
Abstract
Objective
To investigate the relationship between C-reactive protein and albumin ratios (CAR) and all-cause and cardiovascular disease(CVD)-specific mortality in individuals with coronary heart disease(CHD).
Methods
The data from 1895 patients were extracted from the National Health and Nutrition Examination Survey (NHANES) database from 1999–2010. We used weighted COX regression analyses to explore the association between CAR, all-cause, and CVD-specific mortality. Restricted cubic spline(RCS) regression models and threshold effects analysis were used to analyze nonlinear relationships. Subgroup analyses were also performed to explore these relationships further.
Results
During a mean follow-up of 115.78 months, 61.48% of deaths occurred, and 21.85% were due to CVD. After adjusting for potential confounders, each 1-unit increase in CAR was associated with a 65% increase in all-cause mortality and a 67% increase in CVD-specific mortality. The RCS model revealed a non-linear association between CAR and the risk of all-cause mortality and CVD-specific mortality in CHD patients (all non-linear P < 0.001). Threshold effects analysis identified inflection points in regression models of all-cause mortality (0.04, P < 0.001) and CVD-specific mortality (0.05, P = 0.0024). The interaction tests found sex, smoking and diabetes influenced the association between CAR and all-cause mortality and sex, smoking and HF influenced its association with CVD-specific mortality (all P < 0.05).
Conclusion
There was a nonlinear association between CAR and all-cause mortality and CVD mortality in patients with CHD, with a higher hazard ratio before the inflection point. Sex, smoking, diabetes, and HF might have an effect on the associations between CAR and death risks.
Introduction
Coronary atherosclerotic heart disease (CHD) is a heart disease caused by atherosclerotic lesions in the coronary arteries that result in narrowing or blockage of the lumen of the arteries, causing myocardial ischemia, hypoxia, or necrosis. According to data from the American Heart Association, approximately 254.20 million people worldwide live with CHD and there were approximately 9.21 million deaths due to CHD. 1 Monitoring patients’ disease progression and early intervention to reduce patient mortality are necessary.
Inflammation plays an important role in lipid peroxidation, coronary atherosclerosis, and thrombosis.
2
The circulating C-reactive protein (CRP) produced by hepatocytes responds to the inflammatory state of the body and almost any form of tissue injury, infection or inflammation, and indeed also most forms of adverse non-physiological ‘stress’, are associated with increased circulating CRP values.
3
A study has confirmed that high baseline CRP was associated with subsequent risk of myocardial infarction and death in patients with chronic CHD.
4
Serum albumin is an excellent biomarker for predicting nutritional status and inflammation, and hypoalbuminemia is associated with increased all-cause and cardiovascular disease (CVD)-specific mortality in patients with CHD.3,5,6 Combining the two allows for a better assessment of inflammation in coronary artery disease and estimation of CHD patient prognosis. Recent research has demonstrated that C-reactive protein and albumin ratios (CAR) have been used in prognostic studies of myocardial infarction,7,8 heart failure (HF),
9
hypertension,
10
chronic obstructive pulmonary disease(COPD),
11
and cancer
12
with favorable results. Karabağ
However, previous studies are scarce on CAR on all-cause mortality and CVD-specific mortality in patients with CHD. In addition, the sample sizes of previous studies have been relatively small. This paper utilizes a larger sample size population from a public database to examine the association between CAR and elevated all-cause and CVD-specific mortality in patients with CHD.
Methods
Study Design and Participants
The baseline data was obtained from the National Health and Nutrition Examination Survey (NHANES). NHANES is a continuous cross-sectional survey with national representation and complex multi-stage sampling, aiming to assess the nutritional and health status of the non-institutionalized US population. 14 The survey provides much information on demographics, dietary nutrition, physical examination, laboratory examination, and medical history. We collected the information of the first interviewed participants between 1999 and 2010. Then we linked the National Death Index (NDI) of the National Center for Health Statistics (NCHS) to obtain the survival status of the participants and constructed a NHANES longitudinal follow-up cohort. The study was approved by the NCHS Ethical Review Board and all participants provided informed consent. So, no further ethical review or consent was required for our research.
Participants with CHD surveyed from 1999–2010 were included in the study. The number of subjects from 6 consecutive cycles(1999–2010) of the NHANES database was 62160. We excluded subjects who lacked follow-up time or were under the age of 18 years or did not have albumin or CRP data. Missing covariates were added using multiple interpolation methods. Finally, the study concluded with a total enrollment of 1895 subjects (Fig. 1).
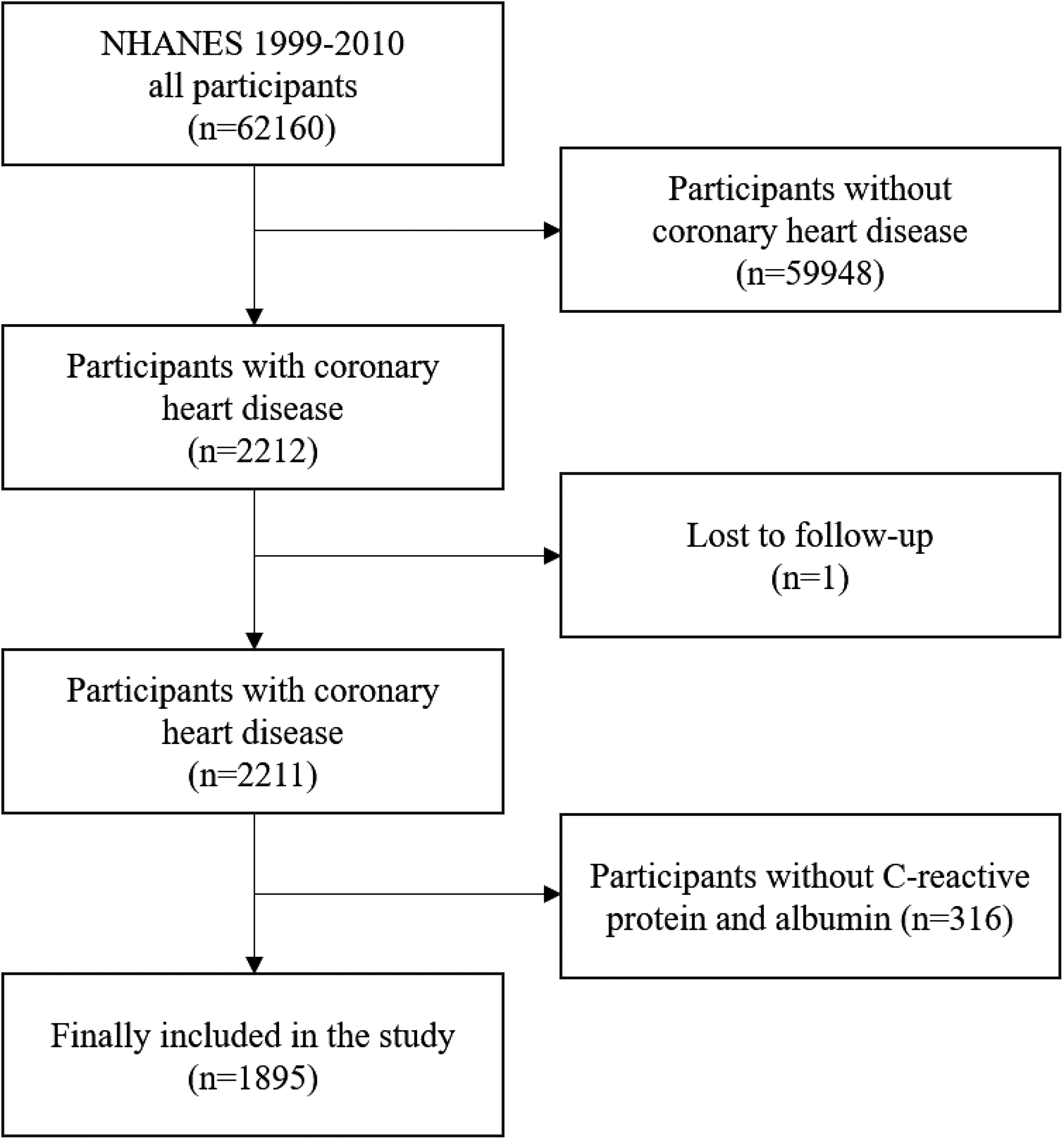
Flowchart of the patient selection process.
Definition of CAR and CHD
CAR was defined as serum CRP (mg/dL)/ serum albumin (g/dL). The history of CHD was obtained through interviews. CHD information was obtained by asking participants: “Has a doctor or other health professional ever told you that you had coronary heart disease?” or “Has a doctor or other health professional ever told you that you had a heart attack (also called myocardial infarction?” If they answered “Yes” to any of the above questions, they were diagnosed with CHD.
Covariates
Data of participants correlated with mortality and CHD were collected. Demographic data included age, gender, race, education level, marital status, and income-poverty ratio (PIR). Medical history information included HF, hypertension, diabetes, stroke, physical activity, body mass index (BMI), waist circumference, smoking, drinking, hypoglycemic therapy (hypoglycemic drugs and insulin), and use of lipid-lowering, antiplatelet, anticoagulants, antihypertensive prescription drugs. Data of strict laboratory analyses included estimated glomerular filtration rate (eGFR), hemoglobin A1c (HbA1c), high-density lipoprotein (HDL), total cholesterol, total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), uric acid, creatinine, hemoglobin, white blood cells count (WBC), lymphocyte count, monocytes count, platelet count. Physical activity was defined as at least 10 min of moderate or vigorous exercise within the past 30 days. 15 Subjects were defined as drinking if they consumed 12 alcoholic drinks in any of the past years. Smoking more than 100 cigarettes in a lifetime was defined as smoking.16,17 Hypertension was defined as self-reported physician-diagnosed hypertension, or a measured systolic blood pressure ≥130 mm Hg or diastolic blood pressure ≥90 mm Hg, diagnosed with hypertension or using antihypertensive agents. 18 The definition of diabetes was self-reported diagnosis, use of insulin or oral hypoglycemic agents, fasting glucose ≥ 7 mmol/L, or HbA1c ≥ 6.5%. 19 eGFR was calculated using the CKD-EPI formula with creatinine. 20
Ascertainment of Outcomes
The study outcomes were all-cause mortality and CVD-specific mortality. The information on mortality in the NHANES in 1999–2010 was linked to mortality data from the NDI death certificate records (www.cdc.gov/nchs/data-linkage/mortality-public.htm) until December 31, 2019, matched using a probabilistic matching algorithm to identify mortality status. The definition of CVD-specific mortality was based on the International Classification of Diseases, 10th Revision (ICD-10). 21
Statistical Analysis
Because of the multi-stage stratified sampling design of NHANES, weights were given to the statistical analyses when they were conducted. For continuous variables, the variables were displayed as the mean ± standard deviation, while the categorical variables were presented as counts and percentages (%). An F-test or a Kruskal-Wallis test was conducted to compare the continuous variables between groups. Depending on the circumstance, Pearson's chi-squared test or Fisher's exact test was used to compare categorical variables.
According to the STROBE statement, 22 we built three models to investigate associations between CAR and all-cause mortality and CVD-specific mortality in CHD patients by weighted COX regression analyses. And based on previous studies,14,17 some covariables were selected as possibly having an effect on mortality in patients with CHD. Variables were not adjusted in Model 1. Age, gender, and race were adjusted in Model 2. Age, gender, race, education level, marital status, PIR, BMI, waist circumference, physical activity, HF, stroke, hypertension, diabetes, smoking, drinking, eGFR, HDL, total cholesterol, lipid-lowering drug, antiplatelet agents, anticoagulants drug, antihypertensive drug, and hypoglycemic therapy were adjusted in Model 3. Kaplan-Meier curves were used to estimate the survival of different CAR groups at different time points and two plots were made according to all-cause mortality and CVD-specific mortality. The log-rank test was used to determine whether the differences between CAR quartiles were statistically significant. Then restricted cubic splines (RCS) regression models were used to study the potential nonlinear relationship between CAR and all-cause mortality and CVD-specific mortality. Besides, threshold effect analysis was applied to find an inflection point using a two-part COX regression model. Finally, subgroup analyses were performed to explore interactions with CAR in Model 3, stratified by age, sex, BMI, HF, diabetics, hypertension, drinking, and smoking.
Hazard ratio (HR) and 95% confidence interval (95% CI) were applied in the association analysis. Two-sided
Results
General Characteristics of Participants
Study subjects ranged in age from as young as 20 to as old as 85. Most participants were male (66.65%) and Non-Hispanic White (65.33%), with a mean age of 68.09 years. During a mean follow-up time of 115.78 months, 61.48% of deaths occurred, and 21.85% were due to CVD. Males, married, smokers and patients with high BMI were prone to have a higher CAR. Subjects with high CAR might have the presence of higher rates of HF, stroke, and hypertension, and have higher levels of uric acid, creatinine, monocyte count, and low levels of total bilirubin. Users of lipid-lowering drugs, anticoagulants, glucose-lowering drugs, and insulin tended to have a higher CAR (all
Baseline Characteristics of Included Participants by CAR Quartile.
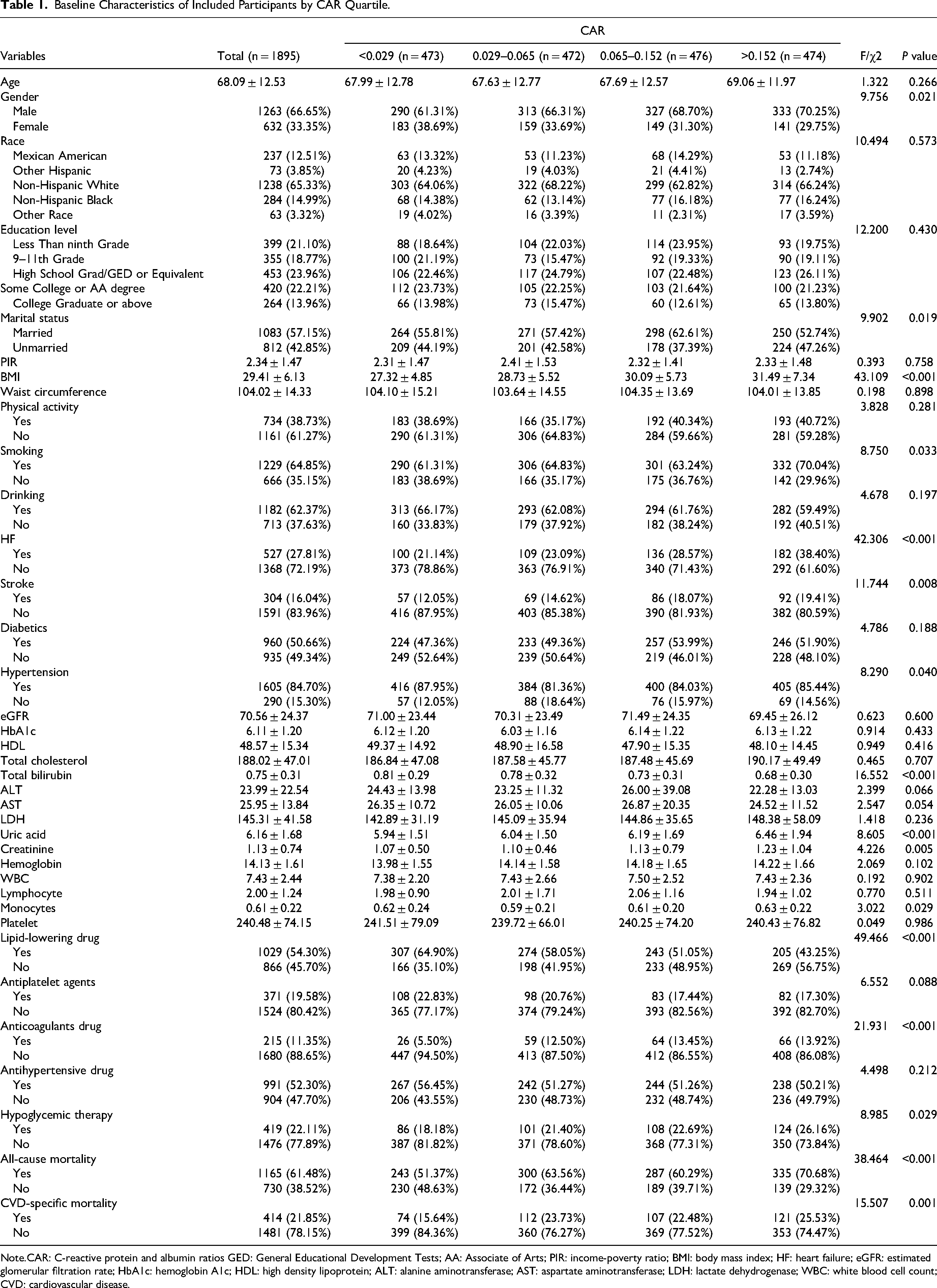
Note.CAR: C-reactive protein and albumin ratios GED: General Educational Development Tests; AA: Associate of Arts; PIR: income-poverty ratio; BMI: body mass index; HF: heart failure; eGFR: estimated glomerular filtration rate; HbA1c: hemoglobin A1c; HDL: high density lipoprotein; ALT: alanine aminotransferase; AST: aspartate aminotransferase; LDH: lactate dehydrogenase; WBC: white blood cell count; CVD: cardiovascular disease.
Association Between CAR and all-Cause and CVD-Specific Mortality
As shown in Table 2 and Table 3, CAR is significantly associated with all-cause (
Association Between CAR and all-Cause Mortality.
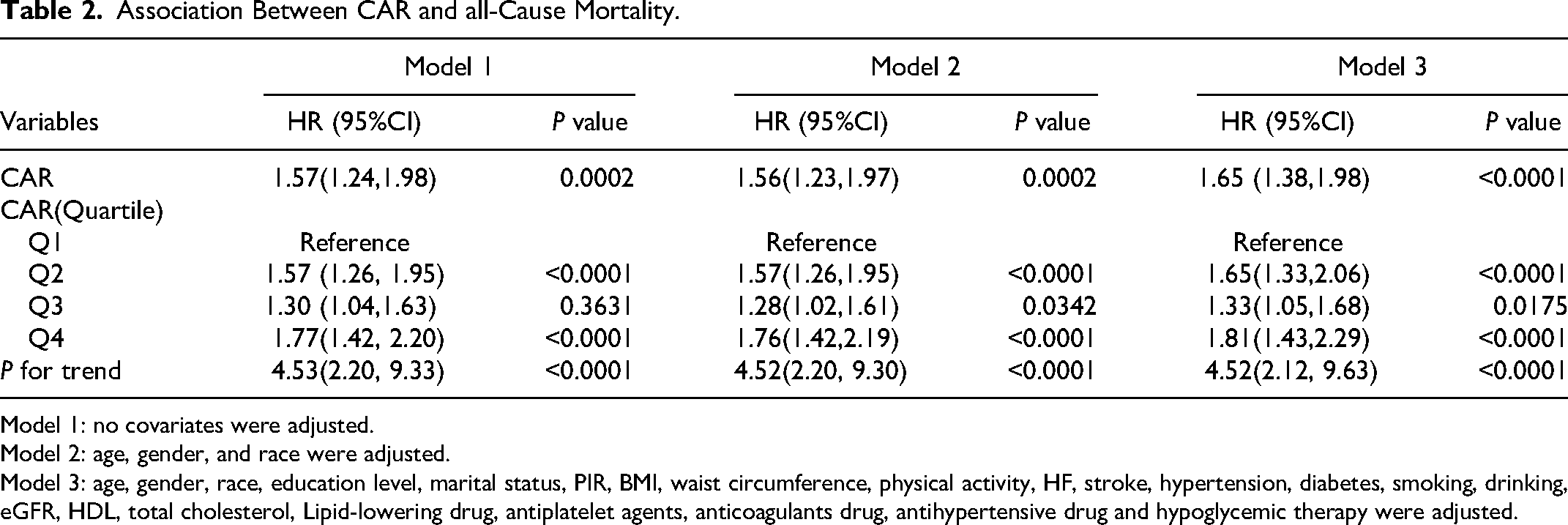
Model 1: no covariates were adjusted.
Model 2: age, gender, and race were adjusted.
Model 3: age, gender, race, education level, marital status, PIR, BMI, waist circumference, physical activity, HF, stroke, hypertension, diabetes, smoking, drinking, eGFR, HDL, total cholesterol, Lipid-lowering drug, antiplatelet agents, anticoagulants drug, antihypertensive drug and hypoglycemic therapy were adjusted.
Association Between CAR and CVD-Specific Mortality.
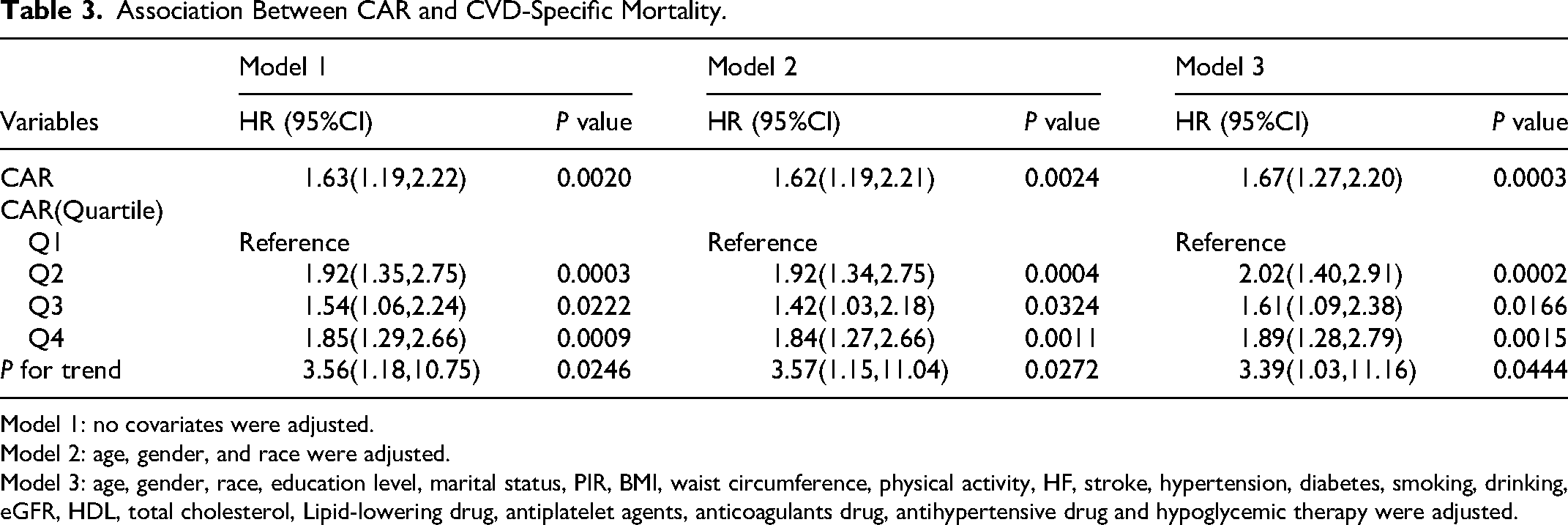
Model 1: no covariates were adjusted.
Model 2: age, gender, and race were adjusted.
Model 3: age, gender, race, education level, marital status, PIR, BMI, waist circumference, physical activity, HF, stroke, hypertension, diabetes, smoking, drinking, eGFR, HDL, total cholesterol, Lipid-lowering drug, antiplatelet agents, anticoagulants drug, antihypertensive drug and hypoglycemic therapy were adjusted.
The Kaplan–Meier curve shows the change in the survival status of patients with CHD by quartiles of CAR over time. The group with the larger CAR had a higher mortality rate at the same follow-up time than the group with the smaller CAR(Fig. 2). The restricted cubic splines regression model revealed a non-linear association(all non-linear
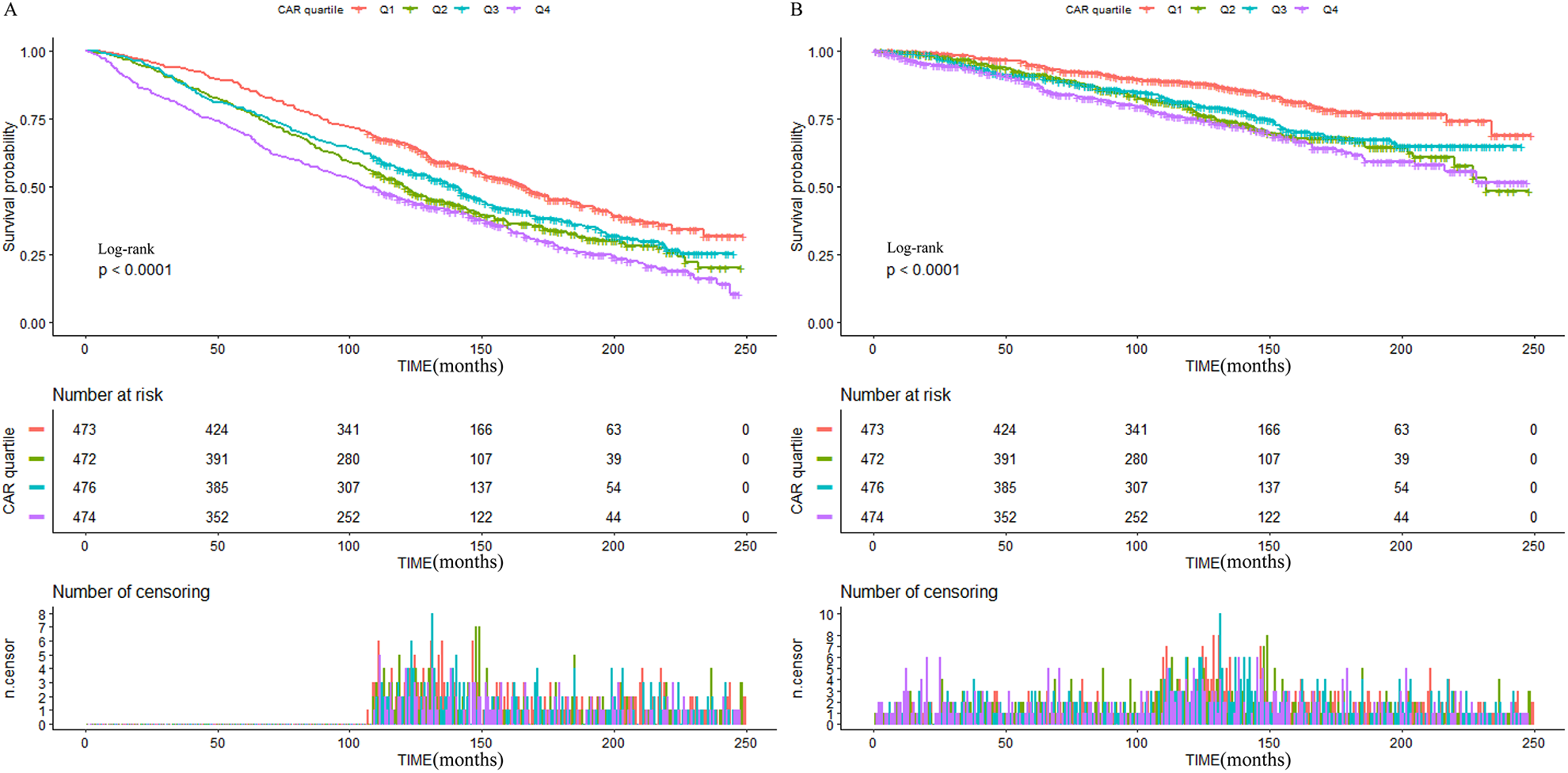
Kaplan–Meier curves for all-cause
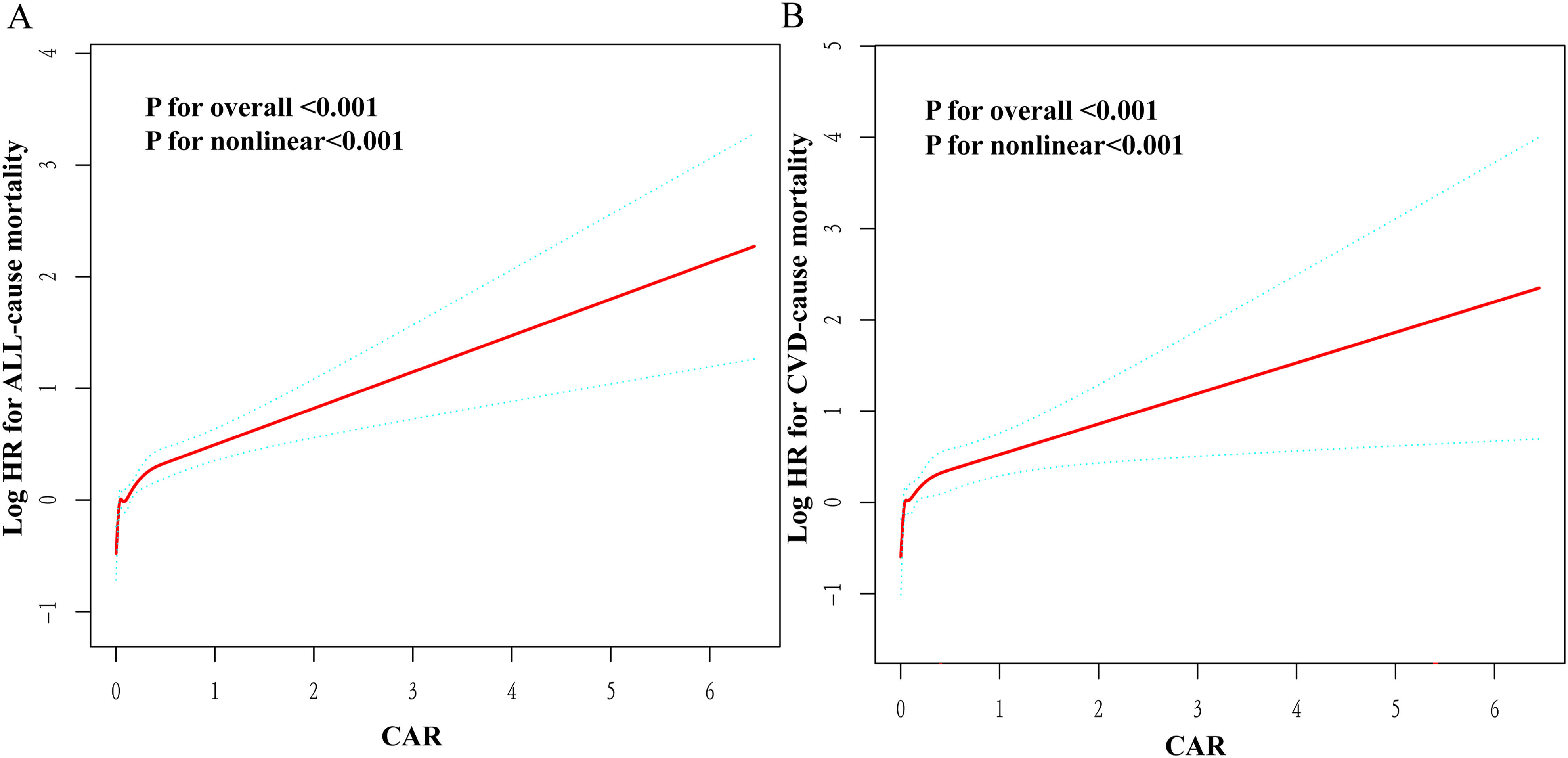
Nonlinear relationship between CAR and all-cause and CVD-specific mortality. The red line in the figure represents Log(HR), and the blue line represents the 95% confidence interval. (A) all-cause mortality, (B) CVD-specific mortality.
Relationships of CAR and all-Cause Mortality and CVD-Specific Mortality in Different Subgroups
As shown in Table 4, after correcting for covariates other than grouping variables, the association between CAR and all-cause mortality is not significant in the BMI 24–28 subgroup. Similarly, analyses of the relationship between CAR and CVD-specific mortality were also not significant in the non-smoking subgroup, the non-HF subgroup, and the non-hypertensive subgroup (all
Subgroup Analysis of the Relationship Between CAR and all-Cause and CVD-Specific Mortality.
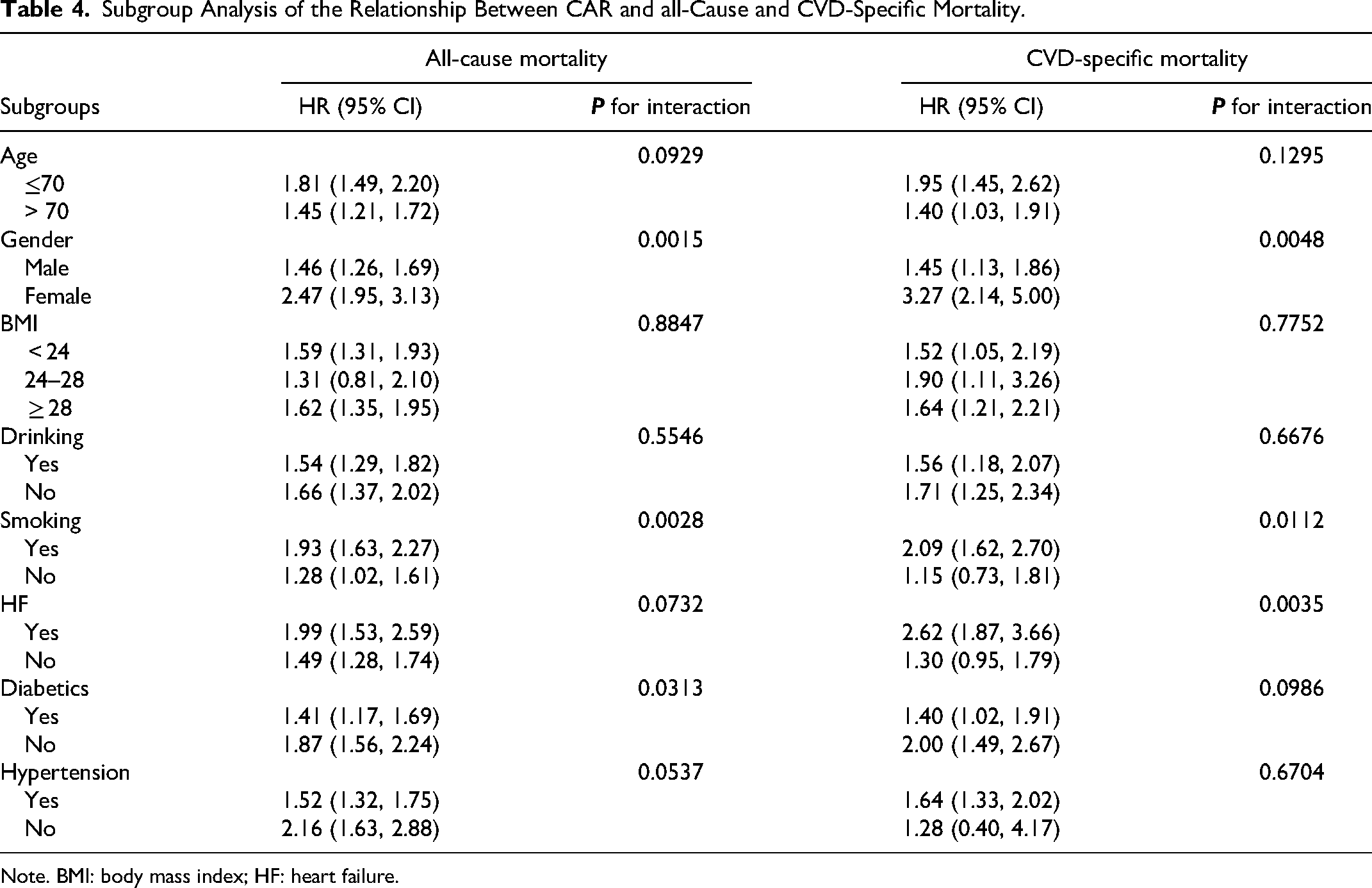
Note. BMI: body mass index; HF: heart failure.
Discussion
In this study, we explored the association between CAR and all-cause mortality and CVD-specific mortality in patients with CHD. The RCS regression models showed a nonlinear association between CAR and elevated all-cause and CVD-specific mortality in patients with CHD after adjusting for the covariates. The interaction tests implicated sex, smoking, diabetes, and HF may affect the aforementioned associations.
Inflammation takes an upmost role in the atherosclerotic process. Pathogenic factors such as low-density lipoprotein (LDL) lead to vascular endothelial damage, which induces a local inflammatory response, and endothelial cells secrete vascular cell adhesion molecules and monocyte chemoattractant protein 1 (MCP-1), which induces monocyte adhesion. 23 Monocytes migrate to the subendothelial lumen and differentiate into macrophages, which convert into foam cells by phagocytosis of oxidized LDL and form lipids. Foam cells secrete chemokines to recruit more macrophages, mast cells, and T cells. Macrophages, mast cells, T cells, and B cells migrate toward the endothelium and secrete large amounts of chemokines such as inflammatory factors, tumor necrosis factor, and MCP-1, which promote a sustained inflammatory response as well as atheromatous plaque formation. 24 Under the combined effect of immune cells, inflammatory factors, and cytokines, matrix metalloproteinases are produced and activated, stimulating fibrous cap reabsorption, leading to rupture of atherosclerotic plaques, causing aggregation of coagulation factors and platelets, and the formation of arterial thrombus, which leads to myocardial infarction and heart attack. 25 CRP is a downstream marker of inflammation that has emerged as a major risk factor for CHD. 26 But CRP and albumin may influence the prognosis of patients with CHD not only by inflammatory mechanisms. CRP has been reported to have pro-atherosclerotic properties by upregulating angiotensin type-1 receptor expression, affecting the renin-angiotensin system and contributing to the pathogenesis of CHD. 27 Serum albumin not only reflects the patient's nutritional status but also exhibits anti-inflammatory, anticoagulant, and antiplatelet aggregation effects. Hypoalbuminemia can compromise serum antioxidant activity and impair endothelium-derived relaxing factor-like activities. 28 Additionally, hypoalbuminemia may contribute to the worsening of ischemic heart disease by favoring myocardial edema. 29
Our results supported the findings of the previous study. Sabanoglu
Our study demonstrates an exponentially increasing relationship between CAR and mortality before the inflection point and a relatively flat relationship after the inflection point. This may be because at the beginning of the inflammatory cascade response burst has a strong effect on mortality, and when fully initiated the mortality-related blood glucose lipids blood pressure, and whether or not antiplatelet medication lipid-lowering medication is taken limit the effect on mortality increase, but this does not negate the effect of inflammation and nutritional status on mortality.
In our subgroup analysis study, some positive results of the interaction test are to be discussed. Women have a more significant association than men. The mechanism of this phenomenon is unclear and may be related to the specific physiology structure of women and their greater responsiveness to inflammation. Women may be more likely to feel stress and stress may contribute to the progression of CHD through inflammation.
33
Fiechter
To the best of our knowledge, this study was the first to explore the nonlinear relationship between CAR and all-cause and CVD-specific mortality in patients with CHD in a U.S. population using a large public database. We used several models to show the significant nonlinear relationship between the above two and employed threshold analysis as well as subgroup analysis to further characterize the relationship. More prospective multicenter studies are needed in the future to validate the predictive power of CAR. In the clinical setting, CRP and albumin derived from routine blood tests are affordable and easily available. CAR may be able to serve as an effective adjunct to prognostic assessment and risk stratification of CHD patients. However, some limitations need to be considered in our study. First, because this is a retrospective study, retrospective bias and selective bias may arise. Second, samples with the deletion of CAR variables missing follow-up data, and interpolation of missing data may affect the results of the study. Third, because of the database data limitations, it is impossible to study the relationship between the dynamic change of CAR over time or the average level and mortality over time. Fourth, some covariates are not suitable to be filled in by interpolation or simply deleted due to missing data as well as there may be unknown covariates affecting the results of the study, so perhaps confounding factors cannot be completely excluded. Fifth, absence of information on PCI and coronary artery bypass grafting resulting from the limitation of the database might result in some bias because the measures could affect prognosis of patients. Sixth, the diagnosis of CHD in the study is based on responses to a medical health questionnaire rather than objective examination. Finally, our study was conducted in Americans, so whether the findings apply to other populations still requires further study.
Conclusion
There was a nonlinear association between CAR and all-cause mortality and CVD-specific mortality in patients with CHD, with a higher HR before the inflection point. In subgroup analyses, there were interactions with CAR for sex, smoking, HF, and diabetes. In the future CAR may be an effective aid in assessing the prognosis of patients with CHD.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241271382 - Supplemental material for Non-linear Association of CAR with all-Cause and Cardiovascular Mortality in Coronary Heart Disease: A Retrospective Cohort Study from NHANES
Supplemental material, sj-docx-1-cat-10.1177_10760296241271382 for Non-linear Association of CAR with all-Cause and Cardiovascular Mortality in Coronary Heart Disease: A Retrospective Cohort Study from NHANES by Ming Ye, Guangzan Yu, Fusheng Han and Hua He in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
Not applicable.
Authors’ Contributions
M. Y, GZ. Y, and FS. H contributed to the study conception and design and writing the manuscript. M. Y, GZ. Y and FS. H performed data collection and analysis. M. Y, GZ. Y and FS. H and H. H commented on the research design, data analysis, writing the manuscript, and supervision of the study. H. H gave the final approval of the manuscript submission. All authors contributed to the article and approved the submitted version.
Availability of Data and Materials
Consent for Publication
Not Applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The NHANES study protocols were approved by the National Center for Health Statistics institutional review board, and all participants provided written consent at enrollment. This study is from a public database, so no approval number is required.
Funding
The work was supported by the Beijing Natural Science Foundation of China (7202037).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.