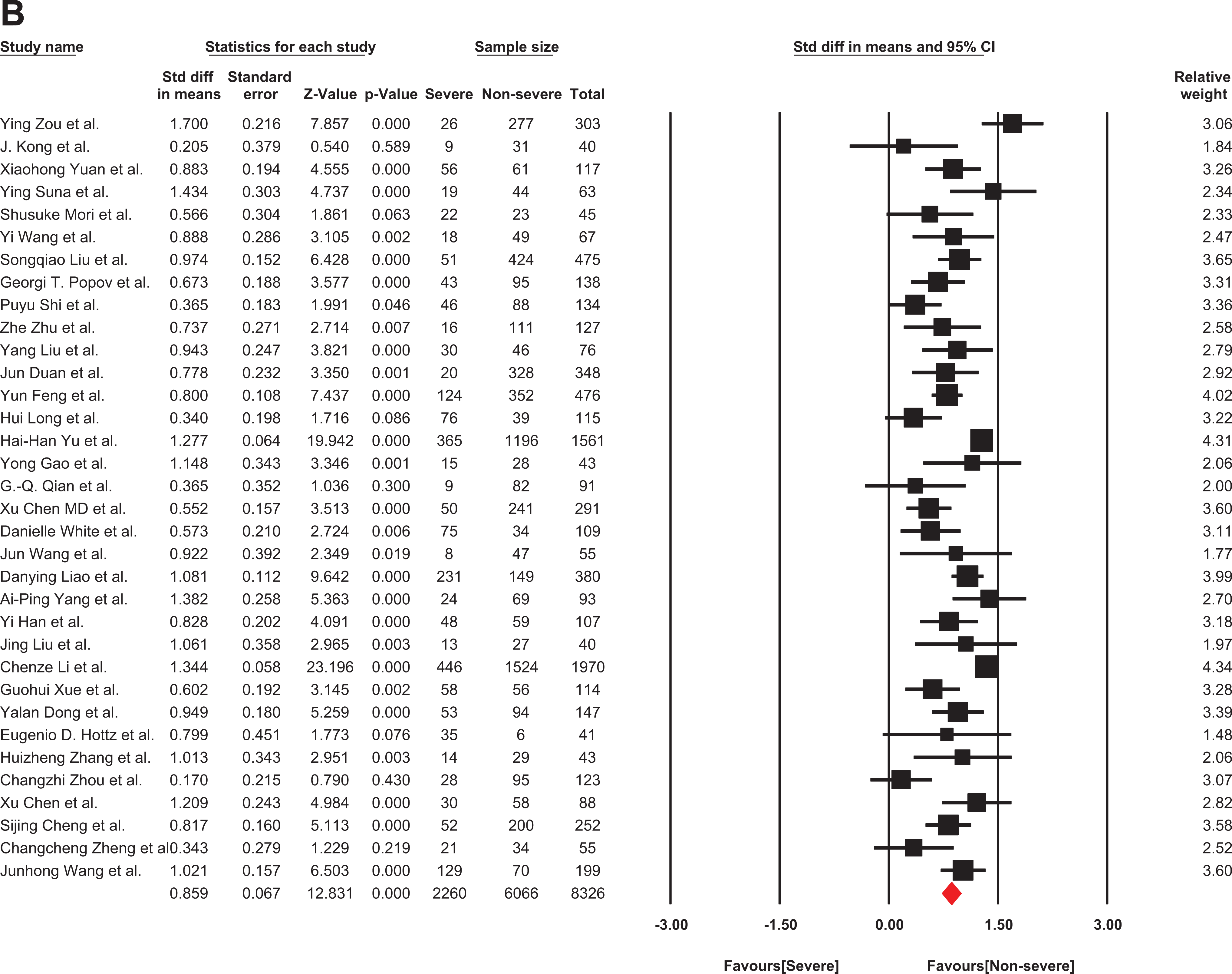
The forest plot of the difference in the D-dimer levels between patients with non-severe and severe COVID-19. Std indicates standard; COVID-19, coronavirus disease 2019.
Seven articles reported FDP levels (852 severe and 1805 non-severe patients with COVID-19). Due to high heterogeneity of retrieved papers (I2 = 84%), they were analyzed by the random model that showed a significant increase in FDP in severe patients with COVID-19 (SMD: 0.725 μg/ml; 95% CI: 0.439 – 1.010) (Figure 4).
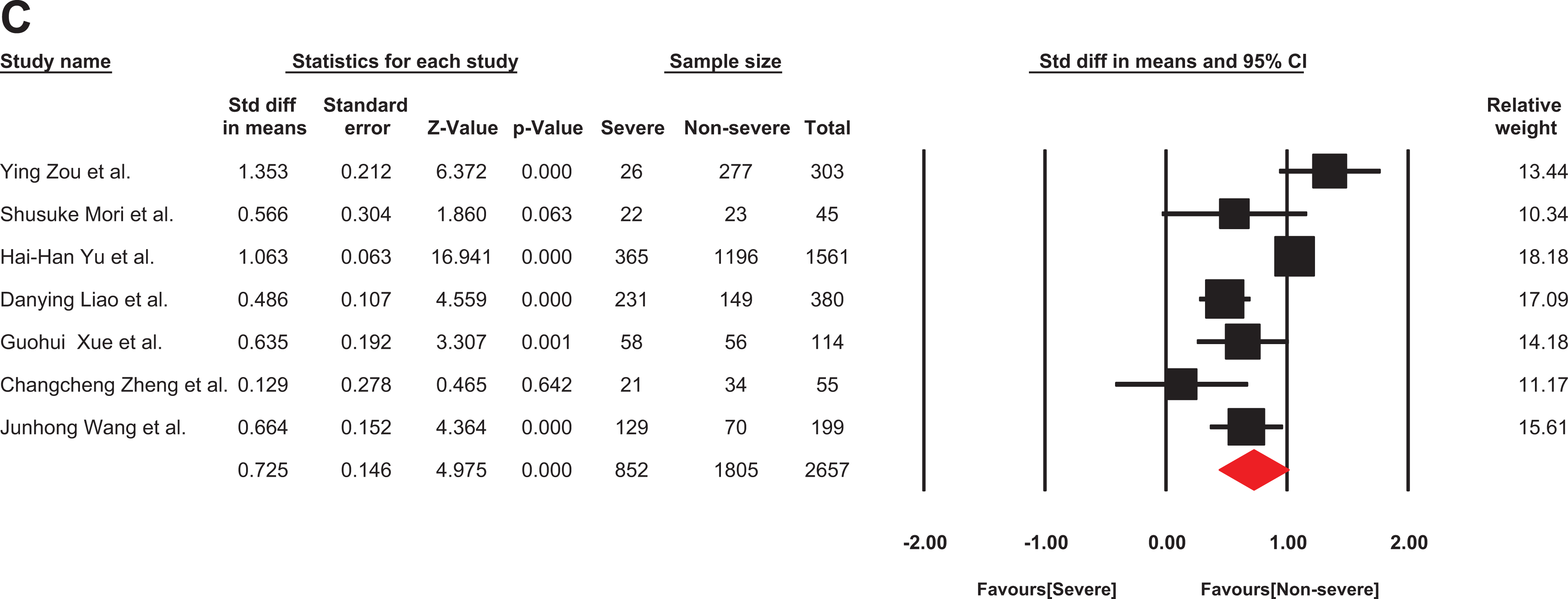
The forest plot of the difference in the FDP in patients with non-severe and severe COVID-19. Std indicates standard; COVID-19, coronavirus disease 2019.
Fibrinogen Level in Icu and Non-Icu Patients with COVID-19
Five studies were involved in the analysis of fibrinogen level between the ICU and non-ICU patients with COVID-19 66 –70 (Table 1). The patients with COVID-19 who had hospitalized in an ICU ward are critically severe ill. They can meet any of the following criteria: shock, need to mechanical ventilation for respiration, and failure of any organ(s) needing ICU monitoring. Hence, patients with COVID-19 in ICU can also be categorized as the most severe form of COVID-19 infection. D-dimer and fibrinogen levels have been registered in 678 non-severe patients (non-ICU patients) and 164 severe patients (ICU patients). There was no heterogeneity for fibrinogen in the 5 studies (I2:0%; P: 0.51), so the data were analyzed using a fixed model. Based on the findings of this report, fibrinogen levels in patients who admitted to ICU are significantly higher than non-ICU patients (SMD: 0.775 g/L; 95% CI: 0.596 –0.995) (Figure 5). D-dimer levels also increased significantly in ICU patients compared to non-ICU patients (I2: 61% P: 0.035) (SMD: 0.582 μg/ml; 95% CI: 0.245 – 0.920) (Figure 6).
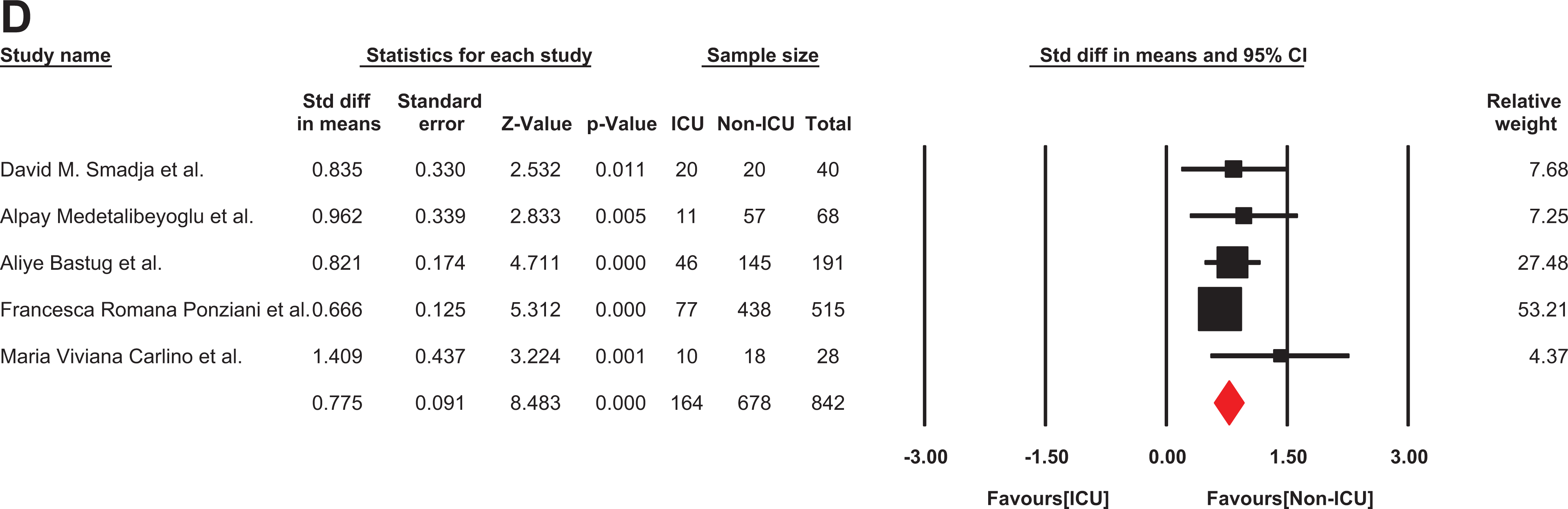
The forest plot of the difference in the fibrinogen level in ICU and non-ICU COVID-19 patients. Std indicates standard; COVID-19, coronavirus disease 2019; ICU, Intensive care unit.
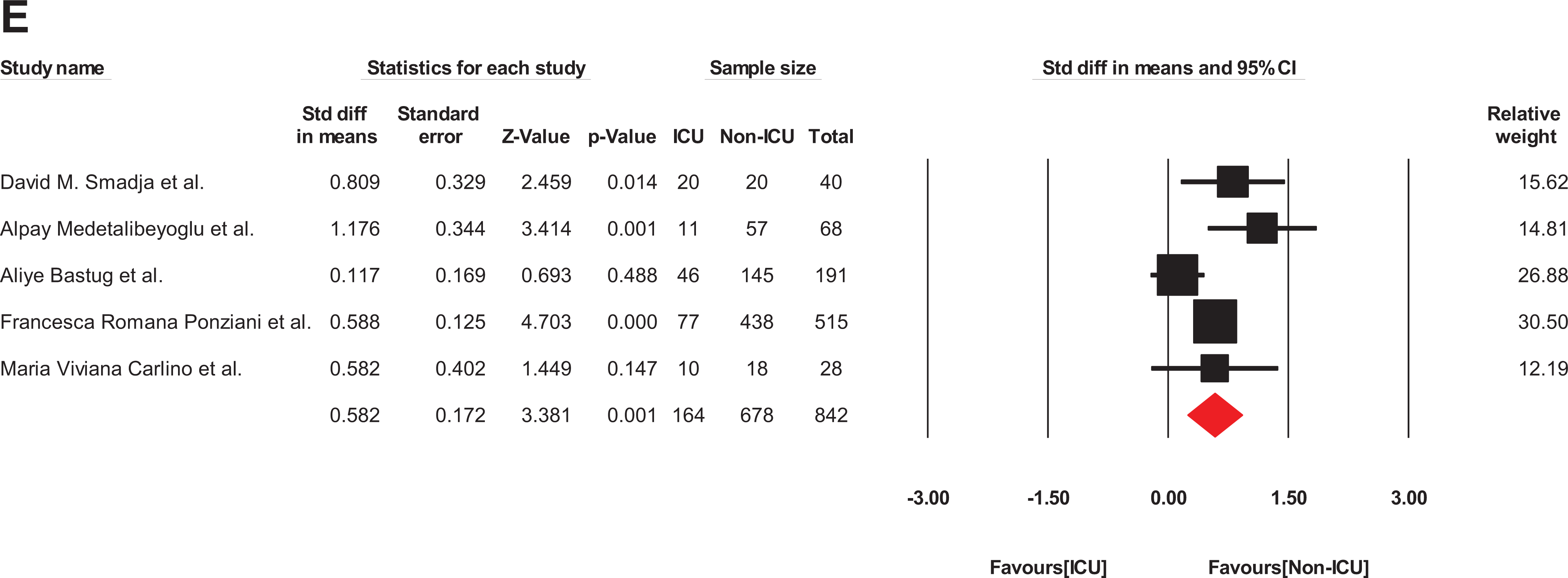
The forest plot of the difference in the D-dimer levels in ICU and non-ICU patients with COVID-19. Std indicates standard; COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Sensitivity Analysis and Publications’ Bias
In order to measure the effect of each sample on the analysis, each article omitted from the analysis to quantify the SMD. We did not notice a substantial change in the effect size before and after extracting each sample. The sensitivity plot for fibrinogen levels in severe and non-severe patients with COVID-19 did not indicate substantial sensitivity (Figure 7). In order to investigate the bias of publication between fibrinogen papers, funnel plot was drawn between severe and non-severe patients. There was no bias in publications (Figure 8). Additionally, asymmetry tests, Begg’s, and Egger’s tests were calculated for all groups (Table 4).

Sensitivity analysis of the Fibrinogen levels between COVID-19 patients with or without the severe disease.
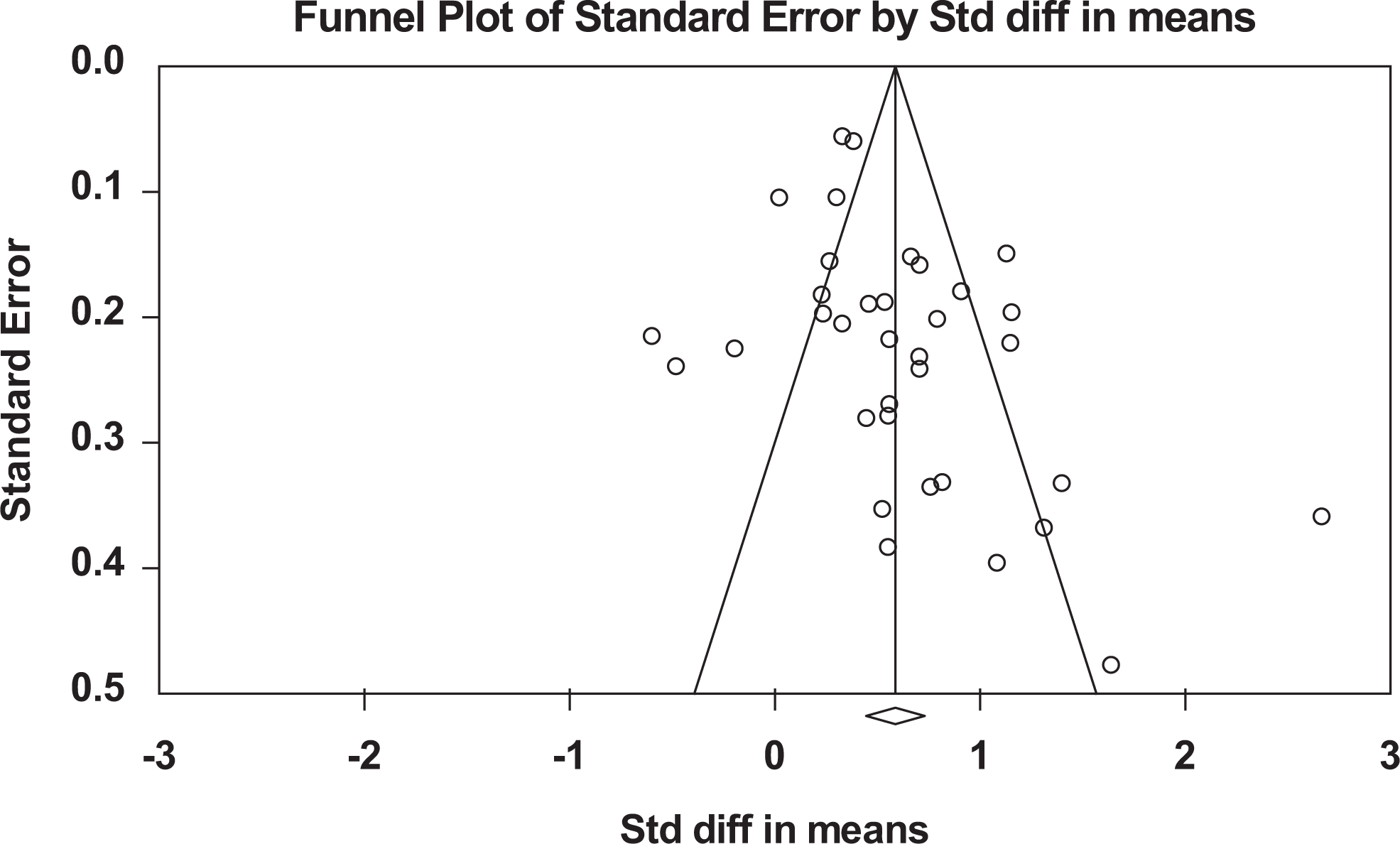
Funnel plot comparing the fibrinogen levels indicators among patients with COVID-19.
Meta-Analysis of some Coagulation Parameters in COVID-19 Patients.

Abbreviations: ICU, Intensive care unit; FIB, fibrinogen; FDP, fibrin degradation product; SMD, standard mean difference; CI, Confidence interval; g, gram; L, liter; μg, Microgram; mL, milliliter; No, number.
Assessment of Publications' Bias by the Egger’s and the Begg’s Test.

Abbreviations: FIB, fibrinogen; FDP, Fibrin degradation product; S, severity group; I, ICU and Non-ICU group
Conclusion
The high prevalence of COVID-19 in the world is associated with noticeable morbidity and mortality, while its pathophysiologic pathways are unclear. Nowadays, by extending our knowledge about SARS-CoV-2, the role of thrombosis in pathophysiology of COVID-19 is becoming clear and clear day by day. Postmortem findings of coagulation parameters in patients with COVID-19 documented extravascular fibrin deposition in parallel to COVID-19 development and organ failure. This systematic review and meta-analysis showed that levels of fibrinogen, FDP, and D-dimer were frequently increased in patients with COVID-19. Moreover, what clearly emerged from our pooled analysis is that the levels of fibrinogen, D-dimer, and FDP were significantly higher in patients with severe COVID-19 compared to those with non-severe COVID-19. Furthermore, the levels of fibrinogen, D-dimer, and FDP were significantly higher in COVID-19 patients who hospitalized in ICU compared to non-ICU patients with COVID-19.
These findings set out the diagnostic importance for fibrinogen, D-dimer, and FDP in COVID-19. Real-time PCR output is not available in many developing countries, and clinical physicians are now using routine tests such as low lymphocyte count, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) to detect COVID-19. The results of the current meta-analysis revealed that fibrinogen, D-dimer and FDP could also be used as serial measurement and diagnostic laboratory parameters for suspicious to COVID-19. Moreover, fibrinogen, D-dimer and FDP can be used as predictors for anticipation that patients with COVID-19 would be seriously ill. Such patients need access to tertiary medical services, including ICU care. Hence, alarming signs from elevated levels of fibrinogen, D-dimer, and FDP would also have informative results on request ICU beds, more intensive care facilities, and also warns the possibility of transferring the patient to the end stage phase. Recently, Tang et al reported that dead hospitalized patients with COVID-19 meet the criteria for disseminated intravascular coagulation (DIC). 71 Hence, monitoring the levels of fibrinogen, D-dimer, and FDP for patients with mild COVID-19 who tend to have severe form of the disease seems to be rational act. On the other hand, elevated levels of these hemostatic laboratory parameters indicate that infected patients need to undergo an anticoagulant or a stronger anti-hemostatic drug (in patients who receive anti-platelet drugs). Fibrinogen is a crucial coagulation factor in coagulation cascade, and so increased levels of fibrinogen can predispose patients to prothrombotic conditions. Developing micro-thrombosis can be cause several organs' dysfunctions in a patient with COVID-19. Such information is critical in understanding, prevention, and treating COVID-19. Overall, physicians treating patients with COVID-19 would tend to have an eye on the levels of fibrinogen, D-dimer, and FDP. Given that, prophylaxis is superior to treatment alternatives, it suggests that regular laboratory monitoring of fibrinogen, D-dimer, and FDP levels can help the physicians to decide triggering anticoagulant prophylaxis regimens.
As D-dimer is a result of the action of fibrinolysis system on fibrin mesh, it is expected that more severe symptoms will occur in patients with COVID-19 who have an abnormality in fibrinolytic system. The assessment of the components of the fibrinolysis system in patients with severe COVID-19 may show any new findings.
Lack of data on the levels of fibrinogen, D-dimer and FDP in patients with COVID-19 who have died was a limitation of this study. It is also recommended that the levels of the current parameters in medical records history of dead patients with COVID-19 to be investigated.
Footnotes
Authorship
RM and KhZ searched the articles, analyzed the papers and wrote the first draft. MH gave idea, wrote discussion and finalized the manuscript.
Conflict of Interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study supported by Mashhad University of Medical Sciences (Grant number: 991446).