
Abstract
Post-thrombotic syndrome (PTS) is one of the most common long-term complications of lower extremity deep vein thrombosis (DVT). In order to study the long-term adverse prognosis of patients with DVT, explore the influencing factors for the prognosis of DVT, and provide a reliable reference for future research in the field of venous thrombosis, we collected and summarized information about the incidence of PTS, the PTS score and grading, the associated symptoms and drug-related adverse reactions in 501 patients with DVT. In our study, 54.1% of patients with DVT (271 of 501) experienced indications and manifestations of PTS, the male to female ratio was approximately 1:1. During the long-term follow up, the most common symptoms of PTS were anterior tibial edema and pain. By statistical analysis, we found that the outcome of thrombosis was the influencing factor of PTS score (1-4 points, P<.05). The grading of PTS was primarily influenced by the history of varicose veins and DVT in the lower extremities. The duration of taking antithrombotic drugs affected the outcome of thrombosis (P<.05), especially among the female patients. In addition, varied factors, such as lower extremity DVT complicated with pulmonary embolism and the duration of antithrombotic drug use were found to increase the chances of experiencing drug-related adverse reactions (odds ratio [OR]=2.798, 95% confidence interval [CI]: 1.413-5.541 / OR=2.778, 95% CI: 1.231-6.269). The above 2 factors were significant only among female patients with DVT (OR=4.03, 95% CI: 1.608-10.103 / OR=3.918, 95% CI: 1.123-13.669).
Keywords
Introduction
Deep venous thrombosis (DVT) is a condition in which blood clots abnormally in the deep venous lumen for various reasons and forms emboli, thereby blocking the venous lumen and leading to blood reflux disorder. DVT usually occurs in the deep veins of the legs, but can also occur in the arms, mesentery, and brain veins. Clinically, DVT is often misdiagnosed due to hidden symptoms, resulting in various complications like limb pain, venous valve deficiency, lower limb swelling, and occasionally venous ulcer. If the embolus detaches and blocks the pulmonary artery or its branches, it results in the formation of pulmonary embolism (PE). In more severe cases, the condition may be complicated with PE, which can be life-threatening. Therefore, once DVT is diagnosed, it is crucial to administer standardized anticoagulant therapy without obvious contraindications to anticoagulation. According to a guideline published by the European Societyment of Vascular Medicine,1,2 despite receiving standardized anticoagulation treatment, patients with DVT are at an elevated risk of experiencing the long-term adverse event known as post-thrombotic syndrome (PTS). It is an important and common long-term adverse event in proximal DVT within the first 2 years, with incidence ranging from 20% to 50%.3,4 At present, the international research on PTS mainly focuses on prevention after DVT,5,6 the diagnosis and management of PTS. 7 A variety of measurements including the Villalta scale and the Venous Clinical Severity Score have been used to diagnose and grade PTS severity in the clinical setting and in the literature. 8 Quality of life (QoL) and long-term prognosis were assessed by validated disease-specific (VEINES-QOL) and generic health-related (SF-36) questionnaires. 2 However, there have been no systematic, comprehensive studies on the QoL and long-term outcomes of patients with PTS, especially those with mild cases. In addition, China and other countries exhibit significant disparities in terms of race, geography, and lifestyle. Therefore, it is vital to conduct a thorough investigation and assessment of the prognosis of patients with DVT in China.
Although thrombosis can occur anywhere in the venous system, it usually forms at the location of injury or blood stasis, especially at the tip of the venous sinus of the calf vein. Upper extremity DVT (UEDVT) accounts for only 4% to 10% of all cases of DVT, 1 and approximately 90% of the DVT occurs in the lower limbs. 2 Based on this, 501 patients with lower extremity DVT were selected in this study. We carefully gathered information on the detailed survival status of the patients through long-term follow up and ultimately summarized the adverse prognosis events.
Research Methods
Data Collection
According to the inclusion and exclusion criteria, we conducted a comprehensive search among patients admitted to the Affiliated Hospital of Nantong University between January 1, 2012 and December 31, 2019. Among these patients, we carefully selected 501 individuals who had been diagnosed with lower extremity DVT using both color Doppler ultrasound and angiography. Detailed survival status was obtained by telephone follow up, and the follow-up deadline was February 26, 2022.
Inclusion criteria considered were as following: (1) they must meet the diagnostic criteria for DVT as outlined in the 2018 guidelines by the American Society of Hematology for management of venous thromboembolism: Diagnosis of Venous Thromboembolism 9 ; (2) they must have developed DVT for the first time; (3) the site of thrombosis was lower extremity; and (4) patients who were willing to be tracked for follow-up purposes.
Exclusion criteria: (1) patients with thrombosis in other parts of the body except the lower limbs; (2) previous history of venous thromboembolism (VTE); (3) patients who refused treatment or were discharged automatically due to personal reasons during hospitalization; (4) patients with missing or incomplete medical records; and (5) patients with incomplete follow-up data or those who declined to participate in follow up.
Follow-up data: Duration of antithrombotic drug treatment after discharge; various adverse drug reactions (abdominal pain, gastrointestinal bleeding, hematochezia, gingival bleeding, and other bleeding); symptom of PTS (pain, spasm, heaviness, paresthesia, pruritus, pretibial edema, sebum sclerosis, pigmentation, flushing, venous dilatation, calf compression pain, skin ulcer) 3 ; PTS score (0-33 points); PTS grading (categorized as none, mild, moderate, and severe); re-examining B-scan ultrasonography of lower extremities; outcome of thrombosis (dissolution, organization, and progression); monitoring for recurrent DVT (including recurrence time, location, presence of PE, and treatment method); determination of use of hormones or not (contraceptives, hormone replacement therapy, testosterone therapy, etc); specific effects on QoL (pain in the affected limb, walking condition, etc); and death (cause of death, DVT related, or not).
Ethical review: This study was reviewed and approved by the Ethics Committee of the Affiliated Hospital of Nantong University. The review number assigned was: 2022-K018-01.
Data Analysis
SPSS 26.0 statistical software was used for the data analysis. The rate or constituent ratio (%) of count data was expressed by Chi-square test or Fisher's exact test. The measurement data was expressed as mean± standard deviation (mean± SD) and analyzed by Student's t test. Rank-sum test was used for comparison between the groups in univariate analysis and binary unconditional or ordered logistic regression was employed for multivariate analysis. P<.05 was considered as statistically significant.
Results
Enrolled population and the included follow up: A total of 749 patients with DVT were admitted to the Affiliated Hospital of Nantong University from January 1, 2012 to December 31, 2019. After reviewing the medical records, a total of 67 patients were excluded according to the inclusion and exclusion criteria. After screening, 682 patients were contacted via telephone for further evaluation. Among these, 108 had passed away due to reasons unrelated to DVT, while 73 patients were unable to be reached for follow up, representing a percentage of 10.7%. Finally, a total of 501 patients with lower extremity DVT were included in the study and the data was analyzed (Figure 1).
Overall prognosis: Among all 501 patients with DVT, (1) more than half of the patients experienced PTS symptoms and signs (271 of 504, 54.1%). Additionally, among these patients, 151 were female (151 of 501, 30.1%) and 120 were male (120 of 501, 24.0%). According to the Villalta grading criteria, 10 451 patients showed no signs of PTS, while 30 patients experienced mild PTS, 3 patients had moderate PTS, and 6 patients had severe PTS. (2) There were 62 patients who experienced adverse reactions of antithrombotic drugs. (3) There were 24 patients with recurrent DVT and the recurrence rate was observed to be 4.79%. (4) There were 11 cases of DVT-related death, with a mortality rate of 2.2% (including 2 cases of recurrent DVT complicated with PE).
PTS-related symptoms and signs: Among the 271 patients with symptoms and signs of PTS, more than half of the patients had symptoms of limb swelling after physical activity (142 of 271, 52.4%), whereas 56 patients reported limb pain in cold weather (56 of 271, 20.7%). Other symptoms that affected the QoL included: inability to walk long distances (37 of 271, 13.7%), using crutches for daily walking (14 of 271, 5.2%), slower speed of stair climbing (12 of 271, 4.4%), appearance of persistent skin ulcers on the lower extremities (6 of 271, 2.1%), inability to walk (4 of 271, 1.5% (Figure 2).
According to the Villalta scoring standard, 271 patients experiencing symptoms underwent assessment, with their symptom and sign severity assigned scores ranging from 1 to 21. The scores were mainly concentrated in the 1 to 4 zones, as displayed in Table 1: According to the Villalta scoring criteria, PTS was classified as absence of PTS (0-4 points), mild PTS (5-9 points), moderate PTS (10-14 points), and severe PTS (15-33 points). The results of statistical analysis indicated that most of the patients were “PTS free” patients (451 of 501, 90.0%), including 246 females and 205 males. There were 30 patients with “mild PTS,”accounting for 6% (14 males, 6.1%; 16 females, 5.9%). There were 3 patients with “moderate PTS,” making up for 0.6% (1 male, 0.4%; 2 females, 0.7%). There were 6 patients with “severe PTS,” accounting for 1.2% (5 males, 2.2%; 1 female, 0.4%). A total of 11 patients died, accounting for 2.2% (6 males and 5 females), as shown in Figure 3.
The relationship between the outcome of thrombosis and PTS score and grading: Among all 501 patients, 294 (294 of 501, 58.7%) returned for follow-up examinations after being discharged among which 150 (150 of 294, 51%) were females and 144 (144 of 294, 49%) were males. Thrombolysis occurred in 77.6% of 294 patients (228 of 294), 80.7% of women (121 of 150) and 74.3% of men (107 of 144). A thrombus formed in 16.3% (48 of 294) of all patients, with higher rates observed among females at 12.7% (19 of 150), compared to males at 20.1% (29 of 144). 6.1% (18 of 294) of the patients experienced thrombosis progression, among which 55.6% (10 of 18) were the female patients and 44.4% (8 of 18) were the male patients.
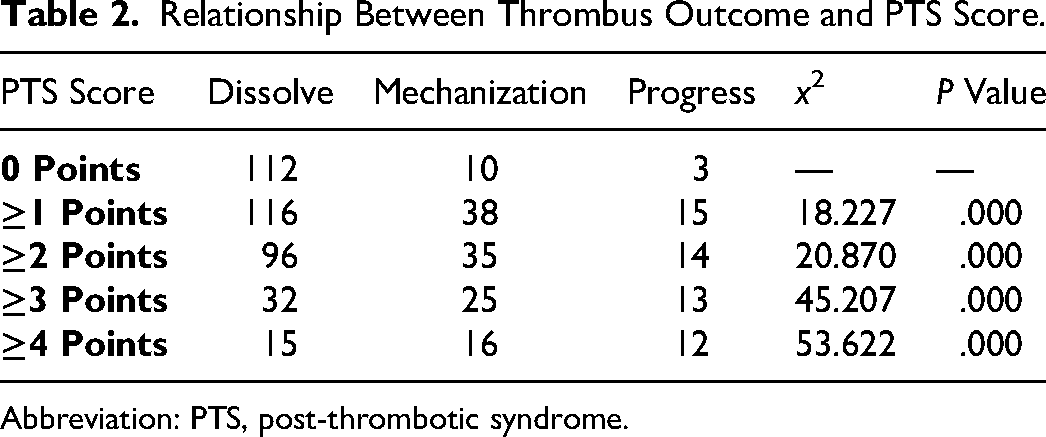
The study found that the severity of thrombosis significantly influenced the PTS score (1-4 points), that is, PTS score ≥1, ≥2, ≥3, and ≥4 points were all affected by the outcome of thrombosis and the difference was statistically significant (P<.05) (Table 2).
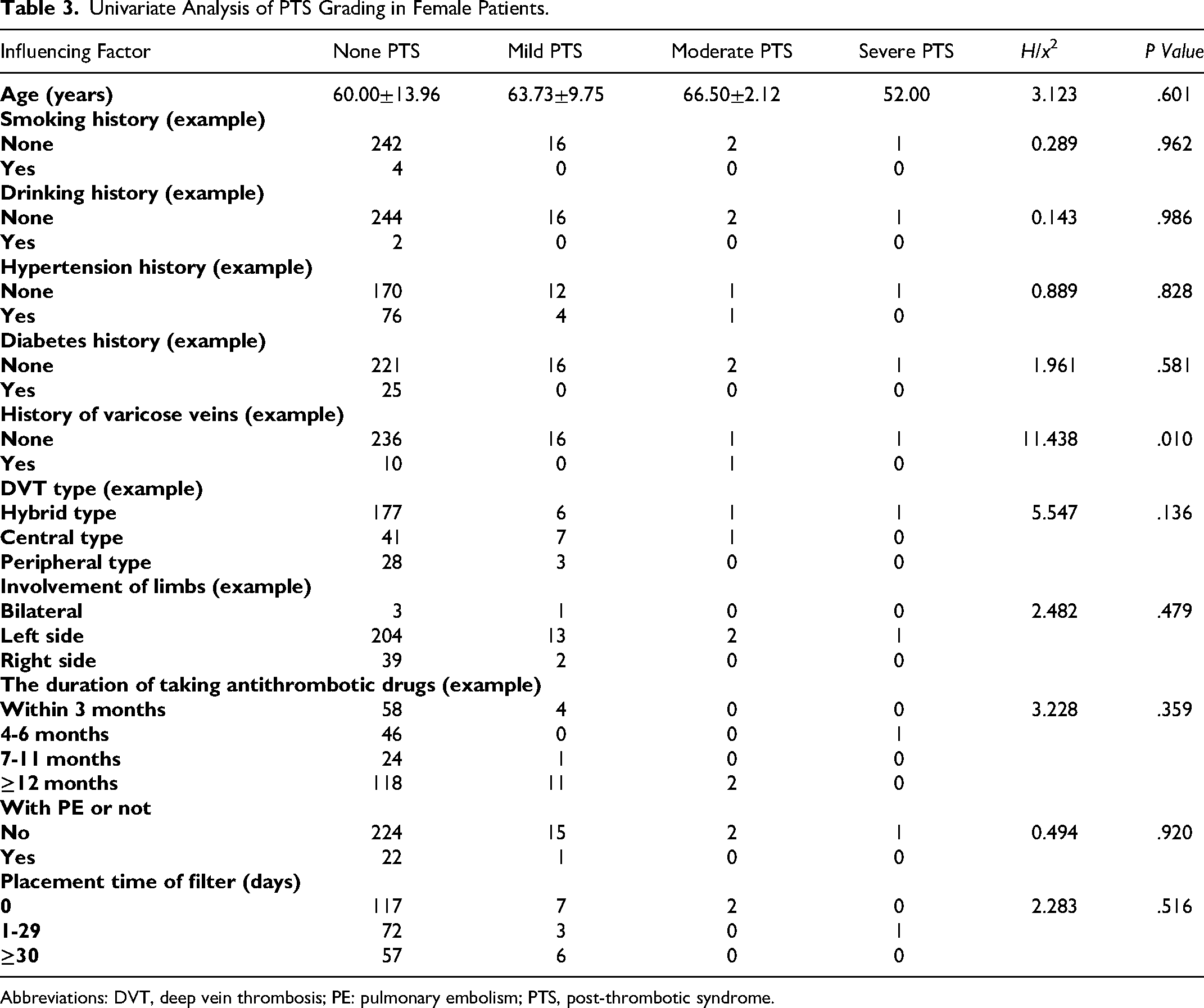
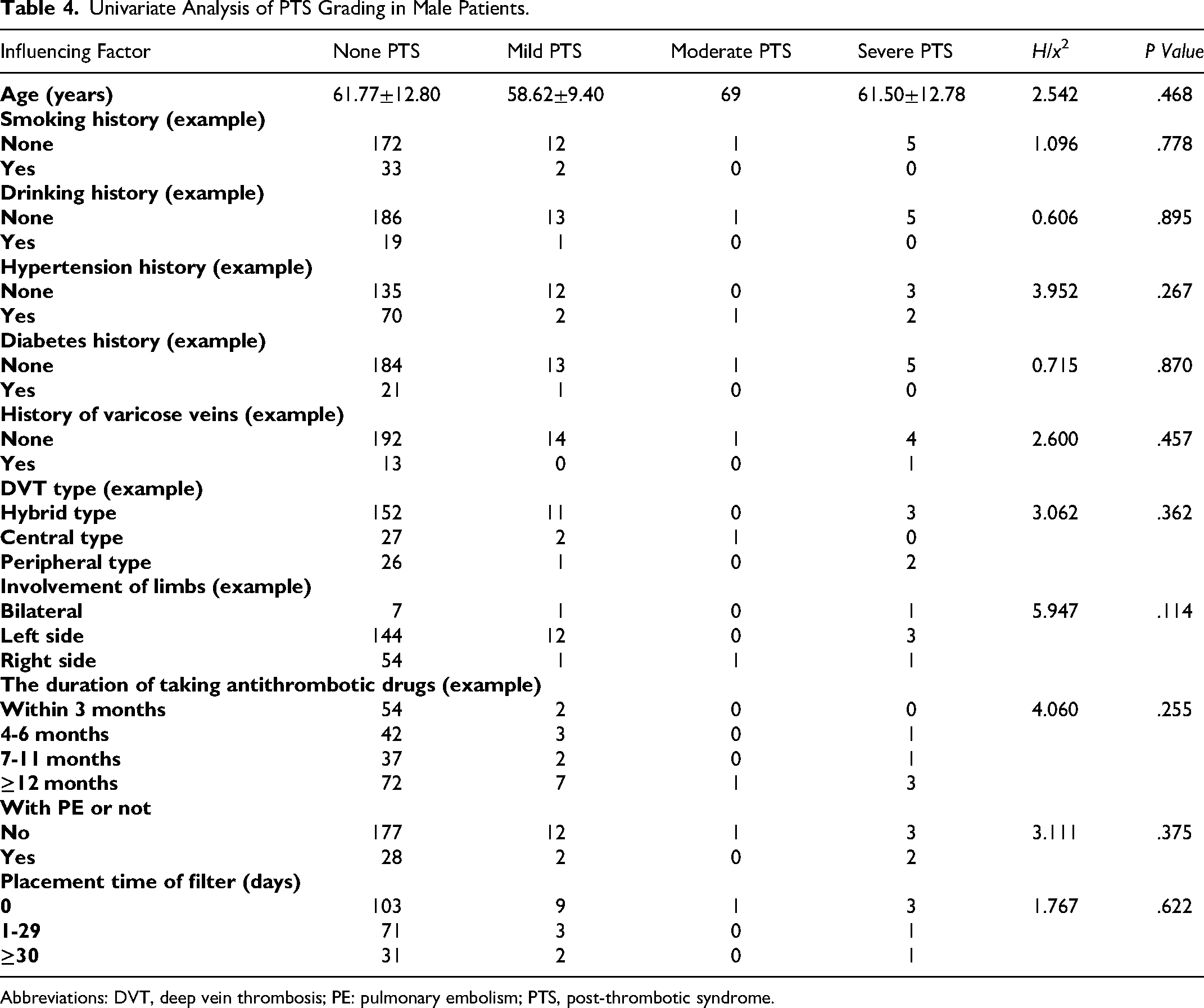
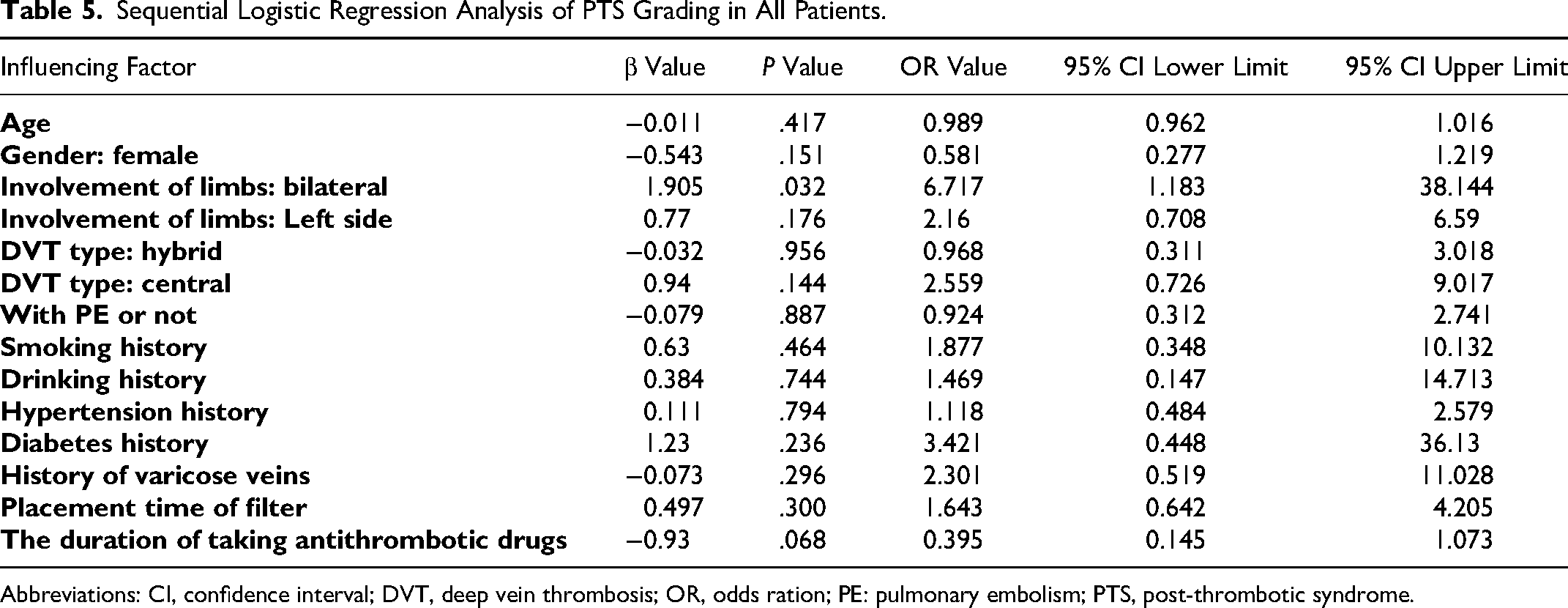
The relationship between the history of lower extremity varicose veins, bilateral lower extremity DVT and PTS score as well as grading: The results of univariate analysis of the enrolled patients revealed that for female patients, history of lower extremity varicose veins was a key factor affecting PTS grading, and the difference was statistically significant (P<.05) (Table 3). While in male patients, all the factors had no significant impact on PTS grading, with no statistical significance (P>.05) (Table 4). The results of multivariate ordered logistic regression analysis for all patients indicated that PTS rating was significantly correlated with bilateral lower limb DVT (odds ratio [OR]=6.717, 95% confidence interval [CI]: 1.183 ∼ 38.144) (Table 5).
Analysis of factors affecting thrombosis outcome: The analysis results of 150 female patients who were re-examined with B-ultrasound of lower limbs showed that the duration of antithrombotic drug use had a significant impact on thrombus outcome, with statistical significance (P<.05), as shown in Table 6, the details are shown in Supplemental materials. Among 144 male patients who were re-examined for B-ultrasound of lower limbs, there was no statistical significance in all influencing factors on thrombus outcome (P>.05), as shown in Table 7, the details are shown in Supplemental materials.
Analysis of factors affecting adverse reactions of antithrombotic drugs: Of all 501 patients, 62 patients experienced antithrombotic adverse reactions, with an incidence of 12.4%. Among 270 female patients, the probability of adverse reactions to antithrombotic drugs in patients with DVT of lower limbs combined with PE was significantly higher than that in patients without PE (4.03 times), and the difference was statistically significant (OR=4.03, 95% CI: 1.608-10.103) (Table 8, the details are shown in Supplemental materials). The probability of adverse reactions in female patients taking antithrombotic drugs for 4 to 6 months was 3.918 times higher than that in female patients taking antithrombotic drugs for 3 months, and the difference was statistically significant (OR=3.918, 95% CI: 1.123-13.669) (Table 9, the details are shown in Supplemental materials). According to the data analysis results, among 231 male patients, age, smoking history, drinking history, hypertension history, diabetes history, varicose vein history, type of DVT and involvement of limbs, time of taking antithrombotic drugs, and whether PE was combined had no significant impact on adverse drug reactions, with no statistical significance (P>.05) (Table 10, the details are shown in Supplemental materials).
Recurrence of DVT: After follow up, it was discovered that a total of 24 patients experienced a recurrence of DVT. Overall, the recurrence rate was determined to be 4.79% (24 of 501), including 11 females (11 of 270, 4.07%), and 13 males (13 of 231, 5.62%). The median time to recurrence was 6 years after the diagnosis and treatment of DVT. According to the site of recurrence, there were 16 instances of ipsilateral lower extremity DVT recurrence (9 females and 7 males), including 2 cases of inferior vena cava filter blockage (both were found in females). There were 6 cases of contralateral lower extremity DVT recurrence (2 were observed in females and 4 were observed in males). In addition, recurrent thrombosis in males involved bilateral lower limbs in 1 case and mesenteric vein in 1 other case. Among the 16 patients with recurrent DVT in the ipsilateral lower extremity, there were 9 cases of mixed DVT (4 were found in females and 5 were found in males), 6 cases of central DVT (5 were observed in females and 1 was observed in male), and 1 case of peripheral DVT (male).
Mortality: According to the results of relevant auxiliary examination and autopsy, the death of 11 patients was associated with DVT diagnosis. Ten of them died of pulmonary embolism as the direct cause of death, and only 1 patient died of systemic bleeding caused by antithrombotic drugs and ineffective treatment. The distribution of time of death (since the first diagnosis of DVT) ranged from half a month to 5 years, as shown in Figure 4. The age of all the deceased patients ranged from 61 to 83 years old, with an average of (73.36±7.47) years old, including 5 females and 6 males. All the 11 patients had a mixed type of initial DVT, including 8 cases of left lower extremity DVT and 3 cases of right DVT. Only 1 case experienced complications involving PE. Two patients experienced recurrent DVT, with both instances occurring in the ipsilateral deep vein. One of them experienced a relapse after being diagnosed and successfully treated for the first DVT, but pulmonary embolism occurred 4 years later after the cure of recurrent DVT, and finally died. The other patient had recurrent DVT 5 years after the first diagnosis and cure, and died of PE at the same time.
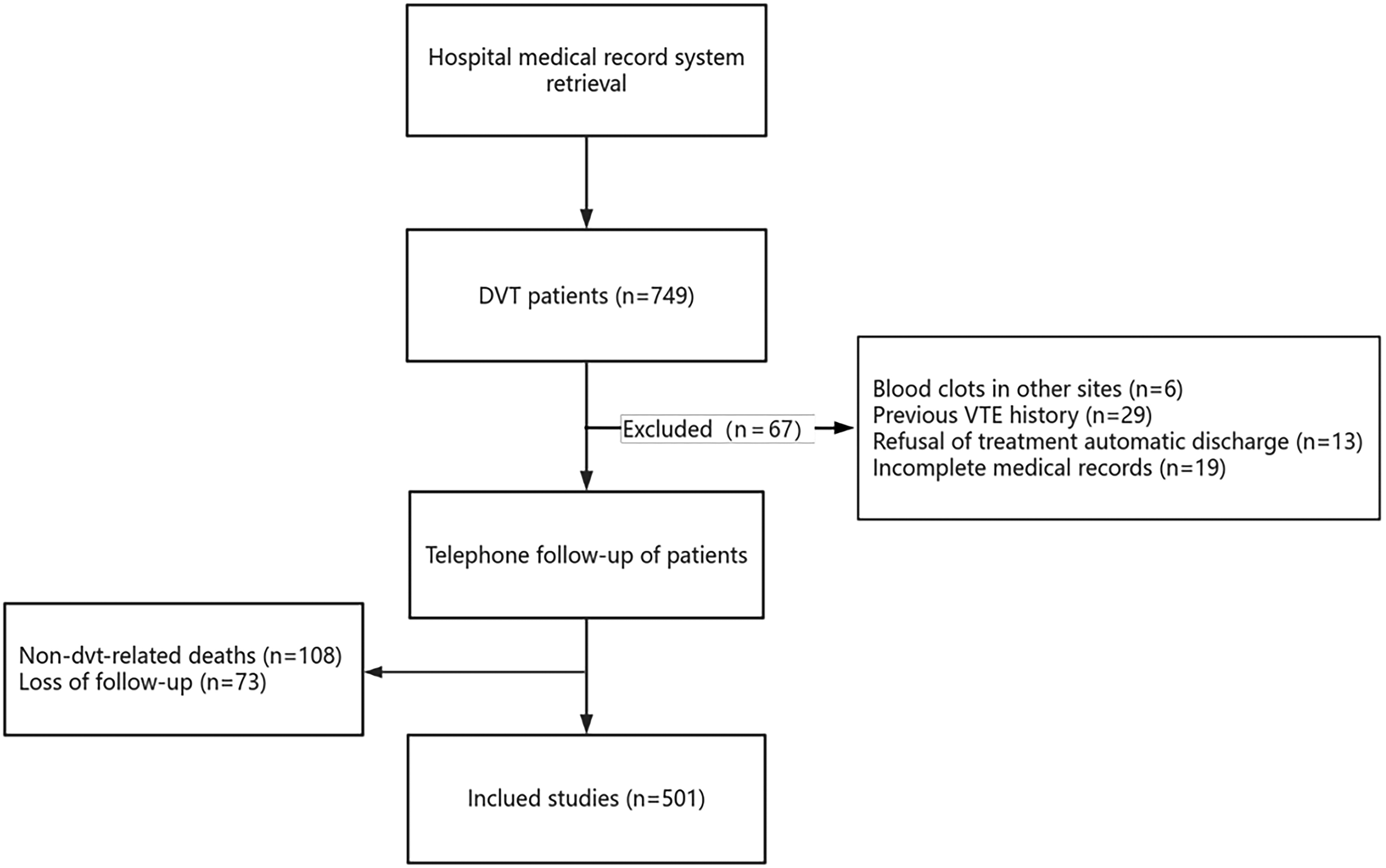
Included crowd.

Distribution of post-thrombotic syndrome (PTS)-related symptoms and signs.
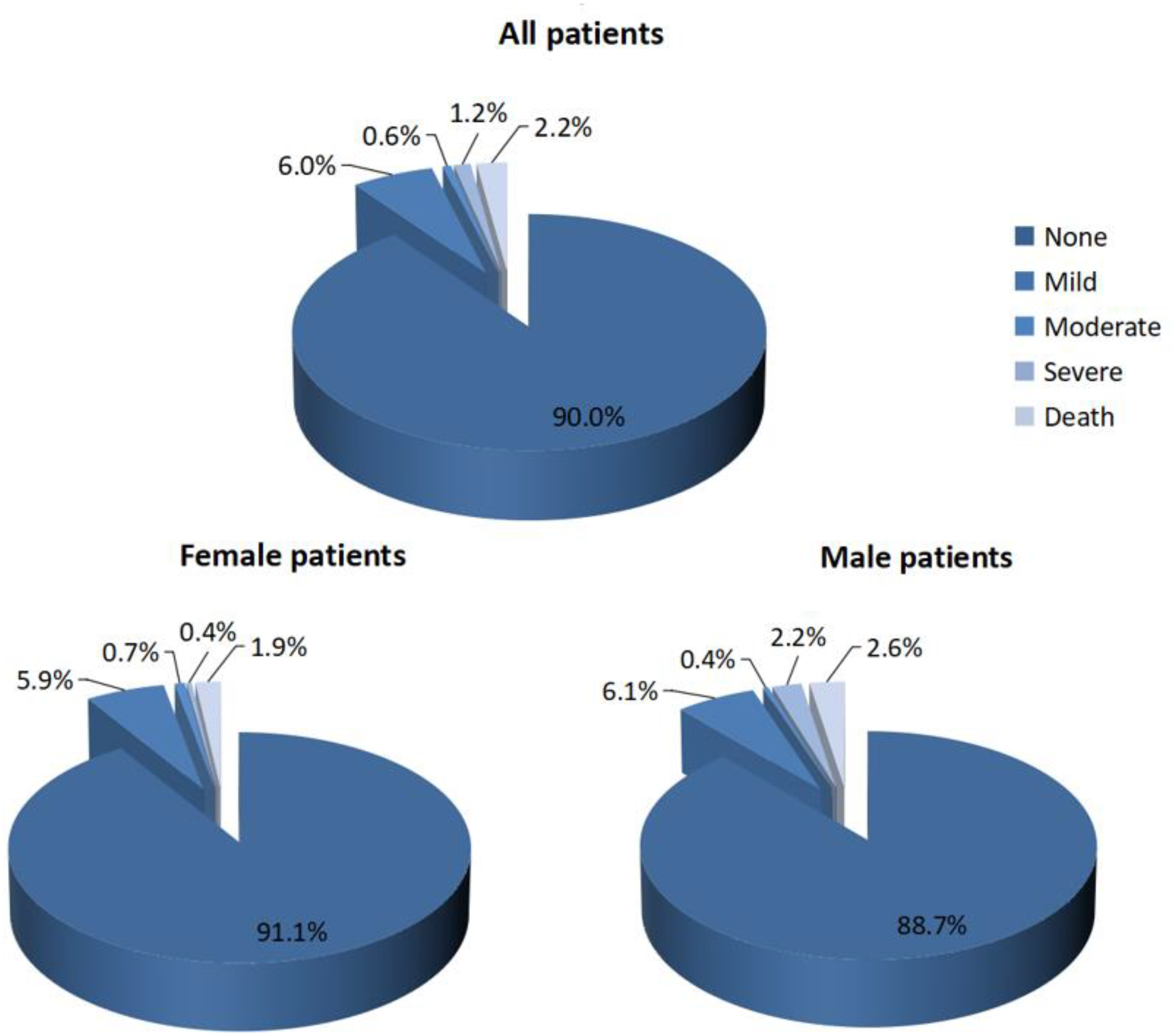
Distribution of post-thrombotic syndrome (PTS) grading.
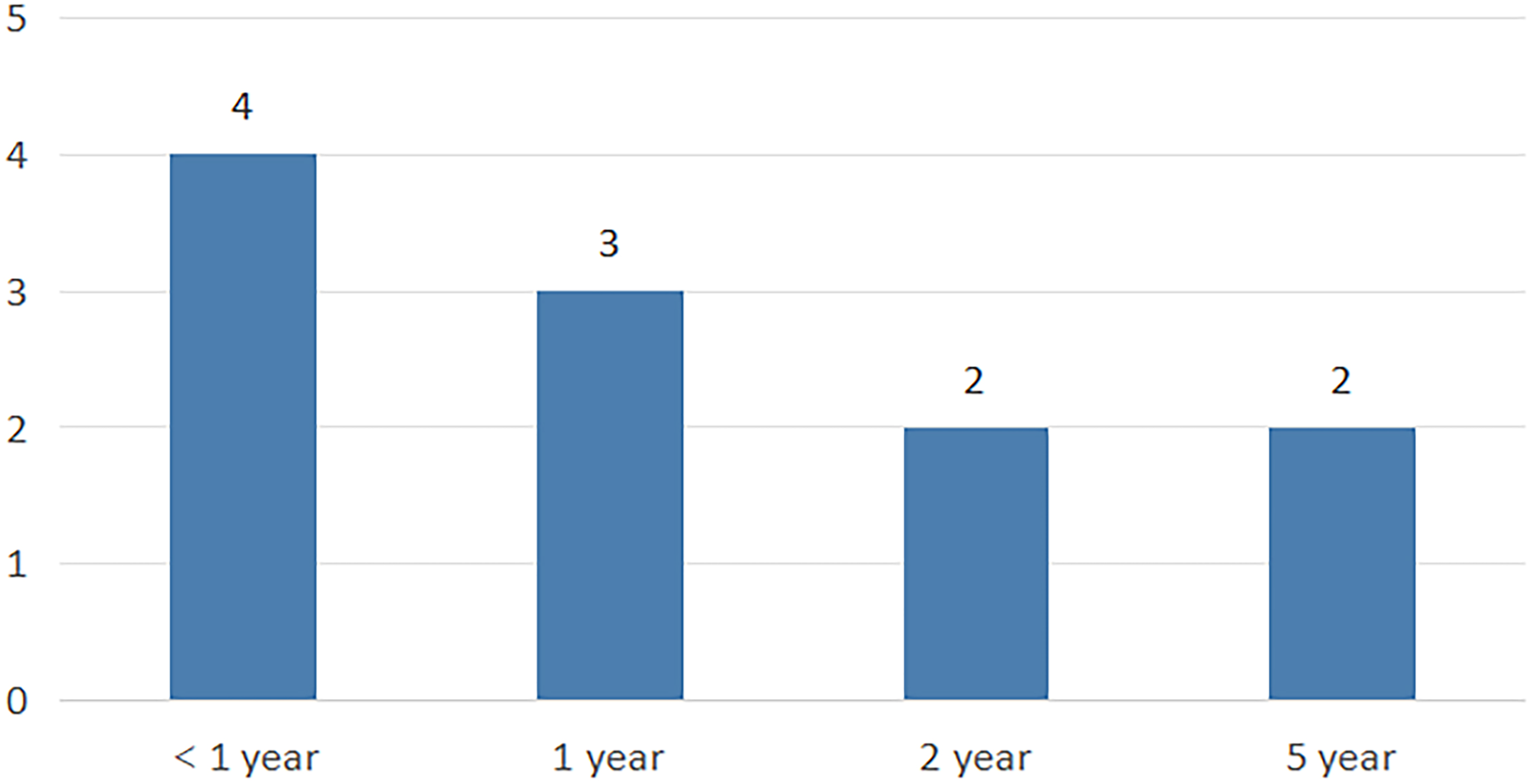
Distribution of time of death (since the first diagnosis of deep vein thrombosis [DVT]).
Distribution of PTS Scores.
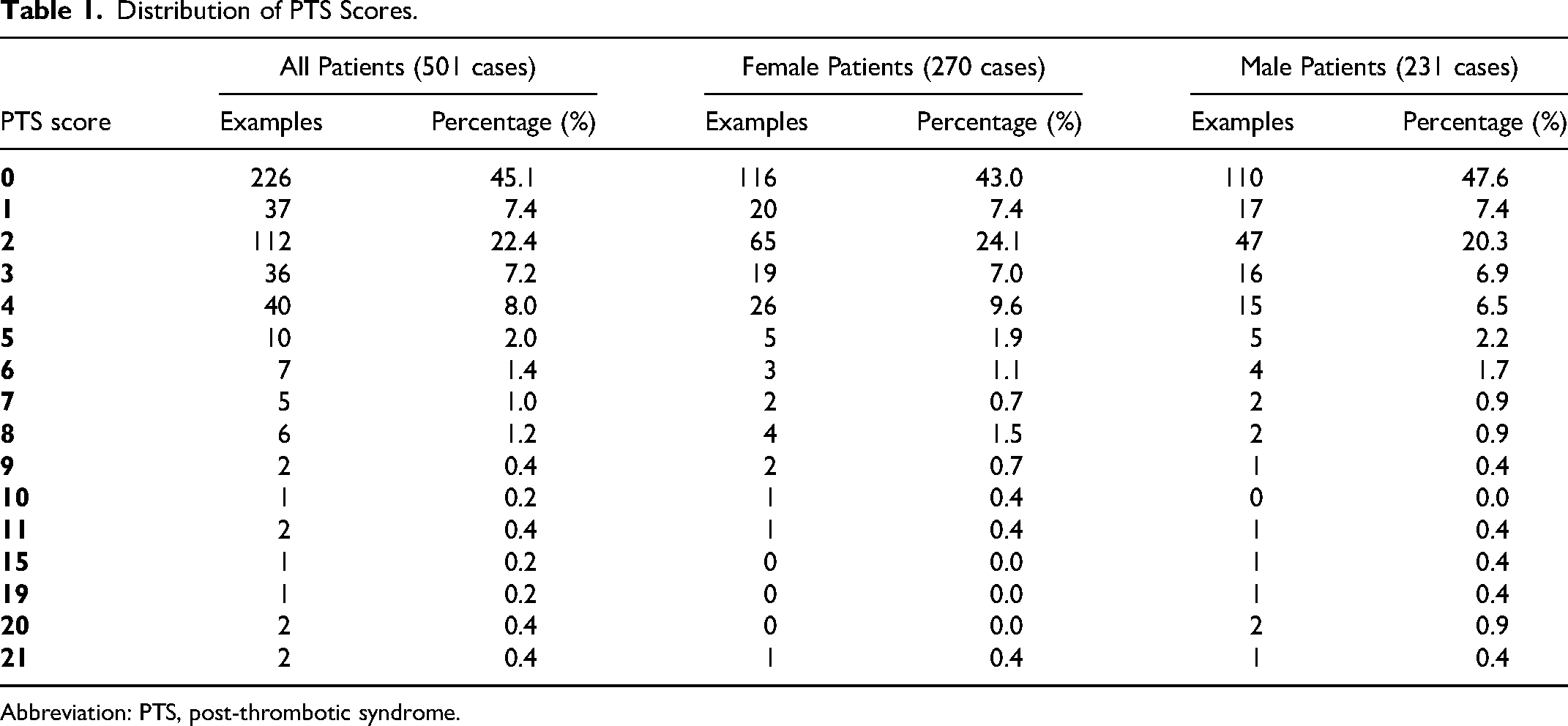
Abbreviation: PTS, post-thrombotic syndrome.
Relationship Between Thrombus Outcome and PTS Score.
Abbreviation: PTS, post-thrombotic syndrome.
Univariate Analysis of PTS Grading in Female Patients.
Abbreviations: DVT, deep vein thrombosis; PE: pulmonary embolism; PTS, post-thrombotic syndrome.
Univariate Analysis of PTS Grading in Male Patients.
Abbreviations: DVT, deep vein thrombosis; PE: pulmonary embolism; PTS, post-thrombotic syndrome.
Sequential Logistic Regression Analysis of PTS Grading in All Patients.
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; OR, odds ration; PE: pulmonary embolism; PTS, post-thrombotic syndrome.
Discussion
Of the 501 patients with DVT included in this study, more than half of the patients had signs and symptoms of PTS (271 of 501, 54.1%). PTS is a chronic venous insufficiency secondary to DVT, caused by dynamic venous hypertension resulting from residual venous emboli and/or valve damage. Recent studies have shown increased arterial stiffness in patients with DVT, 11 more severe arterial wall endothelial dysfunction in lower limbs with PTS than in healthy limbs, 12 and a correlation between VTE disease and arterial disease, but the exact pathophysiology mechanisms of PTS are not completely understood. 13 According to the latest guidelines of the American Society of Hematology, despite the use of standardized anticoagulation therapy, the incidence of PTS in the first year after DVT remains significantly high, approximately reaching 50% and the incidence of severe PTS is 5% to 10%. 14 In our study, PTS was reported to occur in 54.1% of patients with DVT, which was similar to the results of foreign studies.
Among the people we included in our study, the most common symptoms associated with PTS were anterior tibial edema and pain (142 of 271,52.4%), and other specific effects on life included limb swelling after fatigue, pain in cold weather, and inability to walk long distances. According to the Villalta scale, the patients with PTS were mainly concentrated in the 1 to 4 zones (232 of 501, 46.3%), and belonged to the “no PTS” patients (451 of 501, 92.2%). However, most of these “no PTS” patients still experienced mild lower-extremity symptoms (ie, 232 patients with PTS scores of 1-4), such as pain, hyperpigmentation, and paresthesia. The Villalta scale is endorsed by the International Society of Thrombosis and Hemostasis (ISTH) and the American Heart Association (AHA) for the purpose of diagnosing PTS, and is currently widely used.15,16 However, in our study, the “no PTS” diagnosis made with the Villalta scale, seems to ignore some patients with mild or early PTS who were chronically disturbed. For this group of patients, the cornerstone of treatment is compression hosiery, exercise and lifestyle changes, and a large number of studies have emphasized the important role of lifestyle changes and stress therapy in the effective management of PTS. 3 However, the effectiveness of ECS to preventing PTS is still controversial 4 and due to the poor compliance of some patients, the ideal therapeutic effect is often not achieved in clinic. Due to the lack of effective treatment methods, improving Villalta scale or establishing subclinical diagnostic criteria may help in the accurate evaluation of these patients, and the development of novel means for the prevention and treatment of PTS is also necessary. In clinical practice, we should combine the scale with actual symptoms to develop personalized diagnostic strategies, because this approach can not only improve the accuracy of PTS diagnosis and prognostic assessment, but also help to evaluate patients’ poor prognosis and long-term QoL.
In the follow-up evaluation, we usually use venous ultrasound of the lower extremity to directly reflect the outcome of thrombosis. However, only 58.7% (294 of 501) patients were re-examined after discharge. Among the patients who did not undergo re-examination, 49.3% cases (102 of 207) did not follow the medical review due to “mild conscious symptoms.” The results of this study suggested that the outcome of thrombosis was an important factor affecting the PTS score (1-4 points). Therefore, it is important to closely study the outcome of thrombosis. Peripheral venous ultrasound (US) is often used to diagnose and evaluate venous diseases, and it has the advantages of rapid operation, easy operation and noninvasive nature. Furthermore, bilateral lower limb ultrasound can also be effective in delineating venous anatomy, valvular abnormalities and regurgitation, disease extent and pattern, 5 and thus help to develop treatment plans. Other studies also emphasized that follow-up DVT with both lower limbs can not only monitor the progression of thrombosis and detect residual thrombosis as early as possible, but also play a crucial role in predicting hypercoagulation status and DVT recurrence. 6 In actual clinical practice, some patients may be bedridden or have difficulty in moving, and some elderly patients lack of formal education and cognition of the disease. These family and social factors should be taken into consideration. In the follow up and prevention work, it should be emphasized to patients and their families that lower limb B-ultrasound is a powerful tool to predict PTS, which can prevent the recurrence of DVT, early diagnosis of PTS, and urge their timely review, so as to help clinical personnel to detect and effectively manage patients with PTS early.
The results of this study suggest that the history of varicose veins and DVT involvement in both lower limbs are important factors affecting PTS grading. After gender grouping, history of lower extremity varicose veins affected female patients with DVT only. In a retrospective cohort study conducted in Taiwan, varicose veins were identified as an anatomical risk factor for DVT. 7 However, further studies is needed to verify this association8,17 and rule out the influence of any confounding factors, such as smoking or obesity. In addition, according to the Partsch, 18 the presence of varicose veins may be an important risk factor for DVT developing into PTS. In addition, a Russian cohort study suggested that transparients may also undergo changes in venous diameter during the menstrual cycle, with women with heavy premenstrual legs having the narrowest venous diameter in the secretory phase and the widest during the secretory phase. 9 Further studies in the fields of gynecology and endocrinology are needed to verify the relationship between female hormone secretion levels and changes in venous diameter of the lower limbs, as well as the relationship with the occurrence of PTS. For patients with simultaneous DVT in both lower limbs, their PTS grade is higher than that of patients with unilateral limbs, so clinical attention should be paid to the prevention of PTS and the early diagnosis of PTS.
Moreover, the follow-up results of this study indicated that the duration of taking antithrombotic drugs was associated with an increased risk of drug-related side effects, that the probability of adverse reactions in female patients taking antithrombotics for 4 to 6 months was 3.918 times that of women who took antithrombotics for 3 months, and the same lower extremity DVT with PE also increased the likelihood of drug-related adverse reactions. The above 2 factors were significant in female patients with DVT. Therefore, regular review of indicators of antithrombotic medication is particularly important to prevent adverse outcomes, especially in female patients. Common PTS precautions include the use of compression hosiery and a pharmaceutical mechanical catheter to guide thrombolysis. However, the efficacy of these treatments is questioned by large randomized controlled trials (RCT).10,11 To date, timely and effective anticoagulation therapy is the best method to prevent PTS after acute DVT. The researches that has been published so far indicated that both low-molecular weight heparin (LMWH) and direct oral anticoagulants (DOACs) are superior to vitamin K antagonists (VKA) in the prevention of PTS. 12 A recent systematic review and meta-analysis (including data from an RCT and a set of real-world data) suggested that in terms of VTE recurrence, lower mortality and better clinical net benefit, 13 Rivaroxaban was superior to the LMWH. In DOACs, apixaban may have a lower rate of DVT recurrence and associated bleeding risk compared with rivaroxaban.14–16 Currently, DOACs has become the preferred drug for long-term anticoagulation in patients. 19 In this study, due to the drug prices 20 and medical insurance policy adjustment, warfarin is the most commonly used medication for long-term anticoagulation, followed by rivaroxaban. However, due to the limited number of bleeding events, the data were not analyzed. Many studies have confirmed that, 21 DOACs had lower bleeding rates compared to warfarin. The advantages of DOACs include no need for monitoring prothrombin time (PT) or international normalized ratio (INR), fixed dose, short half-life, rapid onset (for monotherapy), and in most cases, no bridging interventional or surgical procedures. The main side effects currently observed are bleeding, but they have been shown to be safer, especially at lower risk of intracranial hemorrhage, compared to the standard heparin-LMWH-VKA regimens used for the treatment of VTE. 22 In 2022, the European Independent Foundation for Vascular Medicine (European IndependentFoundation for Vascular Medicine) studied DOACs and found that the majority of patients (about 60%-70%) did not experience PTS. 23 Furthermore, severe manifestations such as skin ulcers and/or other severe refractory diseases were observed in a minority of patients, 24 is comparable to the long-term follow-up PTS rate mentioned in this study to that observed in studies using thrombolytic therapy. This similarity could be attributed to a reduced variability in anticoagulant activity in the acute phase of the DVT, resulting in a higher probability of venous recanalization. 25 It should be emphasized that patients using antithrombotic drugs should regularly assess the coagulation indicators, liver and kidney function changes, and make necessary adjustments to the drug dose during the follow-up period to prevent the occurrence of adverse events such as anticoagulation-related major bleeding.
The purpose of this study is to investigate the long-term adverse prognosis of patients with DVT for 8 years, followed up for 4 to 10 years, to explore the factors affecting the prognosis of DVT and to provide a reliable reference for future studies in the field of venous thrombosis. However, because this study was a retrospective study and had a long follow-up time, the included population was wide, there were multiple confounding factors. First, the patients who were hospitalized from January 1, 2012 to December 31, 2019 were included in this study. According to the 2012 edition of Guidelines for Diagnosis and Treatment of DVT published by the Vascular Surgery Group of the Surgery Society of Chinese Medical Association, VKA combined with LMWH or ordinary heparin is recommended for acute DVT. After the INR reached the standard and was stable for 24h, LMWH or ordinary heparin was discontinued. The third edition of guidelines, published in 2017, recommended DOACs, or LMWH in combination with VKA, for nontumor patients with early DVT. According to the results of follow up, due to the limitation of drug price and policy factors such as healthcare in general, most of the patients in this study from 2017 to 2019 still adopted warfarin anticoagulation, only a small number of patients were treated with DOACs for anticoagulation. For the confounding effects of DOACs, this study has explained in the discussion section on the correlation between the time of antithrombotic drugs and the side effects of DOACs. Secondly, according to the principle of treatment, the compression hosiery can be used to prevent thrombus recurrence or PTS. 26 Due to the poor patient compliance and the irregular use of compression hosiery after discharge, it was generally impossible to describe the specific duration of compression hosiery at the follow-up visit, which partly affected the accuracy of the final results. Thirdly, the lack of laboratory results during follow up leads to some important data gaps in prognostic factors. Fourth, due to the COVID-19 epidemic, this study could only rely on telephone follow up rather than face-to-face contact, which also affected the accuracy of the follow-up data to some extent.
Regarding follow-up QoL in patients with DVT, there are several important questions regarding QoL to be addressed, including determining whether the QoL of patients with PTS changes with time of treatment, location and extent of DVT, or other factors. By addressing these issues, we can provide comprehensive, evidence-based long-term prognostic information for patients with DVT. This will help to quantify the long-term poor outcomes in patients with PTS.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241266820 - Supplemental material
Supplemental material, sj-docx-1-cat-10.1177_10760296241266820
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Research Physician Development Fund, Affiliated Hospital of Nantong University (YJXYY202204-YSB05).
Ethics Approval
Ethical approval to report this case was obtained from Ethics Committee of Affiliated Hospital of Nantong University (2022-K018-01).
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.