
Abstract
Venous thromboembolism (VTE) is associated with high morbidity and mortality. Risk scores associated with VTE have been widely used in clinical practice. Among numerous scores published, those included in guidelines are usually typical risk scores which have been extensively validated and globally recognized. This review provides an updated overview of the risk scores associated with VTE endorsed by 3 guidelines which are highly recognized in the field of VTE including the European Society of Cardiology, American College of Chest Physicians, and American Society of Hematology, focusing on the development, modification, validation, and comparison of these scores, to provide a comprehensive and updated understanding of all the classic risk scores associated with VTE to medical readers including but not limited to cardiologists, pulmonologists, hematologists, intensivists, physicians, surgeons, and researchers. Although each score recommended by these guidelines was more or less validated, there may still be room for further improvement. It may still be necessary to seek simpler, more practical, and more universally applicable VTE-related risk scores in the future.
Introduction
Venous thromboembolism (VTE) broadly comprises pulmonary embolism (PE) and deep venous thrombosis (DVT), superficial vein thrombosis, and splanchnic vein thrombosis, although generally refers to PE and DVT. VTE is the third most frequent acute cardiovascular disease behind myocardial infarction and stroke globally. Annual incidence rates for PE range from 39 to 115 per 100 000 population, whereas that for DVT range from 53 to 162 per 100 000 population. PE may cause 300 000 deaths per year in the US, and cause more than 370 000 deaths per year in European countries. The recurrence rate after discontinuation of anticoagulation treatment may range from 2.5% to 4.5% per year. The annual incidence of major bleeding could reach 3% during anticoagulation. In a word, VTE is a serious global hazard.1–5
Various risk scores have been developed for the prediction, prophylaxis, diagnosis, treatment, and prognosis of VTE. These scores can help clinicians understand the status quo of patients more accurately, compared with subjective gestalt, so as to make further correct decisions. There are 2 types of risk scores which are general risk model and nomogram. General risk scores that account for the vast majority of all risk scores usually yield a dichotomous or more risk strata, whereas nomograms yield a time-dependent risk probability. General risk scores usually have 6 essential elements which are items in risk scores, points for each item, cutoff points for risk strata, efficiency of scores, user-friendliness to clinicians, and generalizability to patients (Figure 1).
Essential elements of general risk sores of venous thromboembolism (VTE).
Based on the ESC (European Society of Cardiology), ACCP (American College of Chest Physicians), and ASH (American Society of Hematology) guidelines which are highly recognized in the field of VTE, the current review was dedicated to provide cardiologists, pulmonologists, hematologists, intensivists, physicians, surgeons, and researchers, etc, an updated overview of all risk scores associated with VTE recommended by these guidelines, in terms of PE risk, DVT risk, medical thromboprophylaxis, surgical thromboprophylaxis, PE severity, VTE recurrence risk, and bleeding risk. The current review does not cover specialized VTE risk scores such as cancer-associated VTE or COVID-19-related VTE.
Methods
We searched PubMed between March, 1987 and November, 2023, for clinical literature in English by using various combinations of “venous thromboembolism,” “pulmonary embolism,” “deep vein thrombosis,” “guidelines,” “score,” “model,” “recurrence,” “bleeding,” and all names of scores involved (please see the Supplemental Files for the detailed literature retrieval records). We preferentially selected all randomized controlled trials (RCT) available and meta-analyses with high GRADE (Grading of Recommendations Assessment, Development and Evaluation) 6 from the past 5 years as much as possible. When selecting references, we also took into account the impact factor of journal, the number of citations, and the academic background and reputation of authors, for the considered literature. Guidelines and authoritative comprehensive narrative reviews that were published within the past 5 years were also thoroughly read. The bibliography in these publications was reviewed one by one.
Results
The relevant risk scores we retrieved comprised Wells PE, Geneva, PERC, YEARS, Wells DVT, Padua, IMPROVE VTE, Caprini, Rogers, PESI, Bova, FAST, Hestia, Vienna, HERDOO2, DASH, DAMOVES, Ottawa, OBRI, Kuijer, RIETE, HAS-BLED, VTE-BLEED, ACCP, and IMPROVE bleeding scores. The major characteristics of each score reviewed are demonstrated in Table 1. The scoring items and risk strata of all the above-mentioned risk scores are displayed in Table S1 of the Supplemental Files.
Major Characteristics of all Risk Scores Associated With Venous Thromboembolism in Guidelines.
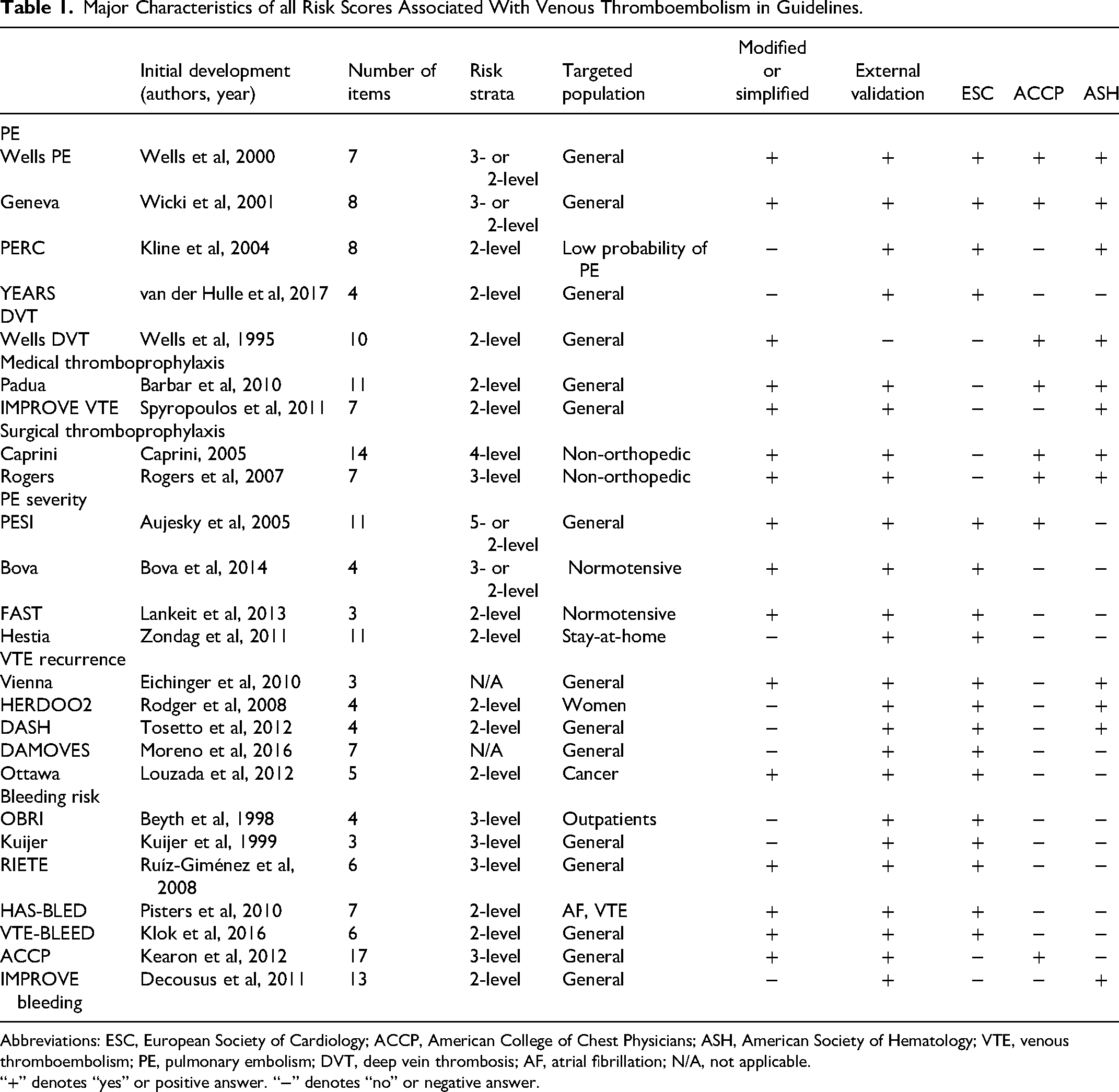
Abbreviations: ESC, European Society of Cardiology; ACCP, American College of Chest Physicians; ASH, American Society of Hematology; VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep vein thrombosis; AF, atrial fibrillation; N/A, not applicable.
“+” denotes “yes” or positive answer. “−” denotes “no” or negative answer.
PE Risk
To date, the scores for pretest prediction (PTP) of PE diagnosis comprising Wells, Geneva, PERC (Pulmonary Embolism Rule-out Criteria), and YEARS scores are more or less endorsed by the latest ESC, 2 ACCP, 7 and ASH 8 guidelines. These scores have been validated in a series of studies. In previous studies, although each one among these 4 scores combined with D-dimer (DD) yields considerable sensitivity or safety and varying specificity in different healthcare settings or subgroups defined by sex, age, cancer, and previous VTE,9,10 their diagnostic efficiency for VTE occurrence is moderate provided not combined with DD.11,12
Wells
Wells score that was first created by Wells et al in 2000 could be the first PE risk score globally recognized.13,14 Wells score was validated in a series of studies9,10 and frequently applied in large-scale international clinical trials,15,16 as well as incorporated into the PEGeD strategy. 17 Despite this, a controversial issue regarding Wells score is that it has a subjective item which is “pulmonary embolism is the most likely diagnosis,” thereby it is not highly favored by ESC guidelines 2 and a latest authoritative state-of-the-art review of VTE. 18
Geneva
The original Geneva score was first derived by Wicki et al in 2001. 19 Due to the poor accessibility of blood gas analysis and chest x-ray in it, it was revised in 2006. 20 It was then modified into a simplified version with comparable efficiency by assigning each item 1 point in the score for improving user-friendliness. 21 Revised Geneva score was also validated in a series of studies9,10 and frequently applied in cutting-edge clinical trials.22,23
PERC
PERC score or rule was first derived by Kline et al in 2004. This rule is applicable to PE-suspected patients with low or very low risk of PE. 24 In a multicenter, prospective, observational study (PERCEPIC), PERC can exclude PE with a low percentage of false-negative results in 1757 European patients with low implicit clinical probability. 25 In a crossover cluster-randomized clinical non-inferiority trial (PROPER) among 1749 patients with a low gestalt clinical probability of PE, the randomization to PERC strategy versus conventional strategy did not result in an inferior rate of thromboembolic events, at baseline and 3-month follow-up. 26
YEARS
YEARS score which is actually an algorithm was firstly proposed by van der Hulle et al in 2017. 27 In the Artemis Study, PE was safely ruled out in 498 pregnant women with suspected PE, by the pregnancy-adapted YEARS diagnostic algorithm across all trimesters of pregnancy. 28 In a cluster-randomized, crossover, non-inferiority trial, compared with a conventional diagnostic strategy, the use of YEARS rule combined with an age-adjusted DD threshold in PERC-positive patients did not result in an inferior rate of thromboembolic events, among 1414 emergency patients with suspected PE. 29
Comparison
There is no identification without comparison. Besides the validation studies for each score, many previous studies compared the performance among these similar scores. In a meta-analysis comparing the performance of Wells, revised Geneva, YEARS, and PERC in different healthcare settings among over 35 000 patients suspected of PE, the Youden index of Wells + PTP-adjusted DD were all highest in the health settings of primary care, referred secondary care, and hospitalized or nursing home care, respectively. 9 In addition, many studies compared Wells and Geneva scores which are similar with each other. In a systematic review that compared the efficiency of original Wells, modified Wells, simplified Wells, revised Geneva, and simplified revised Geneva models in primary care, the Wells rules performed better than Geneva rules in terms of lower failure rates, although efficiency was comparable for all 5 rules. 30
In a prospective multicenter study which compared the efficiency of Wells and revised Geneva scores predicting PE in 1757 outpatients over 65 years, the area under curve (AUC) for Wells and revised Geneva was 0.632 and 0.610, respectively (P = .441). 31 In a retrospective study which compared the predictive power for VTE diagnosis among the Wells, Geneva, YEARS, and PERC scores in 3168 non-surgical hospitalized patients with suspected VTE, Wells score (AUC = 0.694) and revised Geneva score (AUC = 0.697) both performed best among the 4 scores. 11 In another retrospective study which derived a new PE prediction rule prior to imaging tests by synthesizing the scores of Wells, PERC, and Geneva, as well as DD then compared with Wells + DD, PERC + DD, Geneva + DD, and YEARS + DD in patients with suspected PE, the C-index of Wells + DD, PERC + DD, Geneva + DD, and YEARS + DD were 0.759, 0.466, 0.742, and 0.734 in 388 patients of the validation cohort, respectively. 32
DVT Risk
The score for the prediction of DVT occurrence prior to imaging test is Wells DVT score which is endorsed by ACCP 33 and ASH guidelines. 8 The Wells DVT score was first invented by Wells et al in 1995. 34 The prevalence of DVT is approximately 5% in patients with the lowest Wells DVT score of −2, suggesting that DVT cannot be excluded by using the Wells DVT score alone. 35 In a cohort study of 1135 inpatients, the discriminatory accuracy of the Wells DVT score for the risk prediction of DVT was low (AUC = 0.60). 36 In the R-WITT study including 415 patients, the Wells DVT score performed poorly for discriminating the risk of proximal DVT in inpatients with anticoagulation, whereas performed well among patients without anticoagulation, with low inter-rater reliability between physicians. 37 The Wells DVT score is considered to be insufficient to rule out DVT or influence management decisions in the inpatient setting. 38
Medical Thromboprophylaxis
To date, the risk scores for medical thromboprophylaxis of VTE approved by guidelines are Padua and IMPROVE VTE scores. Padua score was recommended by the ACCP guidelines for the prevention of VTE in non-surgical patients, 39 and by the ASH guidelines for VTE prophylaxis in hospitalized and non-hospitalized medical patients. 40 IMPROVE VTE score was recommended by the ASH guidelines. 40
Padua
Padua score that was first established by Barbar et al in 2010 could be the first and most classic VTE risk score globally recognized for medical patients.39–41 In a quasi-RCT, the use of Padua score was associated with a reduced VTE incidence in 235 hospitalized medical patients, compared with the use of clinical judgment in 393 ones (8.5% vs 15.5%, odds ratio [OR] 0.51[0.30-0.86]). 42
IMPROVE VTE
IMPROVE VTE score that was first created by Spyropoulos et al in 2011 has also been extensively used in clinical practice.40,43 A modified version of the IMPROVE VTE score named IMPROVEDD which combined IMPROVE score with DD ≥ 2× the upper limit of normal showed improved risk assessment. An IMPROVEDD score ≥2 identifies hospitalized, medically ill patients with a heightened risk for VTE through 77 days.40,44 In an external validation study of IMPROVE VTE score using a risk score of ≥3 among a total of 19 217 patients, the AUC was 0.702, which was in line with the findings from its derivation cohort. 45 In an external validation study of IMPROVEDD score for VTE risk among 9407 inpatients with COVID-19, the sensitivity, specificity, and AUC were 0.971, 0.215, and 0.702, respectively. 46
Comparison
In a retrospective analysis of 14 660 patients hospitalized for at least 2 days on a medical ward and followed for 3 months in the PREVENU trial, the AUC was 0.63 (0.60-0.66) and 0.64 (0.61-0.67) for IMPROVE and Padua scores, respectively, both underperforming to identify VTE risk in non-critically ill medical inpatients. 47 In the study of Xiong et al, the AUC of Padua and IMPROVE scores for identifying VTE risk were 0.607 (0.533-0.681) and 0.609 (0.538-0.680), respectively. Consistency was significant between Padua and IMPROVE scores (kappa 0.789, P = .812). 11
Surgical Thromboprophylaxis
To date, the risk scores of surgical thromboprophylaxis for non-orthopedic surgical patients endorsed by guidelines are Caprini and Rogers scores. Caprini and Rogers scores were both approved by ACCP 48 and ASH 49 guidelines, respectively.
Caprini
Caprini score that was first invented by Caprini in 2005 could be the first and most classic VTE risk score globally recognized for surgical patients. It has 14 variables that each one represents 1 point, 8 variables that each one represents 2 points, 10 variables that each one represents 3 points, and 5 variables that each one represents 5 points. 50 There were slight modification made to the Caprini score in the ACCP guidelines. 48 In a retrospective cohort study validating Caprini score among 4844 critically ill surgical patients, patients with Caprini score greater than 8 were more likely to develop VTE events in hospitalization, compared with patients with Caprini scores of 7 to 8 (OR 1.37[1.02-1.85], P = .04), 5 to 6 (OR 1.35[1.16-1.57], P < .001), 3 to 4 (OR 1.30[1.16-1.47], P < .001), or 0 to 2 (OR 1.37[1.16-1.64], P < .001). Similarly, patients with Caprini score of 7 to 8 were more likely to develop inpatient VTE when compared with patients with Caprini score of 5 to 6, 3 to 4, or 0 to 2. Use of Caprini score in critically ill surgical patients was valid. 51
Rogers
Rogers score that was first invented by Rogers et al in 2007 has also been extensively endorsed.48,52 In a retrospective single-center study on 533 patients who underwent thoracic surgery, the AUC of Rogers score for VTE risk assessment was 0.52 (P = .62) which is mediocre. 53
Comparison
In a retrospective study comparing the performance of Caprini and Rogers scores in 17 713 patients undergoing surgery for gynecological oncology, the Caprini score was more limited to discriminate VTE risk among gynecological oncology patients because 97% are in the highest-risk category, compared with Rogers score which was actually also mediocre. 54 In the study of Tian et al, the AUC of Caprini score was 0.74 (P < .0001), which was better than that of the Rogers score. 53
PE Severity
To date, the acknowledged scores for the assessment of PE severity are PESI (Pulmonary Embolism Severity Index), Bova, FAST (heart-type fatty acid binding protein [H-FABP] or high-sensitivity troponin T [hsTnT], Syncope, Tachycardia), and Hestia scores, which are all endorsed by the latest ESC guidelines. 2 PESI score is also endorsed by the latest ACCP guidelines. 55 Because the ESC classification of PE severity does not have points, 2 it is not regarded as a score herein.
PESI
PESI score that was first invented by Aujesky et al in 2005 has 5 classes of risk strata. 56 It was then simplified to sPESI (Simplified Pulmonary Embolism Severity Index) by Jiménez et al in 2010, in order to improve user-friendliness. 57 In a meta-analysis including 44 298 PE patients from 71 studies which constructed, validated, updated, or studied prognostic models to predict all-cause or PE-related death for PE patients, both PESI and sPESI scores were most validated. 58
Bova
Bova score was first established by Bova et al in 2014. 59 It is a score for advanced stratification of 30-day PE-related death, hemodynamic collapse, or recurrent PE in patients with acute intermediate-risk symptomatic PE without hemodynamic instability.2,59 In a meta-analysis which evaluated the prognostic performance of Bova score among 8342 acute normotensive PE patients, the weighted AUC for predicting composite adverse outcome was 0.73 ± 0.09. 60
FAST
Similar to the Bova score, FAST which is also a score for advanced stratification of PE-related risk in patients without hemodynamic instability was first devised by Lankeit et al in 2013. 61 In 2014, H-FABP >7 ng·ml–1 by enzyme linked immunosorbent assay (ELISA) in the FAST score was modified into H-FABP ≥6 ng·ml–1 by immunoturbidimetry, because immunoturbidimetry provided prognostic information superior to ELISA, when integrated into FAST score. 62 In 2016, a modified FAST score with an age-adjusted hsTnT cut-off value instead of H-FABP demonstrated good prognostic performance, because H-FABP is not routinely available in the majority of hospitals. 63 In a post-hoc analysis of 868 normotensive PE patients to validate the FAST score, the C-index was similar between the modified FAST score (AUC = 0.67) and the 2019 ESC algorithm (AUC = 0.69). 64
Hestia
Hestia score that was actually a criterion including 11 questions was first created by Zondag et al in 2011. It was designed to assess whether the severity of PE is mild enough to be treated at home. 65 In a randomized non-inferiority trial involving 550 PE patients, the outpatient treatment of patients with PE selected on the basis of the Hestia criteria alone was associated with a low risk of adverse events. 66
Comparison
In the PERGO (Pulmonary Embolism Registry of Göttingen) study which compared the performance of modified FAST and Bova scores in 388 normotensive PE patients, the AUC of modified FAST and Bova scores was comparable (0.82[0.75-0.89] vs 0.80[0.73-0.87]). 63 In a prospective multicenter study comparing the performance for early discharge among PESI score, sPESI score, and Hestia criteria in 547 PE patients, Hestia criteria (41.7%) identified a higher proportion of candidates for early discharge than PESI (24.1%) and sPESI (18.3%). The incidence of a composite of VTE recurrence, major bleeding, or all-cause mortality within 30 days was 2.3%, 3.0%, and 2.6% according to PESI, sPESI, and Hestia criteria, without statistical differences. 67 In the HOME-PE randomized trial comparing Hestia rule and sPESI score in triaging 1970 PE patients for home treatment, the 30-day composite of recurrent VTE, major bleeding, or all-cause death occurred in 3.82% in the Hestia arm and 3.57% in the sPESI arm (P = .004 for non-inferiority) in the per-protocol population, suggesting they have similar safety and effectiveness. 68
VTE Recurrence
To date, the risk scores for VTE recurrence endorsed by guidelines are Vienna, HERDOO2 (Hyperpigmentation, Edema, or Redness in either leg; D-dimer level ≥250 µg·L−1; Obesity [body mass index ≥30]; or Older age [≥65 years]), DASH (D-dimer, Age, Sex, Hormonal therapy), DAMOVES (D-dimer, Age, Mutation, Obesity, Varicose veins, Eight, Sex), and Ottawa scores. All of these scores are recommended by the latest ESC guidelines, 2 whereas Vienna, HERDOO2, and DASH are also recommended by the latest ASH guidelines. 69
Vienna
Vienna score that was a nomogram was first created by Eichinger et al in 2010.2,70
In a prospective cohort study investigating the performance of Vienna score to identify low recurrence risk in 818 VTE patients, the recalibration of Vienna score improved identification of patients at low risk of VTE recurrence and stratification into distinct low-risk strata. 71 Nevertheless, in an RCT validating the clinical impact of Vienna on reducing VTE recurrence risk compared to usual care in 883 patients with unprovoked VTE, the application of the Vienna score was unlikely to reduce overall recurrence risk. 72
HERDOO2
HERDOO2 score that is only applicable for female patients was first created by Rodger et al in 2008.2,73 In the REVERSE II Study that prospectively validated the HERDOO2 score in 3155 consecutive female participants with a first unprovoked VTE, patients with none or one of the HERDOO2 criteria had a low risk of recurrent VTE and could safely discontinue anticoagulants after completing 5-12 months of short-term anticoagulation. 74
DASH
DASH score was first established by Tosetto et al in 2012. 75 In a retrospective cohort study for the external validation of DASH score in 827 patients with unprovoked VTE receiving anticoagulation and follow-up for at least 3 months, the results confirmed the validity of DASH score, particularly in young patients. 76
DAMOVES
DAMOVES score that is a nomogram was first created by Moreno et al in 2016. 77 In the only retrospective study validating DAMOVES score in 121 patients with unprovoked VTE completing at least 3 months of anticoagulation, the AUC was 0.83 (P < .001). 78
Ottawa
Ottawa score that is only applicable for cancer patients was invented by Louzada et al in 2012. 79 The original Ottawa score was modified and validated in 2016 for improving the convenience of clinical use. 80 In a meta-analysis investigating the accuracy of Ottawa score among14 963 patients with cancer-associated VTE, the Ottawa score either in its original or modified form is a useful tool to stratify the 6-month VTE recurrence risk during anticoagulation. 81
Comparison
In a systematic review comparing HERDOO2, Vienna, and DASH scores, although the Vienna score was most promising based on strong development methodology, applicability, and external validation, none of these models can be considered ready for use. 82
In a post-hoc analysis of the PADIS-PE trial validating HERDOO2, DASH, and Vienna scores in 371 patients with first unprovoked PE initially treated for 6 months of anticoagulation, the C-statistics of the aforementioned scores were 0.61, 0.60, and 0.58, respectively. HERDOO2 score was the only one that identified patients with low risk of VTE recurrence after anticoagulation discontinuance. 83
Bleeding Risk
To date, the risk scores for bleeding approved by VTE guidelines are OBRI (Outpatient Bleeding Risk Index), Kuijer, RIETE (Registro Informatizado de la Enfermedad Thromboembolica venosa), HAS-BLED (Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile international normalized ratio, Elderly [>65 years], Drugs/alcohol concomitantly), VTE-BLEED (actiVe cancer, male with uncontrolled hyperTension at baseline, anaEmia, history of BLeeding, agE > _60 years, rEnal Dysfunction), ACCP, and IMPROVE bleeding scores. ACCP score and IMPROVE bleeding score are endorsed by the ACCP84,85 and ASH 40 guidelines, respectively, whereas the rest of scores are all endorsed by the ESC guidelines. 2
OBRI
OBRI score that is specific for outpatients was first established by Beyth et al in 1998. 86 In a prospective study validating OBRI score in 222 consecutive VTE outpatients who were about to undergo standard warfarin anticoagulation, the OBRI score did discriminate between low- and moderate-risk groups (P = .03), and could be used to guide decisions on the optimal duration of anticoagulation. 87
Kuijer
Kuijer score was first invented by Kuijer et al in 1999. 88 In a retrospective study validating Kuijer score in 1 204 895 VTE patients receiving anticoagulant therapy for at least 3 months, a higher Kuijer risk strata was predictive for intracerebral bleeding (OR 1.28, P < .001), gastrointestinal bleeding (OR 1.56, P < .001) as well as necessity of transfusion of blood constituents (OR 2.94, P < .001), independently. 89
RIETE bleeding
RIETE bleeding score was first invented by Ruíz-Giménez et al in 2008. 90 In a prospective multicenter cohort study validating several bleeding scores including the RIETE bleeding for predicting major bleeding in 1034 consecutive VTE patients at the initiation of direct oral anticoagulants treatment, the C-statistics of RIETE bleeding score was modest (0.604). 91
HAS-BLED
HAS-BLED score was first invented by Pisters et al for the assessment of 1-year risk of major bleeding in patients with atrial fibrillation receiving oral anticoagulation in 2010. 92 In a retrospective cohort study validating HAS-BLED score in 132 280 VTE patients receiving the first 6 months of anticoagulant treatment, the C-index of HAS-BLED score was 0.722 for major bleeding, and 0.710 for all bleeding. 93
VTE-BLEED
VTE-BLEED score was first invented by Klok et al in 2016. 94 In a post-hoc analysis of 8240 VTE patients receiving stable anticoagulation in the Hokusai-VTE study, patients identified as high bleeding risk by VTE-BLEED score had a 4-fold increased risk of major bleeding during the chronic phase of treatment. 95
ACCP
ACCP score was first derived by Kearon et al in the CHEST guideline of antithrombotic therapy for VTE disease in 2012. 84 Non-steroidal anti-inflammatory drug was added into its modified version in 2016. 85 In a prospective study validating ACCP score in 2263 VTE patients on long-term anticoagulation in the Italian START2 Register, the C-statistic of the ACCP score was 0.55, 0.50, and 0.56 in the low, moderate, and high bleeding risk strata, respectively. ACCP score has an insufficiently predictive value for bleeding and cannot be used to guide decisions on extended anticoagulation. 96
IMPROVE bleeding
IMPROVE bleeding score was first invented by Decousus et al in 2011. 97 In a prospective study validating IMPROVE bleeding score in 1668 medical inpatients, Kaplan–Meier curves showed a higher cumulative incidence of major bleeding within 14 days in patients with an IMPROVE score ≥7.0 (P = .02). 98
Comparison
In a post-hoc analysis comparing several bleeding scores, including VTE-BLEED, Kuijer, RIETE bleeding, ACCP, OBRI, and HAS-BLED, in 743 patients aged ≥65 years receiving extended treatment with vitamin K antagonists after VTE diagnosis, the scores in order of AUC from largest to smallest were RIETE bleeding (0.63), ACCP (0.59), VTE-BLEED (0.57), Kuijer (0.55), HAS-BLED (0.54), and OBRI (0.47). 99
In a prospective multinational cohort study involving the comparison among modified ACCP, RIETE bleeding, VTE-BLEED, HAS-BLED, and OBRI scores for predicting major bleeding in 2516 patients with unprovoked VTE receiving extended anticoagulation, the scores in order of C-statistics from largest to smallest were ACCP (0.65), VTE-BLEED (0.61), HAS-BLED (0.57), RIETE (0.51), and OBRI (0.51). 100
Discussion
The current review introduces all risk scores associated with VTE recommended by 3 acknowledged guidelines, focusing on the development, modification, validation, and comparison of the scores. It aims to provide medical readers with a basic understanding of classic VTE risk scores, and to provide relevant researchers with an updated status quo of the scores. Despite their validation, the absolute efficiency and generalizability to different patient populations of some scores are still insufficient, and may need further improvement. Meanwhile, the cumbersome or inaccessible items and complicated risk calculation algorithm in some scores may compromise their user-friendliness and limit their widespread generalizability in daily clinical practice. Furthermore, clinicians may also be dazzled by various similar scores. Sometimes less is more, it could be imperative to identify the globally recognized VTE scores that are simple, efficient, user-friendly, and applicable to broad patient populations. In addition, with the rapid development of artificial intelligence, its application in the establishment of VTE scores or in the direct risk assessment of VTE patients may become a tendency in the future.
Limitations
The current review has some limitations. First, this review only covers risk scores associated with VTE recommended by the ESC, ACCP, and ASH guidelines, notwithstanding there are still many other relevant guidelines or other excellent VTE-related scores which are not endorsed by guidelines. Second, the quality of cited literature was not deeply evaluated in the current review. Third, no systematic review was performed in the current work. Fourth, despite our maximum endeavor not to leave out a single important literature, some relevant articles may still have been missed. Fifth, although there was a general criterion for the selection of literature, there were no absolute rules. Accordingly, the determination of literature selection was eventually at the discretion of the authors most of the time.
Conclusions
The current review provides a comprehensive overview of classic VTE risk scores in the VTE guidelines of ESC, ACCP, and ASH and is intended to provide medical readers with a comprehensive understanding of the related field. Although these risk scores are generally creditable, the search for simpler, more practical, and more universal scores may remain important work in the future.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241263856 - Supplemental material for Risk Scores in Venous Thromboembolism Guidelines of ESC, ACCP, and ASH: An Updated Review
Supplemental material, sj-docx-1-cat-10.1177_10760296241263856 for Risk Scores in Venous Thromboembolism Guidelines of ESC, ACCP, and ASH: An Updated Review by Wei Xiong, Yi Cheng and Yunfeng Zhao in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Author Contributions
Concept and design: WX. Literature search: all authors. Drafting of the manuscript: WX, YZ. Critical revision of the manuscript for important intellectual content: all authors. Supervision: WX, YZ. Guarantor: WX, YZ.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the international talent training program of Shanghai Xinhua Hospital (2023YGJRC04), the key sub-specialty construction funding of the Pudong Health System (PWZy2020-15), and the construction funding of clinical characteristic discipline of Pudong Health System (PWYts2021-04).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.