
Abstract
Background:
Complications of deep vein thrombosis (DVT) are related to adequacy of initial anticoagulant therapy. In this study, we analyze consecutive patients with lower-limb proximal DVT and compare the characteristics, treatment, and clinical outcomes of patients receiving entirely ambulatory treatment versus those hospitalized for initial treatment.
Methods:
This was a retrospective study of consecutive patients with a first proximal lower-limb DVT during a 2-year period. Patients were followed for 90 days. Major end points were all-cause mortality, bleeding requiring hospitalization, and recurrent venous thromboembolism (VTE). Events were determined for patients who were hospitalized versus those treated on an entirely ambulatory basis.
Results:
A total of 236 patients were included in the study. Of these, 147 patients were hospitalized and 89 patients received ambulatory treatment. There were 20 fatalities—18 in-hospital and 2 in-ambulatory patients (P = .008). By multivariable Cox regression analysis, the presence of active cancer (hazard ratio [HR] = 5.44; confidence interval [CI]: 2.16-13.7; P = .001), age (HR = 1.06; CI: 1.02-1.1; P = .001), and hospitalization (HR = 5.73; CI: 1.33-24.69; P = .019) were associated with death. Eight hospitalized and 2 ambulatory patients required readmission because of bleeding. Age was the only variable associated with bleeding (HR = 1.10; CI: 1.03-1.18; P = .004). There were no recurrent VTE events.
Conclusion:
In this study of routine management of proximal DVT, we demonstrate that patients suitable for ambulatory care are adequately identified by physicians and may be treated with equal safety and efficacy to hospitalized patients.
Introduction
Deep vein thrombosis (DVT) has an annual incidence of 1 to 2:1000 in adults. 1 It may result in serious morbidity in the form of pulmonary embolism (PE) that may also be fatal or the postthrombotic syndrome. The DVT recurs in up to 30% of patients with an initial unprovoked event. An important factor in determining both short- and long-term complications of DVT is the adequacy of initial anticoagulant therapy. 2
Although once a frequent indication for hospitalization, the advent of low-molecular-weight heparins (LMWHs) for DVT treatment provided the option for ambulatory treatment of these patients with the aim of reducing the costs associated with hospitalization and improving quality of life. Several studies have shown both safety and efficacy of home treatment in comparison to hospitalization for DVT treatment, 1 –6 and the results of these studies are reflected in recent guidelines. 7 However, unlike the case of PE where risk stratification has been used to determine which patients may safely avoid admission, 8,9 no criteria have been defined to guide physician decision-making regarding hospital-initiated DVT treatment versus wholly ambulatory management. 7,10
In this study, we analyze consecutive patients with a first lower-limb proximal DVT presenting to our medical center’s emergency department and compare the characteristics, treatment, and clinical outcomes of patients receiving entirely ambulatory treatment versus those hospitalized for initial treatment.
Methods
Study Design and Participants
This was a single-center retrospective observational study performed from March 2013 to February 2015. Inclusion criteria were age 18 years or older and a first proximal lower-limb DVT diagnosed by Doppler ultrasound at the Meir Medical Center Emergency Department. Patients with concurrent pulmonary embolus diagnosed in the emergency department or during subsequent hospitalization, upper-limb DVT, transfers from other hospitals, patients with a known DVT, previous DVT (in order to avoid bias introduced by prior experience with DVT management), superficial vein thrombosis, or isolated distal vein thrombosis and patients not eligible for anticoagulant therapy were excluded from the study.
Demographic data, prior medical and drug history, were collected. The DVT was considered provoked if an established risk factor for DVT was documented in the 90 days prior to diagnosis. 11 –15 The initial and long-term treatment was documented, and international normalized ratio (INR) measurements for patients receiving vitamin K antagonists (VKAs) were recorded. Patients were followed for 90 days from the day of diagnosis, and the outcomes defined as major end points occurring during this period were collected, namely, all-cause mortality, bleeding requiring hospitalization, and recurrent venous thromboembolism (VTE). Data extraction was performed using the medical center’s computerized database, and the follow-up data were obtained from the patients’ records stored in the Israel national health data storage system, “Ofek” (Ness Technologies, Israel).
The study protocol was approved by the Helsinki Committee of Meir Medical Center.
Statistical Analysis
The median and range of the variables that were studied were calculated and categorical variables by frequency and percentage. Comparison between the groups was performed using the t test for continuous variables and the χ2 test for categorical variables. Rates of mortality and bleeding per 1000 patient days of treatment were calculated, and hazard ratios (HRs) and confidence intervals (CIs) were calculated. Cox regression analysis was used to compare the significant variables between the groups. Kaplan-Meier survival curves were constructed and compared using the log-rank test. Statistical analysis was performed using SPSS version 21.
Results
A total of 348 patients with DVT presented to the emergency department of Meir Medical Center during the study period; 236 patients met the inclusion criteria and comprised the study population. Of these 147 patients were hospitalized and 89 patients received ambulatory treatment (Figure 1). Hospitalized patients were older (median = 73 years, interquartile range [IQR] = 59-85) than the ambulatory patients (median = 68 years, IQR = 56-79; P = .09). There were more women than men hospitalized (60% vs 47%), and hospitalized patients had more underlying illnesses (cardiovascular diseases, hypertension, previous stroke, previous major bleeding, and psychiatric disease), were more likely to be treated with antiplatelet agents at the time of diagnosis (37% vs 26%), and were more likely to have a diagnosis of active cancer (18.4% vs 16.9%) than the ambulatory patients. The percentage of patients with provoked or unprovoked DVT was the same in both patient groups. The DVT following recent surgery was treated on an ambulatory basis more often than in hospital (11.2% vs 6.1%; Table 1).
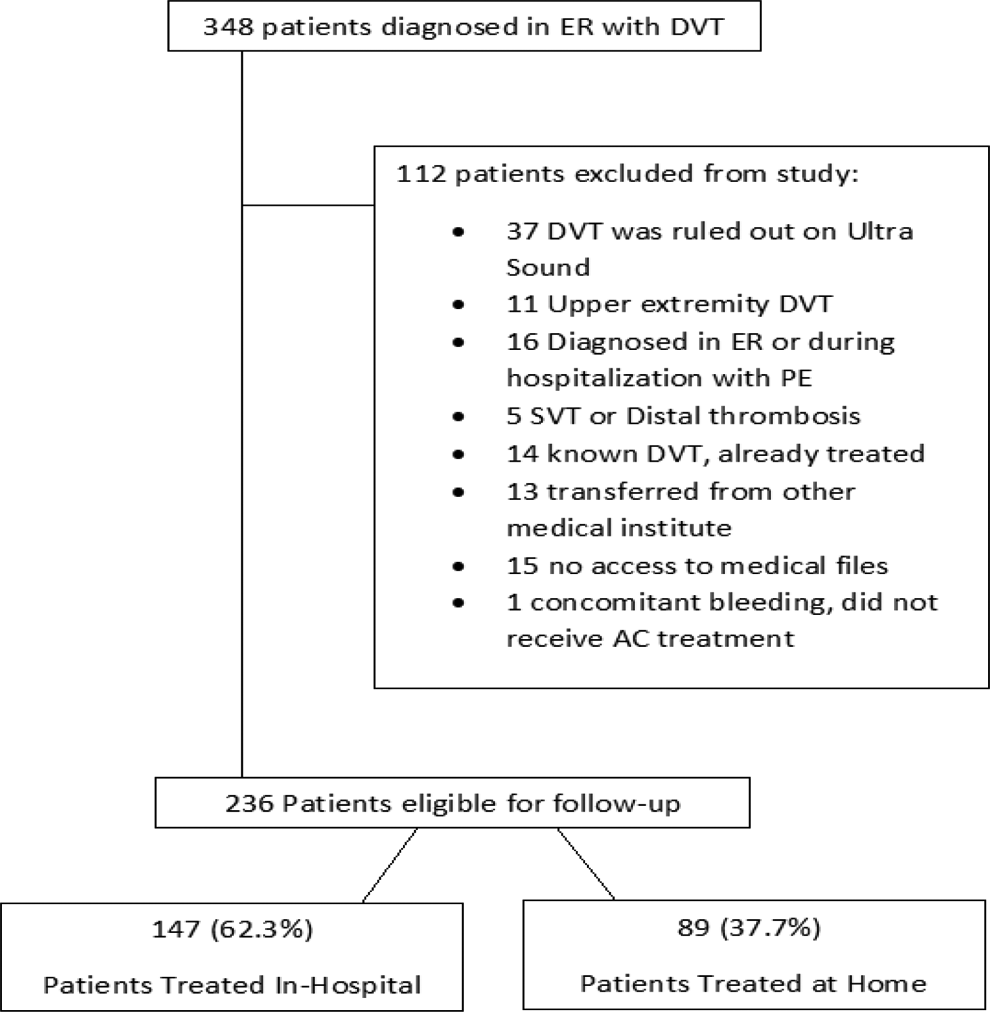
Consort diagram for the study.
Baseline Characteristics of the Patients.
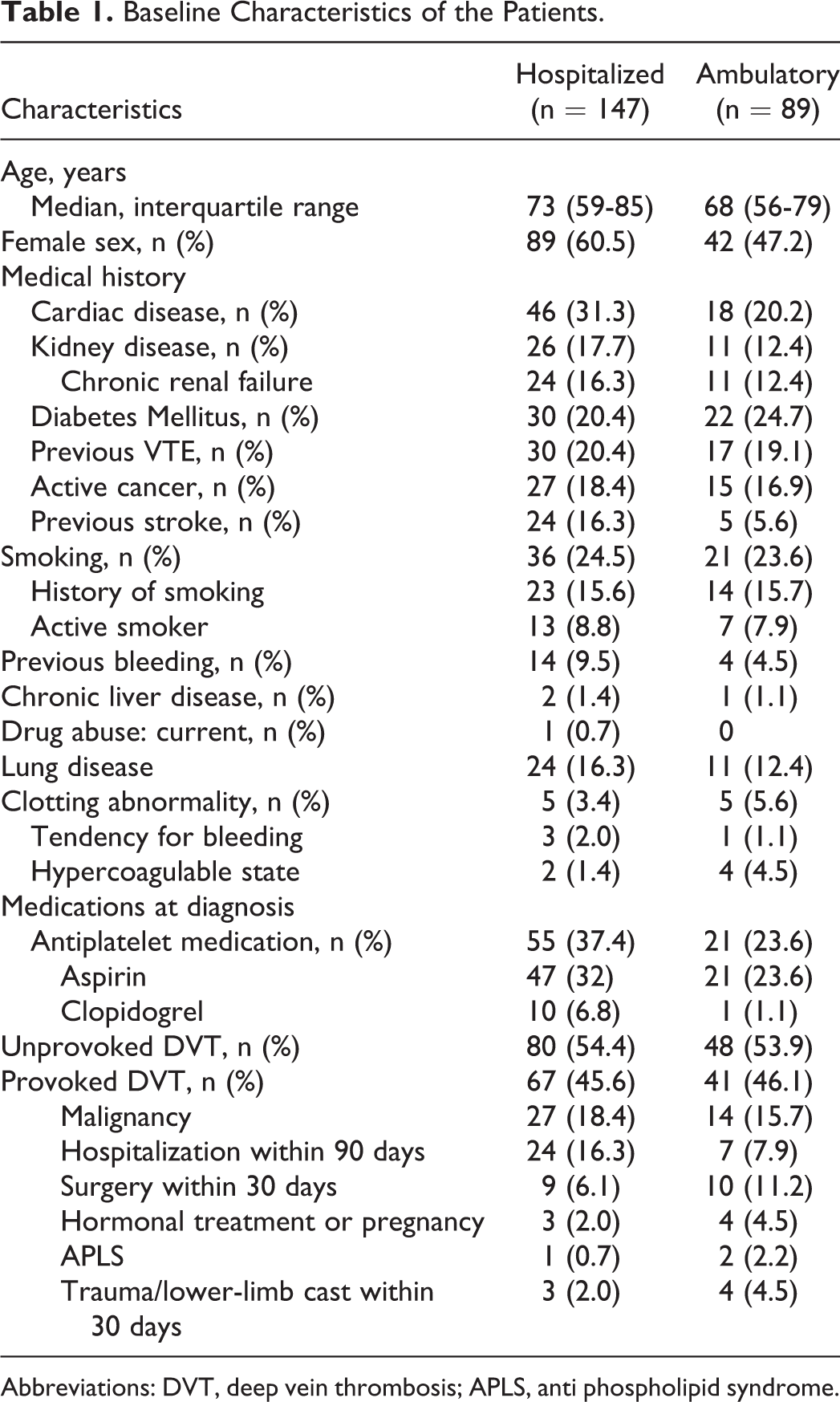
Abbreviations: DVT, deep vein thrombosis; APLS, anti phospholipid syndrome.
More patients received ambulatory treatment in the second study year than in the first (42.6% vs 33.1%), and in the hospitalized group, the mean admission duration decreased from 4.6 to 3.4 days between the first and second study years.
Initial treatment was LMWH (Table 2) for the majority of both hospitalized and ambulatory patients, 96.6% and 95.5%, respectively. Treatment for 90 days after diagnosis, the study duration, was exclusively LMWH in 19.1% of the ambulatory patients versus 32.7% of the hospitalized patients. The VKA was administered as prolonged treatment in 61.8% of the ambulatory patients compared to 44.9% of the hospitalized patients while a non-vitamin K oral anticoagulant (NOAC) was administered in 25.8% of the ambulatory patients and 19% of the hospitalized group. There was a 15.4% increase in the use of NOAC during the second study year in both patient groups, with a corresponding 18.6% decrease in VKA use. The use of LMWH exclusively for the entire study period of 90 days was similar between both study years, 26.4% and 28.7%, respectively. In this study, no patients were transitioned from LMWH/VKA to NOAC treatment.
Treatment of DVT.
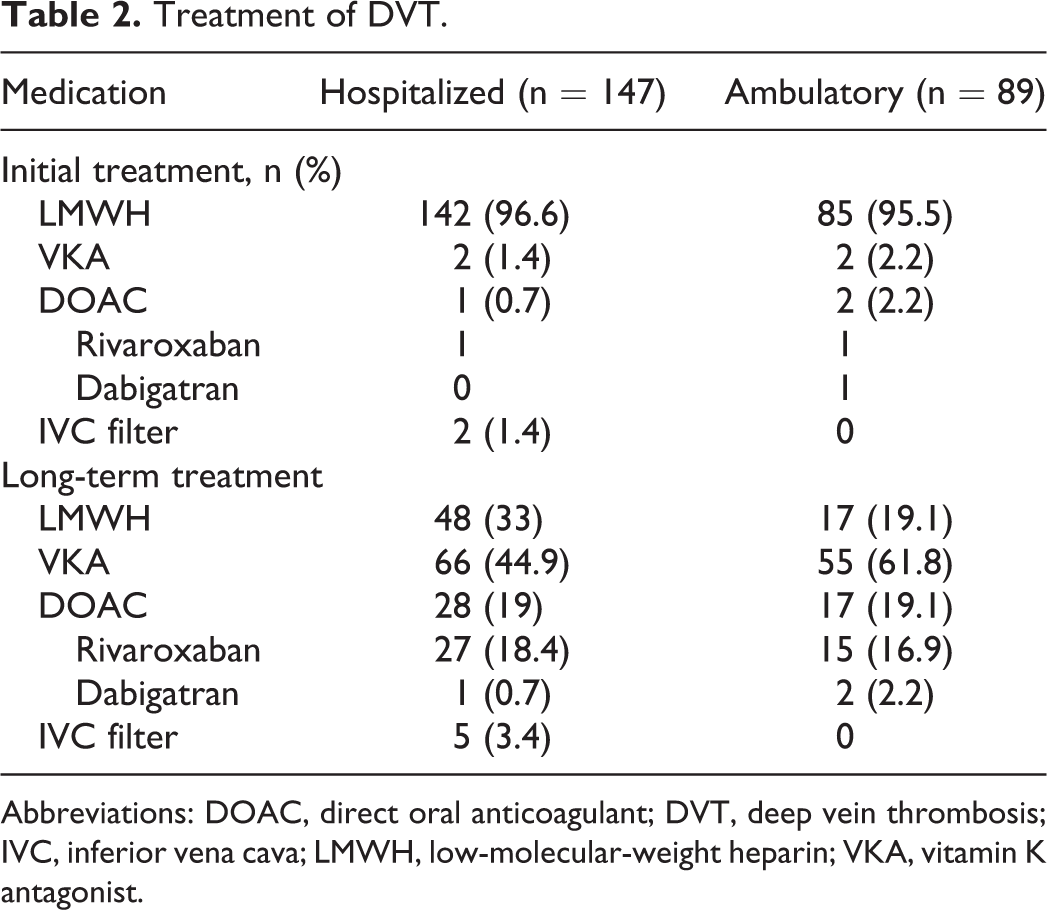
Abbreviations: DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; IVC, inferior vena cava; LMWH, low-molecular-weight heparin; VKA, vitamin K antagonist.
For patients treated with a VKA, INR measurements could be obtained for all but 9 patients. Hospitalized and ambulatory patients had the same percentage of INR measurements in the therapeutic range (INR: 2.0-3.0) during the 90-day follow-up, 33% and 32.1%, respectively, and hospitalized patients had 3 times more INR measurements performed than ambulatory patients (Table 3). Despite this, there was no difference in the time to therapeutic INR level between hospitalized and ambulatory patients (median [IQR] = 13 (7-26) vs 25 (12-38) days, respectively, P = .39).
INR Measurements During Study Period for Vitamin k Antagonist-Treated Patients.
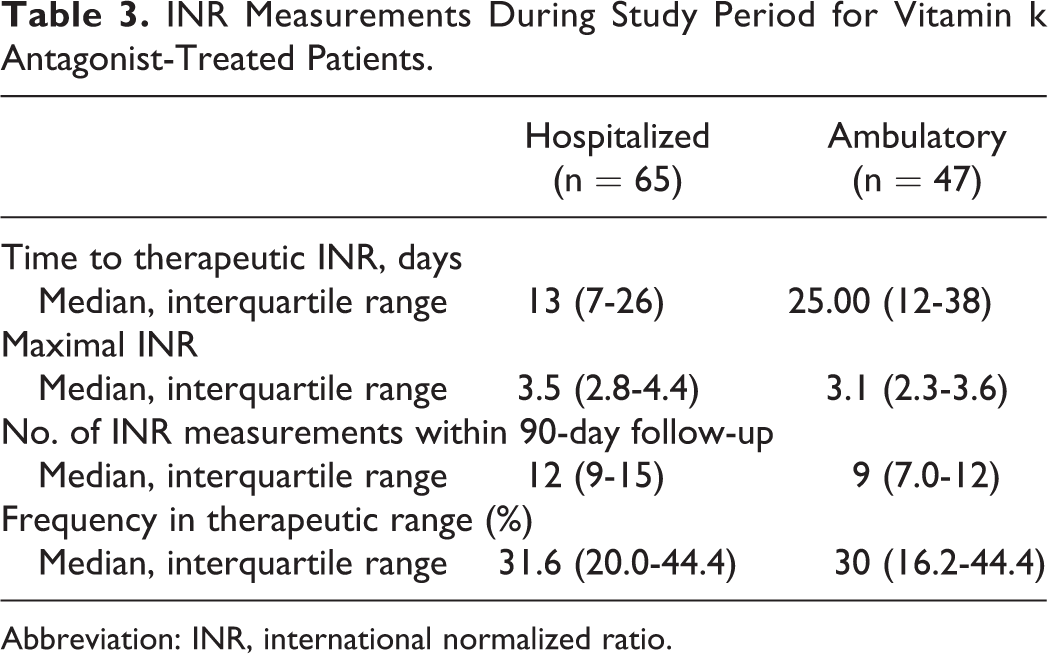
Abbreviation: INR, international normalized ratio.
During the study period, there were 20 fatalities—18 in-hospital patients and 2 in-ambulatory patients (P = .008 by log-rank test; Figure 2; Table 4). By multivariable Cox regression analysis, the presence of active cancer (HRs = 5.44; CI: 2.16-13.7; P = .001), advanced age (HR = 1.06; CI: 1.02-1.1; P = .001), and hospitalization (HR = 5.73; CI: 1.33-24.69; P = .019) were associated with death. Both ambulatory patients who died had terminal cancer at the time of DVT diagnosis. Cause of death could not be determined for 9 out of 18 hospitalized patients who died after discharge and during the 90-day follow-up period.
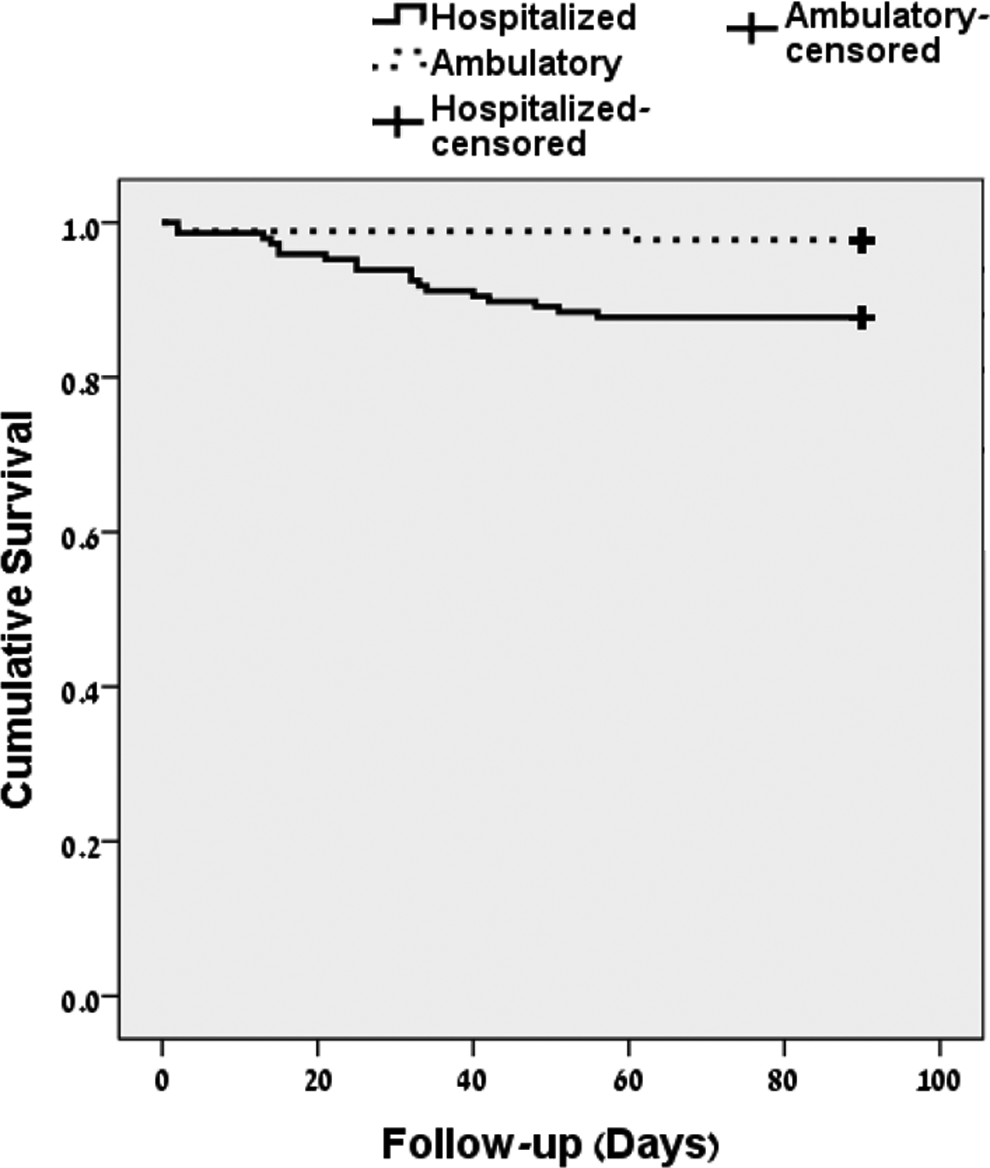
Kaplan-Meier survival curve comparing hospitalized and ambulatory patients censored at the time of death (P = .008 by log-rank test).
Characteristics of Patients Dying During the Study Period.
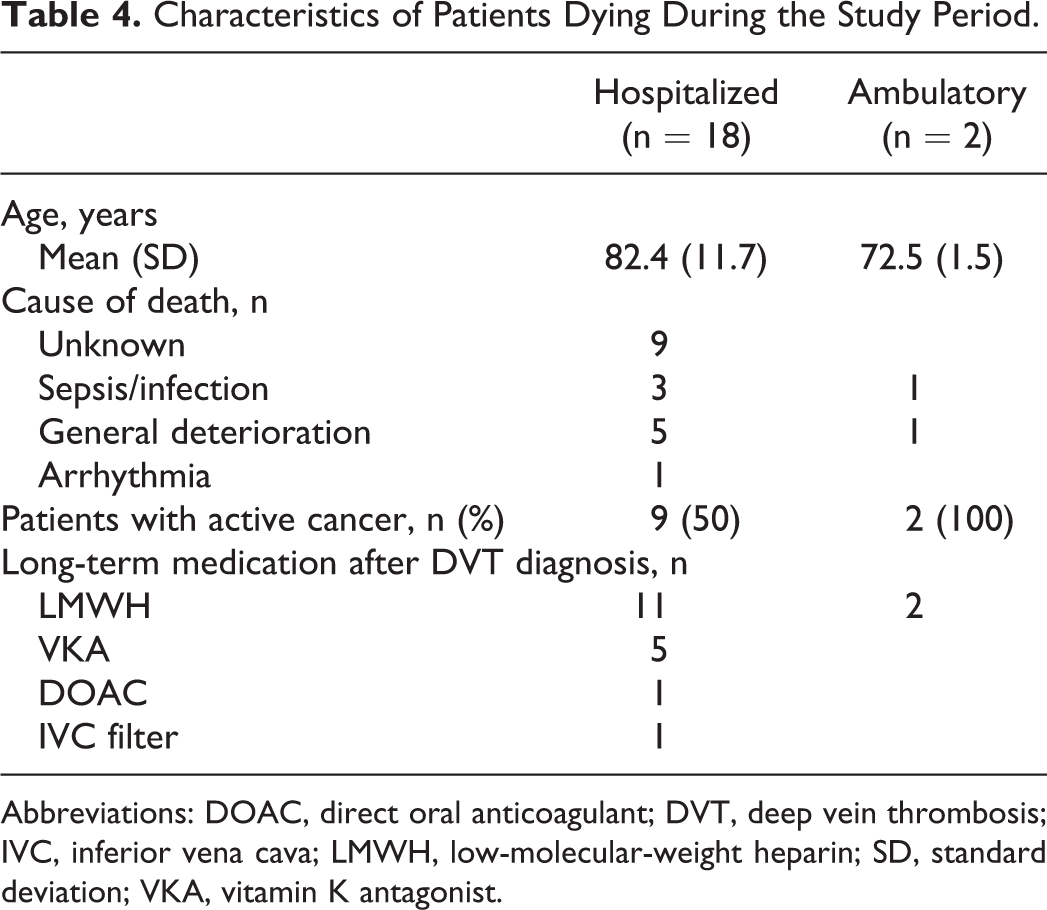
Abbreviations: DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; IVC, inferior vena cava; LMWH, low-molecular-weight heparin; SD, standard deviation; VKA, vitamin K antagonist.
Eight (5.4%) hospitalized and 2 (2.3%) ambulatory patients required readmission because of bleeding. The HR for bleeding for hospitalized versus ambulatory patients was 2.46 (CI: 0.52-11.60; P = .2). Age was the only variable associated with bleeding (HR = 1.10; CI: 1.03-1.18; P = .004). There were no recurrent VTE events in either group.
Discussion
This study demonstrates that ambulatory treatment of proximal lower-limb DVT in routine practice is effective and safe. There was no increase in any of the 3 major outcomes—all-cause mortality, bleeding requiring hospitalization, and recurrent VTE—defined for this study in ambulatory patients. These findings are similar to those from previous studies which have shown that home treatment for patients with acute DVT can be safe, cost-effective, and improve quality of life. 1 –6
Overall mortality for the entire patient population was 8.47% during the 90-day follow-up period, similar to that reported in previous studies that compared home treatment versus hospitalization. 1,11 More patients in the hospitalized group than in the ambulatory group died (12.24% vs 2.25%) which yielded a HR for mortality of 5.71 (CI: 1.33-24.69). The most common cause of death was general deterioration, and there were no mortalities caused by bleeding or VTE. This may significantly underrepresent death in hospital from PE which is frequently discovered only at postmortem and is a well-known cause of in-hospital death, and autopsies were not performed on the 9 patients in this study who died. Furthermore, the cause of death was unknown for 9 of the 18 hospitalized patients who died at home after discharge from the hospital. Although a large proportion of these patients had active malignancy that may have been a proximate cause of death, these important missing data may lead to a further underestimation of incidence thrombosis or bleeding-related mortality. If this were the case, it would increase the relative safety of ambulatory care for patients with DVT.
Although numerically more hospitalized than ambulatory patients were readmitted because of bleeding, this did not translate into an increased HR for bleeding among these patients (HR = 2.46; CI: 0.52-11.60; P = .2).
We observed no recurrent VTE events in either group implying that anticoagulation was equally effective in ambulatory and hospitalized patients, although the patient groups may have been too small to detect a significant difference. Nevertheless, the fact that there was no increase in VTE recurrence among the ambulatory patients during the first 90 days of treatment is encouraging.
In this study, we were also able to determine the frequency of INR measurements in therapeutic range in the VKA-treated patients. Hospitalized patients underwent INR testing 3 times more frequently than ambulatory patients accounted for by increased frequency of in-hospital measurements. Despite this, both groups had the same frequency in therapeutic range: 33% in the hospitalized patients and 32.1% in the ambulatory group. This apparently low frequency may be explained by initial subtherapeutic values obtained while patients receiving concomitant LMWH. Both groups also attained a therapeutic INR after the same duration of anticoagulation.
Important limitations of this study are its retrospective design, and that it was performed at a single center which may limit its generalizability. Patients were not matched for risk factors for bleeding or recurrent VTE, and as may have been predicted, there were several differences between patients receiving entirely ambulatory treatment versus those hospitalized. The hospitalized group was on average nearly 5 years older, with 74.1% of patients being 60 years or older in comparison to only 66.3% of patients in the ambulatory group. There were more women in the hospitalized group (60.5% vs 47.2%) which we could not explain. Women have an increased risk of anticoagulant-associated bleeding which may explain in part the increased incidence of bleeding among the hospitalized patients. Hospitalized patients had more underlying diseases than those in the ambulatory group, and more hospitalized than ambulatory patients were on antiplatelet medications at the time of diagnosis (37.4 vs 23.6%) which might reflect the higher prevalence of cardiovascular diseases and previous stroke in these patients (31.3% vs 20.2% and 16% vs 5.6%). Finally, the retrospective nature of the study and the scope of data that could be collected precluded the ascertainment of cause of death of patients who died at home.
Another important limitation of the study is that NOACs were relatively infrequently prescribed. This is because NOACs were only approved for treatment of VTE in Israel in 2014, and reimbursement was not uniform during the study period. These NOACs will conceivably increase the ease with which patients with VTE can be managed on an entirely ambulatory basis, and their effect on this aspect of VTE management deserves further study.
Despite these limitations, this study has a number of strengths that make its results relevant to clinical practice. It was performed to determine the safety (admission because of bleeding) and efficacy (recurrent VTE) of ambulatory DVT treatment in routine practice. The imbalance in demographic and clinical features between the patient groups indicates that the physicians treating these patients were able to successfully identify a lower risk group of patients in whom discharge from the emergency department did not result in inferior results regarding both safety and efficacy. Another strength of this study is that initial treatment for DVT was the same for all patients—LMWH was administered for 96.6% of hospitalized and 95.5% of ambulatory patients. Long-term treatment differed between the 2 groups—more hospitalized patients received only LMWH for the 90 days of follow-up than did ambulatory patients (32% vs 19%) possibly reflecting a sicker patient population in whom VKA treatment may have been considered inappropriate. The NOACs were administered as long-term anticoagulation to the same extent in both groups (19% in-hospital vs 19.1% in-ambulatory patients), and their use increased during the study period. During the first study year, 12.3% of hospitalized and 10% of ambulatory patients received an NOAC, whereas during the second year of study, 27.3% of hospitalized and 26.5% of ambulatory patients received an NOAC. There was a corresponding decrease in VKA use by approximately 20% in both patient groups. The frequency of LMWH use exclusively remained similar throughout the study. Finally, consecutive patients were studied thus eliminating selection bias and capturing the full spectrum of patients with DVT encountered in practice.
It has become clear that early ambulation after DVT is safe and might even reduce clinical symptoms such as pain and discomfort, 7,10,13 and the standard of care has changed radically from strict bed rest in the 1940s to early ambulation in hospital and finally to entirely ambulatory care. In our study, we confirmed this trend. During the second study year, only 57.4% of patients were hospitalized compared to 66.9% during the first year. Furthermore, duration of hospitalization decreased from a mean of 4.6 to 3.4 days from the first to second study year. A similar trend has been reported among patients in the international RIETE registry of whom 53.7% of patients with DVT received ambulatory treatment, and among the hospitalized patients, mean admission duration decreased from 12.3 days in 2006 to 7 days in 2013. 16
Nevertheless, it is important to acknowledge that DVT poses risks for serious morbidity and mortality if not treated optimally. Although ambulatory care is becoming technically easier to achieve in the era of the NOACs, 2 of which—apixaban and rivaroxaban—may be administered as initial therapy, thus avoiding the need for injections altogether, appropriate patient selection and the existence of sound ambulatory medical services to ensure adequate therapy are essential. 7,10,17
Conclusion
In this study of routine clinical management of proximal lower-limb DVT, we demonstrate that patients suitable for ambulatory care are adequately identified by physicians, and that in our public health-care system, these patients may be treated with equal safety and efficacy to patients initially hospitalized for DVT treatment. The clinical profile of patients selected for admission who may be considered high risk for ambulatory treatment was that of older individuals, the presence of an active malignancy, and multiple comorbidities. Algorithms for the safe discharge of patients with DVT from the emergency department could assist in decision-making in this regard and aid in compliance with established treatment guidelines for ambulatory care for patients with DVT.
Footnotes
Author’s Note
This work was performed in partial fulfillment of the MD thesis requirements of the Sackler Faculty of Medicine, Tel Aviv University (Lisa Mausbach).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.