
Abstract
Objective
To investigate the correlation between neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and risk stratification indicators as well as thrombus burden in patients with moderate-to-high risk acute pulmonary embolism (APE), and to assess the changes in these parameters following interventional therapy.
Methods
This study retrospectively included patients with moderate-to-high risk APE who were admitted to the Department of Interventional Vascular Surgery at Putian First Hospital from May 2020 to May 2024. All patients received anticoagulation therapy, pulmonary artery catheter-directed thrombolysis, and/or mechanical thrombectomy. Patients were further divided into subgroup A if they did not present with any of the following conditions at admission: a) acute inflammatory diseases (including lung infections); b) malignant tumors; c) history of trauma or surgery within the past 2 months. Patients with any of the aforementioned conditions were classified as subgroup B. Additionally, 50 healthy individuals were randomly selected as the healthy control group.
Results
The NLR and PLR in subgroup A were significantly lower than those in subgroup B (P < .01). Compared with the healthy control group, the NLR in the APE group and subgroup A was significantly higher (P < .001). There were no significant differences in NLR and PLR between the troponin I-negative and troponin I-positive groups (P > .05), or between the N-terminal pro-B-type natriuretic peptide (NT-proBNP)-negative and NT-proBNP-positive groups (P > .05). There were no significant correlations between NLR and PLR with risk stratification indicators and pulmonary artery embolism index (P > .05). Compared with before treatment, NLR, troponin I, NT-proBNP, right ventricular diameter/left ventricular diameter ratio, and pulmonary artery embolism index were significantly reduced after treatment (P < .05), while there was no significant difference in PLR before and after treatment (P > .05).
Conclusion
Elevated NLR in patients with APE, which decreases after effective treatment, may be used for assessing disease status and treatment efficacy. However, there is no correlation between NLR and risk stratification indicators or thrombus burden. PLR does not demonstrate significant value in assessing APE.
Keywords
Introduction
Acute pulmonary embolism (APE) is a common cardiovascular emergency with a high mortality rate if not treated properly. 1 Currently, efforts are being made to further refine the risk stratification of APE, and certain parameters have shown promise in this regard. As novel expressions of inflammatory markers, the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have prognostic value in many inflammatory and immune diseases. 2 Moreover, the relationship between NLR and cancer treatment efficacy is currently a hot research topic.3,4
Research indicates that the enhancement of APE-associated thrombotic inflammatory response is related to the release of endogenous glycosaminoglycans and changes in hematological indices. 5 The predictive effect of hematological indices on mortality depends on their relationship with the inflammatory response. 5 Soylu et al's research indicates that an NLR ≥ 5.7 is a predictive factor for in-hospital mortality among patients with APE. 6 Specifically, patients with an NLR value above 5.7 had a mortality rate that was 10.8 times higher than that of patients with an NLR value below 5.7. 6 Phan et al's research shows that when PLR is 256.6, the sensitivity and specificity for predicting all-cause mortality in patients with APE are 53.6% and 82.2%, respectively. 7 Numerous studies have indicated that NLR and PLR are also useful indicators for predicting adverse outcomes in patients with APE, but their value in assessing the severity of APE has been controversial.8-11
Guiding treatment and assessing prognosis through APE risk stratification is the current standard practice. In China, risk stratification is primarily determined based on hemodynamic parameters, right ventricular function, and cardiac biomarkers. Internationally, there is more emphasis on factors such as age and underlying diseases, with the Pulmonary Embolism Severity Index (PESI) being the main determinant of risk stratification. Since this study was retrospective, it was difficult to obtain reliable indicators for accurate risk stratification. Therefore, we chose cardiac troponin I (cTnI), N-terminal pro-B-type natriuretic peptide (NT-proBNP), and right ventricular diameter (RVD)/left ventricular diameter (LVD) for analysis because these indicators are important components of risk stratification and can be accurately obtained. Additionally, pulmonary artery obstruction index (PAOI) is an indicator for assessing pulmonary artery thrombus load. 12 These indicators are all important for measuring the severity of APE. We attempted to analyze the relationship between NLR, PLR, and these indicators.
The objective of this study is to retrospectively analyze the correlation between NLR, PLR and major risk stratification indicators as well as thrombus burden in patients with moderate-to-high risk APE, and to analyze the changes in NLR and PLR before and after treatment.
Materials and Methods
Study Subjects and Grouping
Patients with moderate-to-high risk APE who were admitted to the Interventional Vascular Surgery Department of Putian First Hospital from May 2020 to May 2024 were retrospectively included. Inclusion criteria were: a) high-risk (hypotension or shock) or moderate-risk (imaging indicating right ventricular dysfunction or elevated cardiac biomarkers) APE; b) receipt of anticoagulation therapy, pulmonary artery catheter-directed thrombolysis, and/or mechanical thrombectomy. Exclusion criteria were: a) subacute or chronic pulmonary embolism; b) lack of blood routine test results before treatment. APE patients were further divided into subgroup A if they did not present with any of the following conditions at admission: a) acute inflammatory diseases (including lung infections); b) malignant tumors; c) history of trauma or surgery within the past 2 months. Patients with any of the aforementioned conditions were classified as subgroup B. Blood routine test reports from 50 randomly selected healthy individuals who underwent physical examinations at our center were used as the healthy control group.
Treatment Methods
Anticoagulation Therapy: During catheter-directed thrombolysis, unfractionated heparin was administered intravenously to ensure that the activated partial thromboplastin time was maintained at 1.5 to 2.0 times the normal value. During periods without catheter-directed thrombolysis, low-molecular-weight heparin was administered via subcutaneous injection at a dosage of 100 U/kg, once every 12 h.
Interventional Therapy: For patients with concurrent acute deep venous thrombosis in the lower extremities, an inferior vena cava filter was placed prior to catheter-directed thrombolysis. A 5F Pig catheter was inserted through the femoral vein and positioned in the more severely affected pulmonary artery. Urokinase was administered through the Pig catheter at a dosage of 400 000 to 500 000 U per day. Pulmonary angiography was repeated every 1 to 2 days, and the position of the Pig catheter was adjusted as needed. The thrombolysis time was typically controlled within 2 to 3 days. For some patients with APE who had higher thrombolysis risks and more severe embolism, the Angiojet thrombus extraction device could be used for treatment.
Observation Indices and Criteria
The data for NLR, PLR, cTnI, NT-proBNP, RVD/LVD, and PAOI before treatment represent the measurements taken from the time of admission to the hospital until before the interventional therapy. The data for these indices after treatment represent the measurements taken from the completion of interventional therapy until before discharge. The measurement method for RVD/LVD: On the cross-sectional images of CT pulmonary angiography, measure the maximum internal diameters of the right and left ventricles perpendicular to the interventricular septum, and calculate the ratio between the two. The calculation method for Mastora PAOI: On CT pulmonary angiography, the pulmonary artery is divided into 5 mediastinal artery segments, 6 lobar artery segments, and 20 segmental artery segments. The degree of obstruction is classified into 5 levels: < 25% obstruction is 1 point; 25%–49% obstruction is 2 points; 50%–74% obstruction is 3 points; 75%–99% obstruction is 4 points; and complete obstruction is 5 points. The total score ranges from 0 to 155. PAOI is calculated as (total score / 155) × 100%.
Values exceeding the upper normal limits for cTnI and NT-proBNP were defined as positive, and those not exceeding were defined as negative. The upper limit for cTnI was 0.03 μg/L. The upper limits for NT-proBNP varied by age: 450 ng/L for those under 50 years old, 900 ng/L for those aged 50–75 years old, and 1800 ng/L for those over 75 years old.
Statistical Methods
Measurement data conforming to a normal distribution are expressed as mean ± standard deviation, while those not conforming to a normal distribution are expressed as Median (First Quartile, Third Quartile). Count data are expressed as number of cases (%). Comparisons of measurement data between groups are performed using independent sample t-tests or non-parametric tests. Comparisons of measurement data before and after treatment are performed using paired sample t-tests or non-parametric tests. Correlation analysis is performed using the Spearman correlation test. A P-value < .05 indicates that the difference is statistically significant.
Results
General Baseline Characteristics of APE Patients and Comparison with Healthy Controls
The general baseline characteristics of APE patients are presented in Table 1. The NLR and PLR in subgroup A were significantly lower than those in subgroup B (P < .01). Compared with the healthy control group, the NLR and absolute neutrophil count (ANC) were significantly higher in the APE group and subgroup A (P < .001), while the platelet count (PLT) was significantly lower (P < .001). (Table 1)
General Baseline Characteristics of APE Patients, and Comparison of Cellular Biomarkers among the APE Group, Subgroups, and the Healthy Control Group.
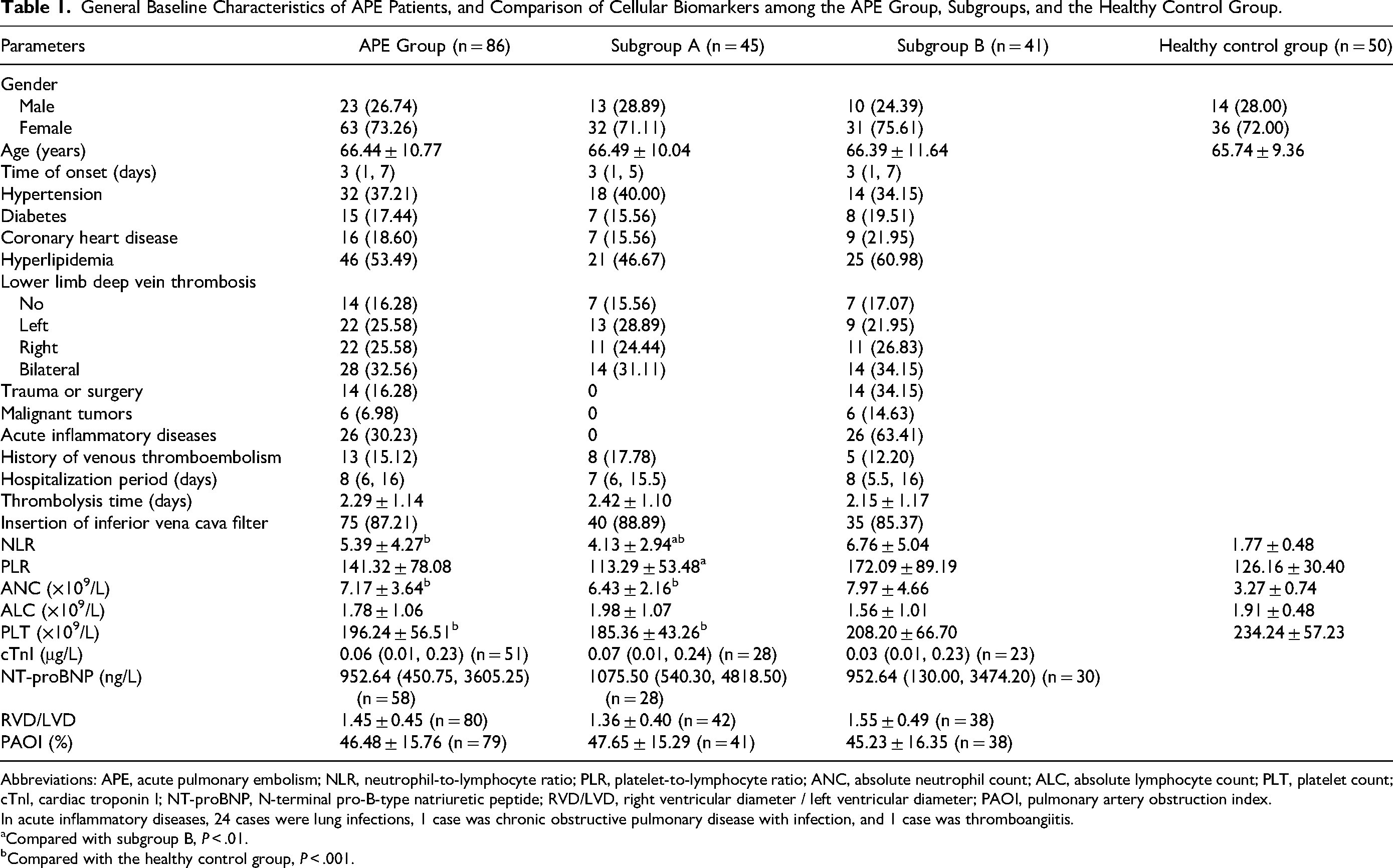
Abbreviations: APE, acute pulmonary embolism; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; PLT, platelet count; cTnI, cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide; RVD/LVD, right ventricular diameter / left ventricular diameter; PAOI, pulmonary artery obstruction index.
In acute inflammatory diseases, 24 cases were lung infections, 1 case was chronic obstructive pulmonary disease with infection, and 1 case was thromboangiitis.
Compared with subgroup B, P < .01.
Compared with the healthy control group, P < .001.
Correlation Analysis of NLR, PLR with Risk Stratification Indicators and PAOI
There were no significant differences in NLR, PLR, ANC, absolute lymphocyte count (ALC), or PLT between the cTnI-negative and cTnI-positive groups (P > .05), and similarly, no significant differences were observed in these parameters between the NT-proBNP-negative and NT-proBNP-positive groups (P > .05). Within subgroup A, the ANC was lower in the cTnI-negative group compared to the cTnI-positive group (P < .05). (Tables 2 and 3) No significant correlations were found between NLR, PLR, and the risk stratification indicators or PAOI (P > .05). The same results were obtained within subgroup A. (Table 4)
Comparison of NLR and PLR Between the cTnI-Negative and cTnI-Positive Groups.
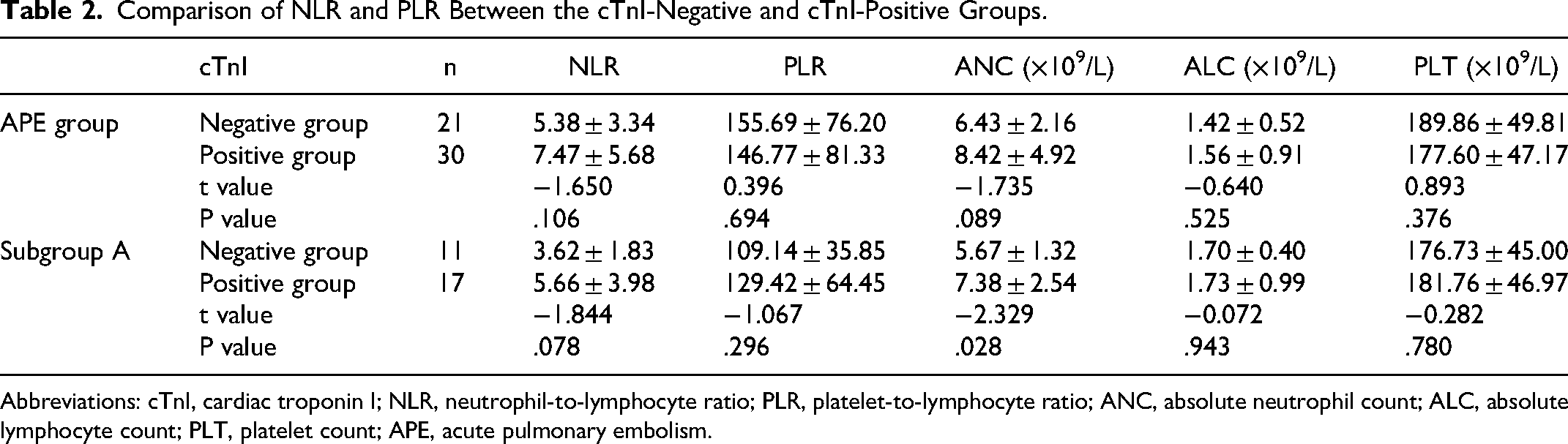
Abbreviations: cTnI, cardiac troponin I; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; PLT, platelet count; APE, acute pulmonary embolism.
Comparison of NLR and PLR Between the NT-proBNP-Negative and NT-proBNP-Positive Groups.
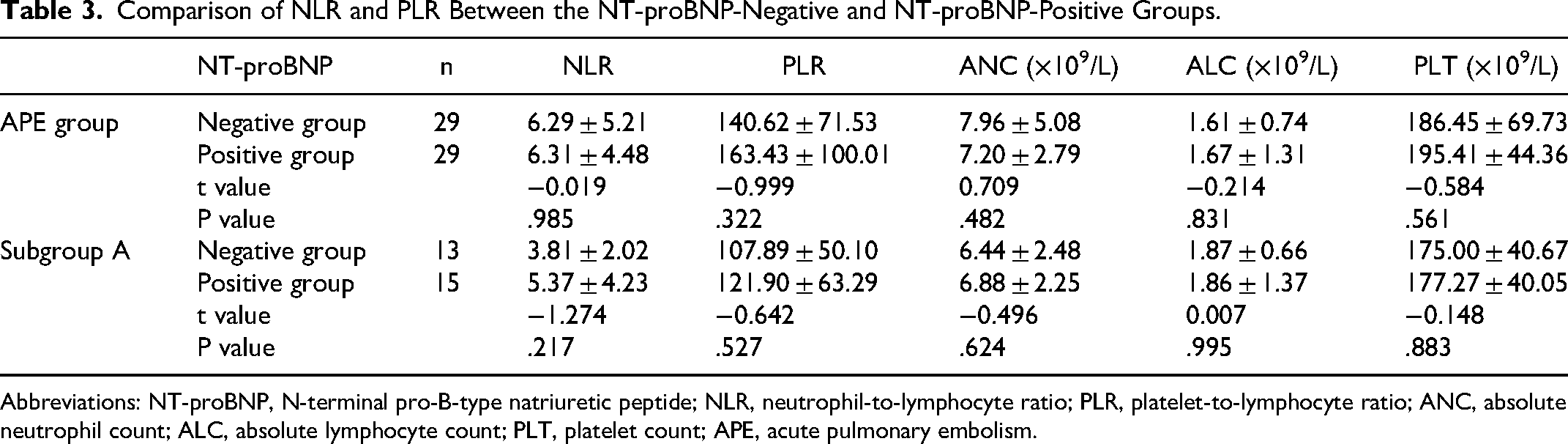
Abbreviations: NT-proBNP, N-terminal pro-B-type natriuretic peptide; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; PLT, platelet count; APE, acute pulmonary embolism.
Correlation Between Cellular Biomarkers and Risk Stratification Indicators in the APE Group and Subgroup A.
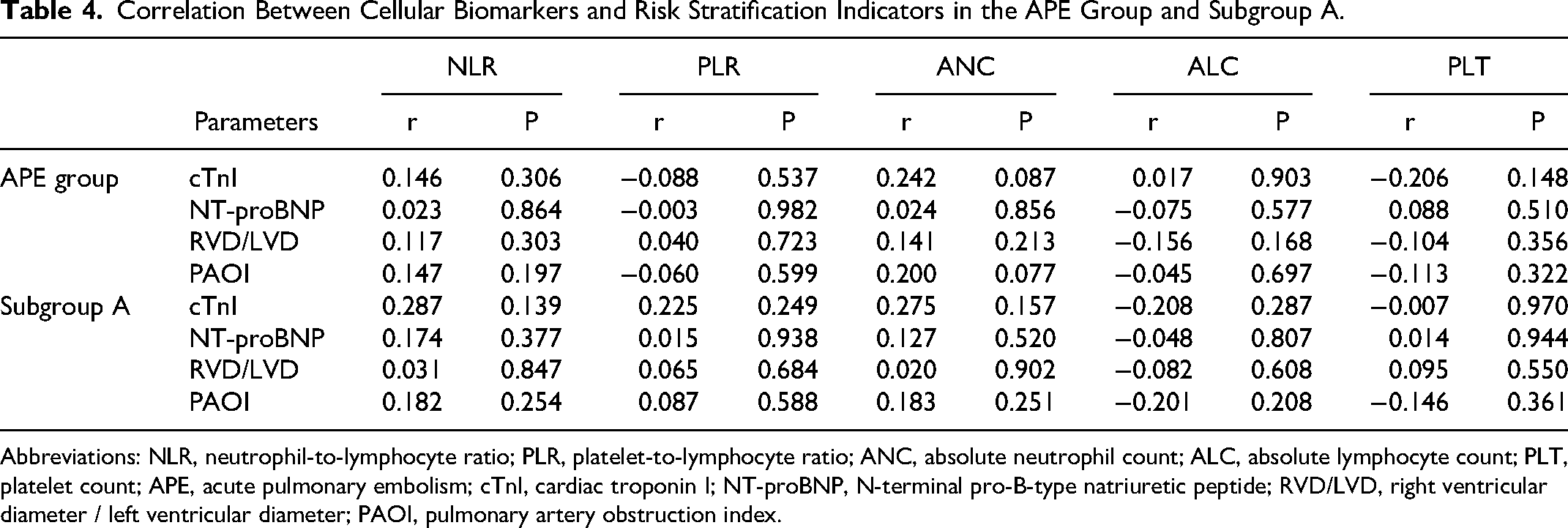
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; PLT, platelet count; APE, acute pulmonary embolism; cTnI, cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide; RVD/LVD, right ventricular diameter / left ventricular diameter; PAOI, pulmonary artery obstruction index.
Changes in Indicators Before and After Treatment
Compared with before treatment, NLR, ANC, ALC, cTnI, NT-proBNP, RVD/LVD, and PAOI were significantly reduced after treatment (P < .05), while there were no significant differences in PLR and PLT before and after treatment (P > .05). The same results were obtained in subgroup A. (Table 5)
Comparison of Indicators Before and After Treatment.
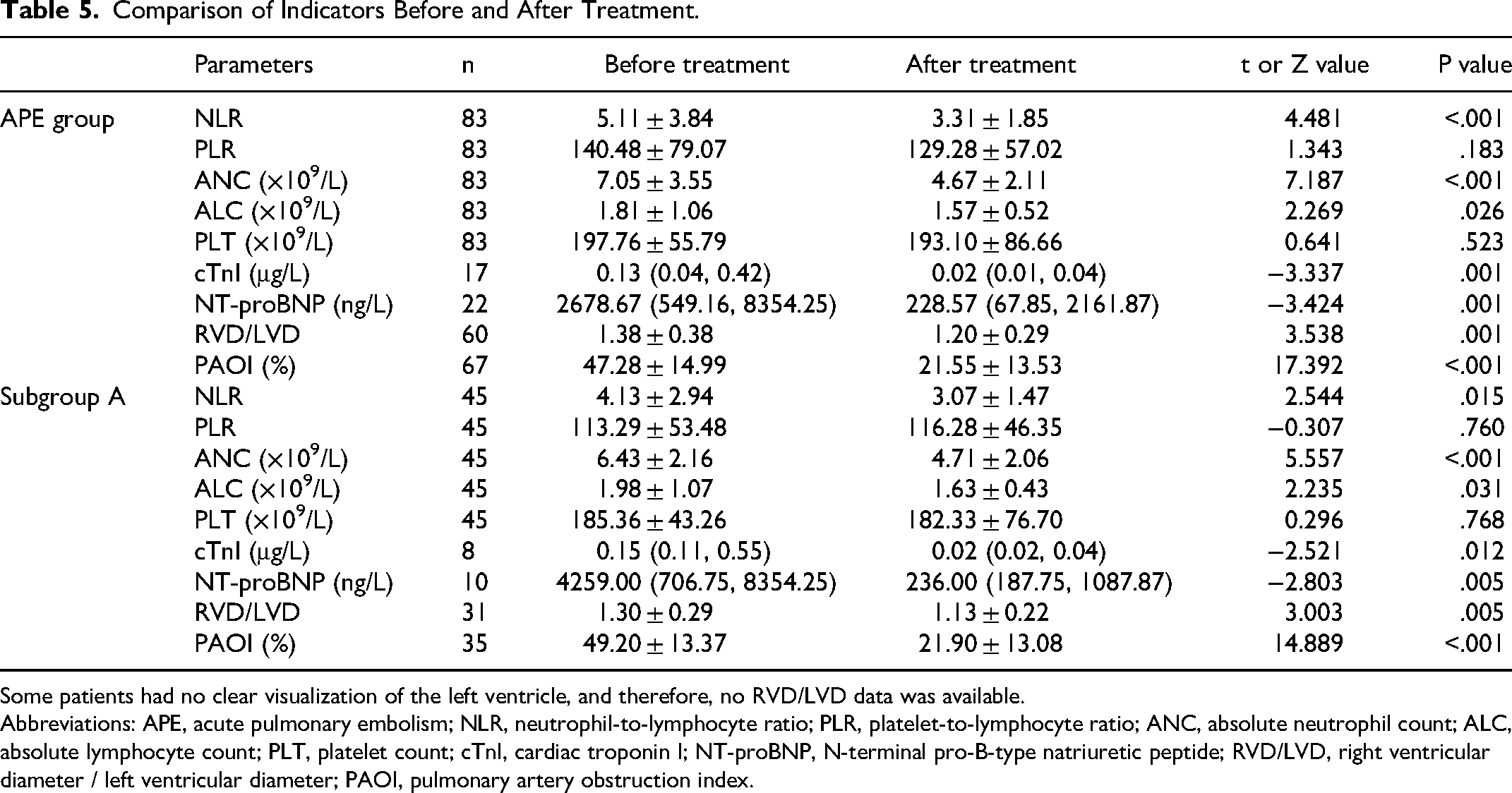
Some patients had no clear visualization of the left ventricle, and therefore, no RVD/LVD data was available.
Abbreviations: APE, acute pulmonary embolism; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; PLT, platelet count; cTnI, cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide; RVD/LVD, right ventricular diameter / left ventricular diameter; PAOI, pulmonary artery obstruction index.
Discussion
The study indicates that NLR and PLR are novel and beneficial indicators for assessing inflammation, disease activity, and severity in many clinical contexts. For instance, a meta-analysis supports the hypothesis that depression is associated with inflammation, and NLR can be used as an indicator for depression. 13 Inflammation and endothelial injury play crucial roles in the progression of APE. 14 Compared with other inflammatory cytokines (such as interleukin-6 and tumor necrosis factor-α), NLR and PLR are simple and cost-effective indicators. In this study, the NLR in the APE group and subgroup A was significantly higher than that in the healthy control group (P < .001), which is consistent with previous research findings. NLR represents the balance between neutrophils and lymphocytes, and a high NLR indicates a high degree of inflammation. The mechanism linking inflammation and APE is not fully understood. Venous endothelial injury triggers an inflammatory response, activating vascular endothelial cells, monocytes, and other cells to secrete tissue factor (coagulation factor III), which further initiate the coagulation process. 15 At the same time, neutrophils are activated and release various inflammatory mediators, further promoting thrombus formation and the release of inflammatory cytokines. 16 Since NLR and PLR are systemic inflammatory factors, factors such as acute inflammatory diseases, malignancies, trauma, surgery, and others that APE patients may have, will inevitably affect inflammatory indicators, especially considering that many patients present with acute lung infections at the time of admission. Therefore, patients with these confounding factors at the time of admission were excluded from subgroup A in this study. The results showed that NLR and PLR in subgroup A were significantly lower than those in subgroup B (P < .01), indicating that these factors indeed had a significant impact on NLR and PLR. If one wants to study the relationship between APE and inflammatory factors, the influence of these factors needs to be carefully considered.
Teodoru et al found that an elevated NLR is significantly associated with increased inpatient mortality in APE. 17 Telo et al demonstrated that NLR and PLR are elevated in high-risk APE patients, and NLR may have predictive value for inpatient mortality and 3-month mortality, while PLR may have predictive value for 3-month mortality. 18 Most previous studies have analyzed the predictive value of NLR and PLR for APE mortality. However, in our study, there were only 4 inpatient deaths, which was not statistically significant, so we did not analyze the relationship between NLR, PLR, and mortality. Nevertheless, we still wanted to investigate whether NLR and PLR have value in assessing the severity of APE.
This study shows that there is no significant increase in PLR among APE patients compared to the healthy control group. There is no significant correlation between PLR and risk stratification indicators or thrombus load, and there is no significant change in PLR before and after treatment. Our findings do not support the notion that PLR has significant assessment value in APE. Compared to NLR, there is relatively less literature supporting the value of PLR in assessing APE severity and predicting mortality. Ertem et al's research shows that NLR is higher in APE patients who died compared to those who survived (P < .001), while there is no significant difference in PLR between the two groups (P = .241). 19 Ma et al found that NLR is an independent predictor of APE prognosis, while PLR is not. 20 The results of this study differ from some previous research. For example, Kurtipek et al's study showed that PLR in APE patients was significantly higher than that in the healthy control group (P < .05). 21 The study by Ozcan Cetin et al showed that PLR is significantly correlated with RVD/LVD, cTnI, and PAOI (P < .01). 22 Conversely, this study found that PLT in the APE group and subgroup A was significantly lower than that in the healthy control group, which may be related to platelet consumption and the use of heparin.
Unexpectedly, this study shows that there is no significant difference in NLR between the negative and positive groups for cardiac biomarkers (cTnI and NT-proBNP), and there is no significant correlation between NLR and risk stratification indicators or thrombus load. Our research indicates that NLR is not significantly correlated with right heart function damage caused by APE, or in other words, using NLR to reflect the severity of APE may not be advisable. The study by Akkus et al suggests that although NLR is higher in APE patients, there is no definitive relationship between NLR and the progression of APE. 23 Previous studies have shown that elevated NLR is associated with short-term or long-term mortality in many diseases such as intracerebral hemorrhage, 24 head and neck squamous cell carcinoma, 25 dermatomyositis, 26 dilated cardiomyopathy, 27 nasopharyngeal carcinoma, 28 chronic obstructive pulmonary disease, 29 etc. This precisely indicates that NLR reflects the overall inflammatory status of critically ill patients, rather than being a specific indicator of APE-related inflammation. Most deaths from APE are caused by underlying diseases such as infections, cancer, heart failure, and chronic lung diseases. The NLR is not very useful for predicting deaths directly attributed to APE, and an elevated NLR may primarily reflect an increase in underlying comorbidities that contribute to the risk of all-cause mortality. Our findings are not entirely consistent with some previous studies. For example, in the study by Soylu et al, the high NLR group had significantly higher RVD/LVD and cTnI levels compared to the low NLR group (P < .05). 6 This difference may be attributed to variations in the study populations. Of course, whether there is a correlation between NLR and risk stratification indicators or thrombus load, and whether NLR has prognostic value for mortality should be considered as two separate issues. For instance, Phan et al found that NLR was not correlated with RVD/LVD, troponin, or B-type natriuretic peptide, but an elevated NLR was associated with all-cause mortality (P < .01). 7
To our knowledge, there is currently no research on the changes in NLR and PLR before and after interventional treatment for patients with APE. In our study, compared to pre-treatment levels, NLR, cTnI, NT-proBNP, RVD/LVD, and PAOI were significantly reduced after treatment. This indicates that in terms of treatment response, NLR shows the same trend of improvement as risk stratification indicators and thrombus load, suggesting that monitoring the trend of changes in the inflammatory environment through NLR may help understand the response to treatment and whether patients with APE are recovering or deteriorating during hospitalization.
Interestingly, this study found that elevated NLR in patients with APE primarily reflects an increase in ANC, rather than a decrease in ALC. In subgroup A, the ANC was lower in the cTnI-negative group than in the positive group (P < .05). Our research suggests that using ANC instead of NLR as an indicator to assess the condition and treatment efficacy of APE may be a feasible approach.
In summary, NLR is elevated in patients with APE and decreases after effective treatment, indicating its potential use in assessing the condition and treatment efficacy. However, there is no correlation between NLR and risk stratification indicators or thrombus load. The study does not support a significant evaluative value of PLR for APE.
Limitations of this study: The small sample size precluded direct investigation of the relationship between NLR, PLR, and mortality. As a retrospective study, accurate PESI scores could not be obtained, and the correlation between NLR, PLR, and PESI could not be investigated.
Footnotes
Acknowledgements
None.
Author Contributions
Xiaojie Gao provided assistance in paper revision and review, as well as contributed to the analysis of some of the data. Huang Chen, Zhongjie Huang and Jianxiong Lin, as members of the research team, provided support for this study. Jinqi Huang managed and coordinated the entire retrospective study to ensure its smooth progress. Qihong Chen was responsible for data collection, analysis, and paper writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
This study was a retrospective analysis not requiring ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
None.