
Abstract
The model for end-stage liver disease (MELD) and the model for end-stage liver disease excluding international normalized ratio (INR) (MELD-XI) scores, which reflect dysfunction of liver and kidneys, have been reported to be related to the prognosis of patients with right-sided “backward” failure. However, the relationship between the MELD/MELD-XI score and the in-hospital adverse events in pulmonary embolism (PE) patients was unknown. Normotensive PE patients were retrospectively enrolled at China–Japan friendship hospital from January 2017 to February 2020. The primary outcome was defined as death and clinical deterioration during hospitalization. Multivariate logistic analysis was used to explore the association between the MELD and MELD-XI scores for in-hospital adverse events. We also compared the accuracy of the MELD, MELD-XI, and the pulmonary embolism severity index (PESI) score using the time-dependent receiver operating characteristic curve and corresponding areas under the curve (AUC). A total of 222 PE patients were analyzed. Logistic regression analysis showed that the MELD score was independently associated with in-hospital adverse events (odds ratio = 1.115, 95% confidential interval = 1.022-1.217, P = .014). The MELD score has an AUC of 0.731 and was better than PESI (AUC of 0.629) in predicting in-hospital adverse events. Among PE patients with normal blood pressure on admission, the MELD score was associated with increased in-hospital adverse events.
Key Learning Points
What is Already Known?
Optimizing the early risk stratification is essential to determine which patients can be treated safely at home and which patients need surveillance and potential treatment upgrading. Right ventricle dysfunction has been shown to be an important predictor of the severity of acute pulmonary embolism (PE), and the model for end-stage liver disease (MELD)/model for end-stage liver disease excluding INR (MELD-XI) score has been proven to be associated with poor prognosis in different cohorts of right-sided “backward” failure.
What this Study Adds?
Our study suggests that the MELD/MELD-XI score can be used as a practical predictor for in-hospital adverse events in PE patients.
Introduction
Normotensive patients with acute pulmonary embolism (PE) are a highly heterogeneous population with short-term mortality of 2.9% to 7.8%1–3; therefore, advanced risk stratification is a highly essential and challenging component of management. Patients with low risk may be candidates for early discharge and continuation of treatment at home,4,5 while early reperfusion treatment should be considered for patients with intermediate-high risk PE. 6 To date, several risk stratification models for mortality have been developed. Of these, the pulmonary embolism severity index (PESI) score is the most extensively validated score. 7 The model for end-stage liver disease (MELD) score which is based on the international normalized ratio (INR), total bilirubin (TB), and creatinine levels, and the model for end-stage liver disease excluding INR (MELD-XI) are traditionally used to reflect liver and renal dysfunction. Right-sided “backward” failure may lead to renal and hepatic congestion then injury; recently, several studies have reported the prognostic relevance of the MELD/MELD-XI score in different cohorts of right-sided “backward” failure, including patients undergoing tricuspid valve surgery, 8 constrictive pericarditis, 9 and right ventricular failure after undergoing left-ventricular assist device (LVAD) implantation. 10 The right ventricular dysfunction has been shown to be an important prognosis predictor for patients with acute PE.11,12 The MELD score might be a useful predictor of mortality among high-risk PE patients admitted to intensive care units. 13 Studies also suggested that the MELD-XI score is associated with the in-hospital mortality of intermediate-to-high risk acute PE. 14 However, the association of the MELD and MELD-XI scores with adverse events has not been reported in normotensive patients with acute PE.
In this study, we aimed to assess the association between MELD and MELD-XI scores and adverse in-hospital outcomes in PE patients with normal blood pressure, and compared their prognostic accuracy with the PESI score.
Methods
Study Design and Participants
Normotensive PE patients admitted to China–Japan Friendship Hospital from January 2017 to February 2020 were retrospectively enrolled. The inclusion criteria were as follows: 1. age ≥18 years; 2. the diagnosis of PE was determined by a positive test using computed tomography pulmonary angiography (CTPA) or a high probability ventilation-perfusion (V/Q) scan; 3. hemodynamic stability on admission with systemic systolic blood pressure (SBP) of at least 90 mm Hg. Patients with chronic thromboembolic pulmonary hypertension, coronary artery disease, and existing severe hepatic and renal insufficiency (chronic kidney disease stage 5 and child-C stage) were excluded from this study. The study protocol was conducted in accordance with the amended Declaration of Helsinki and was approved by the local independent Ethic Committees at China–Japan Friendship Hospital.
Data Collection
We collected the clinical data of all the patients, including age, sex, clinical presentation, vital signs on admission, and the presence of comorbidities. Laboratory panel on admission was comprised of INR, creatinine, TB, troponin I (cTNI) or troponin T (cTNT), brain natriuretic peptide (BNP) or N-terminal B-type natriuretic peptide (NT-proBNP), and arterial blood gas analysis. All INR, creatinine, and TB levels were measured before initiating any anticoagulant therapy. Troponin was defined as elevated if cTNI > 0.4 ng/ml or cTNT > 0.014 ng/ml according to the biochemical tests used in our institution. NT-ProBNP > 600 pg/ml and BNP > 100 pg/ml were considered abnormal and these values were used as cut-off values in our study. The right ventricle (RV) dysfunction was assessed by transthoracic echocardiography or CTPA and defined as follows: (1) tricuspid annular plane systolic excursion (TAPSE) < 16 mm; or (2) RV/left ventricle (LV) > 1.0; or (3) sPAP (systolic pulmonary artery pressure) > 50 mm Hg.
MELD and MELD-XI Scores
The MELD and MELD-XI scores were calculated using the following formula, as previously reported 15 : the MELD score = 11.2 × (ln INR) + 3.78 × (ln TB [mg/dl]) + 9.57 × (ln creatinine [mg/dl]) + 6.43. The MELD-XI score = 11.76 × ln(creatinine [mg/dl]) + 5.11 × ln(TB [mg/dl]) + 9.44. Any values <1 were given the lower limit value of 1 to prevent negative logarithmic values in the formula. 16 The MELD and MELD-XI scores were calculated using laboratory data on admission before initiating anticoagulant therapy.
Definition of Outcomes
The primary outcome was in-hospital adverse events, including in-hospital death and clinical deterioration. Clinical deterioration was defined as hypotension with SBP <90 mm Hg for ≥15 min or need for catecholamine administration, thrombolysis, extracorporeal membrane oxygenation, mechanical ventilation or cardiopulmonary resuscitation during hospitalization.
Statistical Analysis
Normally distributed data were expressed as mean ± standard deviation (SD), and non-distributed data are presented as medians with interquartile ranges. Categorical variables are expressed as numbers and percentages. The statistical significance of differences was analyzed using a one-way analysis of variance for parametric continuous variables and the Kruskal–Wallis rank-sum test for non-parametric continuous variables. The χ2 test was used to compare differences in categorical variables. Univariate logistic analysis was performed and statistically significant variables were entered into a multivariate logistic regression model to assess the association with in-hospital outcomes. Model 1 was adjusted for age and gender. Model 2 was additionally adjusted for heart rate ≥110 beats/min, elevated troponin, elevated BNP or NT-pro BNP levels, and PaO2/FiO2 < 300. The performance of MELD, MELD-XI, and PESI scores for predicting in-hospital adverse events was examined using receiver operating characteristic (ROC) curve analysis.
A two-tailed P < .05 was considered statistically significant. All statistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, version 225.0; IBM Corporation).
Results
Baseline Characteristics
In total, 222 patients hospitalized for acute PE were included (Figure 1). Overall, the mean age of the patients was 68 years + SD, and 44.6% were male. The distributions of MELD-XI and MELD scores are shown in Figure 2. In our study, the mean MELD score was 7.8 and 196 patients (94.2%) had MELD score <15, and 12 patients (5.8%) with MELD ≥15.
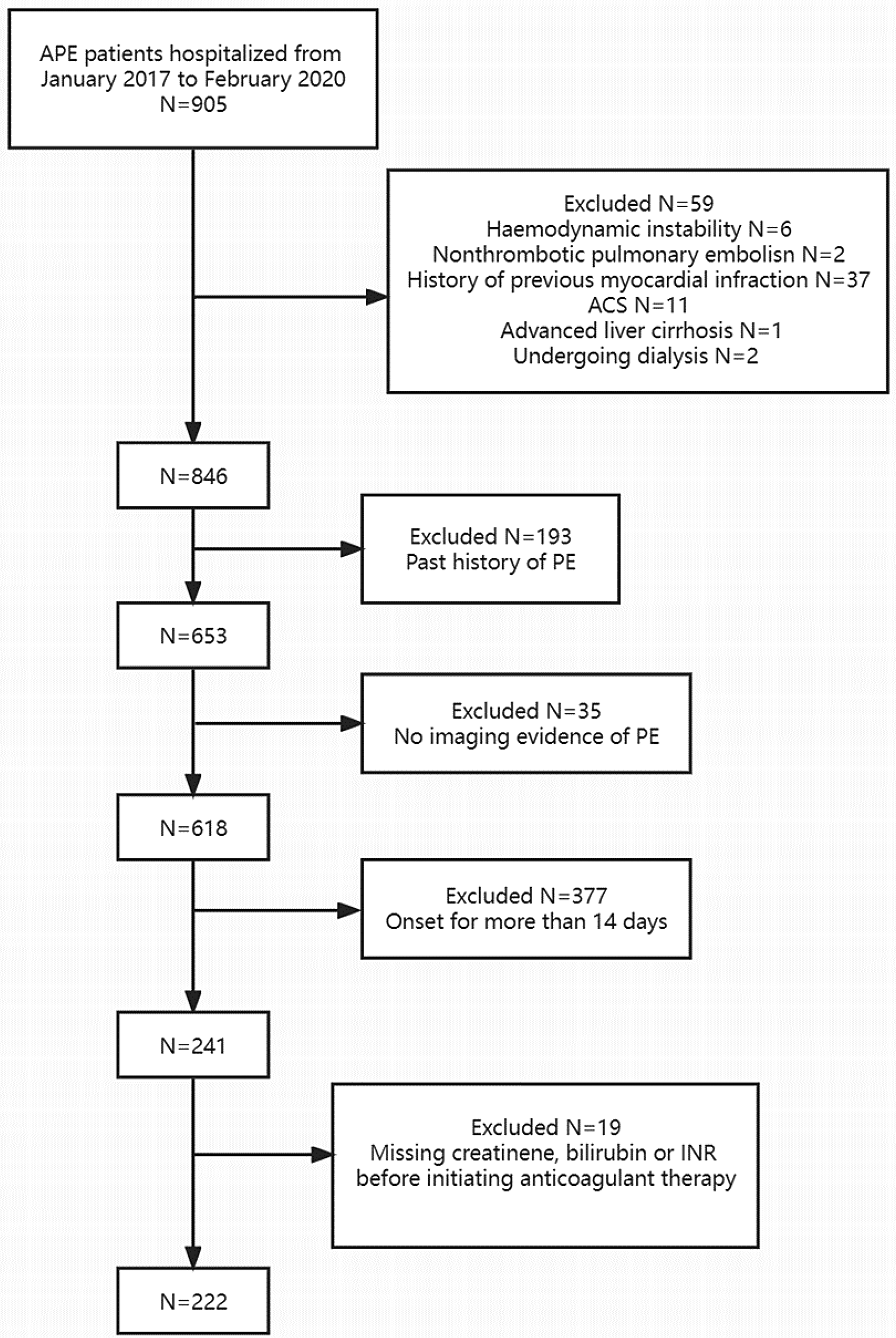
Flowchart of the participants.
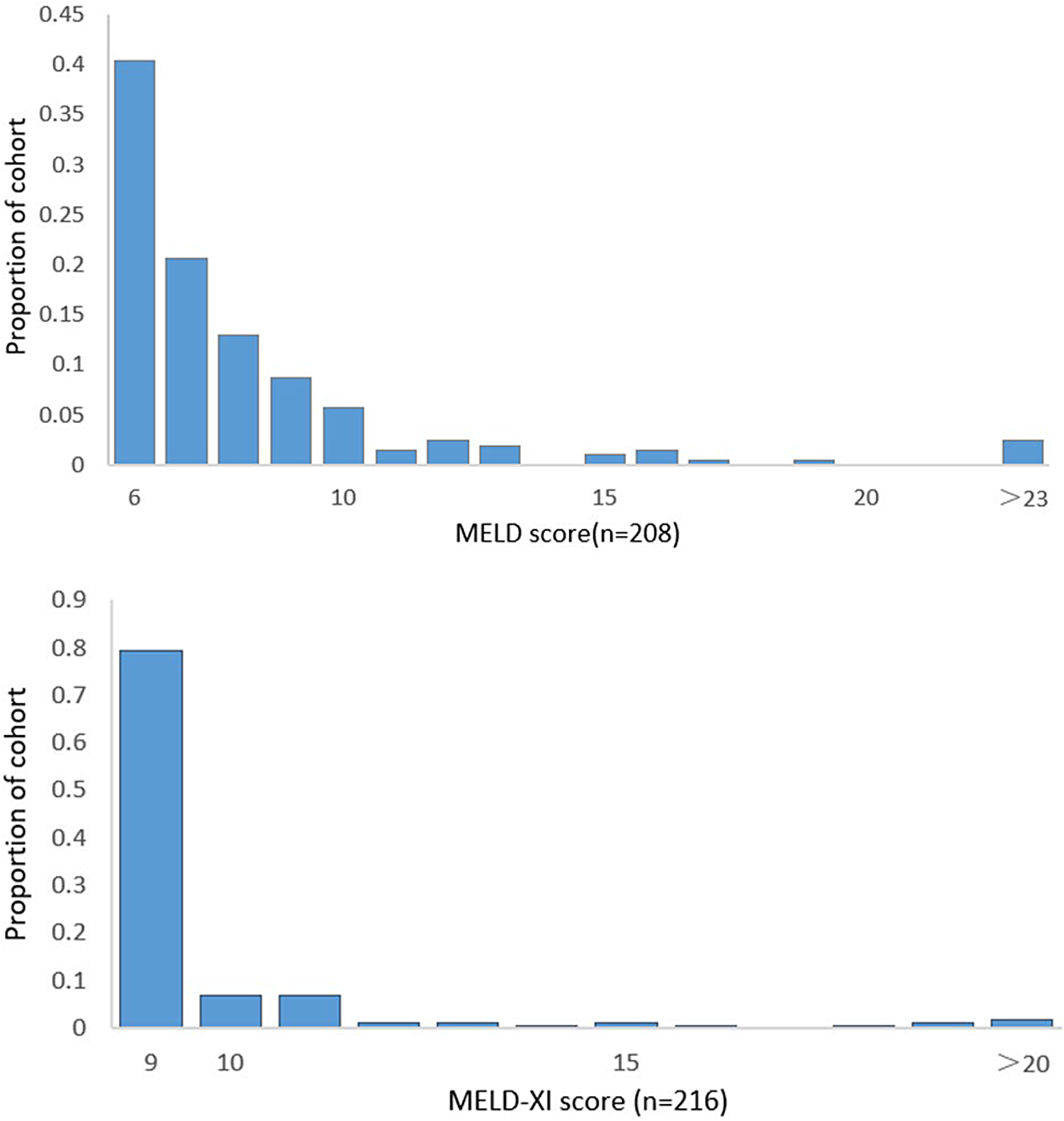
Distribution of model for end-stage liver disease excluding international normalized ratio (MELD-XI) and model for end-stage liver disease (MELD) scores across the cohort.
Compared to the patients without in-hospital adverse events, patients with adverse events had more symptoms such as chest pain and syncope, lower diastolic blood pressure, and higher heart rate. Patients with in-hospital adverse events had higher troponin and BNP levels and lower PaO2/FiO2 (Table 1). Patients with in-hospital adverse events had higher PESI and MELD scores than patients without in-hospital adverse events (101 vs 82 and 9.7 vs 7.6, respectively). However, there was no significant difference among these groups in liver dysfunction, renal insufficiency, and RV dysfunction.
Clinical Characteristics.
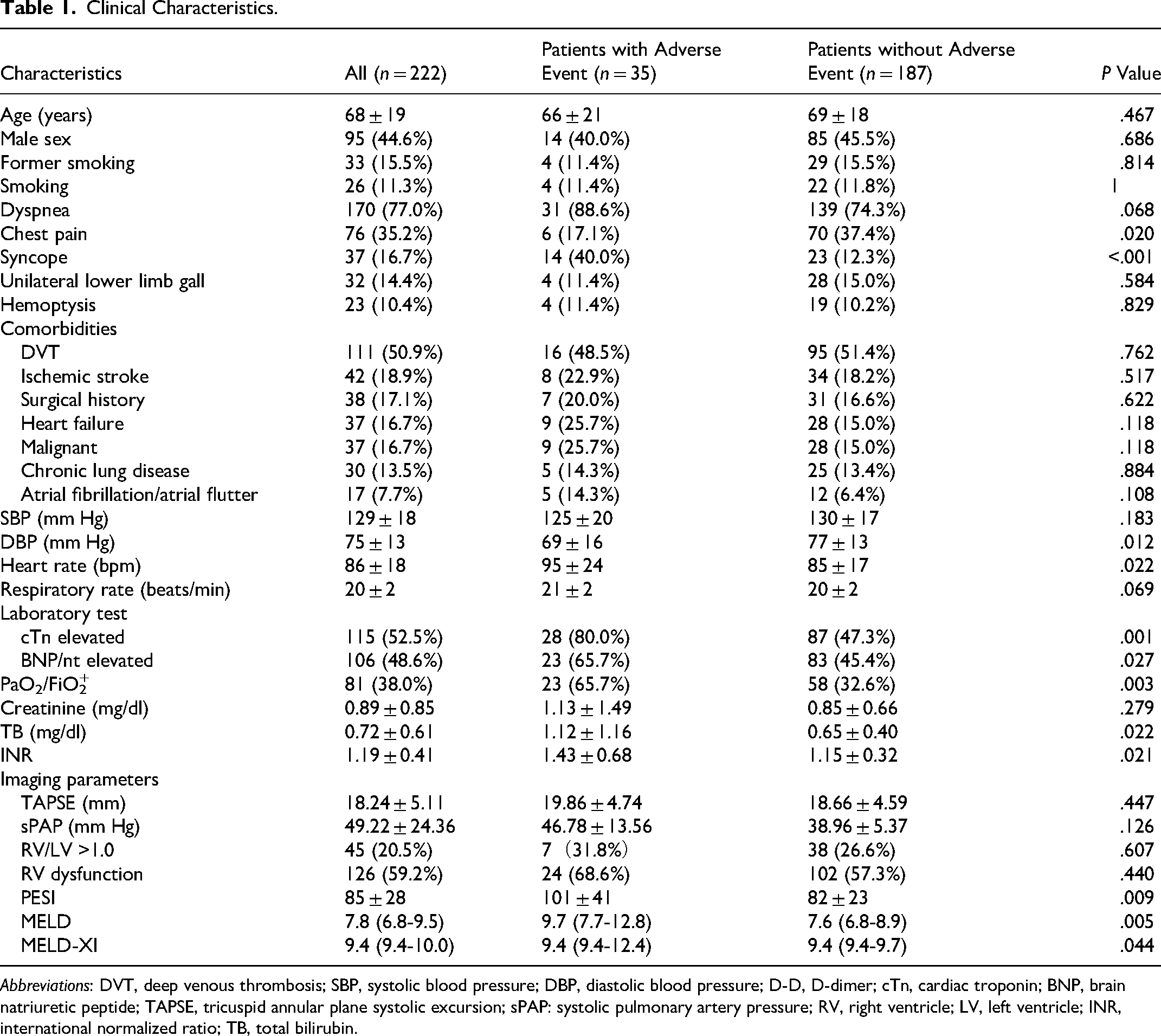
Abbreviations: DVT, deep venous thrombosis; SBP, systolic blood pressure; DBP, diastolic blood pressure; D-D, D-dimer; cTn, cardiac troponin; BNP, brain natriuretic peptide; TAPSE, tricuspid annular plane systolic excursion; sPAP: systolic pulmonary artery pressure; RV, right ventricle; LV, left ventricle; INR, international normalized ratio; TB, total bilirubin.
The Association Between MELD and MELD-XI and In-Hospital Adverse Events
Adverse events were recorded in 35 (15.8%) patients during hospitalization, including 7 in-hospital death (3.2%) and 28 clinical deterioration (12.6%), including SBP <90 mm Hg for ≥15 min (26 cases, 11.7%), need for catecholamine administration (21 cases, 9.5%), thrombolysis (13 cases, 5.9%), mechanical ventilation (19 cases, 8.6%), or cardiopulmonary resuscitation (7 cases, 3.2%). Univariate analysis showed that in-hospital adverse events were associated with pulse ≥110 beats/min (odds ratio [OR] = 3.536, 95% confidential interval [CI] = 1.477-8.471), positive troponin (OR = 4.460, 95% CI = 1.855-10.724), elevated BNP levels (OR = 2.309, 95% CI = 1.084-4.919), and PaO2/FiO2 < 300 (OR = 1.835, 95% CI = 1.441-7.077) (Table S1). Multivariate logistic regression analysis indicated that MELD was independently associated with in-hospital adverse events even after adjusting for age, gender, and these covariates (Table 2).
Association of MELD, MELD-XI, and PESI Scores With In-Hospital Adverse Events.
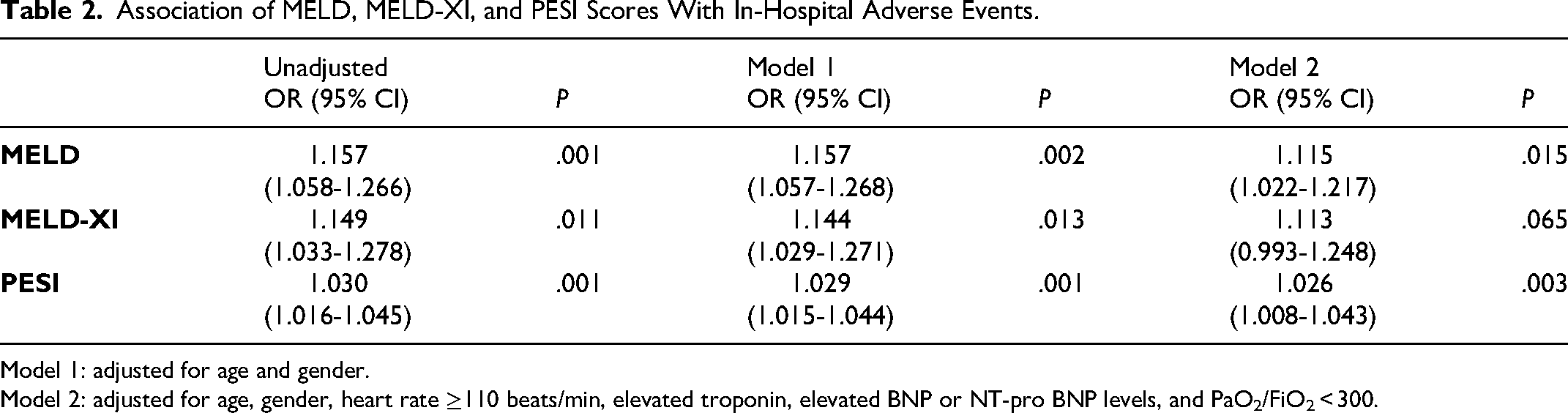
Model 1: adjusted for age and gender.
Model 2: adjusted for age, gender, heart rate ≥110 beats/min, elevated troponin, elevated BNP or NT-pro BNP levels, and PaO2/FiO2 < 300.
Table 3 summarizes the unadjusted and adjusted analysis of the association between MELD score and individual outcomes.
Relative Effect of MELD and MELD-XI Scores on Primary and Secondary Outcomes.
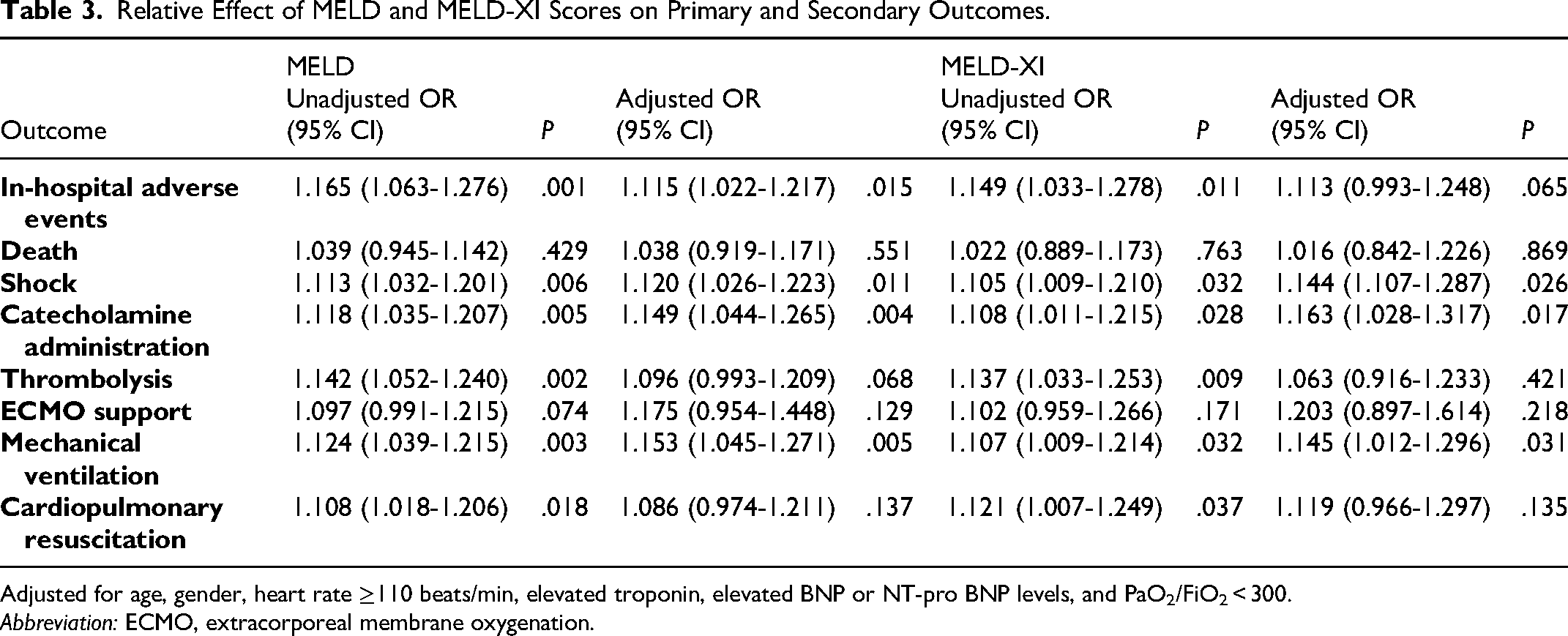
Adjusted for age, gender, heart rate ≥110 beats/min, elevated troponin, elevated BNP or NT-pro BNP levels, and PaO2/FiO2 < 300.
Abbreviation: ECMO, extracorporeal membrane oxygenation.
Figure 3 depicts the effects graphically to emphasize our findings. Even after correction for relevant clinical confounders, both MELD and MELD-XI scores were associated with SBP <90 mm Hg for ≥15 min, catecholamine administration, and mechanical ventilation.
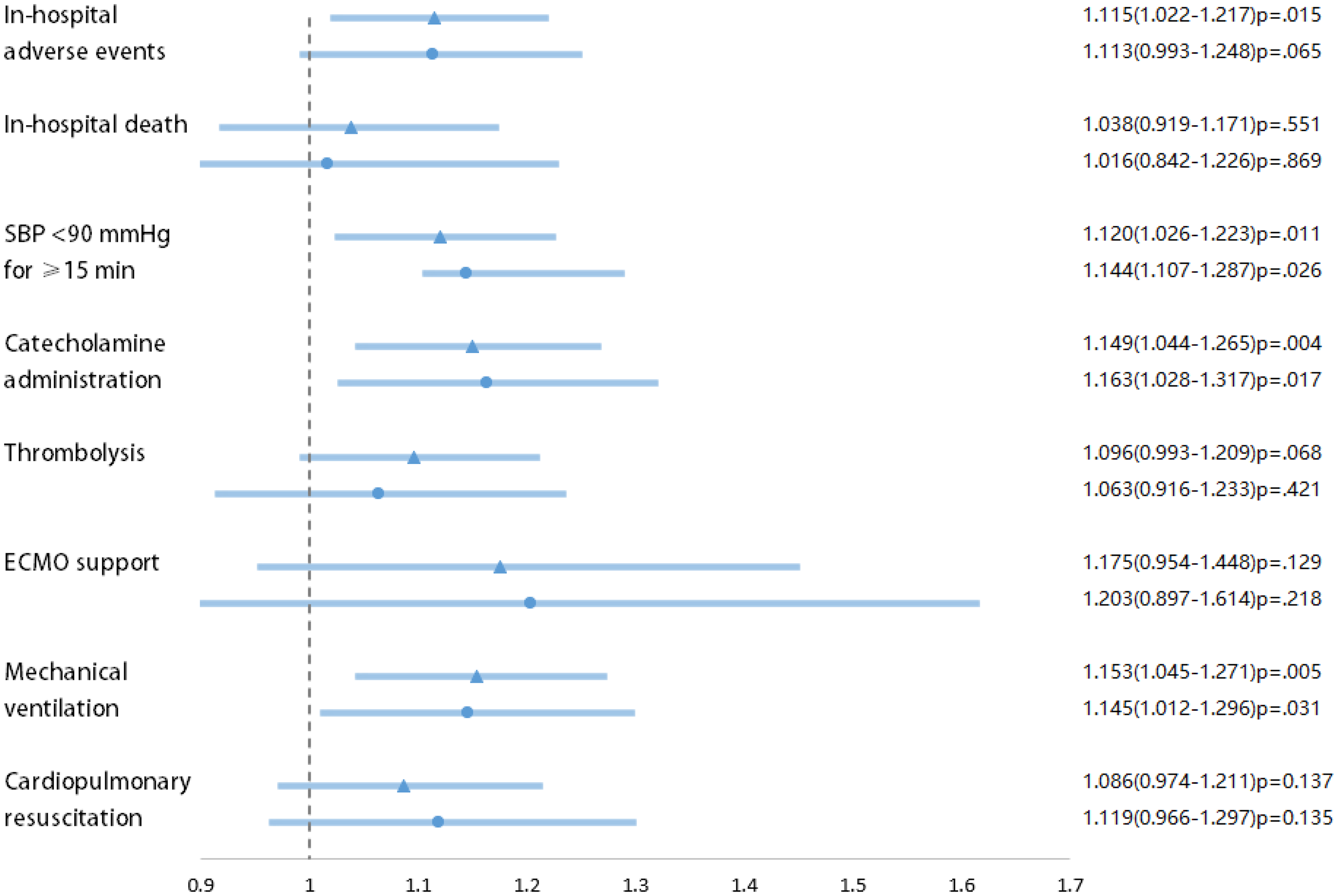
Odds ratios (ORs) of model for end-stage liver disease (MELD) and model for end-stage liver disease excluding international normalized ratio (MELD-XI) scores for the primary outcome and secondary outcomes.
Comparison of the Predictive Value of MELD, MELD-XI, and PESI for In-Hospital Adverse Events
Figure 4 depicts the ROC curves of MELD score, MELD-XI score, and PESI score. The area under the curve of the MELD score for in-hospital adverse events was better 0.731 (95% CI = 0.636-0.827) than the PESI score (0.629, 95% CI = 0.514-0.744) (Table S2). However, the MELD-XI score (0.618, 95% CI = 0.505-0.730) is less effective than the PESI score in predicting adverse events during hospitalization. The cut-off points of MELD score 9.4 had a sensitivity of 60.0% and a specificity of 80.9%.
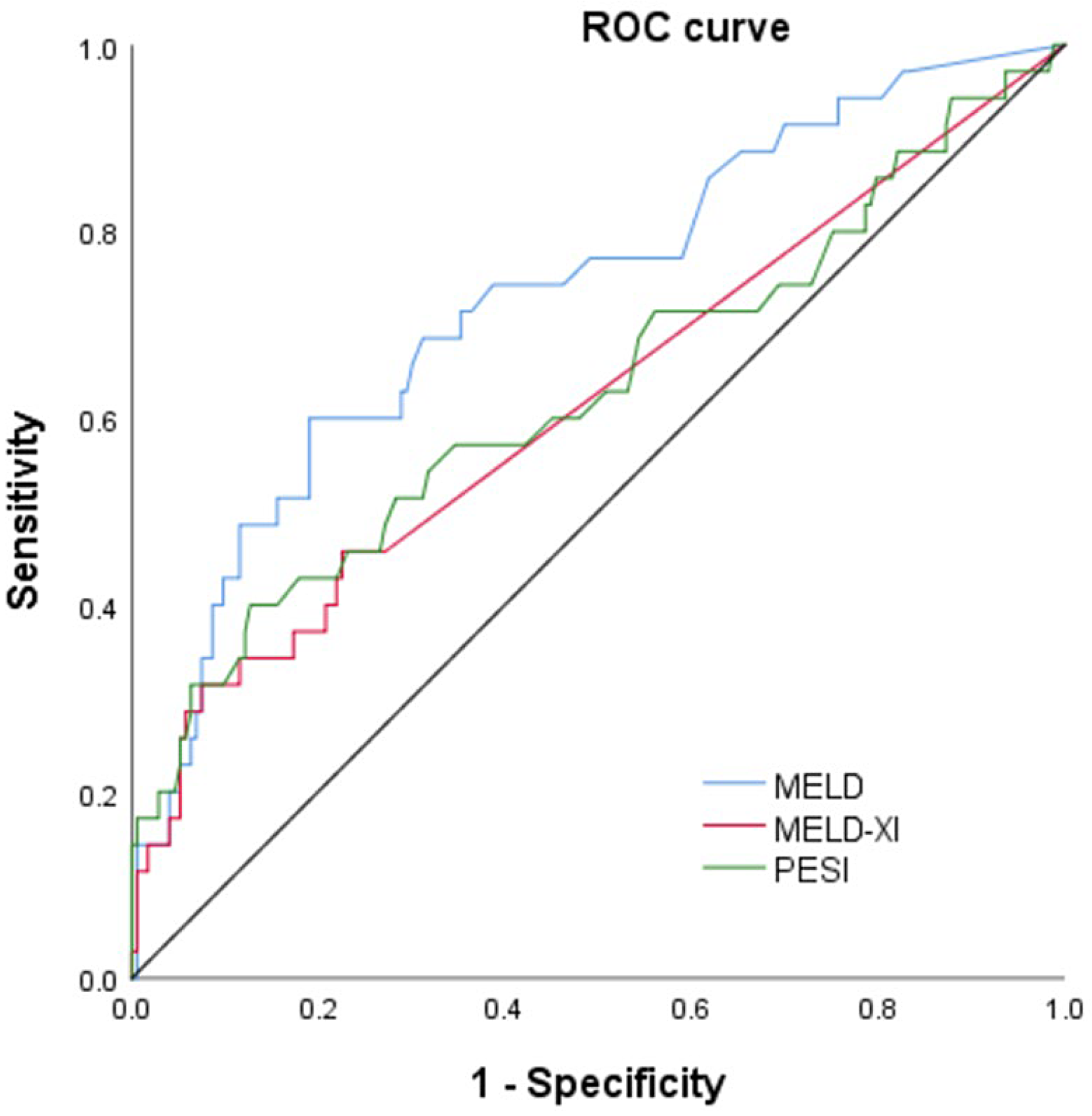
Area under the receiver operating characteristic (ROC) curve of model for end-stage liver disease (MELD), model for end-stage liver disease excluding international normalized ratio (MELD-XI), and pulmonary embolism severity index (PESI) score predicting in-hospital adverse events.
Discussion
In this single center retrospective study of normotensive PE patients, we had two major findings. First, high MELD score was significantly associated with the increased risk of in-hospital adverse events in normotensive patients with acute PE. The cutoff values of the MELD for predicting in-hospital adverse events were 9.4 compared to PESI; MELD score had better predictive performance in predicting in-hospital adverse events.
Accurate risk-stratification assessments are valuable tools that guide physicians to determine appropriate therapeutic management decisions. The MELD score, which is calculated utilizing bilirubin, creatinine, and INR, reflects dysfunction of liver and kidneys. As a modified MELD score, the MELD-XI score excludes INR and thus could be used in patients on anticoagulants. They were developed to predict clinical outcomes of patients with advanced liver disease17,18 and cardiac diseases.9,19,20 A small study (n = 104) 14 of intermediate-to-high PE patients has found MELD-XI to be a predictor of mortality and the optimal cut-off was 10.2. Furthermore, Kadir İdin et al 13 have shown MELD is an independent predictor of 30-day mortality in high-risk patients with acute PE admitted to intensive care units. In the present study, we focus on the various in-hospital outcomes of normotensive acute PE patients, and it also may lead to the optimal cut-off of MELD-XI score ≥12.1 higher than previously reported by Orçun et al. 3
While most risk scoring systems assess cardiopulmonary variables, such as PESI, 7 sPESI, 21 Bova, 22 and FAST (H-FABP, Syncope and tachycardia) score, 23 evidence is mounting that liver24,25 and renal dysfunction26,27 are predictors of prognosis and adverse factors in acute PE. Moreover, the Hestia criteria, which require an assessment of decreasing of liver and kidney functions, could effectively identify acute PE patients who were at low risk of mortality for outpatient treatment or early discharge. 28
The pathophysiological connection between MELD, MELD-XI, and PE might be complex. In PE patients, relative hypoxia,29,30 ischemia, 31 and passive venous congestion 29 are suggested to be the primary driving renal and hepatic injury. First, acute RV dysfunction, triggered by acute PE, usually results in increased central venous pressure and could potentially lead to passive congestion in the liver and kidneys, along with functional impairment of these organs.24,32 Second, dysfunction of the RV can alleviate the load on the LV, subsequently leading to a decrease in stroke volume, which further reduces renal blood flow and liver perfusion. 33 Third, systemic arterial hypoxemia due to acute PE results in liver and kidney dysfunction. 34 In addition, it is likely that MELD/MELD-XI serves as a surrogate marker of general multiorgan dysfunction and mirrors severity of illness. They have been shown to correlate with other scores of poor functional status such as Acute Physiology And Chronic Health Evaluation and to predict outcomes including mortality in the critically ill population.35,36
The MELD/MELD-XI score is dynamic and reflective of the patient's current severity of illness. Whether active thrombolysis is required for intermediate high-risk PE is controversial, in addition to identification of intermediate high-risk PE patients, the score might have a potential role in guiding best timing for the reperfusion. Of note, preoperative improvement in MELD score has been found to improve outcomes for patients with congestive heart failure undergoing LVAD implantation. 37 Only a portion of the identified risk factors for adverse events of PE are modifiable, whether clinical optimization reflected by improved MELD/MELD-XI scores improves outcomes of PE patients has not been investigated. In addition, further studies are warranted to determine whether MELD score can be used as a selection tool for outpatient treatment.
Although no significant improvement was found when compared with PESI, the MELD and MELD-XI scores only consist of two or three parameters, which can be easily measured using inexpensive, routine laboratory tests, so they are simpler and practical risk assessment tools. In conclusion, our findings reinforce the concept of integrating the functional status of the liver and kidney into the risk stratification of acute PE.
Limitations
Our study has a number of limitations that need to be discussed. First, this is a retrospective single-center study, and the sample size was relatively small. Therefore, these conclusions should be verified in different regions and in different populations with larger samples. Second, we could not analyze the association between the MELD/MELD-XI score and long-term prognosis. Additionally, the MELD/MELD-XI score is dynamic and reflective of the patient's current severity of illness, whether preoperative clinical optimization reflected by improved MELD/MELD-XI scores improves outcomes after receiving anticoagulation has not been investigated. Third, INR could artificially elevated by antagonizing vitamin K-dependent pathways, so we collected the biochemical data on admission before initiating anticoagulant therapy. We also assessed the association between the MELD-XI (excluding INR) score and outcomes in order to eliminate the deviation of some patients with heart failure and atrial fibrillation using warfarin. Lastly, despite the fact that a multivariate analysis was conducted, a residual confounding from unmeasured factors may exist, especially liver and kidney biomarkers, gamma-glutamyltransferase, cystatin C, kidney injury molecule-1, and so on, which might affect the study's ultimate results.
Conclusion
Among normotensive patients with acute PE, both the MELD scores are associated with in-hospital adverse events. These results suggest that MELD/MELD-XI score can be used as a practical predictor for in-hospital adverse events in PE patients and further studies are needed to validate these findings.
Footnotes
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Capital Health Research and Development of Special Fund (grant number 2020-2-4065).